Correlation between Sleep Quality and Frailty Status among Middle-Aged and Older Taiwanese People: A Community-Based, Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
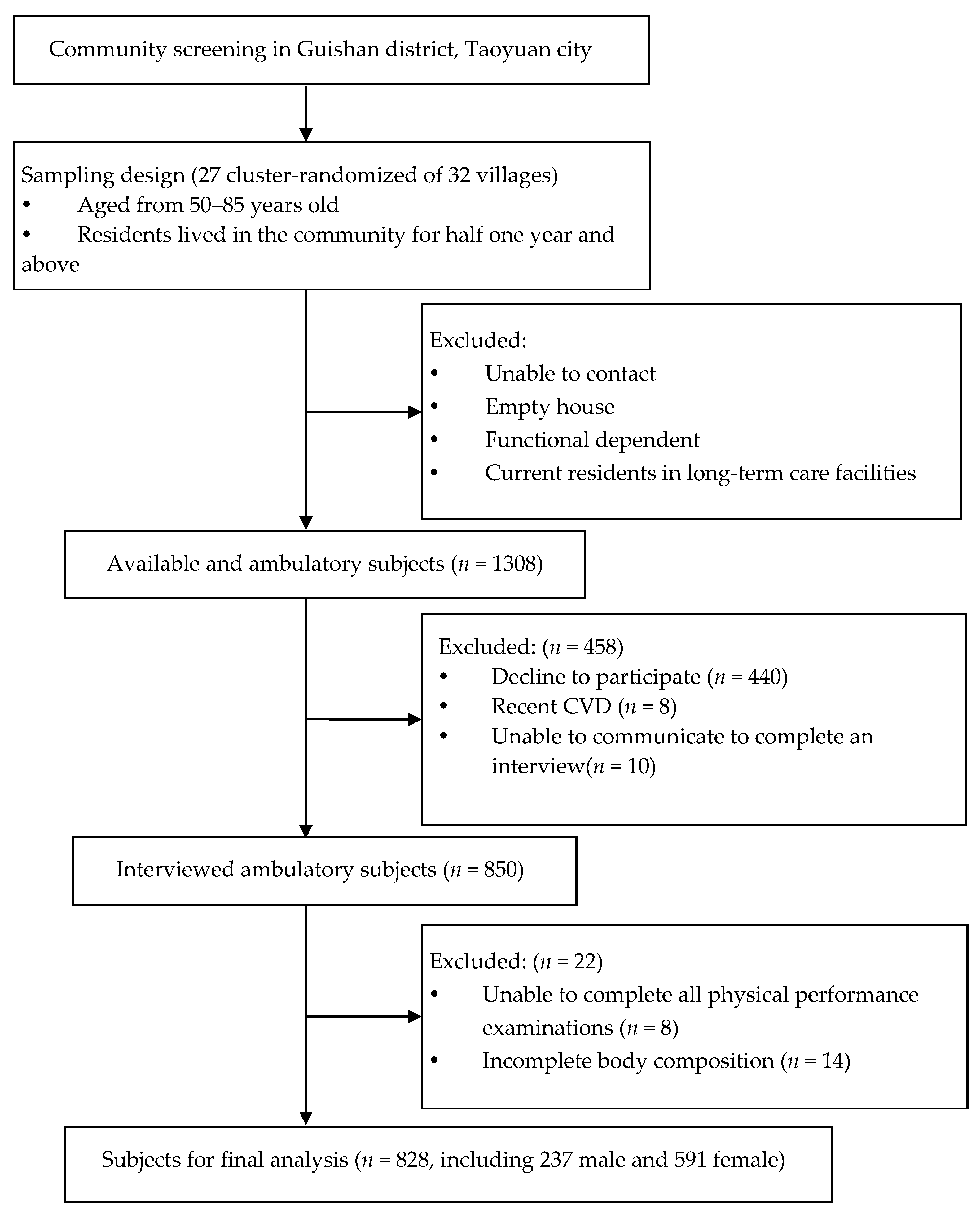
2.1. Study Design and Participants
2.2. Data Collection
2.3. Assessment of Sleep Quality
2.4. Definition of Frailty
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- National Development Council. Available online: https://pop-proj.ndc.gov.tw/upload/download/Population%20Projections%20for%20the%20Republic%20of%20China%20(Taiwan)-2020~2070.pdf (accessed on 13 December 2020).
- National Development Council. Available online: https://pop-proj.ndc.gov.tw/international.aspx?uid=69&pid=60 (accessed on 13 December 2020).
- Hu, H.M. Facing an Aging Society: Taiwan’s Universities in crisis. Gerontol. Geriatr. Educ. 2020, 41, 233–241. [Google Scholar] [CrossRef]
- Chen, H.-C.; Su, T.-P.; Chou, P. A Nine-Year Follow-up Study of Sleep Patterns and Mortality in Community-Dwelling Older Adults in Taiwan. Sleep 2013, 36, 1187–1198. [Google Scholar] [CrossRef] [Green Version]
- Tian, Y.; Li, L. Epidemiological study of sleep disorder in the elderly. Zhonghua Liu Xing Bing Xue Za Zhi. 2017, 38, 988. [Google Scholar]
- Magnavita, N.; Garbarino, S. Sleep, health and wellness at work: A scoping review. Int. J. Environ. Res. Public Health 2017, 14, 1347. [Google Scholar] [CrossRef] [Green Version]
- Garbarino, S.; Lanteri, P.; Durando, P.; Magnavita, N.; Sannita, W.G. Co-morbidity, mortality, quality of life and the healthcare/welfare/social costs of disordered sleep: A rapid review. Int. J. Environ. Res. Public Health 2016, 13, 831. [Google Scholar] [CrossRef]
- Jike, M.; Itani, O.; Watanabe, N.; Buysse, D.J.; Kaneita, Y. Long sleep duration and health outcomes: A systematic review, meta-analysis and meta-regression. Sleep Med. Rev. 2018, 39, 25–36. [Google Scholar] [CrossRef]
- Gulia, K.K.; Kumar, V.M. Sleep disorders in the elderly: A growing challenge. Psychogeriatrics 2018, 18, 155–165. [Google Scholar] [CrossRef]
- Tai, S.-Y.; Wang, W.-F.; Yang, Y.-H. Current status of sleep quality in Taiwan: A nationwide walk-in survey. Ann. Gen. Psychiatry 2015, 14, 36. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Hwang, A.-C.; Liu, L.-K.; Lee, W.-J.; Chen, L.-Y.; Peng, L.-N.; Lin, M.-H.; Chen, L.-K. Association of frailty and cardiometabolic risk among community-dwelling middle-aged and older people: Results from the I-Lan longitudinal aging study. Rejuvenation Res. 2015, 18, 564–572. [Google Scholar] [CrossRef]
- Hewitt, J.; Long, S.; Carter, B.; Bach, S.; McCarthy, K.; Clegg, A. The prevalence of frailty and its association with clinical outcomes in general surgery: A systematic review and meta-analysis. Age Ageing 2018, 47, 793–800. [Google Scholar] [CrossRef] [Green Version]
- Ofori-Asenso, R.; Chin, K.L.; Mazidi, M.; Zomer, E.; Ilomaki, J.; Zullo, A.R.; Gasevic, D.; Ademi, Z.; Korhonen, M.J.; LoGiudice, D. Global incidence of frailty and prefrailty among community-dwelling older adults: A systematic review and meta-analysis. JAMA Netw. Open 2019, 2, e198398. [Google Scholar] [CrossRef] [Green Version]
- Wai, J.L.-T.; Yu, D.S.-F. The relationship between sleep–wake disturbances and frailty among older adults: A systematic review. J. Adv. Nurs. 2020, 76, 96–108. [Google Scholar] [CrossRef]
- Pourmotabbed, A.; Boozari, B.; Babaei, A.; Asbaghi, O.; Campbell, M.S.; Mohammadi, H.; Hadi, A.; Moradi, S. Sleep and frailty risk: A systematic review and meta-analysis. Sleep Breath. 2020, 24, 1187–1197. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Blackwell, T.L.; Redline, S.; Ancoli-Israel, S.; Paudel, M.L.; Cawthon, P.M.; Dam, T.T.L.; Barrett-Connor, E.; Leung, P.C.; Stone, K.L. Sleep disturbances and frailty status in older community-dwelling men. J. Am. Geriatr Soc. 2009, 57, 2085–2093. [Google Scholar] [CrossRef] [Green Version]
- Hanlon, P.; Nicholl, B.I.; Jani, B.D.; Lee, D.; McQueenie, R.; Mair, F.S. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: A prospective analysis of 493 737 UK Biobank participants. Lancet Public Health 2018, 3, e323–e332. [Google Scholar] [CrossRef]
- Ma, W.Y.; Yang, C.Y.; Shih, S.R.; Hsieh, H.J.; Hung, C.S.; Chiu, F.C.; Lin, M.S.; Liu, P.H.; Hua, C.H.; Hsein, Y.C.; et al. Measurement of Waist Circumference: Midabdominal or iliac crest? Diabetes Care 2013, 36, 1660–1666. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.; Wu, Z.; Chen, Y.; Kan, Y.; Geng, M.; Xu, N.; Qian, H.; Wang, H.F.; Niu, M. Factors associated with appendicular skeletal muscle mass among male Chinese patients with stable chronic obstructive pulmonary disease: A hospital-based cross-sectional study. Med. Baltim. 2019, 98, e17361. [Google Scholar] [CrossRef]
- Tsai, P.S.; Wang, S.Y.; Wang, M.Y.; Su, C.T.; Yang, T.T.; Huang, C.J.; Fang, S.C. Psychometric evaluation of the Chinese version of the Pittsburgh Sleep Quality Index (CPSQI) in primary insomnia and control subjects. Qual. Life Res. 2005, 14, 1943–1952. [Google Scholar] [CrossRef]
- Xue, Q.-L. The frailty syndrome: Definition and natural history. Clin. Geriatr. Med. 2011, 27, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Carleton, R.N.; Thibodeau, M.A.; Teale, M.J.N.; Welch, P.G.; Abrams, M.P.; Robinson, T.; Asmundson, G.J.G. The center for epidemiologic studies depression scale: A review with a theoretical and empirical examination of item content and factor structure. PLoS ONE 2013, 8, e58067. [Google Scholar] [CrossRef] [Green Version]
- Stewart, A.L.; Mills, K.M.; King, A.C.; Haskell, W.L.; Gillis, D.; Ritter, P.L. CHAMPS physical activity questionnaire for older adults: Outcomes for interventions. Med. Sci. Sports Exerc. 2001, 33, 1126–1141. [Google Scholar] [CrossRef]
- Liu, X.; Hou, L.; Xia, X.; Liu, Y.; Zuo, Z.; Zhang, Y.; Zhao, W.; Hao, Q.; Yue, J.; Dong, B. Prevalence of sarcopenia in multi ethnics adults and the association with cognitive impairment: Findings from West-China health and aging trend study. BMC Geriatr. 2020, 20, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Otte, J.L.; Rand, K.L.; Landis, C.A.; Paudel, M.L.; Newton, K.M.; Woods, N.; Carpenter, J.S. Confirmatory factor analysis of the Pittsburgh Sleep Quality Index in women with hot flashes. Menopause 2015, 22, 1190. [Google Scholar] [CrossRef] [Green Version]
- Lichstein, K.L.; Taylor, D.J.; McCrae, C.S.; Petrov, M. Insomnia: Epidemiology and risk factors. In Principles and Practice of Sleep Medicine: Fifth Edition; Elsevier Inc.: Amsterdam, The Netherlands, 2010; pp. 827–837. [Google Scholar]
- Hayashino, Y.; Yamazaki, S.; Takegami, M.; Nakayama, T.; Sokejima, S.; Fukuhara, S. Association between number of comorbid conditions, depression, and sleep quality using the Pittsburgh Sleep Quality Index: Results from a population-based survey. Sleep Med. 2010, 11, 366–371. [Google Scholar] [CrossRef]
- Zhang, H.; Li, Y.; Zhao, X.; Mao, Z.; Abdulai, T.; Liu, X.; Tu, R.; Wang, Y.; Qian, X.; Jiang, J. The association between PSQI score and hypertension in a Chinese rural population: The Henan Rural Cohort Study. Sleep Med. 2019, 58, 27–34. [Google Scholar] [CrossRef]
- Okubo, N.; Matsuzaka, M.; Takahashi, I.; Sawada, K.; Sato, S.; Akimoto, N.; Umeda, T.; Nakaji, S. Relationship between self-reported sleep quality and metabolic syndrome in general population. BMC Public Health 2014, 14, 562. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.K.; Fielding, R.A. Exercise as an intervention for frailty. Clin. Geriatr. Med. 2011, 27, 101–110. [Google Scholar] [CrossRef] [Green Version]
- Kojima, G.; Walters, K.; Iliffe, S.; Taniguchi, Y.; Tamiya, N. Marital status and risk of physical frailty: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2020, 21, 322–330. [Google Scholar] [CrossRef]
- Cobo, A.; Vázquez, L.A.; Reviriego, J.; Rodríguez-Mañas, L. Impact of frailty in older patients with diabetes mellitus: An overview. Endocrinol. Y Nutr. Engl. Ed. 2016, 63, 291–303. [Google Scholar] [CrossRef]
- Stewart, R. Cardiovascular disease and frailty: What are the mechanistic links? Clin. Chem. 2019, 65, 80–86. [Google Scholar] [CrossRef] [Green Version]
- Kalmbach, D.A.; Pillai, V.; Arnedt, J.T.; Drake, C.L. DSM-5 Insomnia and Short Sleep: Comorbidity Landscape and Racial Disparities. Sleep 2016, 39, 2101–2111. [Google Scholar] [CrossRef]
- Irwin, M.R. Why sleep is important for health: A psychoneuroimmunology perspective. Annu. Rev. Psychol. 2015, 66, 143–172. [Google Scholar] [CrossRef] [Green Version]
- Álvarez-Satta, M.; Berna-Erro, A.; Carrasco-Garcia, E.; Alberro, A.; Saenz-Antoñanzas, A.; Vergara, I.; Otaegui, D.; Matheu, A. Relevance of oxidative stress and inflammation in frailty based on human studies and mouse models. Aging Albany Ny 2020, 12, 9982. [Google Scholar] [CrossRef]
- Rothman, M.D.; Leo-Summers, L.; Gill, T.M. Prognostic significance of potential frailty criteria. J. Am. Geriatr Soc. 2008, 56, 2211–2216. [Google Scholar] [CrossRef]
- Gordon, S.; Baker, N.; Kidd, M.; Maeder, A.; Grimmer, K. Pre-frailty factors in community-dwelling 40–75 year olds: Opportunities for successful ageing. BMC Geriatr. 2020, 20, 1–13. [Google Scholar] [CrossRef]
- Pengo, M.F.; Won, C.H.; Bourjeily, G. Sleep in Women Across the Life Span. Chest 2018, 154, 196–206. [Google Scholar] [CrossRef]
- Woods, N.F.; Mitchell, E.S. Sleep symptoms during the menopausal transition and early postmenopause: Observations from the Seattle Midlife Women’s Health Study. Sleep 2010, 33, 539–549. [Google Scholar] [CrossRef]
- Shen, T.-Y.; Strong, C.; Yu, T. Age at menopause and mortality in Taiwan: A cohort analysis. Maturitas 2020, 136, 42–48. [Google Scholar] [CrossRef]
- Chamberlain, A.M.; St Sauver, J.L.; Jacobson, D.J.; Manemann, S.M.; Fan, C.; Roger, V.L.; Yawn, B.P.; Finney Rutten, L.J. Social and behavioural factors associated with frailty trajectories in a population-based cohort of older adults. BMJ Open 2016, 6, e011410. [Google Scholar] [CrossRef] [Green Version]
- Minarik, P.A. Sleep disturbance in midlife women. J. Obs. Gynecol. Neonatal. Nurs. 2009, 38, 333–343. [Google Scholar] [CrossRef]


{kind=link}
| Variables | CPSQI | |||
|---|---|---|---|---|
| Total (n = 828) | CPSQI ≤ 5 (n = 388) | CPSQI > 5 (n = 440) | p Value | |
| Age (year) ¶ | 64.00 (59.00, 70.00) | 64.00 (59.00, 69.00) | 65.00 (60.00, 71.00) | 0.21 |
| SBP (mmHg) ¶ | 127.00 (116.00, 138.00) | 128.00 (118.00, 139.00) | 125.50 (115.00, 136.75) | 0.047 * |
| BMI (kg/m2) ¶ | 24.20 (22.00, 26.60) | 24.35 (22.10, 26.70) | 24.20 (21.93, 26.60) | 0.75 |
| WC (cm) | 85.08 ± 10.07 | 85.56 ± 9.82 | 84.67 ± 10.28 | 0.20 |
| ASMI (kg/m2) ¶ | 7.07 (6.55, 8.05) | 7.21 (6.58, 8.25) | 6.97 (6.52, 7.89) | 0.02 * |
| Gait speed (m/s) ¶ | 1.43 (1.30, 1.58) | 1.46 (1.29, 1.61) | 1.41 (1.26, 1.56) | 0.02 * |
| Hand grip strength (kg) ¶ | 25.60 (21.70, 31.68) | 26.50 (21.80, 33.85) | 24.80 (21.43, 29.70) | 0.002 § |
| Men, n (%) | 237 (28.62%) | 126 (32.47%) | 111 (25.23%) | 0.02 * |
| Exercise habit, n (%) | 602 (72.71%) | 282 (72.68%) | 320 (72.73%) | 0.99 |
| Marital status (single), n (%) | 171 (20.65%) | 70 (18.04%) | 101 (22.95%) | 0.08 |
| Education level | 0.03 * | |||
| No, n (%) | 65 (7.85%) | 27 (6.96%) | 38 (8.64%) | |
| Primary, n (%) | 314 (37.92%) | 132 (34.02%) | 182 (41.36%) | |
| Secondary, n (%) | 366 (44.20%) | 181 (46.65%) | 185 (42.05%) | |
| College, n (%) | 83 (10.02%) | 48 (12.37%) | 35 (7.95%) | |
| DM, n (%) | 119 (14.37%) | 51 (13.14%) | 68 (15.45%) | 0.34 |
| HTN, n (%) | 265 (32.00%) | 107 (27.58%) | 158 (35.91%) | 0.01 * |
| Hyperlipidemia, n (%) | 111 (13.41%) | 41 (10.57%) | 70 (15.91%) | 0.02 * |
| CVD, n (%) | 63 (7.61%) | 22 (5.67%) | 41 (9.32%) | 0.05 |
| Frailty status | <0.001 § | |||
| Non-frailty, n (%) | 592 (71.50%) | 306 (78.87%) | 286 (65.00%) | |
| Pre-frailty/frailty, n (%) | 236 (28.50%) | 82 (21.13%) | 154 (35.00%) | |
| Variables | Frailty | |||
|---|---|---|---|---|
| Total | Non-Frailty | Prefrailty/Frailty | p Value | |
| (n = 828) | (n = 592) | (n = 236) | ||
| Age (year) ¶ | 64.00 (59.00, 70.00) | 64.00 (59.00, 69.00) | 66.00 (60.00, 73.00) | <0.001 § |
| SBP (mmHg) ¶ | 127.00 (116.00, 138.00) | 127.00 (116.00, 138.00) | 125.00 (116.25, 137.75) | 0.56 |
| BMI (kg/m2) ¶ | 24.20 (22.00, 26.60) | 24.20 (22.10, 26.60) | 24.30 (21.80, 26.68) | 0.98 |
| WC (cm) | 85.08 ± 10.07 | 84.72 ± 9.65 | 86.00 ± 11.01 | 0.10 |
| ASMI (kg/m2) ¶ | 7.07 (6.55, 8.05) | 7.06 (6.55, 8.06) | 7.14 (6.56, 8.06) | 0.38 |
| Gait speed (m/s) ¶ | 1.43 (1.30, 1.58) | 1.46 (1.31, 1.61) | 1.34 (1.16, 1.54) | <0.001 § |
| Hand grip strength (kg) ¶ | 25.60 (21.70, 31.68) | 26.50 (23.00, 32.80) | 23.00 (17.60, 29.20) | <0.001 § |
| Men, n (%) | 237 (28.62%) | 166 (28.04%) | 71 (30.08%) | 0.56 |
| Exercise habit, n (%) | 602 (72.71%) | 450 (76.01%) | 152 (64.41%) | 0.001 § |
| Marital status (single), n (%) | 171 (20.65%) | 109 (18.41%) | 62 (26.27%) | 0.01 * |
| Education level | 0.001 § | |||
| No, n (%) | 65 (7.85%) | 35 (5.91%) | 30 (12.71%) | |
| Primary, n (%) | 314 (37.92%) | 215 (36.32%) | 99 (41.95%) | |
| Secondary, n (%) | 366 (44.20%) | 276 (46.62%) | 90 (38.14%) | |
| College, n (%) | 83 (10.02%) | 66 (11.15%) | 17 (7.20%) | |
| DM, n (%) | 119 (14.37%) | 74 (12.50%) | 45 (19.07%) | 0.02 * |
| HTN, n (%) | 265 (32.00%) | 181 (30.57%) | 84 (35.59%) | 0.16 |
| Hyperlipidemia, n (%) | 111 (13.41%) | 87 (14.70%) | 24 (10.17%) | 0.08 |
| CVD, n (%) | 63 (7.61%) | 38 (6.42%) | 25 (10.59%) | 0.04 * |
| Sleep quality | <0.001 § | |||
| CPSQI ≦ 5, n (%) | 388 (46.86%) | 306 (51.69%) | 82 (34.75%) | |
| CPSQI > 5, n (%) | 440 (53.14%) | 286 (48.31%) | 154 (65.25%) | |
| Variables | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | |
| CPSQI ≤ 5 | 1 | - | - | 1 | - | - | 1 | - | - |
| CPSQI > 5 | 2.00 | (1.46–2.75) | <0.001 | 2.01 | (1.46–2.76) | <0.001 | 1.95 | (1.38–2.77) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shih, A.-C.; Chen, L.-H.; Tsai, C.-C.; Chen, J.-Y. Correlation between Sleep Quality and Frailty Status among Middle-Aged and Older Taiwanese People: A Community-Based, Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 9457. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249457
Shih A-C, Chen L-H, Tsai C-C, Chen J-Y. Correlation between Sleep Quality and Frailty Status among Middle-Aged and Older Taiwanese People: A Community-Based, Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2020; 17(24):9457. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249457
Chicago/Turabian StyleShih, An-Chen, Lee-Hwa Chen, Chin-Chueh Tsai, and Jau-Yuan Chen. 2020. "Correlation between Sleep Quality and Frailty Status among Middle-Aged and Older Taiwanese People: A Community-Based, Cross-Sectional Study" International Journal of Environmental Research and Public Health 17, no. 24: 9457. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249457