
A Proposed Theoretical Model for Sustainable and Safe Commensality among Older Adults


Abstract
:1. Introduction
1.1. Definitions of Commensality
1.2. Identifying the Problem
1.3. Food Safety and Commensality
1.4. Hospitality and Commensality
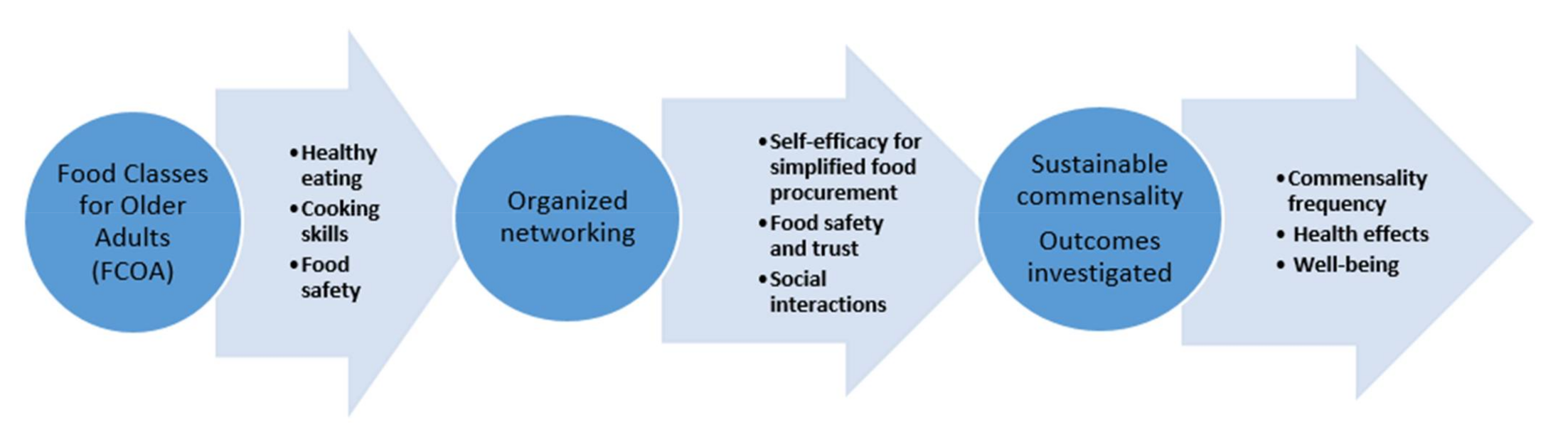
2. A Proposed Theoretical Model for Sustainable and Safe Commensality Among Older Adults
2.1. Food Classes for Older Adults
2.2. Healthy Eating and Cooking Skills
2.3. Food Safety
3. Organized Networking
3.1. Self-Efficacy for Simplified Food Procurement
3.2. Food Safety and Trust
4. Social Interactions
5. Sustainable Commensality and Proposed Measurements
5.1. Commensality Frequency
5.2. Health Effects
5.3. Well-Being
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Giacoman, K. The dimensions and role of commensality: A theoretical model drawn from the significance of communal eating among adults in Santiago, Chile. Appetite 2016, 107, 460–470. [Google Scholar] [CrossRef]
- Fischler, C. Commensality, society and culture. Soc. Sci. Inf. 2011, 50, 528–548. [Google Scholar] [CrossRef]
- Chee-Beng, T. Commensality and the Organization of Social Relations. In Commensality, from Everyday Food to Feast; Kerner, S., Chou, S., Warmind, M., Eds.; Bloomsbury Academic USA: New York, NY, USA, 2015; pp. 13–29. [Google Scholar]
- Vesnaver, E.; Keller, H. Social influences and eating behavior in later life. J. Nutr. Gerontol. Geriatr. 2011, 30, 2–23. [Google Scholar] [CrossRef]
- Herman, P. The social facilitation of eating. A review. Appetite 2015, 86, 61–73. [Google Scholar] [CrossRef]
- Pachucki, M.; Karter, A.; Adlerc, N.; Moffet, H.; Warton, E.; Schillinger, D.; Hendrickson O’Connelle, B.; Laraiaf, B. Eating with others and meal location are differently associated with nutrient intake by sex: The diabetes study of northern California (DISTANCE). Appetite 2018, 127, 203–213. [Google Scholar] [CrossRef]
- Mc Corry-Breen, F.; Coveney, J.; Pflaum, C.A.H. A literature scoping review of eating practices and food environments in 1 and 2-person households in the UK, Australia and USA. Appetite 2018, 126, 43–53. [Google Scholar] [CrossRef]
- SCB, Statistiska Centralbyrån. Statistics Sweden. Available online: http://www.scb.se (accessed on 2 September 2020). (In Swedish).
- World Health Organization. Integrated Surveillance of Noncommunicable Diseases (iNCD) A European Union-WHO Project; WHO Regional Office for Europe: Copenhagen, Denmark, 2015. [Google Scholar]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition-A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Swedish Food Agency. Sjukdomsbördan av Inhemska Fall av Matförgiftning Smittskyddsunderlag 2018-Del 1. Livsmedelsverkets Rapportserie, Nr 2, 1–32. Available online: https://www.livsmedelsverket.se/globalassets/publikationsdatabas/rapporter/2019/l-2019-nr-02-sjukdomsbordan-av-inhemska-fall-av-matforgiftning-smittskyddsunderlag-del-1-livsmedelsverkets_rapportserie.pdf?AspxAutoDetectCookieSupport=1 (accessed on 27 October 2019). (In Swedish).
- Cecchini, M.; Sassi, F.; A Lauer, J.; Lee, Y.Y.; Guajardo-Barron, V.; Chisholm, D. Tackling of unhealthy diets, physical inactivity, and obesity: Health effects and cost-effectiveness. Lancet 2010, 376, 1775–1784. [Google Scholar] [CrossRef]
- Agrifood Economics Centre. Samhällskostnader För Fem Livsmedelsburna Sjukdomar i Sverige. Policy Brief. Available online: http://www.agrifood.se/publication.aspx?FKeyID=1822 (accessed on 18 January 2021).
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 779–788. [Google Scholar] [CrossRef]
- Herman, C.P.; Roth, D.A.; Polivy, J. Effects of the presence of others on food intake: A normative interpretation. Psychol. Bull. 2003, 129, 873–886. [Google Scholar] [CrossRef]
- Hetherington, M.M.; Anderson, A.S.; Norton, G.N.M.; Newson, L. Situational effects on meal intake: A comparison of eating alone and eating with others. Physiol. Behav. 2006, 88, 498–505. [Google Scholar] [CrossRef]
- Redmond, E.C.; Griffith, C.J. Consumer food handling in the home: A review of food safety studies. J. Food Prot. 2003, 66, 130–161. [Google Scholar] [CrossRef]
- Marklinder, I.M.; Lindblad, M.; Eriksson, L.M.; Finnson, A.M.; Lindqvist, R. Home storage temperatures and consumer handling of refrigerated foods in Sweden. J. Food Prot. 2004, 67, 2570–2577. [Google Scholar] [CrossRef]
- Ovca, A.; Jevšnik, M. Maintaining a cold chain from purchase to the home and at home: Consumer opinions. Food Control. 2009, 20, 167–172. [Google Scholar] [CrossRef]
- Thomas, N.; Emond, R. Living alone but eating together: Exploring lunch clubs as a dining out experience. Appetite 2017, 119, 34–40. [Google Scholar] [CrossRef]
- Sidenvall, B.; Nydahl, M.; Fjellström, C. The meal as a gift—The meaning of cooking among retired women. J. Appl. Gerontol. 2000, 19, 405–423. [Google Scholar] [CrossRef]
- Johannesson, J.; Rothenberg, E.; Ivanoff, S.; Slinde, F. Gender differences in practice, knowledge and attitudes regarding food habits and meal patterns among community dwelling older adults. J. Aging Res. Clin. Pract. 2016, 5, 220–228. [Google Scholar]
- Marklinder, I.; Ahlgren, R.; Blücher, A.; Börjesson, S.-M.E.; Hellkvist, F.; Moazzami, M.; Schelin, J.; Zetterström, E.; Eskhult, G.; Danielsson-Tham, M.-L.; et al. Food safety knowledge, sources thereof and self-reported behaviour among university students in Sweden. Food Control 2020, 113, 107130. [Google Scholar] [CrossRef]
- European Food Safety Authority. The European Union summary report to trends and sources of zoonoses, zoonotic agents and foodborne outbreaks in 2013. EFSA J. 2015, 13, 3991. [Google Scholar]
- Krause, G.; Altmann, D.; Faensen, D.; Porten, K.; Benzler, J.; Pfoch, T.; Ammon, A.; Kramer, M.H.; Claus, H. SurvNet electronic surveillance system for infectious disease outbreaks, Germany. Emerg. Infect. Dis. 2007, 13, 1548–1555. [Google Scholar] [CrossRef]
- Public Health Agency of Sweden. Available online: https://www.folkhalsomyndigheten.se/the-public-health-agency-of-sweden/ (accessed on 27 October 2019).
- Jevšnik, M.; Hlebec, V.; Peter, R. Consumers’ awareness of food safety from shopping to eating. Food Control 2008, 19, 737–745. [Google Scholar] [CrossRef]
- Langiano, E.; Ferrara, M.; Lanni, L.; Viscardi, V.; Abbatecola, A.M.; De Vito, E. Food safety at home: Knowledge and practices of consumers. J. Public Health 2011, 20, 47–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrd-Bredbenner, C.; Berning, J.; Martin-Biggers, J.; Quick, V. Food safety in home kitchens: A synthesis of the literature. Int. J. Environ. Res. Public Health 2013, 10, 4060–4085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Røssvoll, E.; Lavik, R.; Ueland, Ø.; Jacobsen, E.; Hagtvedt, T.; Langsrud, S. Food safety practices among Norwegian consumers. J. Food Prot. 2013, 76, 1939–1947. [Google Scholar] [CrossRef]
- Marklinder, I.; Magnusson, M.; Nydahl, M. CHANCE: A healthy lifestyle in terms of food handling and hygiene. Br. Food J. 2013, 115, 223–234. [Google Scholar] [CrossRef]
- Marklinder, I.; Nydahl, M. Health Knowledge and Behaviour Among Residents in a Swedish City District-Designing Health Information for the Public. In Community Health Information in Europe; Freytag-Leyer, B., Alisch, M., Eds.; University Press: Kassel, Germany, 2011; pp. 87–103. [Google Scholar]
- O’key, V.; Hugh-Jones, S. I don’t need anybody to tell me what I should be doing: A discursive analysis of maternal accounts of (mis)trust of healthy eating information. Appetite 2010, 54, 524–532. [Google Scholar] [CrossRef]
- Evans, E.W.; Redmond, E.C. Older adult consumer knowledge, attitudes, and self-reported storage practices of ready-to-eat food products and risks associated with listeriosis. J. Food Prot. 2016, 79, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Galenkamp, H.; Deeg, D.J.H. Increasing social participation of older people: Are there different barriers for those in poor health? Introduction to the special section. Eur. J. Ageing 2016, 13, 87–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nydahl, M.; Koochek, A. Hälsofrämjande aktiviteter riktade mot äldre-erfarenheter från Matskola för äldre. Svensk Geriatrik 2019, 1, 16–21. (In Swedish) [Google Scholar]
- Lange, M.; Göranzon, H.; Marklinder, I. Self-reported food safety knowledge and behavior among Home and Consumer Studies students. Food Control 2016, 67, 265–272. [Google Scholar] [CrossRef]
- Bandura, A. Health promotion from the perspective of social cognitive theory. Psychol. Heal. 1998, 13, 623–649. [Google Scholar] [CrossRef]
- Richert, J.; Reuter, T.; Wiedemann, A.U.; Lippke, S.; Ziegelmann, J.; Schwarzer, R. Differential effects of planning and self-efficacy on fruit and vegetable consumption. Appetite 2010, 54, 611–614. [Google Scholar] [CrossRef] [PubMed]
- Berg, L. Trust in the age of mad cow disease: A comparative study of consumers’ evaluation of safety in Belgium, Britain and Norway. Appetite 2004, 42, 21–32. [Google Scholar] [CrossRef]
- Ozawa, S.; Sripad, P. How do you measure trust in the health system? A systematic review of the literature. Soc. Sci. Med. 2013, 91, 10–14. [Google Scholar] [CrossRef]
- Turrini, A.; D’Addezio, L.; Maccati, F.; Davy, B.M.; Arber, S.; Davidson, K.; Grunert, K.; Schuhmacher, B.; Pfau, C.; Kozłowska, K.; et al. The informal networks in food procurement by older people—A cross European comparison. Ageing Int. 2010, 35, 253–275. [Google Scholar] [CrossRef]
- Holmes, B.; Roberts, C. Diet quality and the influence of social and physical factors on food consumption and nutrient intake in materially deprived older people. Eur. J. Clin. Nutr. 2011, 65, 538–545. [Google Scholar] [CrossRef] [Green Version]
- Gustafsson, K.; Andersson, J.; Andersson, I.; Nydahl, M.; Sjödén, P.-O.; Sidenvall, B. Associations between perceived cooking ability, dietary intake and meal patterns among older women. Scand. J. Nutr. 2002, 46, 31–39. [Google Scholar] [CrossRef]
- Grunert, K.G.; Dean, M.; Raats, M.M.; Nielsen, N.A.; Lumbers, M. A measure of satisfaction with food-related life. Appetite 2007, 49, 486–493. [Google Scholar] [CrossRef]
- Marovelli, B. Cooking and eating together in London: Food sharing initiatives as collective spaces of encounter. Geoforum 2019, 99, 190–201. [Google Scholar] [CrossRef]
- Berleen, G. A healthier Elderly Population in Sweden; National Institute of Public Health: Sandviken, Sweden, 2004. [Google Scholar]
- Sahyoun, N.R.; Pratt, C.A.; Anderson, A. Evaluation of nutrition education interventions for older adults: A proposed framework. J. Am. Diet. Assoc. 2004, 104, 58–69. [Google Scholar] [CrossRef]
- Nydahl, M.; Jacobsson, F.; Enroth, M.; Marklinder, I. A simplified information model increased the level of health knowledge among the residence in a city district. Br. Food J. 2012, 114, 910–925. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Session 1 (3 h) | Nutritious food—how do I know it is good enough to promote good health? |
| |
| |
| |
| |
| |
| Practical and social part | |
| Cooking and commensality | |
| Summing up | |
| Session 2 (3 h) | Taste, smell, and hygiene. How to handle food to avoid ill health |
| |
| |
| |
| |
| Practical and social part | |
| Cooking and commensality | |
| Summing up | |
| Session 3 (3 h) | Practical aspects—food ingredients and food procurement |
| |
| |
| |
| |
| Practical and social part | |
| Cooking and commensality | |
| Summing up | |
| Session 4 (3 h) | To cook or not to cook |
| |
| |
| |
| |
| |
| |
| Practical and social part | |
| Cooking and commensality | |
| Summing up | |
| Session 5 (3 h) | The contents of the last session are based on the participants’ requests |
| Theory part | |
| Practical and social part Cooking and commensality | |
| Summing up |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marklinder, I.; Nydahl, M. A Proposed Theoretical Model for Sustainable and Safe Commensality among Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 1172. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031172
Marklinder I, Nydahl M. A Proposed Theoretical Model for Sustainable and Safe Commensality among Older Adults. International Journal of Environmental Research and Public Health. 2021; 18(3):1172. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031172
Chicago/Turabian StyleMarklinder, Ingela, and Margaretha Nydahl. 2021. "A Proposed Theoretical Model for Sustainable and Safe Commensality among Older Adults" International Journal of Environmental Research and Public Health 18, no. 3: 1172. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031172