
Low COVID-19 Vaccine Acceptance Is Correlated with Conspiracy Beliefs among University Students in Jordan

 ,
, 
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Overview of Survey Items
2.3. Measures
2.3.1. Intention to Get COVID-19 Vaccines
2.3.2. Assessment of COVID-19 Vaccine Conspiracy Beliefs
2.3.3. Covariates in Multinomial Regression Analysis
2.3.4. Vaccine Conspiracy Beliefs Scale (VCBS)
2.3.5. Intention to Get COVID-19 Vaccines in Relation to VCBS
2.4. Ethical Considerations
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Survey Respondents
3.2. Low Intent to Get COVID-19 Vaccines among the Respondent Students
3.3. Low Acceptance of Influenza Vaccines among the Respondent Students
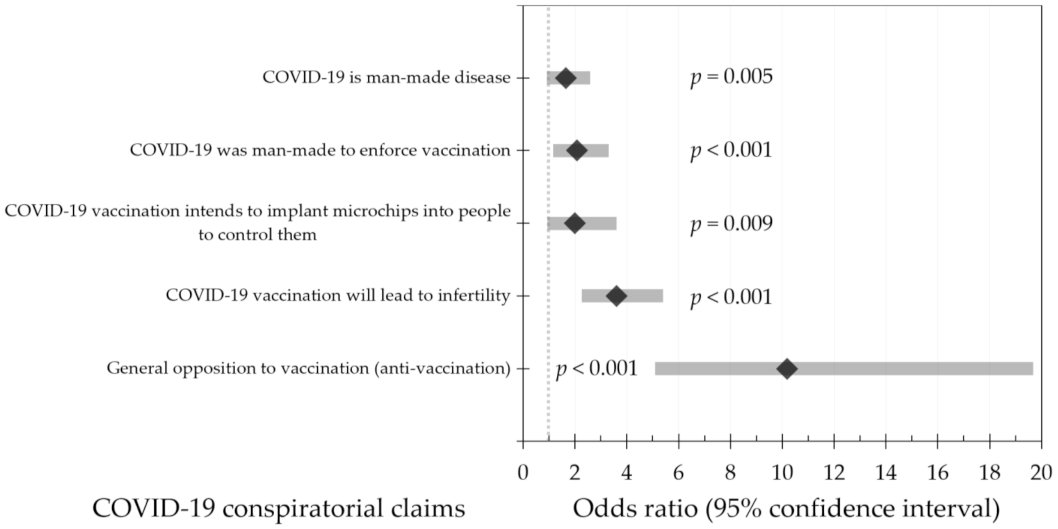
3.4. The Belief in Conspiratorial Claims Was Associated with Lower COVID-19 Vaccine Acceptance
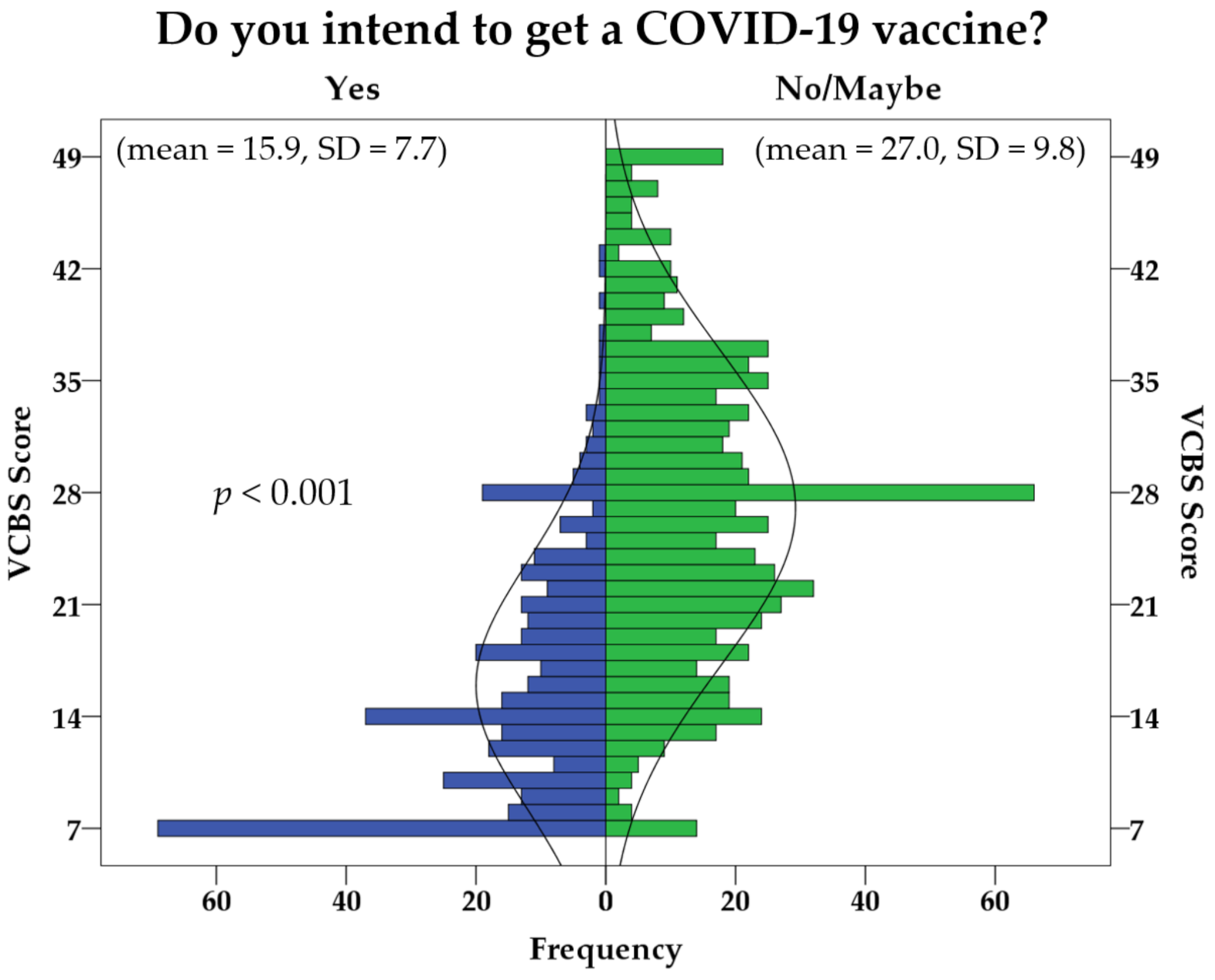
3.5. Vaccine Conspiracy Beliefs Were Associated with a Significantly Higher Level of COVID-19 Vaccine Hesitancy
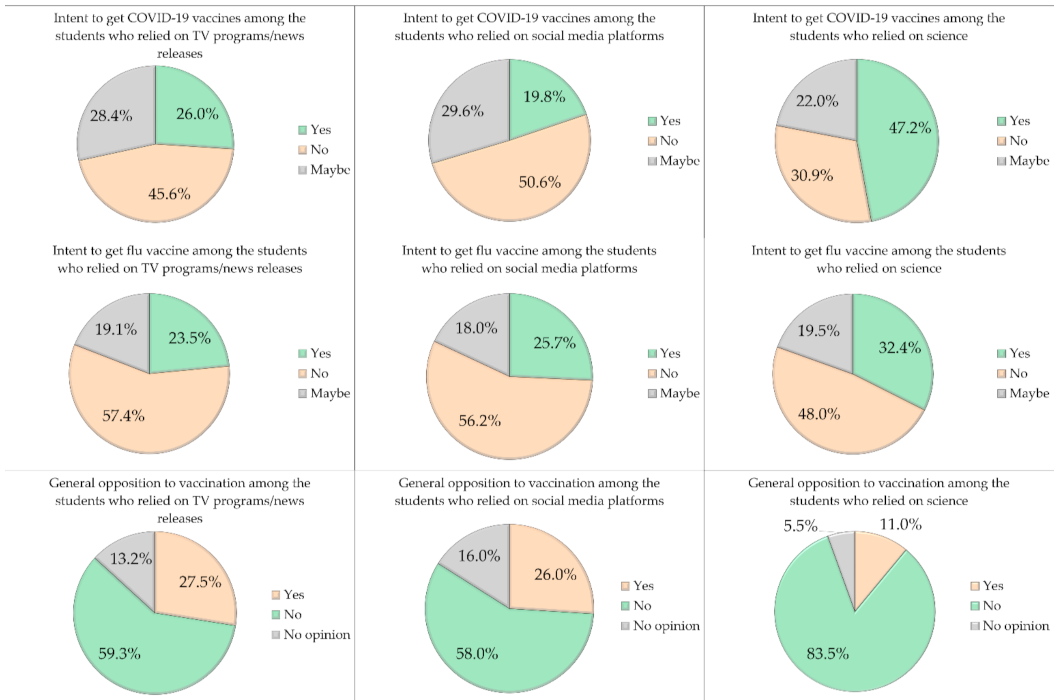
3.6. Dependence on Social Media Platforms Was Associated with COVID-19 Vaccine Hesitancy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gates, B. Responding to Covid-19—A Once-in-a-Century Pandemic? N. Engl. J. Med. 2020, 382, 1677–1679. [Google Scholar] [CrossRef] [PubMed]
- Worldometer. COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 26 January 2021).
- Kissler, S.M.; Tedijanto, C.; Goldstein, E.; Grad, Y.H.; Lipsitch, M. Projecting the transmission dynamics of SARS-CoV-2 through the postpandemic period. Science 2020, 368, 860–868. [Google Scholar] [CrossRef]
- Reperant, L.A.; Osterhaus, A. COVID-19: Losing battles or winning the war? One Health Outlook 2020, 2, 9. [Google Scholar] [CrossRef]
- Rawat, K.; Kumari, P.; Saha, L. COVID-19 vaccine: A recent update in pipeline vaccines, their design and development strategies. Eur. J. Pharmacol. 2021, 892, 173751. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2020, 384, 403–416. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, Y.; Huang, B.; Deng, W.; Quan, Y.; Wang, W.; Xu, W.; Zhao, Y.; Li, N.; Zhang, J.; et al. Development of an Inactivated Vaccine Candidate, BBIBP-CorV, with Potent Protection against SARS-CoV-2. Cell 2020, 182, 713–721.e719. [Google Scholar] [CrossRef] [PubMed]
- Marco, V. COVID-19 vaccines: The pandemic will not end overnight. Lancet Microbe 2020, 2. [Google Scholar] [CrossRef]
- Mellet, J.; Pepper, M.S. A COVID-19 Vaccine: Big Strides Come with Big Challenges. Vaccines 2021, 9, 39. [Google Scholar] [CrossRef]
- Korber, B.; Fischer, W.M.; Gnanakaran, S.; Yoon, H.; Theiler, J.; Abfalterer, W.; Hengartner, N.; Giorgi, E.E.; Bhattacharya, T.; Foley, B.; et al. Tracking Changes in SARS-CoV-2 Spike: Evidence that D614G Increases Infectivity of the COVID-19 Virus. Cell 2020, 182, 812–827.e819. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Wu, C.; Li, X.; Song, Y.; Yao, X.; Wu, X.; Duan, Y.; Zhang, H.; Wang, Y.; Qian, Z. On the origin and continuing evolution of SARS-CoV-2. Natl. Sci. Rev. 2020, 7, 1012–1023. [Google Scholar] [CrossRef] [Green Version]
- Leung, K.; Shum, M.H.; Leung, G.M.; Lam, T.T.; Wu, J.T. Early transmissibility assessment of the N501Y mutant strains of SARS-CoV-2 in the United Kingdom, October to November 2020. Eurosurveillance 2021, 26, 2002106. [Google Scholar] [CrossRef]
- Su, Y.C.; Anderson, D.E.; Young, B.E.; Zhu, F.; Linster, M.; Kalimuddin, S.; Low, J.G.; Yan, Z.; Jayakumar, J.; Sun, L.; et al. Discovery of a 382-nt deletion during the early evolution of SARS-CoV-2. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Sallam, M.; Ababneh, N.A.; Dababseh, D.; Bakri, F.G.; Mahafzah, A. Temporal increase in D614G mutation of SARS-CoV-2 in the Middle East and North Africa. Heliyon 2021, 7, e06035. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Alley, S.J.; Stanton, R.; Browne, M.; To, Q.G.; Khalesi, S.; Williams, S.L.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. As the Pandemic Progresses, How Does Willingness to Vaccinate against COVID-19 Evolve? Int. J. Environ. Res. Public Health 2021, 18, 797. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Grech, V.; Gauci, C. Vaccine hesitancy in the University of Malta Faculties of Health Sciences, Dentistry and Medicine vis-a-vis influenza and novel COVID-19 vaccination. Early Hum. Dev. 2020. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Salali, G.D.; Uysal, M.S. COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psychol. Med. 2020, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Groenewoud, R.; Rachor, G.S.; Asmundson, G.J.G. A Proactive Approach for Managing COVID-19: The Importance of Understanding the Motivational Roots of Vaccination Hesitancy for SARS-CoV2. Front. Psychol. 2020, 11, 575950. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.C.; Dubey, V. Addressing vaccine hesitancy: Clinical guidance for primary care physicians working with parents. Can. Fam. Physician Med. Fam. Can. 2019, 65, 175–181. [Google Scholar]
- MacDonald, N.E.; Hesitancy, S.W.G.o.V. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Watel, P.; Larson, H.J.; Ward, J.K.; Schulz, W.S.; Verger, P. Vaccine hesitancy: Clarifying a theoretical framework for an ambiguous notion. PLoS Curr. 2015, 7. [Google Scholar] [CrossRef]
- de Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Bohm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, A.; Robinson, K.; Vallee-Tourangeau, G. The 5As: A practical taxonomy for the determinants of vaccine uptake. Vaccine 2016, 34, 1018–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgaertner, B.; Ridenhour, B.J.; Justwan, F.; Carlisle, J.E.; Miller, C.R. Risk of disease and willingness to vaccinate in the United States: A population-based survey. PLoS Med. 2020, 17, e1003354. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.T.; Hanage, W.P.; Owusu-Boaitey, N.; Cochran, K.B.; Walsh, S.P.; Meyerowitz-Katz, G. Assessing the age specificity of infection fatality rates for COVID-19: Systematic review, meta-analysis, and public policy implications. Eur. J. Epidemiol. 2020, 35, 1123–1138. [Google Scholar] [CrossRef] [PubMed]
- Zarocostas, J. How to fight an infodemic. Lancet 2020, 395, 676. [Google Scholar] [CrossRef]
- Stein, R.A.; Ometa, O.; Pachtman Shetty, S.; Katz, A.; Popitiu, M.I.; Brotherton, R. Conspiracy theories in the era of COVID-19: A tale of two pandemics. Int. J. Clin. Pract. 2021, 75, e13778. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Taim, D.; Eid, H.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. COVID-19 misinformation: Mere harmless delusions or much more? A knowledge and attitude cross-sectional study among the general public residing in Jordan. PLoS ONE 2020, 15, e0243264. [Google Scholar] [CrossRef] [PubMed]
- Ball, P.; Maxmen, A. The epic battle against coronavirus misinformation and conspiracy theories. Nature 2020, 581, 371–374. [Google Scholar] [CrossRef]
- Uscinski, J.E.; Enders, A.M.; Klofstad, C.; Seelig, M.; Funchion, J.; Everett, C.; Wuchty, S.; Premaratne, K.; Murthi, M. Why do people believe COVID-19 conspiracy theories? Harv. Kennedy Sch. Misinformation Rev. 2020, 1. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. Conspiracy Beliefs Are Associated with Lower Knowledge and Higher Anxiety Levels Regarding COVID-19 among Students at the University of Jordan. Int. J. Environ. Res. Public Health 2020, 17, 4915. [Google Scholar] [CrossRef]
- Larson, H.J. The biggest pandemic risk? Viral misinformation. Nature 2018, 562, 309–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Depoux, A.; Martin, S.; Karafillakis, E.; Preet, R.; Wilder-Smith, A.; Larson, H. The pandemic of social media panic travels faster than the COVID-19 outbreak. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jolley, D.; Douglas, K.M. The effects of anti-vaccine conspiracy theories on vaccination intentions. PLoS ONE 2014, 9, e89177. [Google Scholar] [CrossRef]
- Ministry of Higher Education & Scientific Research. J. Statistics. Available online: http://mohe.gov.jo/en/pages/Statistics.aspx (accessed on 4 January 2021).
- Checkmarket. Sample Size Calculator. Available online: https://www.checkmarket.com/ (accessed on 4 January 2021).
- Shapiro, G.K.; Holding, A.; Perez, S.; Amsel, R.; Rosberger, Z. Validation of the vaccine conspiracy beliefs scale. Papillomavirus Res. 2016, 2, 167–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Mulukom, V.; Pummerer, L.J.; Alper, S.; Bai, H.M.; Čavojová, V.; Farias, J.; Kay, C.S.; Lazarevic, L.B.; Lobato, E.J.C.; Marinthe, G. Antecedents and consequences of COVID-19 conspiracy beliefs: A rapid review of the evidence. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Andrade, G. Medical conspiracy theories: Cognitive science and implications for ethics. Med. Health Care Philos. 2020, 23, 505–518. [Google Scholar] [CrossRef]
- Patrinely, J.R., Jr.; Zakria, D.; Berkowitz, S.T.; Johnson, D.B.; Totten, D.J. COVID-19: The Emerging Role of Medical Student Involvement. Med Sci. Educ. 2020, 1–3. [Google Scholar] [CrossRef]
- Remy, V.; Zollner, Y.; Heckmann, U. Vaccination: The cornerstone of an efficient healthcare system. J. Mark. Access Health Policy 2015, 3. [Google Scholar] [CrossRef] [Green Version]
- Vyas, D.; Galal, S.M.; Rogan, E.L.; Boyce, E.G. Training Students to Address Vaccine Hesitancy and/or Refusal. Am. J. Pharm. Educ. 2018, 82, 6338. [Google Scholar] [CrossRef]
- Duggan, M.; Brenner, J. The Demographics of Social Media Users. 2012. Available online: https://www.pewresearch.org/internet/2013/02/14/the-demographics-of-social-media-users-2012/ (accessed on 26 January 2021).
- Caserotti, M.; Girardi, P.; Rubaltelli, E.; Tasso, A.; Lotto, L.; Gavaruzzi, T. Associations of COVID-19 risk perception with vaccine hesitancy over time for Italian residents. Soc. Sci. Med. 2021, 272, 113688. [Google Scholar] [CrossRef] [PubMed]
- Domnich, A.; Cambiaggi, M.; Vasco, A.; Maraniello, L.; Ansaldi, F.; Baldo, V.; Bonanni, P.; Calabro, G.E.; Costantino, C.; de Waure, C.; et al. Attitudes and Beliefs on Influenza Vaccination during the COVID-19 Pandemic: Results from a Representative Italian Survey. Vaccines 2020, 8, 711. [Google Scholar] [CrossRef]
- Department of Statistics Jordan. Estimated Population of the Kingdom by Sex, Age Group and Sex Ratio 2004–2019. Available online: http://dosweb.dos.gov.jo/ (accessed on 19 February 2021).
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 vaccine hesitancy among medical students. J. Public Health 2020. [Google Scholar] [CrossRef]
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 2020, 35, 781–783. [Google Scholar] [CrossRef]
- Naeem, S.B.; Bhatti, R. The Covid-19 ‘infodemic’: A new front for information professionals. Health Inf. Libr. J. 2020, 37, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Marco-Franco, J.E.; Pita-Barros, P.; Vivas-Orts, D.; González-de-Julián, S.; Vivas-Consuelo, D. COVID-19, Fake News, and Vaccines: Should Regulation Be Implemented? Int. J. Environ. Res. Public Health 2021, 18, 744. [Google Scholar] [CrossRef]
- Wardle, C.; Singerman, E. Too little, too late: Social media companies’ failure to tackle vaccine misinformation poses a real threat. BMJ 2021, 372, n26. [Google Scholar] [CrossRef] [PubMed]
- Rosselli, R.; Martini, M.; Bragazzi, N.L. The old and the new: Vaccine hesitancy in the era of the Web 2.0. Challenges and opportunities. J. Prev. Med. Hyg. 2016, 57, E47–E50. [Google Scholar] [PubMed]
- Karlsson, L.C.; Soveri, A.; Lewandowsky, S.; Karlsson, L.; Karlsson, H.; Nolvi, S.; Karukivi, M.; Lindfelt, M.; Antfolk, J. Fearing the disease or the vaccine: The case of COVID-19. Personal. Individ. Differ. 2021, 172, 110590. [Google Scholar] [CrossRef]
- Salmon, D.A.; Dudley, M.Z.; Glanz, J.M.; Omer, S.B. Vaccine hesitancy: Causes, consequences, and a call to action. Vaccine 2015, 33 (Suppl. 4), D66–D71. [Google Scholar] [CrossRef]
- The Lancet. COVID-19 vaccines: No time for complacency. Lancet 2020, 396, 1607. [Google Scholar] [CrossRef]
- Larson, H.J.; Clarke, R.M.; Jarrett, C.; Eckersberger, E.; Levine, Z.; Schulz, W.S.; Paterson, P. Measuring trust in vaccination: A systematic review. Human Vaccines Immunother. 2018, 14, 1599–1609. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Academic Discipline | School/Faculty | School/Faculty | School/Faculty |
|---|---|---|---|---|
| Feature | Health n 2 (%) | Scientific n (%) | Humanities n (%) | |
| Mean age (SD 1) | 20.8 (2.7) | 22.5 (4.4) | 23.9 (6.6) | |
| Age categories | ≤21 years | 473 (75.3) | 136 (49.6) | 97 (47.5) |
| >21 years | 155 (24.7) | 138 (50.4) | 107 (52.5) | |
| Nationality | Jordanian | 471 (75.0) | 253 (92.3) | 188 (92.2) |
| Non-Jordanian | 157 (25.0) | 21 (7.7) | 16 (7.8) | |
| University | Public | 582 (92.7) | 249 (90.9) | 149 (73.0) |
| Private | 46 (7.3) | 25 (9.1) | 55 (27.0) | |
| Sex | Male | 168 (26.8) | 82 (29.9) | 54 (26.5) |
| Female | 460 (73.2) | 192 (70.1) | 150 (73.5) | |
| Educational level | Undergraduate | 596 (94.9) | 225 (82.1) | 149 (73.0) |
| Postgraduate | 32 (5.1) | 49 (17.9) | 55 (27.0) | |
| History of chronic disease | Yes | 57 (9.1) | 28 (10.2) | 20 (9.8) |
| No | 571 (90.9) | 246 (89.8) | 184 (90.2) | |
| Experience of COVID-19 in self or family | Yes | 252 (40.1) | 103 (37.6) | 69 (33.8) |
| No | 376 (59.9) | 171 (62.4) | 135 (66.2) |
| Variable | Feature | Intent for COVID-19 Vaccination | p-Value 3 | |
|---|---|---|---|---|
| Yes | No/Maybe | |||
| n2 (%) | n (%) | |||
| Mean age (SD 1) | 21.4 (3.6) | 21.9 (4.6) | 0.215 | |
| Age categories | ≤21 years | 256 (36.3) | 450 (63.7) | 0.207 |
| >21 years | 130 (32.5) | 270 (67.5) | ||
| Nationality | Jordanian | 289 (31.7) | 623 (68.3) | <0.001 ** |
| Non-Jordanian | 97 (50.0) | 97 (50.0) | ||
| University | Public | 359 (36.6) | 621 (63.4) | 0.001 ** |
| Private | 27 (21.4) | 99 (78.6) | ||
| School/Faculty | Health | 273 (43.5) | 355 (56.5) | <0.001 ** |
| Scientific | 64 (23.4) | 210 (76.6) | ||
| Humanities | 49 (24.0) | 155 (76.0) | ||
| Sex | Male | 128 (42.1) | 176 (57.9) | 0.002 ** |
| Female | 258 (32.2) | 544 (67.8) | ||
| Educational level | Undergraduate | 339 (34.9) | 631 (65.1) | 0.929 |
| Postgraduate | 47 (34.6) | 89 (65.4) | ||
| History of chronic disease | Yes | 35 (33.3) | 70 (66.7) | 0.723 |
| No | 351 (35.1) | 650 (64.9) | ||
| Experience of COVID-19 in self or family | Yes | 150 (35.4) | 274 (64.6) | 0.793 |
| No | 236 (34.6) | 446 (65.4) | ||
| Variable | Feature | Acceptance of Influenza Vaccination | p-Value 3 | |
|---|---|---|---|---|
| Yes | No/Maybe | |||
| n2 (%) | n (%) | |||
| Mean age (SD 1) | 21.2 (3.5) | 21.9 (4.6) | 0.033 * | |
| Age categories | ≤21 years | 219 (31.0) | 487 (69.0) | 0.027 * |
| >21 years | 99 (24.8) | 301 (75.3) | ||
| Nationality | Jordanian | 249 (27.3) | 663 (72.7) | 0.021 * |
| Non-Jordanian | 69 (35.6) | 125 (64.4) | ||
| University | Public | 287 (29.3) | 693 (70.7) | 0.274 |
| Private | 31 (24.6) | 95 (75.4) | ||
| School/Faculty | Health | 212 (33.8) | 416 (66.2) | <0.001 ** |
| Scientific | 56 (20.4) | 218 (79.6) | ||
| Humanities | 50 (24.5) | 154 (75.5) | ||
| Sex | Male | 95 (31.3) | 209 (68.8) | 0.259 |
| Female | 223 (27.8) | 579 (72.2) | ||
| Educational level | Undergraduate | 285 (29.4) | 685 (70.6) | 0.217 |
| Postgraduate | 33 (24.3) | 103 (75.7) | ||
| History of chronic disease | Yes | 40 (38.1) | 65 (61.9) | 0.026 * |
| No | 278 (27.8) | 723 (72.2) | ||
| Experience of COVID-19 in self or family | Yes | 136 (32.1) | 288 (67.9) | 0.054 |
| No | 182 (26.7) | 500 (73.3) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sallam, M.; Dababseh, D.; Eid, H.; Hasan, H.; Taim, D.; Al-Mahzoum, K.; Al-Haidar, A.; Yaseen, A.; Ababneh, N.A.; Assaf, A.; et al. Low COVID-19 Vaccine Acceptance Is Correlated with Conspiracy Beliefs among University Students in Jordan. Int. J. Environ. Res. Public Health 2021, 18, 2407. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052407
Sallam M, Dababseh D, Eid H, Hasan H, Taim D, Al-Mahzoum K, Al-Haidar A, Yaseen A, Ababneh NA, Assaf A, et al. Low COVID-19 Vaccine Acceptance Is Correlated with Conspiracy Beliefs among University Students in Jordan. International Journal of Environmental Research and Public Health. 2021; 18(5):2407. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052407
Chicago/Turabian StyleSallam, Malik, Deema Dababseh, Huda Eid, Hanan Hasan, Duaa Taim, Kholoud Al-Mahzoum, Ayat Al-Haidar, Alaa Yaseen, Nidaa A. Ababneh, Areej Assaf, and et al. 2021. "Low COVID-19 Vaccine Acceptance Is Correlated with Conspiracy Beliefs among University Students in Jordan" International Journal of Environmental Research and Public Health 18, no. 5: 2407. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052407