
Impact of Fear of Contracting COVID-19 and Complying with the Rules of Isolation on Nutritional Behaviors of Polish Adults



Abstract
:1. Introduction
- There is a relationship between the level of fear of contracting Covid-19 and the degree to which isolation rules are being observed.
- The group with the highest fear level and isolation adherence consists predominantly of women, as well as young and elderly people.
- The changes in eating behavior concern such areas as food purchases, eating patterns, and type of food product consumed.
- The greatest changes in all of the analyzed areas of eating behavior occur in the group exhibiting the highest fear level and isolation adherence.
- The most positive changes, from the health point of view, occur in the group exhibiting the highest fear level and isolation adherence.
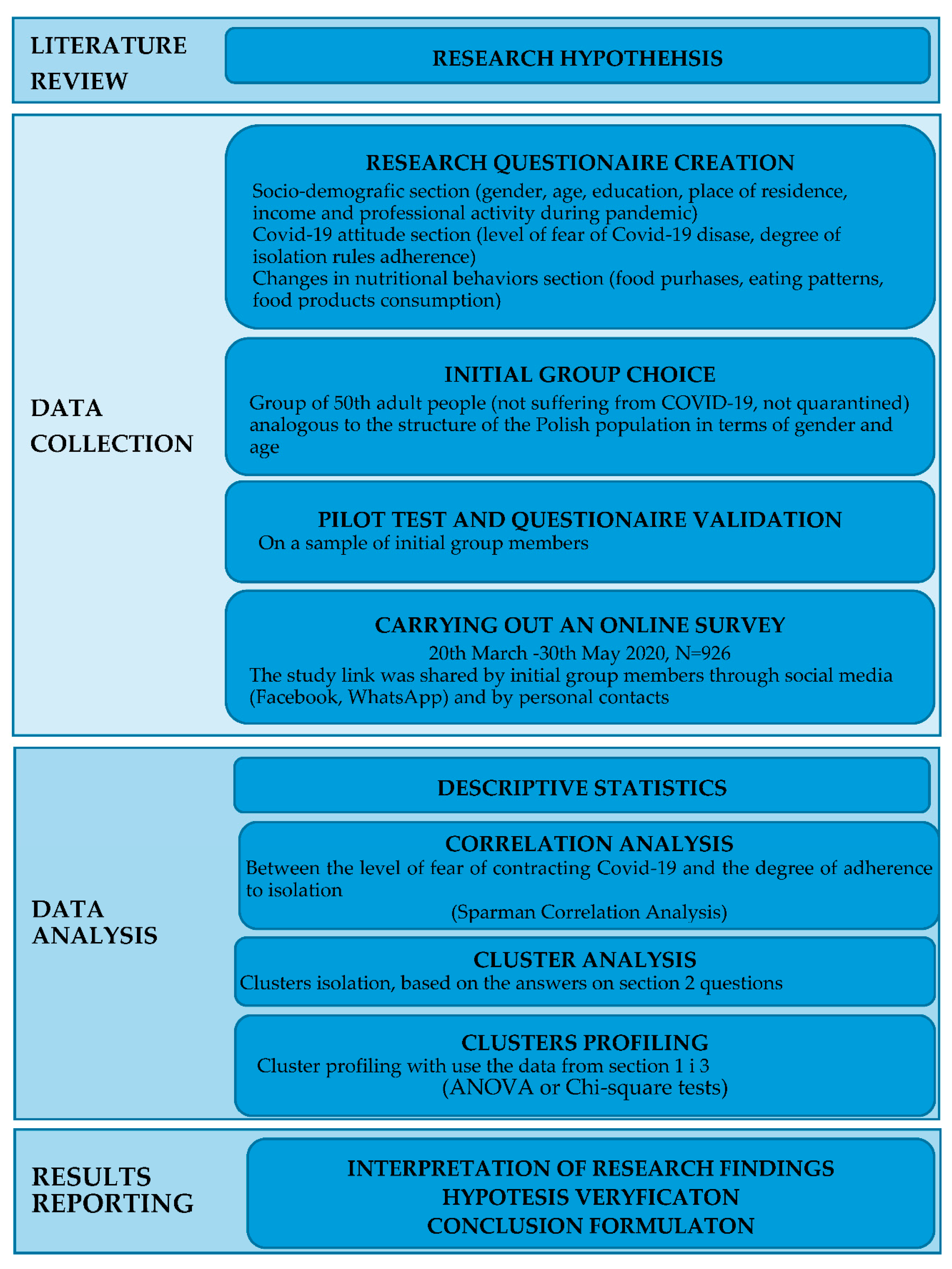
2. Materials and Methods
2.1. Data Collecting
2.2. Research Questionnaire
2.3. Statistical Analysis
3. Results
- Fearing and following the rules (FFR, N = 352, 38%)—persons who are very afraid of getting sick and follow the safety rules most strictly.
- Moderately fearing and following the rules (MFFR, N = 400, 43.2%)—persons who are moderately afraid of getting sick and rather follow the safety rules.
- Not fearing and not following the rules (NFFR, N = 174, 18.8%)—persons who are least afraid of getting sick and rather or do not follow the rules (Table 1).
3.1. Socio-Demographic and Economic Characteristics of the Study Population and Isolated Clusters
3.2. Changes in Food Purchases
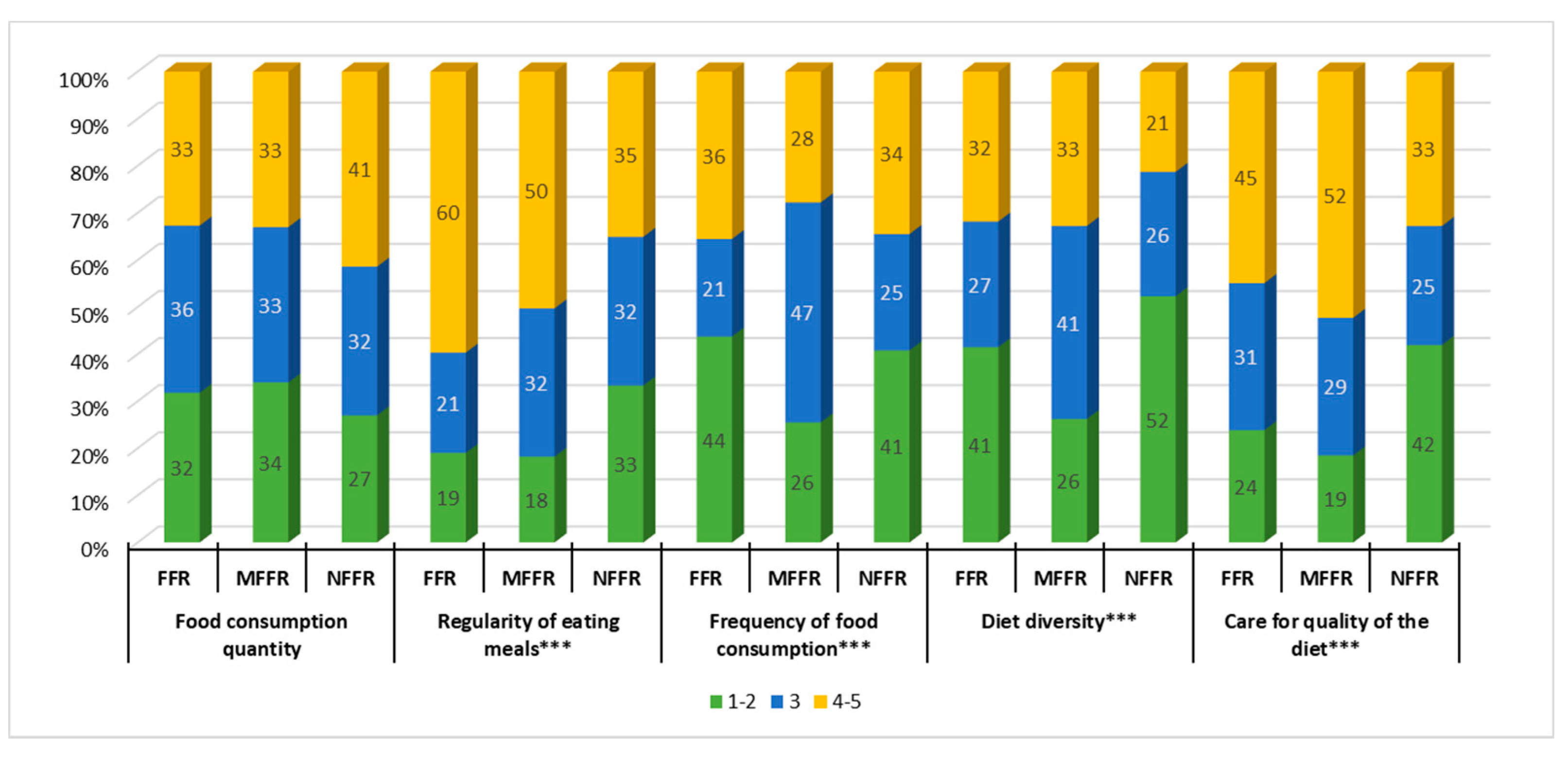
3.3. Changes in Eating Patterns
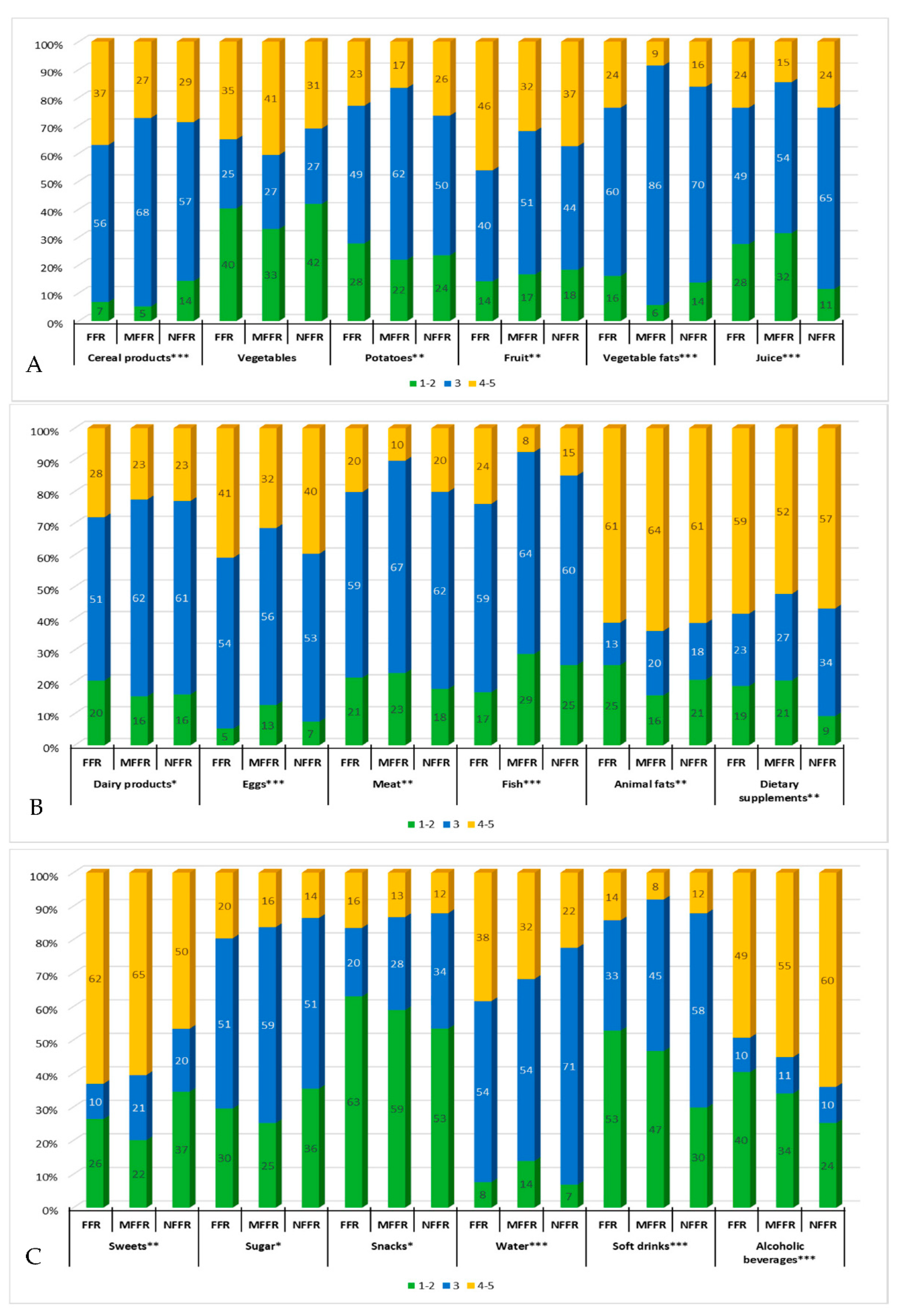
3.4. Changes in the Level of Food Product Consumption
4. Discussion
5. Limitations and Further Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Asmundson, G.J.; Taylor, S. Coronaphobia: Fear and the 2019-nCoV outbreak. J. Anxiety Disord. 2020, 70, 102196. [Google Scholar] [CrossRef]
- Mertens, G.; Gerritsen, L.; Duijndam, S.; Salemink, E.; Engelhard, I.M. Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. J. Anxiety Disord. 2020, 74, 102258. [Google Scholar] [CrossRef]
- Naja, F.; Hamadeh, R. Nutrition amid the COVID-19 pandemic: A multi-level framework for action. Eur. J. Clin. Nutr. 2020, 74, 1117–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cybulska, A.; Pankowski, K. Życie Codzienne w Czasach Zarazy—Komunikat z Badań. Available online: https://www.cbos.pl/SPISKOM.POL/2020/K_060_20.PDF (accessed on 22 January 2021).
- Chopra, S.; Ranjan, P.; Singh, V.; Kumar, S.; Arora, M.; Hasan, M.S.; Kasiraj, R.; Suryansh; Kaur, D.; Vikram, N.K.; et al. Impact of COVID-19 on lifestyle-related behaviours- a cross-sectional audit of responses from nine hundred and ninety-five participants from India. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 2021–2030. [Google Scholar] [CrossRef]
- Cunningham-Rundles, S.; McNeeley, D.F.; Moon, A. Mechanisms of nutrient modulation of the immune response. J. Allergy Clin. Immunol. 2005, 115, 1119–1128. [Google Scholar] [CrossRef]
- Ramos, R.V.; Martínez-Carrillo, B.E.; Aranda-González, I.I.; Guadarrama, A.L.; Pardo-Morales, R.V.; Tlatempa, P.; Jarillo-Luna, R.A. Diet, exercise and gut mucosal immunity. Proc. Nutr. Soc. 2010, 69, 644–650. [Google Scholar] [CrossRef]
- Gleeson, M.; Nieman, D.C.; Pedersen, B.K. Exercise, nutrition and immune function. J. Sports Sci. 2004, 22, 115–125. [Google Scholar] [CrossRef]
- Amar, S.; Zhou, Q.; Shaik-Dasthagirisaheb, Y.; Leeman, S.E. Diet-induced obesity in mice causes changes in immune responses and bone loss manifested by bacterial challenge. Proc. Natl. Acad. Sci. USA 2007, 104, 20466–20471. [Google Scholar] [CrossRef] [Green Version]
- Greeno, C.G.; Wing, R.R. Stress-induced eating. Psychol. Bull. 1994, 115, 444. [Google Scholar] [CrossRef] [PubMed]
- Stone, A.A.; Brownell, K.D. The stress-eating paradox: Multiple daily measurements in adult males and females. Psychol. Health 1994, 9, 425–436. [Google Scholar] [CrossRef]
- Weinstein, S.E.; Shide, D.J.; Rolls, B.J. Changes in Food Intake in Response to Stress in Men and Women: Psychological Factors. Appetite 1997, 28, 7–18. [Google Scholar] [CrossRef]
- Oliver, G.; Wardle, J.; Gibson, E.L. Stress and Food Choice: A Laboratory Study. Psychosom. Med. 2000, 62, 853–865. [Google Scholar] [CrossRef] [PubMed]
- Macht, M. Characteristics of Eating in Anger, Fear, Sadness and Joy. Appetite 1999, 33, 129–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devonport, T.J.; Nicholls, W.; Fullerton, C. A systematic review of the association between emotions and eating behaviour in normal and overweight adult populations. J. Health Psychol. 2017, 24, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Anton, S.D.; Miller, P.M. Do Negative Emotions Predict Alcohol Consumption, Saturated Fat Intake, and Physical Activity in Older Adults? Behav. Modif. 2005, 29, 677–688. [Google Scholar] [CrossRef] [PubMed]
- Cardi, V.; Leppanen, J.; Treasure, J. The effects of negative and positive mood induction on eating behaviour: A meta-analysis of laboratory studies in the healthy population and eating and weight disorders. Neurosci. Biobehav. Rev. 2015, 57, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T.; Gibson, E.L.; Baños, R.; Cebolla, A.; Winkens, L.H. Is comfort food actually comforting for emotional eaters? A (moderated) mediation analysis. Physiol. Behav. 2019, 211, 112671. [Google Scholar] [CrossRef]
- Jribi, S.; Ben Ismail, H.; Doggui, D.; Debbabi, H. COVID-19 virus outbreak lockdown: What impacts on household food wastage? Environ. Dev. Sustain. 2020, 22, 3939–3955. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.; Park, M.; Hong, K.; Hyun, E. The Impact of an Epidemic Outbreak on Consumer Expenditures:An Empirical Assessment for MERS Korea. Sustainability 2016, 8, 454. [Google Scholar] [CrossRef] [Green Version]
- Durante, K.M.; Laran, J. The Effect of Stress on Consumer Saving and Spending. J. Mark. Res. 2016, 53, 814–828. [Google Scholar] [CrossRef]
- Hobbs, M.; Pearson, N.; Foster, P.J.; Biddle, S.J.H. Sedentary behaviour and diet across the lifespan: An updated systematic review. Br. J. Sports Med. 2014, 49, 1179–1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celik, B.; Dane, S. The effects of COVID-19 Pandemic Outbreak on Food Consumption Preferences and Their Causes. J. Res. Med. Dent. Sci. 2020, 8, 169–173. [Google Scholar]
- Luo, Y.; Chen, L.; Xu, F.; Gao, X.; Han, D.; Na, L. Investigation on knowledge, attitudes, and practices about food safety and nutrition in the Chinese during the epidemic of corona virus disease 2019. Public Health Nutr. 2020, 24, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Pišot, S.; Milovanović, I.; Šimunič, B.; Gentile, A.; Bosnar, K.; Prot, F.; Bianco, A.; Lo Coco, G.; Bartoluci, S.; Katović, D. Maintaining everyday life praxis in the time of COVID-19 pandemic measures (ELP-COVID-19 survey). Eur. J. Public Health 2020, 30, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Zupo, R.; Castellana, F.; Sardone, R.; Sila, A.; Giagulli, V.A.; Triggiani, V.; Cincione, R.I.; Giannelli, G.; De Pergola, G. Preliminary Trajectories in Dietary Behaviors during the COVID-19 Pandemic: A Public Health Call to Action to Face Obesity. Int. J. Environ. Res. Public Health 2020, 17, 7073. [Google Scholar] [CrossRef]
- Liu, N.; Zhang, F.; Wei, C.; Jia, Y.; Shang, Z.; Sun, L.; Wu, L.; Sun, Z.; Zhou, Y.; Wang, Y.; et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Res. 2020, 287, 112921. [Google Scholar] [CrossRef]
- Kendler, K.S.; Thornton, L.M.; Prescott, C.A. Gender Differences in the Rates of Exposure to Stressful Life Events and Sensitivity to Their Depressogenic Effects. Am. J. Psychiatry 2001, 158, 587–593. [Google Scholar] [CrossRef]
- McLean, C.P.; Anderson, E.R. Brave men and timid women? A review of the gender differences in fear and anxiety. Clin. Psychol. Rev. 2009, 29, 496–505. [Google Scholar] [CrossRef]
- Bish, A.; Michie, S. Demographic and attitudinal determinants of protective behaviours during a pandemic: A review. Br. J. Health Psychol. 2010, 15, 797–824. [Google Scholar] [CrossRef] [Green Version]
- Shevlin, M.; McBride, O.; Murphy, J.; Miller, J.G.; Hartman, T.K.; Levita, L.; Mason, L.; Martinez, A.P.; McKay, R.; Stocks, T.V.A. Anxiety, Depression, Traumatic Stress, and COVID-19 Related Anxiety in the UK General Population During the COVID-19 Pandemic. BJPsych Open. 2020, 6, e125. [Google Scholar] [CrossRef]
- Wang, W.; Tang, J.; Wei, F. Updated understanding of the outbreak of 2019 novel coronavirus (2019-nCoV) in Wuhan, China. J. Med. Virol. 2020, 92, 441–447. [Google Scholar] [CrossRef] [Green Version]
- Barendse, W. Should animal fats be back on the table? A critical review of the human health effects of animal fat. Anim. Prod. Sci. 2014, 54, 831–855. [Google Scholar] [CrossRef] [Green Version]
- Trumbo, P.R.; Rivers, C.R. Systematic review of the evidence for an association between sugar-sweetened beverage consumption and risk of obesity. Nutr. Rev. 2014, 72, 566–574. [Google Scholar] [CrossRef] [Green Version]
- Corrao, G.; Bagnardi, V.; Zambon, A.; La Vecchia, C. A meta-analysis of alcohol consumption and the risk of 15 diseases. Prev. Med. 2004, 38, 613–619. [Google Scholar] [CrossRef]
- Parekh, N.; Deierlein, A. Health Behaviors during the COVID-19 Pandemic: Implications for Obesity. Public Health Nutr. 2020, 23, 1–14. [Google Scholar]
- Or, F.; Kim, Y.; Simms, J.; Austin, S.B. Taking Stock of Dietary Supplements’ Harmful Effects on Children, Adolescents, and Young Adults. J. Adolesc. Health 2019, 65, 455–461. [Google Scholar] [CrossRef]
- Balanzá–Martínez, V.; Atienza–Carbonell, B.; Kapczinski, F.; De Boni, R.B. Lifestyle behaviours during the COVID-19–time to connect 2020. Acta Psychiatr. Scand. 2020, 141, 399–400. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Level of Variable | Total | MFR * | FFR * | NFFR * | p-Value | Cramer V |
|---|---|---|---|---|---|---|---|
| n/% | 926/100 | 400/43.2 | 352/38 | 174/18.8 | |||
| Compliance with isolation rules | I definitely follow the rules | 367 | 95/23.8 | 271/77.0 | 1/0.6 | <0.0001 | 0.80 |
| I rather follow the rules | 385 | 303/75.7 | 80/22.7 | 2/1.1 | |||
| I rather or do not follow the rules | 174 | 2/0.5 | 1/0.3 | 171/98.3 | |||
| Fear of getting sick | I am very afraid of getting sick | 373 | 2/0.5 | 350/99.4 | 21/12.1 | <0.0001 | 0.77 |
| I am a bit afraid of getting sick | 431 | 365/91.2 | 1/0.3 | 65/37.4 | |||
| I am not afraid of getting sick | 122 | 33/8.3 | 1/0.3 | 88/50.5 |
| Specification | Total | FFR * | MFFR | NFFR | p |
|---|---|---|---|---|---|
| Gender | |||||
| Woman | 75.05 | 83.52 | 73.25 | 62.07 | <0.0001 |
| Man | 24.95 | 16.48 | 26.75 | 37.93 | |
| Age | |||||
| 18–25 y.o. | 18.79 | 15.63 | 21.00 | 20.11 | <0.0001 |
| 26–35 y.o. | 23.33 | 21.31 | 23.75 | 26.44 | |
| 36–45 y.o. | 18.68 | 23.30 | 14.25 | 19.54 | |
| 46–55 y.o. | 18.79 | 24.43 | 19.00 | 6.90 | |
| 56–65 y.o. | 12.74 | 8.81 | 18.00 | 8.62 | |
| over 65 y.o. | 7.67 | 6.53 | 4.00 | 18.39 | |
| Place of residence | |||||
| Rural area | 20.73 | 19.89 | 17.50 | 29.89 | <0.0001 |
| Town up to 10,000 people | 11.45 | 9.38 | 14.25 | 9.20 | |
| Town between 10,000 and 500,000 people | 19.33 | 16.76 | 20.25 | 22.41 | |
| City over 500,000 people | 48.49 | 53.98 | 48.00 | 38.51 | |
| Income | |||||
| Up to PLN 2000 (448€) ** | 21.16 | 21.03 | 22.25 | 19.96 | <0.0001 |
| PLN 2001–3000 (449–673€) | 30.02 | 22.44 | 35.50 | 34.06 | |
| PLN 3001–4000 (674–897€) | 24.30 | 32.39 | 19.75 | 22.99 | |
| Over PLN 4000 (897€) | 24.52 | 24.16 | 22.50 | 22.99 | |
| Education | |||||
| Primary/vocational | 3.89 | 2.84 | 2.50 | 9.20 | <0.0001 |
| Secondary | 29.27 | 25.28 | 30.75 | 33.91 | |
| Higher | 66.85 | 71.88 | 66.75 | 56.90 | |
| Professional activity during the COVID-19 pandemic | |||||
| I work/study as before (no changes) | 19.55 | 12.50 | 19.25 | 34.48 | <0.0001 |
| I work/study remotely | 35.21 | 36.65 | 40.25 | 20.69 | |
| I partially work/study remotely | 20.41 | 20.17 | 21.25 | 18.97 | |
| I do not work/study during the pandemic | 8.42 | 7.10 | 8.25 | 11.49 | |
| I do not work/study as before (no changes) | 16.41 | 23.58 | 11.00 | 14.37 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kowalczuk, I.; Gębski, J. Impact of Fear of Contracting COVID-19 and Complying with the Rules of Isolation on Nutritional Behaviors of Polish Adults. Int. J. Environ. Res. Public Health 2021, 18, 1631. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041631
Kowalczuk I, Gębski J. Impact of Fear of Contracting COVID-19 and Complying with the Rules of Isolation on Nutritional Behaviors of Polish Adults. International Journal of Environmental Research and Public Health. 2021; 18(4):1631. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041631
Chicago/Turabian StyleKowalczuk, Iwona, and Jerzy Gębski. 2021. "Impact of Fear of Contracting COVID-19 and Complying with the Rules of Isolation on Nutritional Behaviors of Polish Adults" International Journal of Environmental Research and Public Health 18, no. 4: 1631. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041631