
Analyses of Weight/Blood Pressure Changes before and after Tonsillectomy in Adults: A Longitudinal Follow-Up Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
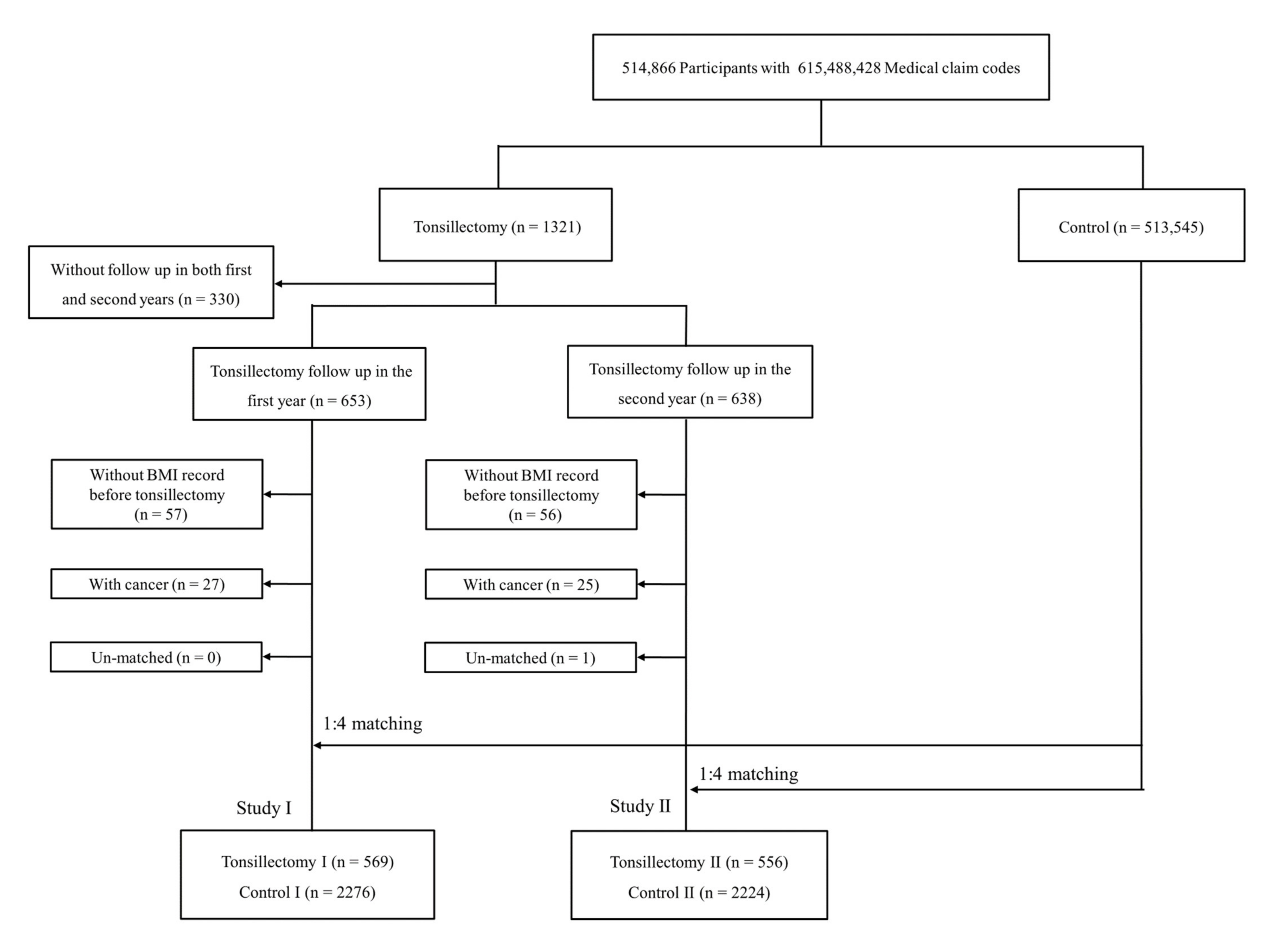
2.1. Study Population
2.2. Definition of Variables
2.3. Covariates
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Erickson, B.K.; Larson, D.R.; Sauver, J.L.S.; Meverden, R.A.; Orvidas, L.J. Changes in incidence and indications of tonsillectomy and adenotonsillectomy, 1970–2005. Otolaryngol. Neck Surg. 2009, 140, 894–901. [Google Scholar] [CrossRef]
- Jeyakumar, A.; Fettman, N.; Armbrecht, E.S.; Mitchell, R. A Systematic Review of Adenotonsillectomy as a Risk Factor for Childhood Obesity. Otolaryngol. Neck Surg. 2011, 144, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Lewis, T.L.; Johnson, R.F.; Choi, J.; Mitchell, R.B. Weight gain after adenotonsillectomy: A case control study. Otolaryngol. Neck Surg. 2015, 152, 734–739. [Google Scholar] [CrossRef]
- Beauchamp, M.T.; Regier, B.; Nzuki, A.; Romine, R.S.; Sweeney, B.; Liu, M.; Davis, A. Weight change before and after adenotonsillectomy in children: An analysis based upon pre-surgery body mass category. Clin. Otolaryngol. 2020, 45, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Rozycki, S.; Gessler, E.M. Posttonsillectomy Weight Loss in Adults. Otolaryngol. Neck Surg. 2015, 152, 1035–1038. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-H.; Kang, K.-T.; Chiu, S.-N.; Chang, I.-S.; Weng, W.-C.; Lee, P.-L.; Hsu, W.-C. Association of Adenotonsillectomy With Blood Pressure Among Hypertensive and Nonhypertensive Children With Obstructive Sleep Apnea. JAMA Otolaryngol. Neck Surg. 2018, 144, 300–307. [Google Scholar] [CrossRef] [Green Version]
- Quante, M.W.R.; Weng, J.; Rosen, C.L.; Amin, R.; Garetz, S.L.; Katz, E.; Paruthi, S.; Arens, R.; Muzumdar, H.; Marcus, C.L.; et al. The effect of adenotonsillectomy for childhood sleep apnea on cardiometabolic measures. Sleep 2015, 38, 1395–1403. [Google Scholar] [PubMed]
- Araújo, M.; Ouayoun, M.; Poirier, J.; Bayle, M.; Vasquez, E.; Fleury, B. Transitory increased blood pressure after upper airway surgery for snoring and sleep apnea correlates with the apnea-hypopnea respiratory disturbance index. Braz. J. Med. Biol. Res. 2003, 36, 1741–1749. [Google Scholar]
- Pang, K.P.; Pang, E.B.; Pang, K.A.; Vicini, C.; Chan, Y.H.; Rotenberg, B.W. Upper airway surgery for obstructive sleep apnea reduces blood pressure. Laryngoscope 2018, 128, 523–527. [Google Scholar] [CrossRef]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Tobacco Smoking and Alcohol Consumption Are Related to Benign Parotid Tumor: A Nested Case-Control Study Using a National Health Screening Cohort. Clin. Exp. Otorhinolaryngol. 2019, 12, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000. [Google Scholar]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Practice of epidemiology: Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Vaiman, M.; Krakovski, D.; Haitov, Z. Oxycodone and Dexamethasone for pain management after tonsillectomy: A placebo-controlled EMG assessed clinical trial. Med. Sci. Monit. 2011, 17, PI25–PI31. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.R.; Helander, E.; Chheda, N.N. Trigeminal Nerve Blockade in the Pterygopalatine Fossa for the Management of Postoperative Pain in Three Adults Undergoing Tonsillectomy: A Proof-of-Concept Report. Pain Med. 2020, 21, 2441–2446. [Google Scholar] [CrossRef] [PubMed]
- Young, T.; Peppard, P.E.; Gottlieb, D.J. Epidemiology of obstructive sleep apnea: A population health perspective. Am. J. Respir. Crit. Care Med. 2002, 165, 1217–1239. [Google Scholar] [CrossRef] [PubMed]
- Phillips, B.G.; Hisel, T.M.; Kato, M.; Pesek, C.A.; Dyken, M.E.; Narkiewicz, K.; Somers, V.K. Recent weight gain in patients with newly diagnosed obstructive sleep apnea. J. Hypertens. 1999, 17, 1297–1300. [Google Scholar] [CrossRef]
- Drager, L.F.; Brunoni, A.R.; Jenner, R.; Lorenzi-Filho, G.; Benseñor, I.M.; Lotufo, P.A. Effects of CPAP on body weight in patients with obstructive sleep apnoea: A meta-analysis of randomised trials. Thorax 2015, 70, 258–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedner, J.; Darpö, B.; Ejnell, H.; Carlson, J.; Caidahl, K. Reduction in sympathetic activity after long-term CPAP treatment in sleep apnoea: Cardiovascular implications. Eur. Respir. J. 1995, 8, 222–229. [Google Scholar] [CrossRef]
- Shechter, A. Effects of continuous positive airway pressure on energy balance regulation: A systematic review. Eur. Respir. J. 2016, 48, 1640–1657. [Google Scholar] [CrossRef]
- Shek, E.W.; Brands, M.W.; Hall, J.E. Chronic Leptin Infusion Increases Arterial Pressure. Hypertension 1998, 31, 409–414. [Google Scholar] [CrossRef] [Green Version]
- Fava, C.; Dorigoni, S.; Dalle Vedove, F.; Danese, E.; Montagnana, M.; Guidi, G.C. Effect of CPAP on blood pressure in patients with OSA/hypopnea: A systematic review and meta-analysis. Chest 2014, 145, 762–771. [Google Scholar] [CrossRef] [PubMed]
- Camacho, M.; Li, D.; Kawai, M.; Zaghi, S.; Teixeira, J.; Senchak, A.J.; Brietzke, S.E.; Frasier, S.; Certal, V. Tonsillectomy for adult obstructive sleep apnea: A systematic review and meta-analysis. Laryngoscope 2016, 126, 2176–2186. [Google Scholar] [CrossRef] [PubMed]
- Pillar, G.; Shehadeh, N. Abdominal Fat and Sleep Apnea: The chicken or the egg? Diabetes Care 2008, 31, S303–S309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbé, F.; Durán-Cantolla, J.; Sánchez-de-la-Torre, M.; Martínez-Alonso, M.; Carmona, C.; Barceló, A. Effect of continuous positive airway pressure on the incidence of hypertension and cardiovascular events in nonsleepy patients with obstructive sleep apnea: A randomized controlled trial. JAMA 2012, 307, 2161–2168. [Google Scholar]


{kind=link}
| Characteristics | Study I | Study II | ||||
|---|---|---|---|---|---|---|
| Tonsillectomy I | Control I | p-Value | Tonsillectomy II | Control II | p-Value | |
| Age (years old, n, %) | 1 | 1 | ||||
| 40–44 | 56 (9.8) | 224 (9.8) | 61 (11.0) | 244 (11.0) | ||
| 45–49 | 167 (29.4) | 668 (29.4) | 161 (29.0) | 644 (29.0) | ||
| 50–54 | 167 (29.4) | 668 (29.4) | 189 (34.0) | 756 (34.0) | ||
| 55–59 | 126 (22.1) | 504 (22.1) | 95 (17.1) | 380 (17.1) | ||
| 60–64 | 38 (6.7) | 152 (6.7) | 36 (6.5) | 144 (6.5) | ||
| 65–69 | 13 (2.3) | 52 (2.3) | 11 (2.0) | 44 (2.0) | ||
| 70–74 | 1 (0.2) | 4 (0.2) | 2 (0.4) | 8 (0.4) | ||
| 75–79 | 1 (0.2) | 4 (0.2) | 1 (0.2) | 4 (0.2) | ||
| Sex (n, %) | 1 | 1 | ||||
| Male | 413 (72.6) | 1652 (72.6) | 409 (73.6) | 1636 (73.6) | ||
| Female | 156 (27.4) | 624 (27.4) | 147 (26.4) | 588 (26.4) | ||
| Income (n, %) | 1 | 1 | ||||
| 1 (lowest) | 47 (8.3) | 188 (8.3) | 47 (8.5) | 188 (8.5) | ||
| 2 | 57 (10.0) | 228 (10.0) | 50 (9.0) | 200 (9.0) | ||
| 3 | 57 (10.0) | 228 (10.0) | 61 (11.0) | 244 (11.0) | ||
| 4 | 115 (20.2) | 460 (20.2) | 115 (20.7) | 460 (20.7) | ||
| 5 (highest) | 293 (51.5) | 1172 (51.5) | 283 (50.9) | 1132 (50.9) | ||
| Region of residence (n, %) | 1 | 1 | ||||
| Urban | 284 (49.9) | 1136 (49.9) | 275 (49.5) | 1100 (49.5) | ||
| Rural | 285 (50.1) | 1140 (50.1) | 281 (50.5) | 1124 (50.5) | ||
| Obesity (n, %) | 1 | 1 | ||||
| Underweight | 3 (0.5) | 12 (0.5) | 2 (0.4) | 8 (0.4) | ||
| Normal | 124 (21.8) | 496 (21.8) | 129 (23.2) | 516 (23.2) | ||
| Overweight | 161 (28.3) | 644 (28.3) | 156 (28.1) | 624 (28.1) | ||
| Obese I | 244 (42.9) | 976 (42.9) | 230 (41.4) | 920 (41.4) | ||
| Obese II | 37 (6.5) | 148 (6.5) | 39 (7.0) | 156 (7.0) | ||
| Smoking status (n, %) | 0.49 | 0.041 1 | ||||
| Nonsmoker | 323 (56.8) | 1296 (56.9) | 327 (58.8) | 1322 (59.4) | ||
| Past smoker | 113 (19.9) | 409 (18.0) | 111 (20.0) | 355 (16.0) | ||
| Current smoker | 133 (23.4) | 571 (25.1) | 118 (21.2) | 547 (24.6) | ||
| Alcohol consumption (n, %) | 0.606 | 0.105 | ||||
| <1 time a week | 344 (60.5) | 1334 (58.6) | 345 (62.1) | 1296 (58.3) | ||
| ≥1 time a week | 225 (39.5) | 942 (41.4) | 211 (38.0) | 928 (41.7) | ||
| Fasting blood glucose (n, %) | 0.958 | 0.957 | ||||
| <100 mg/dL | 361 (63.4) | 1441 (63.3) | 357 (64.2) | 1440 (64.8) | ||
| 100–125 mg/dL | 168 (29.5) | 667 (29.3) | 158 (28.4) | 618 (27.8) | ||
| ≥126 mg/dL | 40 (7.0) | 168 (7.4) | 41 (7.4) | 166 (7.5) | ||
| Total cholesterol (n, %) | 0.282 | 0.372 | ||||
| <200 mg/dL | 301 (52.9) | 1186 (52.1) | 293 (52.7) | 1172 (52.7) | ||
| 200–239 mg/dL | 205 (36.0) | 782 (34.4) | 179 (32.2) | 762 (34.3) | ||
| ≥240 mg/dL | 63 (11.1) | 308 (13.5) | 84 (15.1) | 290 (13.0) | ||
| CCI score (n, %) | 0.047 1 | 0.004 1 | ||||
| 0 | 444 (78.0) | 1875 (82.4) | 427 (76.8) | 1859 (83.6) | ||
| 1 | 92 (16.2) | 314 (13.8) | 97 (17.5) | 280 (12.6) | ||
| 2 | 24 (4.2) | 53 (2.3) | 24 (4.3) | 57 (2.6) | ||
| 3 | 05 (0.9) | 24 (1.1) | 6 (1.1) | 19 (0.9) | ||
| ≥4 | 4 (0.7) | 10 (0.4) | 2 (0.4) | 9 (0.4) | ||
| Systolic blood pressure (mean, SD) 2 | 125.38 ± 13.95 | 125.45 ± 15.37 | 0.93 | 125.49 ± 14.80 | 125.61 ± 15.84 | 0.869 |
| Diastolic blood pressure (mean, SD) 2 | 79.68 ± 10.54 | 79.02 ± 10.53 | 0.181 | 79.41 ± 10.79 | 79.41 ± 10.71 | 0.995 |
| Characteristics | Tonsillectomy I | Control I | Interaction 3 | Linear Mixed Model 5 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Previous (Mean, SD) | Post 1 yr (Mean, SD) | p-Value 1 | Previous (Mean, SD) | Post 1 yr (Mean, SD) | p-Value 1 | p-Value | EV 4 | p-Value 2 | |
| Total participants (n = 2845) | |||||||||
| BMI | 25.14 ± 3.03 | 25.08 ± 2.98 | 0.198 | 25.05 ± 3.05 | 24.99 ± 2.99 | 0.047 1 | 0.732 | 0.070 | 0.609 |
| SBP | 125.38 ± 13.95 | 123.85 ± 13.87 | 0.017 1 | 125.45 ± 15.37 | 125.30 ± 15.08 | 0.647 | 0.344 | −0.808 | 0.064 |
| DBP | 79.68 ± 10.54 | 78.50 ± 10.19 | 0.018 1 | 79.02 ± 10.53 | 78.65 ± 10.16 | 0.096 | 0.826 | 0.687 | 0.022 2 |
| Age <50 years old, men (n = 905) | |||||||||
| BMI | 25.08 ± 2.86 | 25.19 ± 2.81 | 0.224 | 24.91 ± 2.75 | 24.95 ± 2.74 | 0.331 | 0.252 | 0.147 | 0.513 |
| SBP | 126.45 ± 13.50 | 124.75 ± 13.62 | 0.103 | 125.27 ± 14.94 | 125.08 ± 14.44 | 0.736 | 0.734 | −0.684 | 0.345 |
| DBP | 81.80 ± 10.19 | 80.20 ± 10.09 | 0.059 | 80.04 ± 10.76 | 79.63 ± 10.41 | 0.315 | 0.621 | 1.039 | 0.048 2 |
| Age < 50 years old, women (n = 210) | |||||||||
| BMI | 24.08 ± 3.32 | 23.99 ± 3.41 | 0.715 | 24.06 ± 3.45 | 24.06 ± 3.44 | 0.944 | 0.715 | −0.005 | 0.993 |
| SBP | 120.05 ± 11.93 | 120.38 ± 13.49 | 0.881 | 120.33 ± 16.16 | 118.80 ± 16.01 | 0.186 | 0.355 | −1.069 | 0.510 |
| DBP | 75.50 ± 9.35 | 75.05 ± 8.59 | 0.756 | 74.80 ± 10.36 | 74.30 ± 10.62 | 0.539 | 0.536 | 0.752 | 0.497 |
| Age ≥50 years old, men (n = 1160) | |||||||||
| BMI | 25.55 ± 2.95 | 25.38 ± 2.86 | 0.035 1 | 25.44 ± 3.12 | 25.30 ± 2.95 | 0.008 1 | 0.952 | 0.092 | 0.668 |
| SBP | 126.55 ± 14.13 | 124.52 ± 13.26 | 0.061 | 127.23 ± 14.35 | 127.25 ± 14.65 | 0.965 | 0.066 | −0.900 | 0.172 |
| DBP | 80.28 ± 10.82 | 79.44 ± 9.95 | 0.324 | 80.15 ± 9.88 | 79.74 ± 9.84 | 0.239 | 0.312 | 0.525 | 0.260 |
| Age ≥50 years old, women (n = 570) | |||||||||
| BMI | 24.80 ± 3.23 | 24.67 ± 3.21 | 0.302 | 24.83 ± 3.09 | 24.77 ± 3.16 | 0.377 | 0.881 | −0.005 | 0.986 |
| SBP | 123.29 ± 14.43 | 122.32 ± 15.41 | 0.503 | 124.00 ± 17.13 | 124.09 ± 15.77 | 0.901 | 0.783 | −0.633 | 0.564 |
| DBP | 76.61 ± 9.87 | 75.17 ± 10.39 | 0.160 | 76.65 ± 10.76 | 76.46 ± 9.44 | 0.698 | 0.374 | 0.292 | 0.672 |
| Characteristics | Tonsillectomy II | Control II | Interaction 3 | Linear Mixed Model 5 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Previous (Mean, SD) | Post 2 yr (Mean, SD) | p-Value 1 | Previous (Mean, SD) | Post 2 yr (Mean, SD) | p-Value 1 | p-Value | EV 4 | p-Value 2 | |
| Total participants (n = 2780) | |||||||||
| BMI | 25.14 ± 3.04 | 25.21 ± 3.06 | 0.238 | 25.05 ± 3.02 | 25.03 ± 3.07 | 0.378 | 0.128 | 0.039 | 0.783 |
| SBP | 125.49 ± 14.80 | 123.81 ± 13.95 | 0.012 1 | 125.61 ± 15.84 | 125.32 ± 14.57 | 0.388 | 0.559 | −0.184 | 0.681 |
| DBP | 79.41 ± 10.79 | 77.76 ± 10.08 | 0.001 1 | 79.41 ± 10.71 | 78.72 ± 10.13 | 0.005 1 | 0.524 | −0.180 | 0.561 |
| Age <50 years old, men (n = 890) | |||||||||
| BMI | 25.42 ± 2.78 | 25.45 ± 2.68 | 0.778 | 25.41 ± 2.93 | 25.36 ± 3.00 | 0.338 | 0.506 | −0.047 | 0.840 |
| SBP | 125.97 ± 13.62 | 124.81 ± 14.59 | 0.318 | 125.87 ± 15.27 | 125.19 ± 13.73 | 0.231 | 0.852 | −0.297 | 0.685 |
| DBP | 80.97 ± 9.76 | 79.70 ± 10.75 | 0.144 | 80.62 ± 10.30 | 79.69 ± 9.82 | 0.024 1 | 0.911 | 0.355 | 0.488 |
| Age <50 years old, women (n = 220) | |||||||||
| BMI | 23.72 ± 2.98 | 23.90 ± 2.91 | 0.410 | 23.88 ± 3.11 | 24.02 ± 3.16 | 0.103 | 0.802 | −0.165 | 0.743 |
| SBP | 117.02 ± 14.18 | 118.41 ± 16.70 | 0.523 | 118.19 ± 15.51 | 119.72 ± 14.51 | 0.189 | 0.925 | −1.217 | 0.410 |
| DBP | 74.00 ± 11.14 | 74.34 ± 9.82 | 0.827 | 73.84 ± 10.70 | 74.47 ± 9.30 | 0.441 | 0.831 | 0.828 | 0.411 |
| Age ≥50 years old, men (n = 1155) | |||||||||
| BMI | 25.26 ± 2.94 | 25.32 ± 2.95 | 0.518 | 25.12 ± 2.87 | 25.06 ± 2.92 | 0.112 | 0.275 | 0.116 | 0.582 |
| SBP | 126.99 ± 14.34 | 124.15 ± 13.30 | 0.008 1 | 127.06 ± 14.99 | 126.81 ± 14.26 | 0.625 | 0.361 | 0.030 | 0.965 |
| DBP | 80.21 ± 10.74 | 77.77 ± 9.52 | 0.003 1 | 80.29 ± 10.74 | 79.59 ± 9.95 | 0.072 | 0.516 | −0.015 | 0.976 |
| Age ≥50 years old, women (n = 515) | |||||||||
| BMI | 24.98 ± 3.55 | 25.11 ± 3.80 | 0.445 | 24.78 ± 3.33 | 24.82 ± 3.37 | 0.558 | 0.557 | 0.065 | 0.860 |
| SBP | 124.92 ± 16.86 | 123.64 ± 12.61 | 0.418 | 125.09 ± 17.81 | 124.59 ± 16.06 | 0.581 | 0.929 | 0.181 | 0.874 |
| DBP | 77.26 ± 11.55 | 75.83 ± 9.57 | 0.237 | 77.74 ± 10.42 | 76.92 ± 10.69 | 0.161 | 0.819 | −0.402 | 0.586 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wee, J.H.; Min, C.; Yoo, D.M.; Park, M.W.; Song, C.M.; Park, B.; Choi, H.G. Analyses of Weight/Blood Pressure Changes before and after Tonsillectomy in Adults: A Longitudinal Follow-Up Study. Int. J. Environ. Res. Public Health 2021, 18, 1948. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041948
Wee JH, Min C, Yoo DM, Park MW, Song CM, Park B, Choi HG. Analyses of Weight/Blood Pressure Changes before and after Tonsillectomy in Adults: A Longitudinal Follow-Up Study. International Journal of Environmental Research and Public Health. 2021; 18(4):1948. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041948
Chicago/Turabian StyleWee, Jee Hye, Chanyang Min, Dae Myoung Yoo, Min Woo Park, Chang Myeon Song, Bumjung Park, and Hyo Geun Choi. 2021. "Analyses of Weight/Blood Pressure Changes before and after Tonsillectomy in Adults: A Longitudinal Follow-Up Study" International Journal of Environmental Research and Public Health 18, no. 4: 1948. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041948