
Effect of the Information Support Robot on the Daily Activity of Older People Living Alone in Actual Living Environment

 , , ,
, , ,
Abstract
:1. Introduction
Related Work
2. Materials and Methods
2.1. Subjects
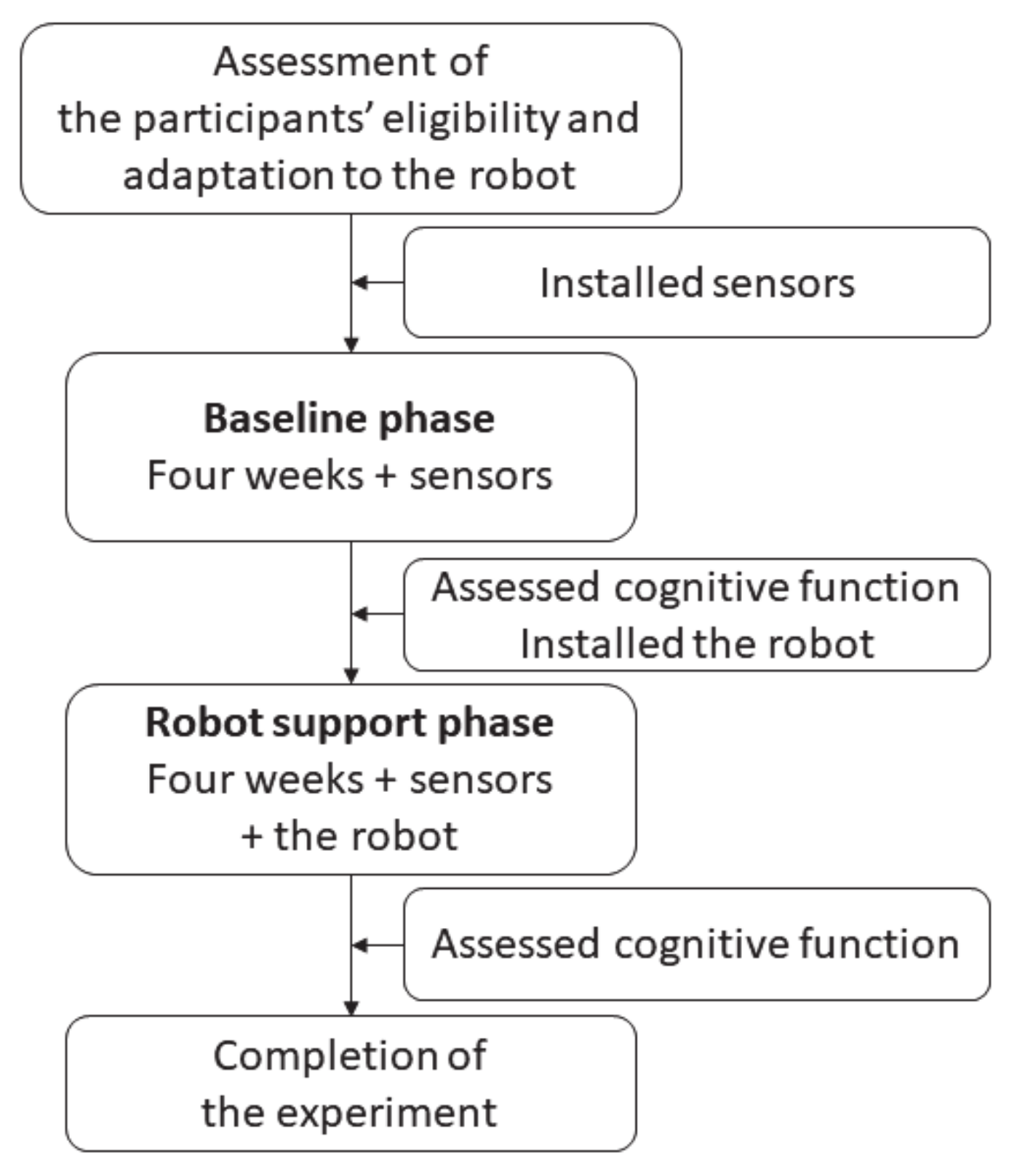
2.2. Procedure
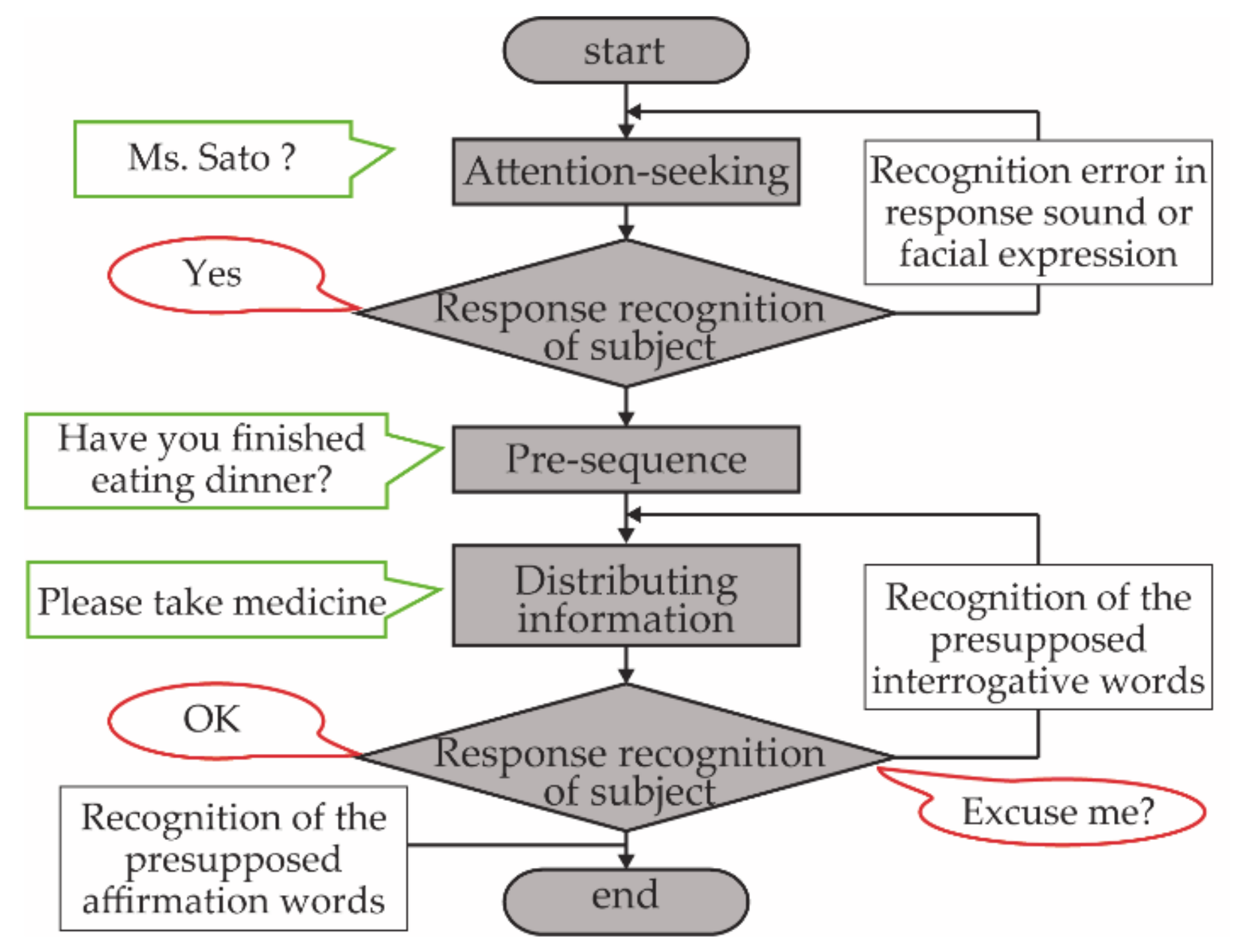
2.3. Information Support Robot
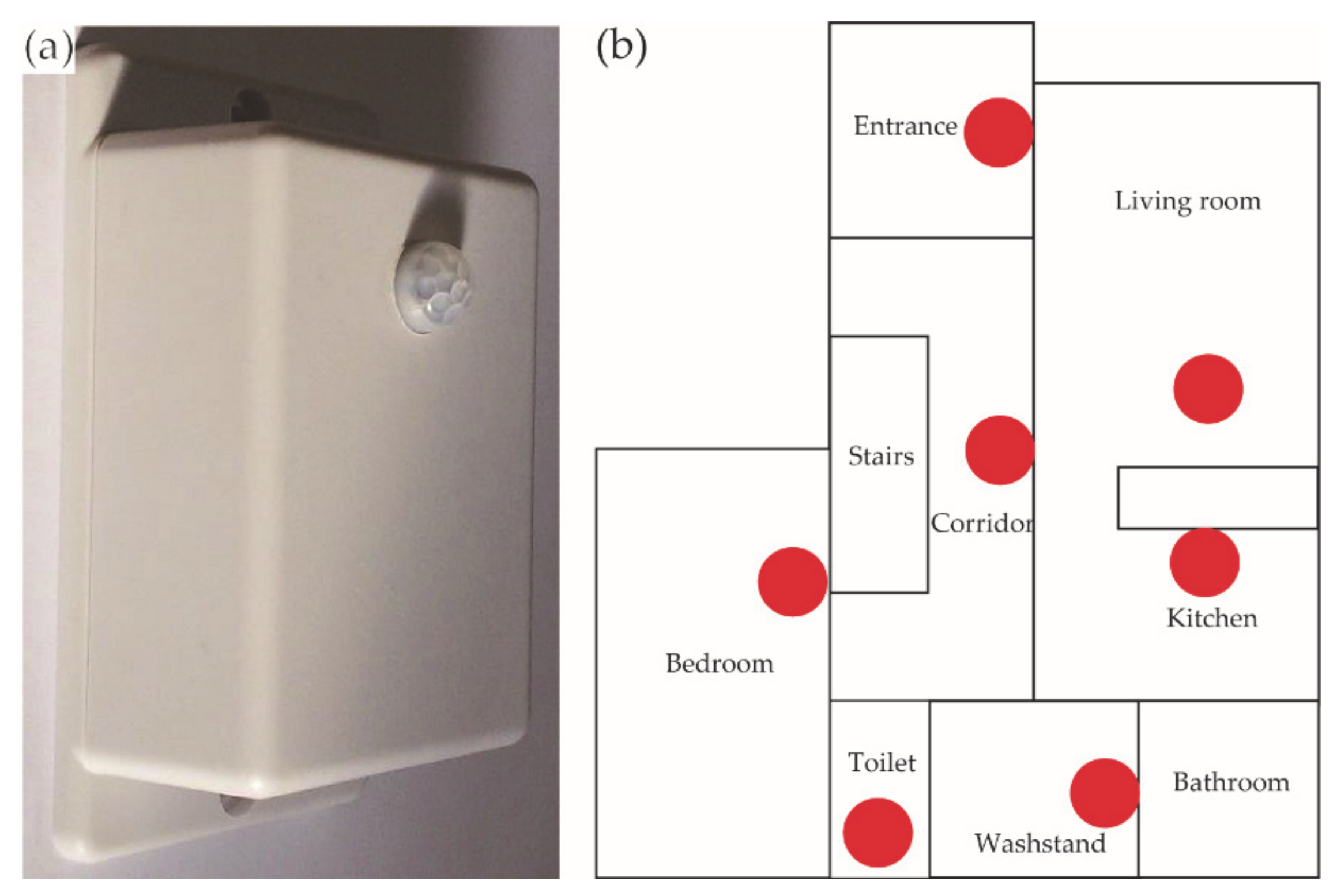
2.4. Measures
2.5. Statistical Analyses
3. Results
3.1. Subjects’ Cognitive Characteristics
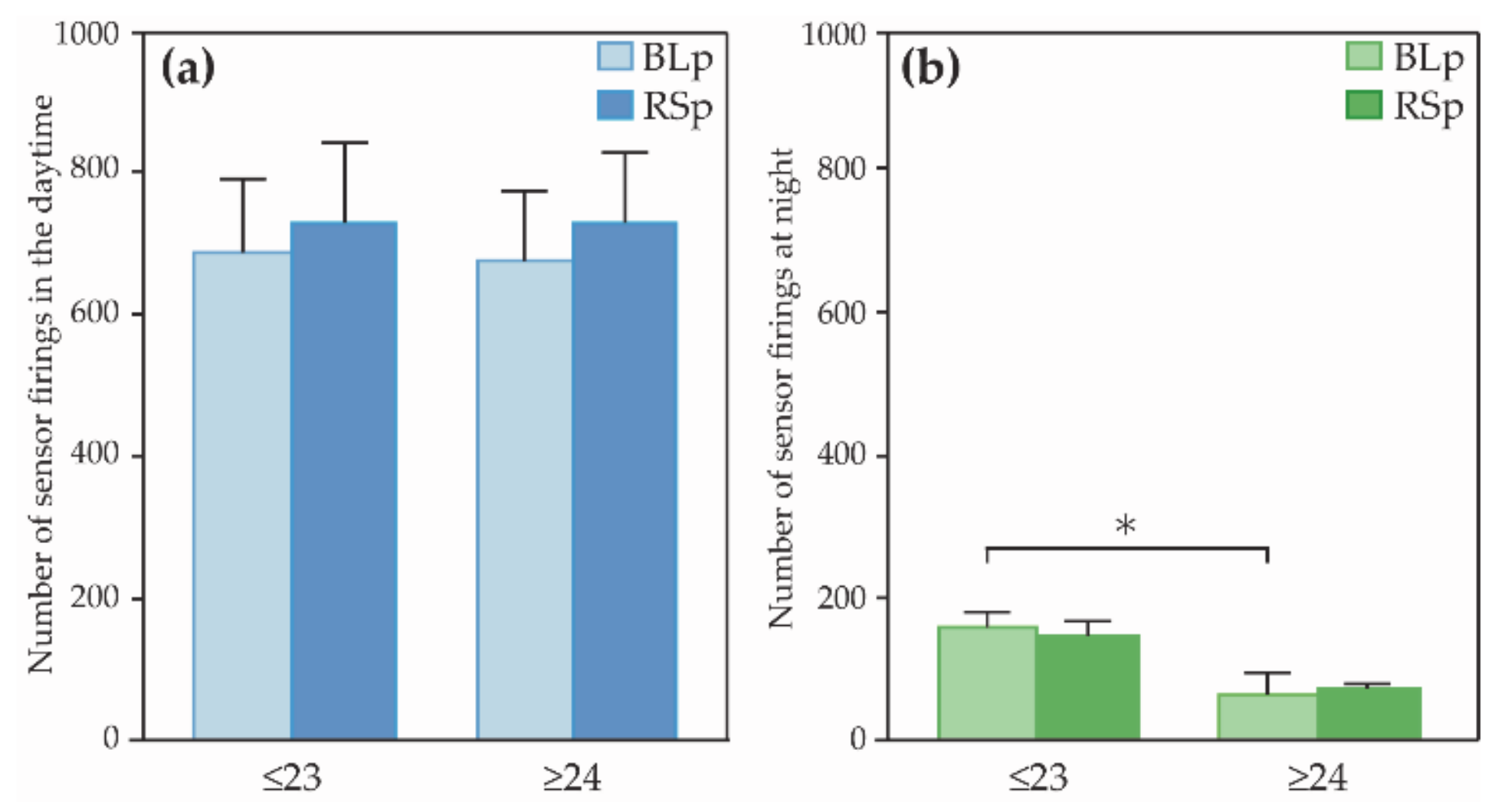
3.2. Comparison of the Indices of Daily Activities
4. Discussion
Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cabinet Office Annual Report on the Ageing Society. 2018. Available online: https://www8.cao.go.jp/kourei/english/annualreport/2018/pdf/c1-1.pdf (accessed on 11 September 2019).
- Kalpa, K.; Steve, I.; Danielle, H.; Cameron, S.; Gerhard, G.; Andreas, S.E. Health risk appraisal in older people 1: Are older people living alone an “at-risk” group? Br. J. Gen. Pract. 2007, 57, 271–276. [Google Scholar]
- Evans, I.E.M.; Llewellyn, D.J.; Matthews, F.E.; Woods, R.T.; Brayne, C.; Clare, L. Living alone and cognitive function in later life. Arch. Gerontol. Geriatr. 2019, 81, 222–233. [Google Scholar] [CrossRef]
- Honjo, K.; Tani, Y.; Saito, M.; Sasaki, Y.; Kondo, K.; Kawachi, I.; Kondo, N. Living Alone or With Others and Depressive Symptoms, and Effect Modification by Residential Social Cohesion Among Older Adults in Japan: The JAGES Longitudinal Study. J. Epidemiol. 2018, 28, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Jeong, S.; Cho, S.I. Effects of living alone versus with others and of housemate type on smoking, drinking, dietary habits, and physical activity among elderly people. Epidemiol. Health 2017, 39, e2017034. [Google Scholar] [CrossRef] [PubMed]
- Bei, B.; Wiley, J.F.; Trinder, J.; Manber, R. Beyond the mean: A systematic review on the correlates of daily intraindividual variability of sleep/wake patterns. Sleep Med. Rev. 2016, 28, 108–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korchut, A.; Szklener, S.; Abdelnour, C.; Tantinya, N.; Hernández-Farigola, J.; Ribes, J.C.; Skrobas, U.; Grabowska-Aleksandrowicz, K.; Szczesniak-Stanczyk, D.; Rejdak, K. Challenges for service robots-requirements of elderly adults with cognitive impairments. Front. Neurol. 2017, 8, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Kachouie, R.; Sedighadeli, S.; Khosla, R.; Chu, M.T. Socially Assistive Robots in Elderly Care: A Mixed-Method Systematic Literature Review. Int. J. Hum. Comput. Interact. 2014, 30, 369–393. [Google Scholar] [CrossRef]
- Inoue, T.; Nihei, M.; Narita, T.; Onoda, M.; Ishiwata, R.; Mamiya, I.; Shino, M.; Kojima, H.; Ohnaka, S.; Fujita, Y.; et al. Field-based development of an information support robot for persons with dementia. Technol. Disabil. 2012, 24, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Van Der Heide, L.A.; Willems, C.G.; Spreeuwenberg, M.D.; Rietman, J.; De Witte, L.P. Implementation of CareTV in care for the elderly: The effects on feelings of loneliness and safety and future challenges. Technol. Disabil. 2012, 24, 283–291. [Google Scholar] [CrossRef]
- Perälä, S.; Mäkelä, K.; Salmenaho, A.; Latvala, R. Technology for Elderly with Memory Impairment and Wandering Risk. E-Health Telecommun. Syst. Netw. 2013, 2, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Blom, M.M.; Zarit, S.H.; Groot Zwaaftink, R.B.M.; Cuijpers, P.; Pot, A.M. Effectiveness of an internet intervention for family caregivers of people with dementia: Results of a randomized controlled trial. PLoS ONE 2015, 10, e0116622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, M.; Ishii, A.; Yamano, E.; Ogikubo, H.; Okazaki, M.; Kamimura, K.; Konishi, Y.; Emoto, S.; Watanabe, Y. Effect of a human-type communication robot on cognitive function in elderly women living alone. Med. Sci. Monit. 2012, 18, CR550–CR557. [Google Scholar] [CrossRef] [Green Version]
- Tapus, A.; Tapus, C.; Mataric, M. Music Therapist Robot: A Solution for Helping People with Cognitive Impairments. In Proceedings of the IJCAI Workshop on Intelligent Systems for Assisted Cognition, Pasadena, CA, USA, 11–17 July 2009; pp. 297–298. [Google Scholar] [CrossRef]
- Wada, K.; Shibata, T. Social and physiological influences of living with seal robots in an elderly care house for two months. Gerontechnology 2009, 7, 235. [Google Scholar] [CrossRef] [Green Version]
- Robinson, H.; Macdonald, B.; Broadbent, E. Physiological effects of a companion robot on blood pressure of older people in residential care facility: A pilot study. Australas. J. Ageing 2015, 34, 27–32. [Google Scholar] [CrossRef]
- Demange, M.; Lenoir, H.; Pino, M.; Cantegreil-Kallen, I.; Rigaud, A.S.; Cristancho-Lacroix, V. Improving well-being in patients with major neurodegenerative disorders: Differential efficacy of brief social robot-based intervention for 3 neuropsychiatric profiles. Clin. Interv. Aging 2018, 13, 1303–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sefcik, J.S.; Johnson, M.J.; Yim, M.; Lau, T.; Vivio, N.; Mucchiani, C.; Cacchione, P.Z. Stakeholders’ Perceptions Sought to Inform the Development of a Low-Cost Mobile Robot for Older Adults: A Qualitative Descriptive Study. Clin. Nurs. Res. 2018, 27, 61–80. [Google Scholar] [CrossRef] [PubMed]
- Monk, T.H.; Reynolds, C.F.; Buysse, D.J.; DeGrazia, J.M.; Kupfer, D.J. The relationship between lifestyle regularity and subjective sleep quality. Chronobiol. Int. 2003, 20, 97–107. [Google Scholar] [CrossRef]
- Manber, R.; Bootzin, R.R.; Acebo, C.; Carskadon, M.A. The effects of regularizing sleep-wake schedules on daytime sleepiness. Sleep 1996, 19, 432–441. [Google Scholar] [CrossRef] [Green Version]
- Zisberg, A.; Gur-Yaish, N.; Shochat, T. Contribution of routine to sleep quality in community elderly. Sleep 2010, 33, 509–514. [Google Scholar] [CrossRef] [Green Version]
- Naylor, E.; Penev, P.D.; Orbeta, L.; Janssen, I.; Ortiz, R.; Colecchia, E.F.; Keng, M.; Finkel, S.; Zee, P.C. Daily social and physical activity increases slow-wave sleep and daytime neuropsychological performance in the elderly. Sleep 2000, 23, 87–95. [Google Scholar] [CrossRef]
- Foley, D.J.; Monjan, A.A.; Brown, S.L.; Simonsick, E.M.; Wallace, R.B.; Blazer, D.G. Sleep complaints among elderly persons: An epidemiologic study of three communities. Sleep 1995, 18, 425–432. [Google Scholar] [CrossRef]
- Bemelmans, R.; Gelderblom, G.J.; Jonker, P.; de Witte, L. Socially assistive robots in elderly care: A systematic review into effects and effectiveness. J. Am. Med. Dir. Assoc. 2012, 13, 114–120.e1. [Google Scholar] [CrossRef]
- Ienca, M.; Fabrice, J.; Elger, B.; Caon, M.; Pappagallo, A.S.; Kressig, R.W.; Wangmo, T. Intelligent Assistive Technology for Alzheimer’s Disease and Other Dementias: A Systematic Review. J. Alzheimer’s Dis. 2017, 56, 1301–1340. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.H.; Wrobel, J.; Cornuet, M.; Kerhervé, H.; Damnée, S.; Rrigaud, A.S. Acceptance of an assistive robot in older adults: A mixed-method study of human-robot interaction over a 1-month period in the living lab setting. Clin. Interv. Aging 2014, 9, 801–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thodberg, K.; Sørensen, L.U.; Christensen, J.W.; Poulsen, P.H.; Houbak, B.; Damgaard, V.; Keseler, I.; Edwards, D.; Videbech, P.B. Therapeutic effects of dog visits in nursing homes for the elderly. Psychogeriatrics 2016, 16, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Jøranson, N.; Pedersen, I.; Rokstad, A.M.M.; Ihlebæk, C. Effects on Symptoms of Agitation and Depression in Persons with Dementia Participating in Robot-Assisted Activity: A Cluster-Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2015, 16, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Abdi, J.; Al-Hindawi, A.; Ng, T.; Vizcaychipi, M.P. Scoping review on the use of socially assistive robot technology in elderly care. BMJ Open 2018, 8, e018815. [Google Scholar] [CrossRef] [Green Version]
- Gross, H.-M.; Mueller, S.; Schroeter, C.; Volkhardt, M.; Scheidig, A.; Debes, K.; Richter, K.; Doering, N. Robot companion for domestic health assistance: Implementation, test and case study under everyday conditions in private apartments. In Proceedings of the 2015 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Hamburg, Germany, 28 September–2 October 2015; Volume 2015, pp. 5992–5999. [Google Scholar]
- Broadbent, E.; Peri, K.; Kerse, N.; Jayawardena, C.; Kuo, I.; Datta, C.; MacDonald, B. Robots in older people’s homes to improve medication adherence and quality of life: A randomised cross-over trial. In Proceedings of the International Conference on Social Robotics; Springer: Cham, Switzerland, 2014; Volume 8755, pp. 64–73. [Google Scholar]
- Orejana, J.R.; MacDonald, B.A.; Ahn, H.S.; Peri, K.; Broadbent, E. Healthcare Robots in Homes of Rural Older Adults. In International Conference on Social Robotics; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2015; Volume 9388, pp. 512–521. ISBN 978-3-319-25553-8. [Google Scholar]
- Monk, T.H.; Buysse, D.J.; Potts, J.M.; DeGrazia, J.M.; Kupfer, D.J. Morningness-eveningness and lifestyle regularity. Chronobiol. Int. 2004, 21, 435–443. [Google Scholar] [CrossRef] [PubMed]
- De Joode, E.; Van Heugten, C.; Verhey, F.; Van Boxtel, M. Efficacy and usability of assistive technology for patients with cognitive deficits: A systematic review. Clin. Rehabil. 2010, 24, 701–714. [Google Scholar] [CrossRef]
- Law, M.; Sutherland, C.; Ahn, H.S.; Macdonald, B.A.; Peri, K.; Johanson, D.L.; Vajsakovic, D.S.; Kerse, N.; Broadbent, E. Developing assistive robots for people with mild cognitive impairment and mild dementia: A qualitative study with older adults and experts in aged care. BMJ Open 2019, 9, e031937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zsiga, K.; Tóth, A.; Pilissy, T.; Péter, O.; Dénes, Z.; Fazekas, G. Evaluation of a companion robot based on field tests with single older adults in their homes. Assist. Technol. 2018, 30, 259–266. [Google Scholar] [CrossRef]
- Abdollahi, H.; Mollahosseini, A.; Lane, J.T.; Mahoor, M.H. A pilot study on using an intelligent life-like robot as a companion for elderly individuals with dementia and depression. In Proceedings of the 2017 IEEE-RAS 17th International Conference on Humanoid Robotics (Humanoids), Birmingham, UK, 15–17 November 2017; pp. 541–546. [Google Scholar] [CrossRef] [Green Version]
- Moyle, W.; Jones, C.; Murfield, J.; Thalib, L.; Beattie, E.; Shum, D.; O’Dwyer, S.; Mervin, M.C.; Draper, B. Effect of a robotic seal on the motor activity and sleep patterns of older people with dementia, as measured by wearable technology: A cluster-randomised controlled trial. Maturitas 2018, 110, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Nishiura, Y.; Inoue, T.; Nihei, M. Appropriate talking pattern of an information support robot for people living with dementia: A case study. J. Assist. Technol. 2014, 8, 177–187. [Google Scholar] [CrossRef]
- Sugishita, M.; Hemmi, I. Validity and Reliability of the Min Mental State Examination-Japanese (MMSE-J): A Preliminary Report. Jpn. J. Cogn. Neurosci. 2010, 12, 186–190. [Google Scholar] [CrossRef]
- Matsuda, O.; Saito, M.; Kurokawa, Y.; Miyamoto, N.; Maruyama, K.; Matsuda, H.; Nakatani, M. A study of the reliability and validity of the Japanese version of the Neurobehavioral Cognitive Status Examination (NCSE). Jpn. J. Geriatr. Psychiatry 2001, 12, 1177–1187. [Google Scholar]
- Matsuda, O.; Kumazawa, Y.; Sakuraba, Y.; Matsuda, H.; Nakatani, M.; Saito, M. The development of the Japanese version of the Neurobehavioral Cognitive Status Examination (NCSE), Second Report. Jpn. J. Geriatr. Psychiatry 2003, 14, 475–483. [Google Scholar]
- Tsuruoka, Y.; Takahashi, M.; Suzuki, M.; Sato, K.; Shirayama, Y. Utility of the Neurobehavioral Cognitive Status Examination (COGNISTAT) in differentiating between depressive states in late-life depression and late-onset Alzheimer’s disease: A preliminary study. Ann. Gen. Psychiatry 2016, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- D’Onofrio, G.; Sancarlo, D.; Ricciardi, F.; Panza, F.; Seripa, D.; Cavallo, F.; Giuliani, F.; Greco, A. Information and Communication Technologies for the Activities of Daily Living in Older Patients with Dementia: A Systematic Review. J. Alzheimer’s Dis. 2017, 57, 927–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceolim, M.F.; Menna-Barreto, L. Sleep/wake cycle and physical activity in healthy elderly people. Sleep Res. Online 2000, 3, 87–95. [Google Scholar] [PubMed]
- McKee, G.; Kearney, P.M.; Kenny, R.A. The factors associated with self-reported physical activity in older adults living in the community. Age Ageing 2015, 44, 586–592. [Google Scholar] [CrossRef] [Green Version]
- Van Cauwenberg, J.; De Bourdeaudhuij, I.; De Meester, F.; Van Dyck, D.; Salmon, J.; Clarys, P.; Deforche, B. Relationship between the physical environment and physical activity in older adults: A systematic review. Health Place 2011, 17, 458–469. [Google Scholar] [CrossRef] [PubMed]
- Moschny, A.; Platen, P.; Klaaßen-Mielke, R.; Trampisch, U.; Hinrichs, T. Barriers to Physical Activity Participation in Older Adults. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urwyler, P.; Stucki, R.; Rampa, L.; Müri, R.; Mosimann, U.P.; Nef, T. Cognitive impairment categorized in community-dwelling older adults with and without dementia using in-home sensors that recognise activities of daily living. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Zhu, G.; Zhao, Q.; Guo, Q.; Meng, H.; Hong, Z.; Ding, D. Prevalence and risk factors of poor sleep quality among chinese elderly in an urban community: Results from the Shanghai aging study. PLoS ONE 2013, 8, e0081261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellström, Y.; Persson, G.; Hallberg, I.R. Quality of life and symptoms among older people living at home. J. Adv. Nurs. 2004, 48, 584–593. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Index | Definition |
|---|---|---|
| i | Wake-up time | Last sleep end time before 12:00 |
| ii | Bedtime | First sleep start time after 18:00 |
| iii | Sleep duration | Total time for each sleep from 18:00 on the day to 12:00 on the next day. In the case of the other sensors outside the bedroom fired between sleep periods, it is also considered as sleep if the sleep-to-sleep interval is less than 10 min. |
| iv | Number of sensor firings in the daytime | Number of sensor firings data not during sleep. |
| v | Number of sensor firings at night | Number of sensor firings data during sleep. |
| ≤23 Group (n = 7) | ≥24 Group (n = 7) | Effect Size | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Age a (Range) | 82.1 (76–93) | 83.4 (76–88) | 0.13 x | ||||||
| Intra y | Inter z | ||||||||
| Baseline Phase (BLp) | Robot Support Phase (RSp) | BLp | RSp | ≤23 | ≤24 | BLp | RSp | ||
| Mini-Mental State Examination-Japanese (MMSE-J) a | 19.9 (14–23) | 19.3 (16–22) | 27.7 (24–30) | 28.6 (26–30) | 0.10 | 0.43 | − | − | |
| The Japanese version of the Neurobehavioral Cognitive Status Examination (COGNISTAT) b | Orientation | 6.0 (1.5–8.5) | 5.0 (0.5–8) | 10.0 (9.5–10) | 10.0 (10–10) | 0.00 | 0.00 | 0.68 * | 0.80 * |
| Attention | 6.0 (3–10) | 8.0 (3.75–10) | 8.0 (4.5–10) | 3.0 (1–6.5) | 0.38 | 0.56 | 0.04 | 0.40 | |
| Comprehension | 7.0 (5.5–10) | 7.0 (4.75–7) | 10.0 (10–10) | 10.0 (10–10) | 0.65 | 0.00 | 0.60 | 0.77 * | |
| Repetition | 11.0 (8.5–11) | 9.0 (7–11) | 11.0 (8.5–11) | 11.0 (8.5–11) | 0.17 | 0.22 | 0.06 | 0.17 | |
| Naming | 9.0 (7–9) | 7.0 (7–8.5) | 9.0 (9–10) | 10.0 (9–10) | 0.00 | 0.38 | 0.42 | 0.59 * | |
| Constructional ability | 7.0 (6–8) | 7.0 (7–7.75) | 11.0 (10–11) | 11.0 (10–11) | 0.21 | 0.00 | 0.81 * | 0.79 * | |
| Memory | 7.0 (6–7) | 5.5 (5–6.75) | 9.0 (8.5–10) | 10.0 (8–10) | 0.62 | 0.22 | 0.68 * | 0.78 * | |
| Calculation | 8.0 (5–10) | 7.0 (4–10) | 10.0 (10–10) | 10.0 (10–10) | 0.00 | 0.00 | 0.60 | 0.55 | |
| Similarities | 8.0 (7–9) | 10.0 (9.25–10) | 10.0 (9.5–10.5) | 10.0 (9.5–11) | 0.77 * | 0.22 | 0.59 * | 0.28 | |
| Judgment | 9.0 (9–10.5) | 9.5 (9–10) | 12.0 (10.5–12) | 12.0 (9.5–12) | 0.00 | 0.38 | 0.42 | 0.32 | |
| ≤23 Group | ≥24 Group | |||||
|---|---|---|---|---|---|---|
| BLp | RSp | Effect Size | BLp | RSp | Effect Size | |
| Wake-up time | 6:05 (0:19) | 6:08 (0:19) | 0.13 | 6:13 (0:33) | 5:57 (0:34) | 0.77 * |
| Bedtime | 22:03 (0:25) | 21:53 (0:18) | 0.19 | 21:21 (0:47) | 21:26 (0:45) | 0.32 |
| Sleep duration | 7:52 (0:29) | 7:59 (0:22) | 0.06 | 9:24 (0:59) | 8:38 (0:41) | 0.89 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mizuno, J.; Saito, D.; Sadohara, K.; Nihei, M.; Ohnaka, S.; Suzurikawa, J.; Inoue, T. Effect of the Information Support Robot on the Daily Activity of Older People Living Alone in Actual Living Environment. Int. J. Environ. Res. Public Health 2021, 18, 2498. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052498
Mizuno J, Saito D, Sadohara K, Nihei M, Ohnaka S, Suzurikawa J, Inoue T. Effect of the Information Support Robot on the Daily Activity of Older People Living Alone in Actual Living Environment. International Journal of Environmental Research and Public Health. 2021; 18(5):2498. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052498
Chicago/Turabian StyleMizuno, Jumpei, Daisuke Saito, Ken Sadohara, Misato Nihei, Shinichi Ohnaka, Jun Suzurikawa, and Takenobu Inoue. 2021. "Effect of the Information Support Robot on the Daily Activity of Older People Living Alone in Actual Living Environment" International Journal of Environmental Research and Public Health 18, no. 5: 2498. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052498