Leading Enterovirus Genotypes Causing Hand, Foot, and Mouth Disease in Guangzhou, China: Relationship with Climate and Vaccination against EV71

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
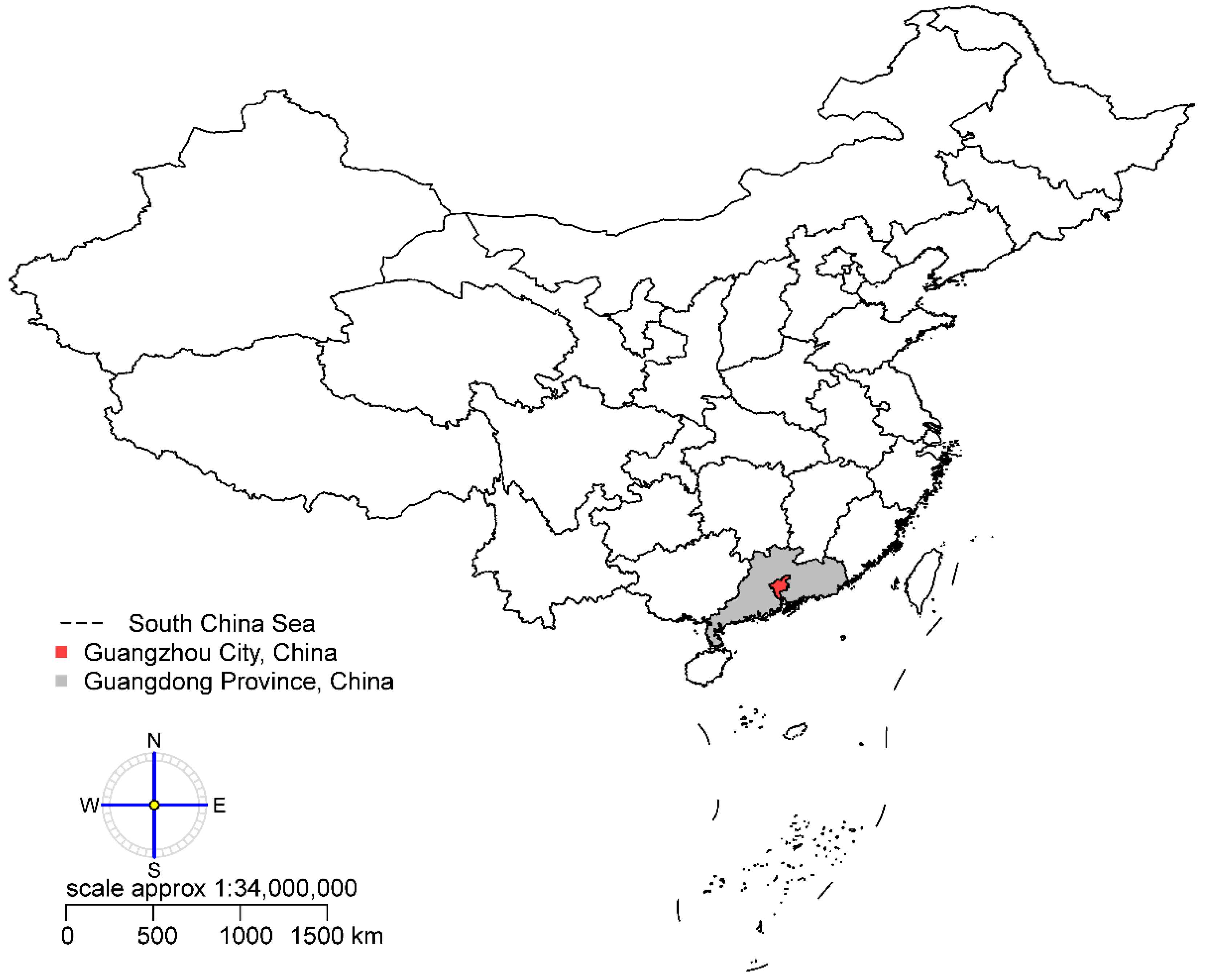
2.1. Study Area
2.2. Data Collection
2.3. Statistical Analysis
3. Results
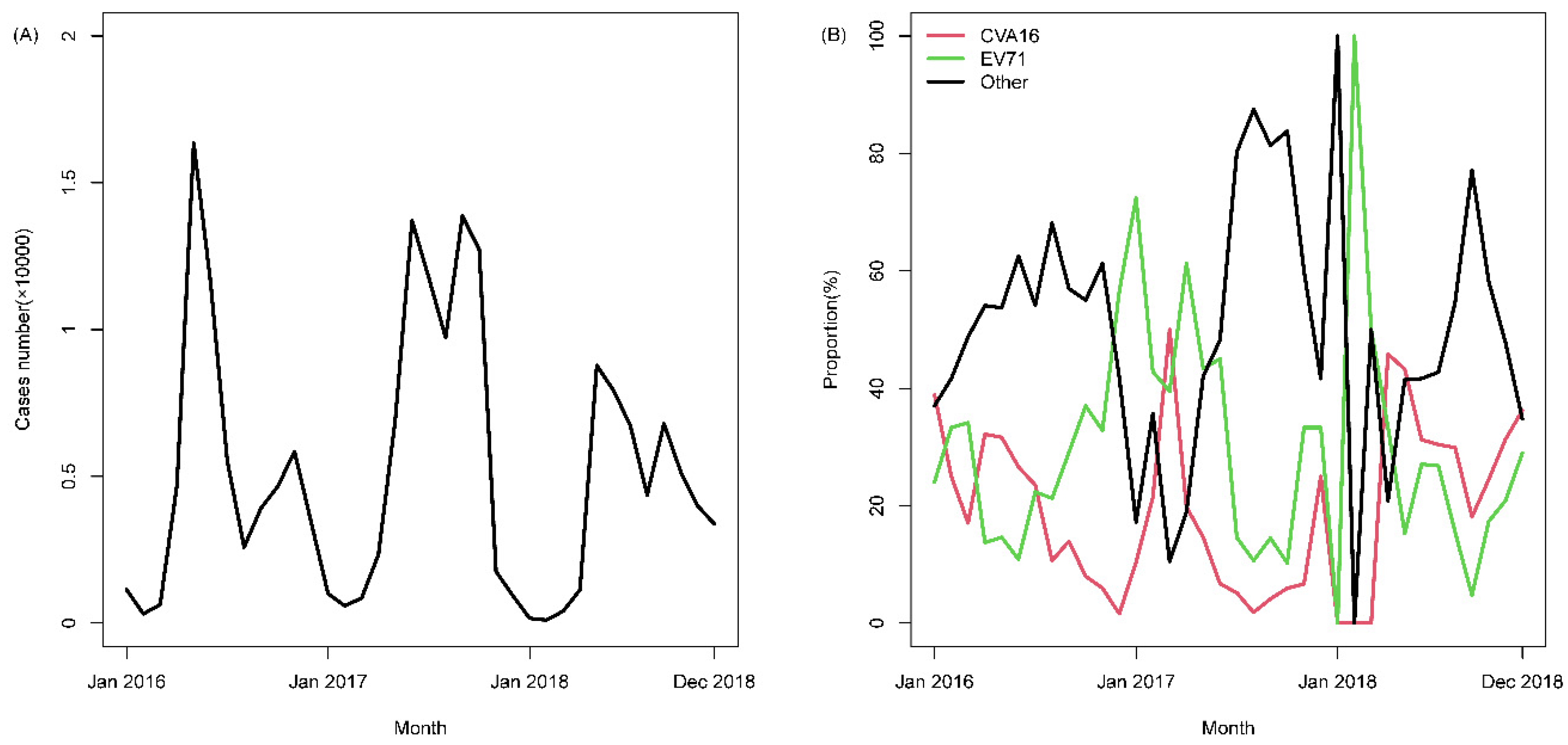
3.1. Characteristics of HFMD Cases
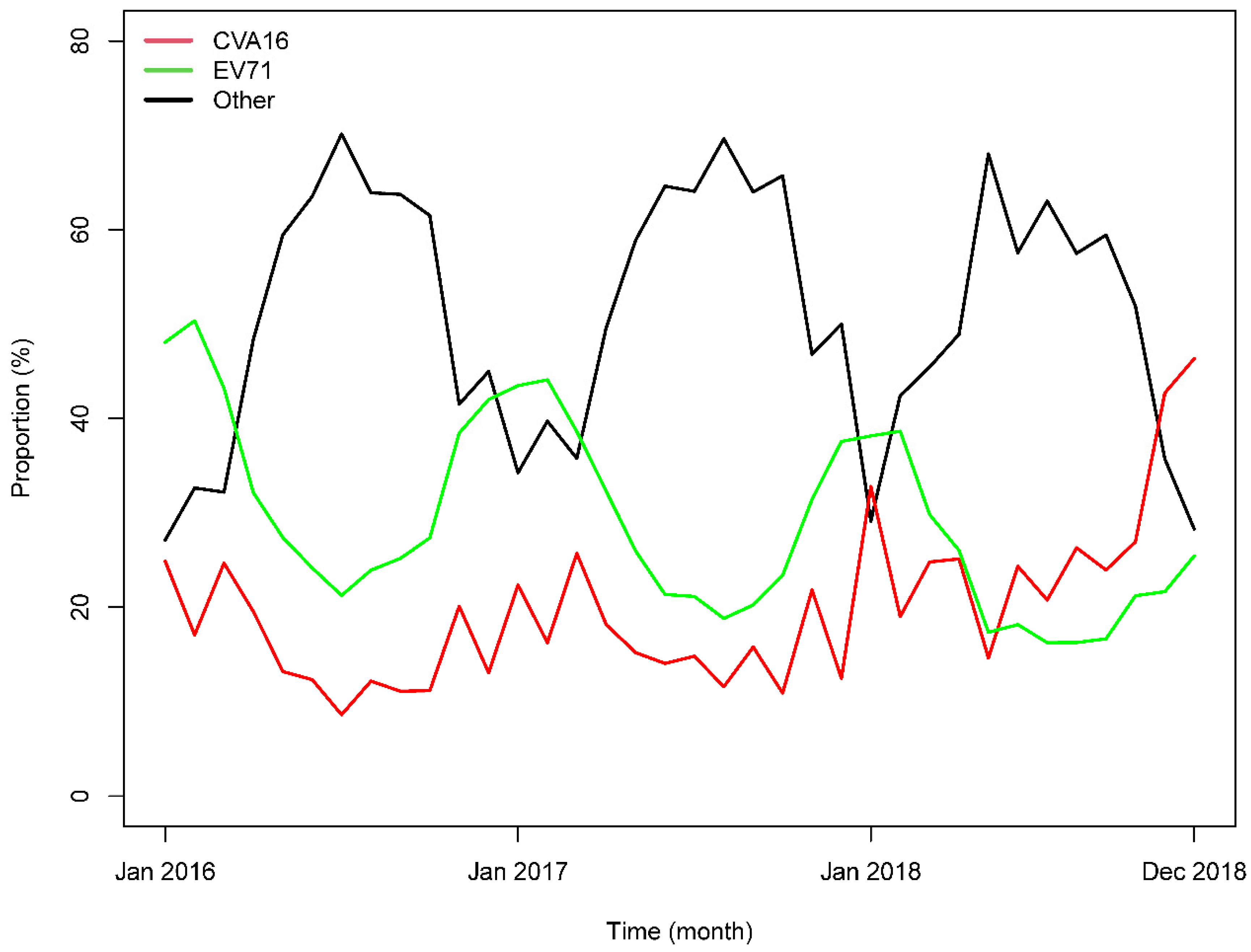
3.2. Associations between HFMD Cases and Genotype Frequency
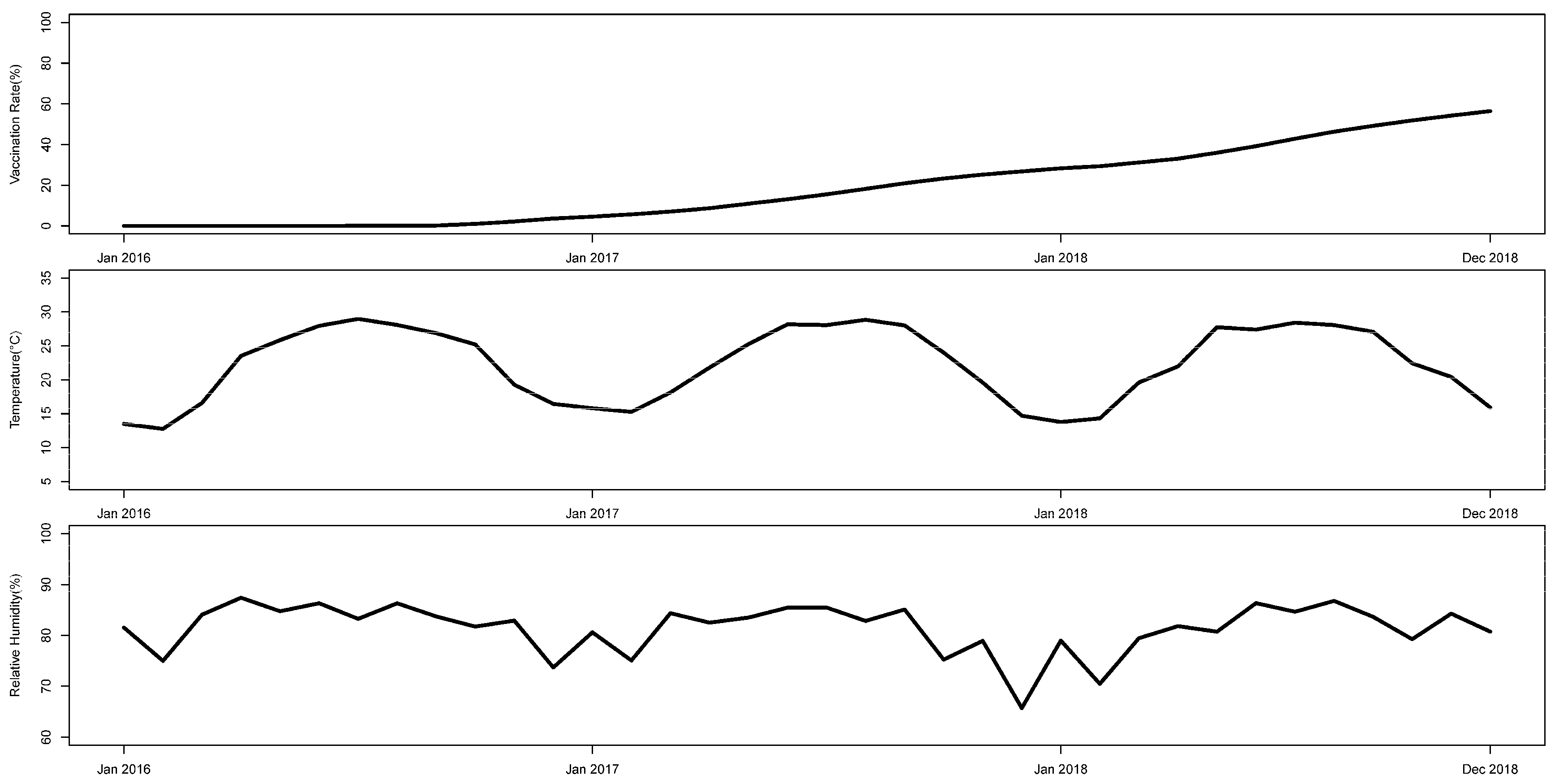
3.3. Associations between Genotype Frequency and Climate Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- U.S. Centers for Disease Control and Prevention. Hand, Foot, and Mouth Disease (HFMD). Available online: https://www.cdc.gov/hand-foot-mouth/index.html (accessed on 9 July 2020).
- Gonzalez, G.; Carr, M.J.; Kobayashi, M.; Hanaoka, N.; Fujimoto, T. Enterovirus-associated hand-foot and mouth disease and neurological complications in Japan and the rest of the world. Int. J. Mol. Sci. 2019, 20, 5201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Disease Prevention and Control. Epidemic Situation of Notifiable Infectious Diseases in China. Available online: http://www.nhc.gov.cn/wjw/rdts/list.shtml (accessed on 9 July 2020). (In Chinese)
- Ministry of Education of the People’s Republic of China. Regulations for Reporting of Infectious Diseases in Schools and Child Care Institutions (Trial). Available online: http://www.moe.gov.cn/srcsite/A17/moe_943/s3285/200604/t20060406_81035.html (accessed on 9 July 2020).
- Bruu, A.L. Enteroviruses: Polioviruses, Coxsackieviruses, Echoviruses and Newer Enteroviruses. In A Practical Guide to Clinical Virology. Philadelphia; Haaheim, L.R., Pattison, J.R., Whitley, R.J., Eds.; John Wiley & Sons, Ltd: Hoboken, NJ, USA, 2003; pp. 44–45. [Google Scholar] [CrossRef]
- Duffy, S. Why are RNA virus mutation rates so damn high? PLoS Biol. 2018, 16, e3000003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, Q.Y.; Wang, Y.; Bian, L.; Xu, M.; Liang, Z. EV71 vaccine, a new tool to control outbreaks of hand, foot and mouth disease (HFMD). Expert Rev. Vaccines 2016, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Huang, Y.; Bloom, M.S.; Zhang, Z.; Yang, Z.; Lu, J.; Xu, J.; Hao, Y. Assessing the vaccine effectiveness for hand, foot, and mouth disease in Guangzhou, China: A time-series analysis. Hum. Vacc. Immunother. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Peng, D.; Ma, Y.; Liu, Y.; Lv, Q.; Yin, F. Epidemiological and aetiological characteristics of hand, foot, and mouth disease in Sichuan Province, China, 2011–2017. Sci. Rep. 2020, 10, 6117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, H.; Li, Y.; Zhang, J.; Chen, Y.; Guo, Y.; Xiao, S.; Hu, J.; Wang, W.; Zhang, W.; Hu, Y.; et al. Quantifying the risk of hand, foot, and mouth disease (HFMD) attributable to meteorological factors in East China: A time series modelling study. Sci. Total Environ. 2020, 728, 138548. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Gasparrini, A.; Huang, J.; Liao, Q.; Liu, F.; Yin, F.; Yu, H.; Li, X. The exposure-response relationship between temperature and childhood hand, foot and mouth disease: A multicity study from mainland China. Environ. Int. 2017, 100, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Lawrence, W.R.; Zhang, W.; Zhang, D.; Yu, S.; Hao, Y. Interactions between climate factors and air pollution on daily HFMD cases: A time series study in Guangdong, China. Sci. Total Environ. 2019, 656, 1358–1364. [Google Scholar] [CrossRef] [PubMed]
- Wikipedia. Guangzhou. 5 September 2020. Available online: https://en.wikipedia.org/wiki/Guangzhou (accessed on 11 September 2020).
- National Health Commission of China. Hand, Foot and Mouth Disease Prevention and Control Guidelines. 2 May 2008. Available online: http://www.nhc.gov.cn/jkj/s3577/200805/e73df45b7b1549188b1d4e1efd604da9.shtml (accessed on 11 December 2020).
- Egozcue, J.J.; Pawlowsky-Glahn, V.; Mateu-Figueras, G.; Barceló-Vidal, C. Isometric Logratio transformations for compositional data analysis. Math. Geol. 2003, 35, 279–300. [Google Scholar] [CrossRef]
- Pons-Salort, M.; Grassly, N.C. Serotype-specific immunity explains the incidence of diseases caused by human enteroviruses. Science 2018, 361, 800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bian, L.; Wang, Y.; Yao, X.; Mao, Q.; Xu, M.; Liang, Z. Coxsackievirus A6: A new emerging pathogen causing hand, foot and mouth disease outbreaks worldwide. Expert Rev. Anti Infect. 2015, 13, 1061–1071. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Zhang, G.; Guo, P.; Liu, J.; Gao, Q.; Xu, X.; Gong, L. Epidemiological characterizations, pathogen spectrum and molecular characteristics of Coxsackievirus A16 from patients with HFMD in Yantai, Shandong, China between 2011 and 2015. Hum. Vacc. Immunother. 2017, 13, 1831–1838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.; Ju, Y.; Chen, M.; Xie, Z.; Zhou, K.; Tan, Y.; Mo, J. Epidemiological and genetic characteristics of EV71 in hand, foot, and mouth disease in Guangxi, southern China, from 2010 to 2015. PLoS ONE 2017, 12, e188640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, X.; Zhang, M.; Zhao, C.; Zheng, P.; Zhang, X.; Xu, J. From monovalent to multivalent vaccines, the exploration for potential preventive strategies against hand, foot, and mouth disease (HFMD). Virol. Sin. 2020. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Leung, K.; Jit, M.; Yu, H.; Yang, J.; Liao, Q.; Liu, F.; Zheng, Y.; Wu, J.T. Cost-effectiveness of bivalent versus monovalent vaccines against hand, foot and mouth disease. Clin. Microbiol. Infect. 2020, 26, 373–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, S.; Changizi, N.; Hamarneh, G. The isometric log-ratio transform for probabilistic multi-label anatomical shape representation. IEEE Trans. Med. Imaging 2014, 33, 1890–1899. [Google Scholar] [CrossRef] [PubMed]
- Buccianti, A.; Mateu-Figueras, G.; Pawlowsky-Glahn, V. Compositional Data Analysis in the Geosciences: From Theory to Practice; Geological Society of London: London, UK, 2006. [Google Scholar]
- Yang, H.; He, Y.; Zhang, Z.; Xian, H.; Luo, M.; Zhang, H.; Yao, X. Etiology of hand, foot and mouth disease in Shenzhen, Guangdong, 2011. Dis. Surveill. 2013, 28, 189–192. (In Chinese) [Google Scholar] [CrossRef]
- Guo, W.; Chen, G.; Xie, G.; Du, L.; Tang, Q. Mosaic genome of Human Coxsackievirus A4 associated with herpangina and HFMD in Yancheng, China, 2016 and 2018. Int. J. Infect. Dis. 2020, 96, 538–540. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total | Undetected | Genotyped |
|---|---|---|---|
| n(%) | n(%) | n(%) | |
| 185,838 (100) | 180,771 (97.27) | 5067 (2.73) | |
| Year | |||
| 2016 | 60,685 (32.65) | 58,815 (32.54) | 1870 (36.91) |
| 2017 | 76,195 (41.00) | 74,117 (41.00) | 2078 (41.01) |
| 2018 | 48,958 (26.34) | 47,839 (26.46) | 1119 (22.08) |
| Age | |||
| 0+ | 22,449 (12.08) | 21,745 (12.03) | 704 (13.89) |
| 1+ | 55,423 (29.82) | 53,832 (29.78) | 1591 (31.40) |
| 2+ | 33,481 (18.02) | 32,686 (18.08) | 795 (15.69) |
| 3+ | 33,288 (17.91) | 32,368 (17.91) | 920 (18.16) |
| 4+ | 19,540 (10.51) | 19,012 (10.52) | 528 (10.42) |
| 5+ | 9821 (5.28) | 9535 (5.27) | 286 (5.64) |
| 6+ | 11,836 (6.37) | 11,593 (6.41) | 243 (4.80) |
| Sex | |||
| Male | 112,181 (60.36) | 109,077 (60.34) | 3104 (61.26) |
| Female | 73,657 (39.64) | 71,694 (39.66) | 1963 (38.74) |
| Severity | |||
| Mild cases | 185,833 (100.00) | 180,771 (100.00) | 5062 (99.90) |
| Severe cases | 5 (0.00) | 0 (0.00) | 5 (0.10) |
| Virus | |||
| Undetected | 180,771 (97.27) | 180,771 (100.00) | — |
| CVA16 | 985 (0.53) | — | 985 (19.44) |
| EV71 | 1202 (0.65) | — | 1202 (23.72) |
| Other enterovirus | 2880 (1.55) | — | 2880 (56.84) |
| Factors | ILRCVA16 | ILREV71 | ||
|---|---|---|---|---|
| β | 95%CI | β | 95%CI | |
| Vaccination rate (%) | −0.562 * | (−0.809, −0.316) | −0.235 * | (−0.435, −0.035) |
| Temperature (°C) | −0.056 * | (−0.103, −0.010) | −0.062 * | (−0.088, −0.035) |
| Humidity (%) | −0.009 | (−0.068, 0.049) | −0.041 * | (−0.078, −0.004) |
| Factors | ILRCVA16 | ILREV71 | ||
|---|---|---|---|---|
| β | 95%CI | β | 95%CI | |
| Vaccination rate (%) | −0.461 * | (−0.713, −0.210) | −0.152 | (−0.326, 0.022) |
| Temperature (°C) | −0.068 * | (−0.126, −0.009) | −0.065 * | (−0.105, −0.024) |
| Humidity (%) | 0.041 | (−0.027, 0.108) | 0.011 | (−0.035, 0.058) |
| Factors | Other Enteroviruses | CVA16 | EV71 | |||
|---|---|---|---|---|---|---|
| % | (P2.5, P97.25) | % | (P2.5, P97.25) | % | (P2.5, P97.25) | |
| Vaccination rate (%) | 13.84 | (6.55, 20.38) | −8.77 | (−13.86, −2.52) | −5.07 | (−9.41, −0.30) |
| Temperature (°C) | 2.52 | (1.00, 3.99) | −0.76 | (−2.20, 0.76) | −1.76 | (−2.79, −0.71) |
| Humidity (%) | −1.10 | (−2.76, 0.58) | 0.80 | (−0.92, 2.59) | 0.30 | (−1.03, 1.57) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, Z.; Huang, Y.; Lawrence, W.R.; Xu, J.; Yang, Z.; Lu, J.; Zhang, Z.; Hao, Y. Leading Enterovirus Genotypes Causing Hand, Foot, and Mouth Disease in Guangzhou, China: Relationship with Climate and Vaccination against EV71. Int. J. Environ. Res. Public Health 2021, 18, 292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010292
Du Z, Huang Y, Lawrence WR, Xu J, Yang Z, Lu J, Zhang Z, Hao Y. Leading Enterovirus Genotypes Causing Hand, Foot, and Mouth Disease in Guangzhou, China: Relationship with Climate and Vaccination against EV71. International Journal of Environmental Research and Public Health. 2021; 18(1):292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010292
Chicago/Turabian StyleDu, Zhicheng, Yong Huang, Wayne R. Lawrence, Jianxiong Xu, Zhicong Yang, Jianyun Lu, Zhoubin Zhang, and Yuantao Hao. 2021. "Leading Enterovirus Genotypes Causing Hand, Foot, and Mouth Disease in Guangzhou, China: Relationship with Climate and Vaccination against EV71" International Journal of Environmental Research and Public Health 18, no. 1: 292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010292