
Detecting and Treating Psychosocial and Lifestyle-Related Difficulties in Chronic Disease: Development and Treatment Protocol of the E-GOAL eHealth Care Pathway

 , , , and
, , , and
Abstract
:1. Introduction
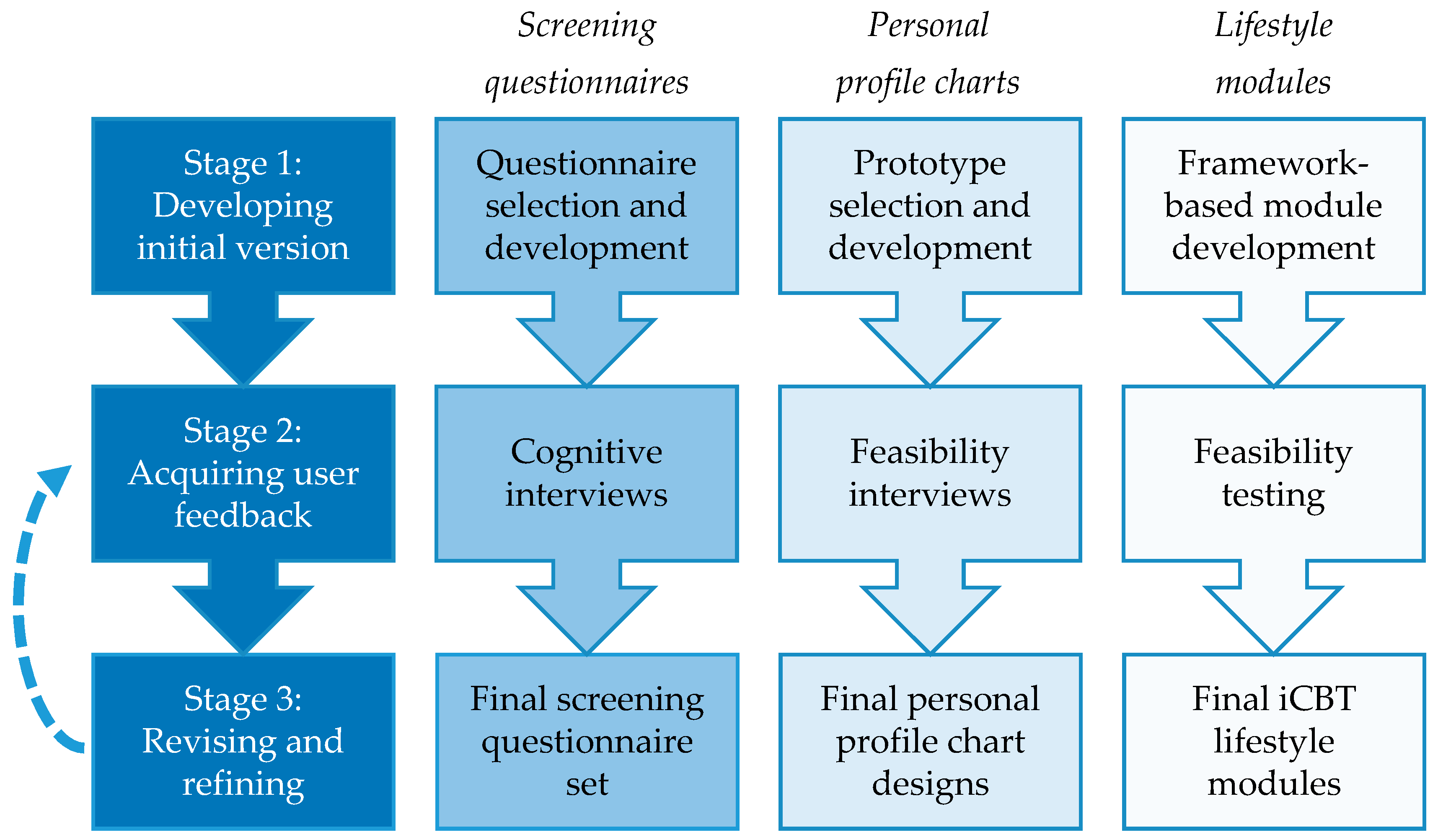
2. Development
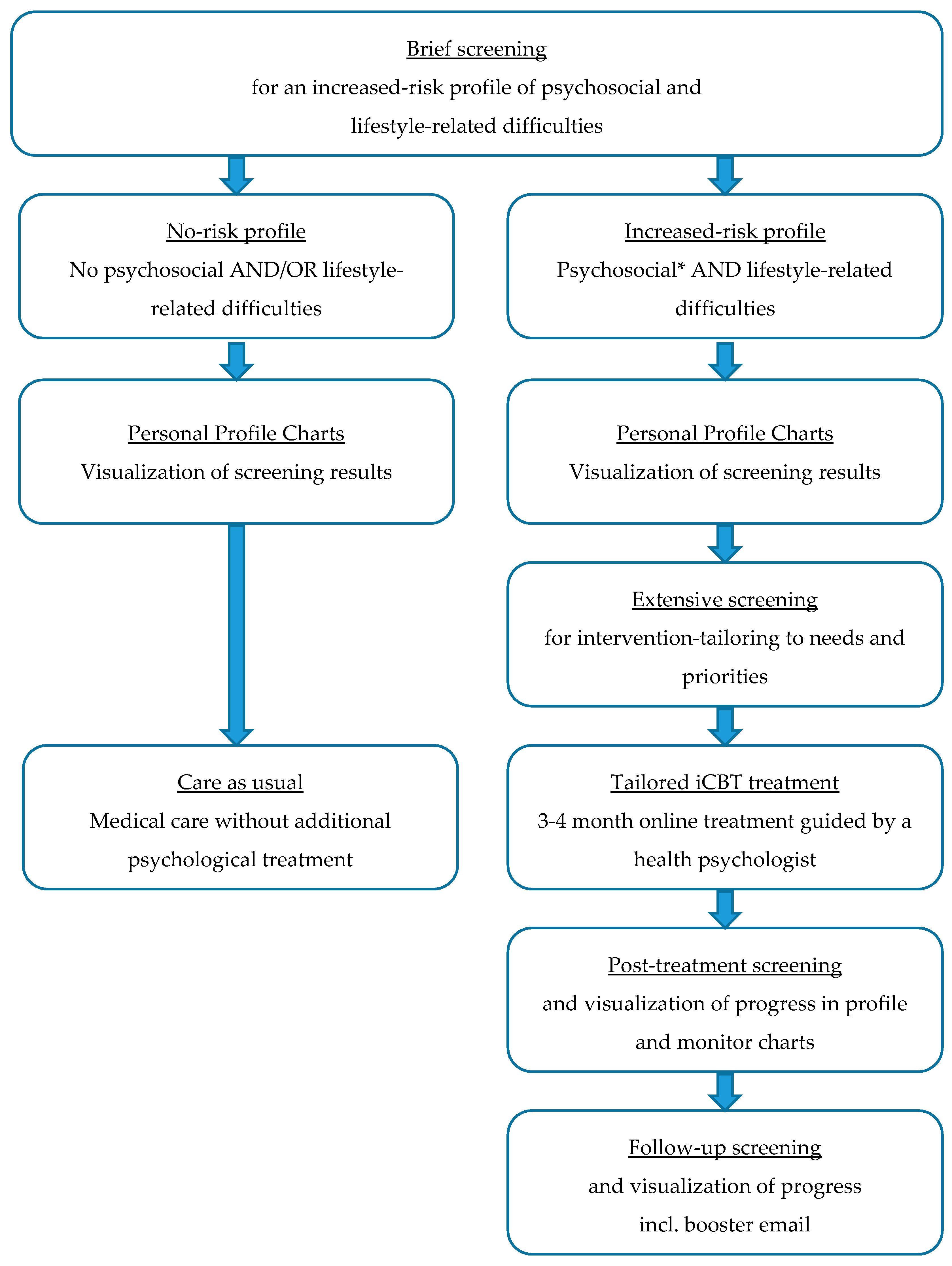
2.1. Screening Tool
2.2. Screening Questionnaires: Increased-Risk Profile Identification and Intervention Tailoring
2.2.1. Development Screening Questionnaires Stage 1: Developing Initial Version
Part 1: Questionnaires for Increased-Risk Profile Identification
Part 2: Questionnaires for Intervention-Tailoring
2.2.2. Development Screening Questionnaires Stage 2: Acquiring User Feedback
2.2.3. Development Screening Questionnaires Stage 3: Revising and Refining
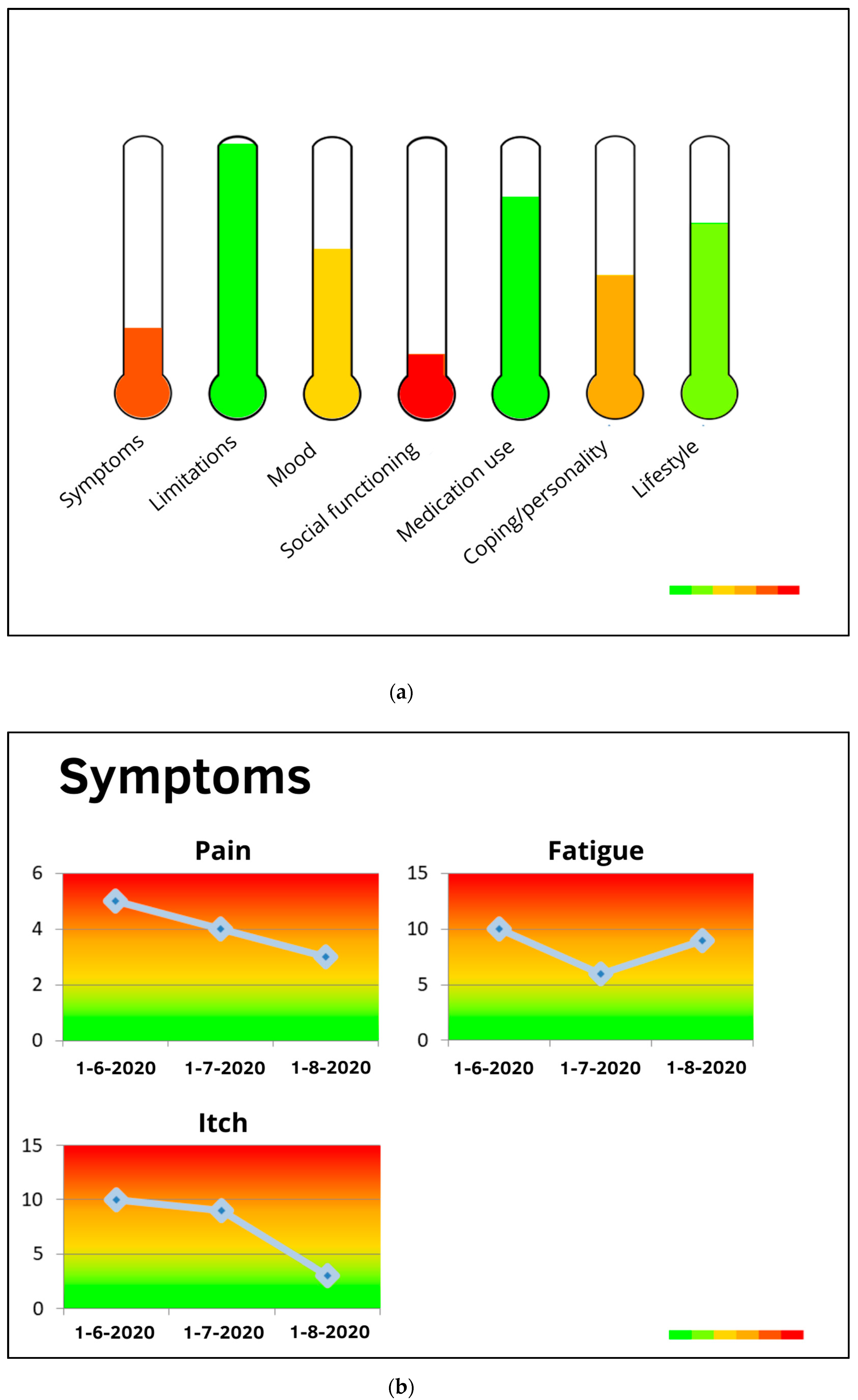
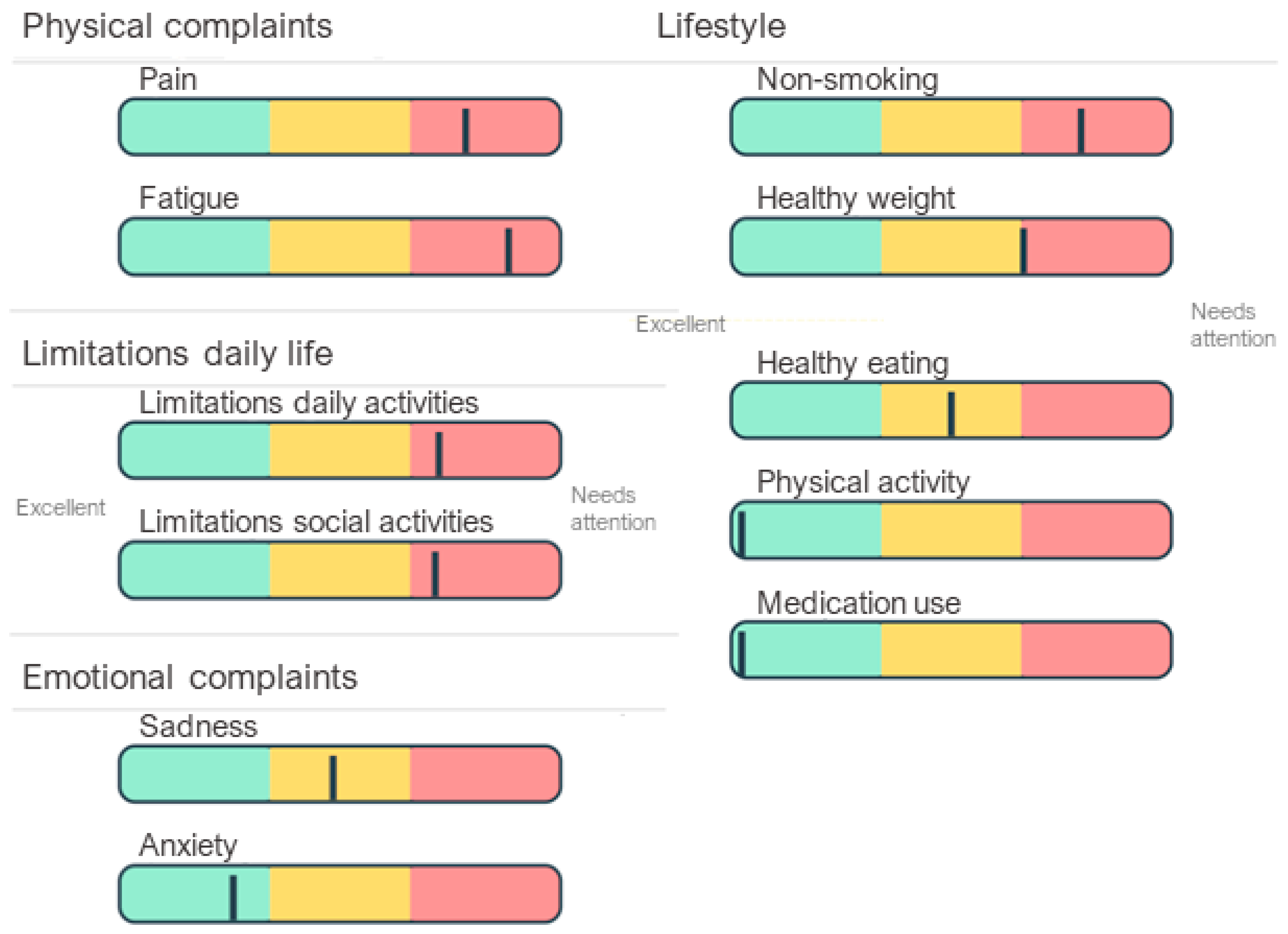
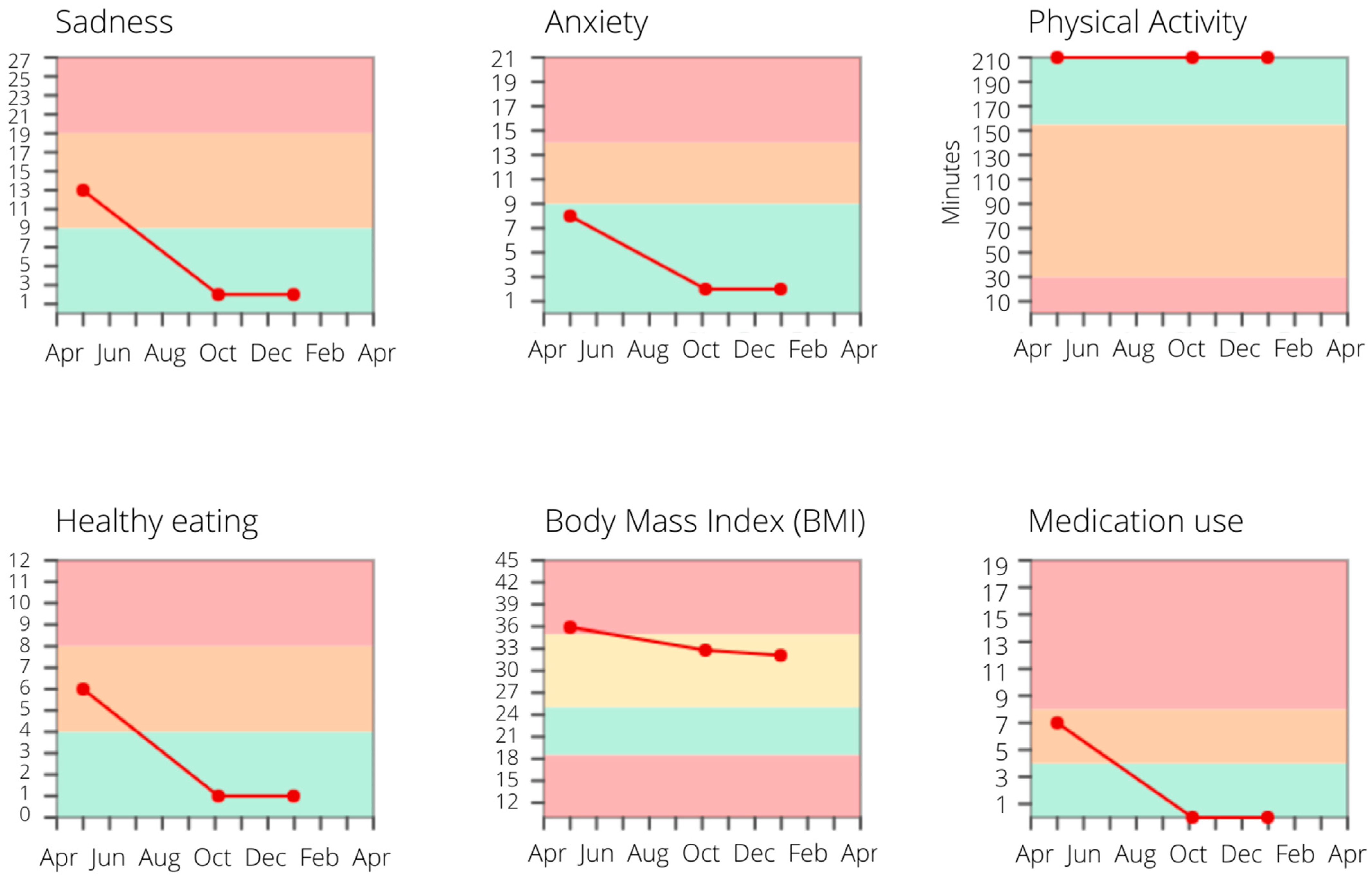
2.3. Personal Profile Charts to Visualize Screening Results
2.3.1. Development Personal Profile Charts Stage 1: Developing Initial Version
2.3.2. Development Personal Profile Charts Stage 2: Acquiring User Feedback
2.3.3. Development Personal Profile Charts Stage 3: Revising and Refining
2.4. iCBT Treatment
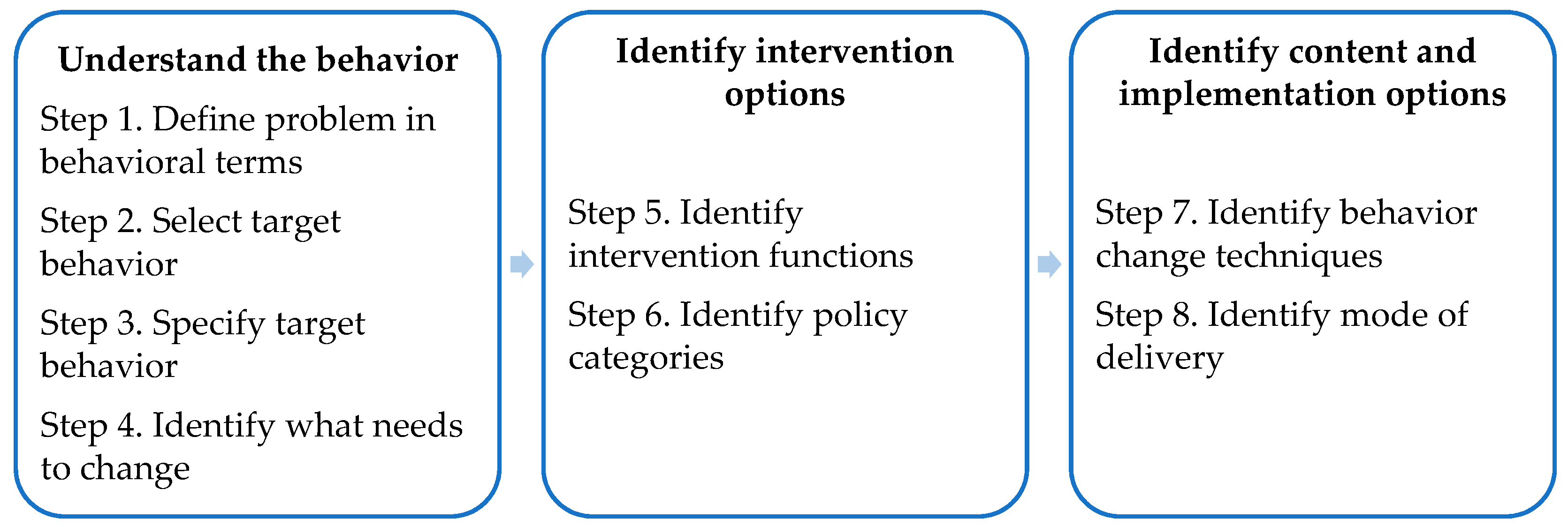
2.5. Treatment: Lifestyle Modules
2.5.1. Development Treatment Stage 1: Developing Initial Version
2.5.2. Development Treatment Stage 2: Acquiring User Feedback
2.5.3. Development Treatment Stage 3: Revising and Refining
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association. Lifestyle management: Standards of medical care in diabetes-2019. Diabetes Care 2019, 42, S46–S60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. World Health Statistics 2018: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Italy, 2018. [Google Scholar]
- Rippe, J.M. Lifestyle medicine: The health promoting power of daily habits and practices. Am. J. Lifestyle Med. 2018, 12, 499–512. [Google Scholar] [CrossRef] [PubMed]
- KDIGO CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2013, 3, 1–150. [Google Scholar] [CrossRef] [Green Version]
- Ricardo, A.C.; Anderson, C.A.; Yang, W.; Zhang, X.M.; Fischer, M.J.; Dember, L.M.; Fink, J.C.; Frydrych, A.; Jensvold, N.G.; Lustigova, E.; et al. Healthy lifestyle and risk of kidney disease progression, atherosclerotic events, and death in CKD: Findings from the Chronic Renal Insufficiency Cohort (CRIC) Study. Am. J. Kidney Dis. 2015, 65, 412–424. [Google Scholar] [CrossRef] [Green Version]
- Teo, K.; Lear, S.; Islam, S.; Mony, P.; Dehghan, M.; Li, W.; Rosengren, A.; Lopez-Jaramillo, P.; Diaz, R.; Oliveira, G.; et al. Prevalence of a healthy lifestyle among individuals with cardiovascular disease in high-, middle- and low-income countries: The Prospective Urban Rural Epidemiology (PURE) Study. JAMA 2013, 309, 1613–1621. [Google Scholar] [CrossRef] [Green Version]
- Neuendorf, R.; Harding, A.; Stello, N.; Hanes, D.; Wahbeh, H. Depression and anxiety in patients with Inflammatory Bowel Disease: A systematic review. J. Psychosom. Res. 2016, 87, 70–80. [Google Scholar] [CrossRef]
- Yohannes, A.M.; Willgoss, T.G.; Baldwin, R.C.; Connolly, M.J. Depression and anxiety in chronic heart failure and chronic obstructive pulmonary disease: Prevalence, relevance, clinical implications and management principles. Int. J. Geriatr. Psychiatry 2010, 25, 1209–1221. [Google Scholar] [CrossRef]
- Read, J.R.; Sharpe, L.; Modini, M.; Dear, B.F. Multimorbidity and depression: A systematic review and meta-analysis. J. Affect. Disord. 2017, 221, 36–46. [Google Scholar] [CrossRef]
- Detweiler-Bedell, J.B.; Friedman, M.A.; Leventhal, H.; Miller, I.W.; Leventhal, E.A. Integrating co-morbid depression and chronic physical disease management: Identifying and resolving failures in self-regulation. Clin. Psychol. Rev. 2008, 28, 1426–1446. [Google Scholar] [CrossRef] [Green Version]
- Hoang, D.; Kristoffersen, I.; Li, I.W. All in the mind? Estimating the effect of mental health on health behaviours. Soc. Sci. Med. 2019, 225, 69–84. [Google Scholar] [CrossRef]
- Cardol, C.K.; Boslooper-Meulenbelt, K.; Van Middendorp, H.; Meuleman, Y.; Evers, A.W.M.; Van Dijk, S. Psychosocial barriers and facilitators for adherence to a healthy lifestyle among patients with chronic kidney disease: A focus group study. BMC Nephrol. under review.
- Sumlin, L.L.; Garcia, T.J.; Brown, S.A.; Winter, M.A.; Garcia, A.A.; Brown, A.; Cuevas, H.E. Depression and adherence to lifestyle changes in type 2 diabetes A systematic review. Diabetes Educ. 2014, 40, 731–744. [Google Scholar] [CrossRef] [PubMed]
- Belaiche, S.; Decaudin, B.; Dharancy, S.; Noel, C.; Odou, P.; Hazzan, M. Factors relevant to medication non-adherence in kidney transplant: A systematic review. Int. J. Clin. Pharm. 2017, 39, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Farris, S.G.; Abrantes, A.M.; Bond, D.S.; Stabile, L.M.; Wu, W.C. Anxiety and fear of exercise in cardiopulmonary rehabilitation: Patient and practitioner perspectives. J. Cardiopulm. Rehabil. 2019, 39, E9–E13. [Google Scholar] [CrossRef] [PubMed]
- Ciere, Y.; van der Vaart, R.; van der Meulen-De Jong, A.E.; Maljaars, P.W.J.; van Buul, A.R.; Koopmans, J.G.; Snoeck-Stroband, J.B.; Chavannes, N.H.; Sont, J.K.; Evers, A.W.M. Implementation of an eHealth self-management care path for chronic somatic conditions. Clin. Ehealth 2019, 2, 3–11. [Google Scholar] [CrossRef]
- Lemmens, L.C.; Molema, C.C.M.; Versnel, N.; Baan, C.A.; de Bruin, S.R. Integrated care programs for patients with psychological comorbidity: A systematic review and meta-analysis. J. Psychosom. Res. 2015, 79, 580–594. [Google Scholar] [CrossRef]
- Bernard, P.; Romain, A.J.; Caudroit, J.; Chevance, G.; Carayol, M.; Gourlan, M.; Dancause, K.N.; Moullec, G. Cognitive behavior therapy combined with exercise for adults with chronic diseases: Systematic review and meta-analysis. Health Psychol. 2018, 37, 433–450. [Google Scholar] [CrossRef]
- Evers, A.W.M.; Gieler, U.; Hasenbring, M.I.; van Middendorp, H. Incorporating biopsychosocial characteristics into personalized healthcare: A clinical approach. Psychother. Psychosom. 2014, 83, 148–157. [Google Scholar] [CrossRef]
- Moss-Morris, R. Adjusting to chronic illness: Time for a unified theory. Brit. J. Health Psychiatry 2013, 18, 681–686. [Google Scholar] [CrossRef]
- Pabst, S.; Bertram, A.; Zimmermann, T.; Schiffer, M.; de Zwaan, M. Physician reported adherence to immunosuppressants in renal transplant patients: Prevalence, agreement, and correlates. J. Psychosom. Res. 2015, 79, 364–371. [Google Scholar] [CrossRef]
- Coventry, P.A.; Hays, R.; Dickens, C.; Bundy, C.; Garrett, C.; Cherrington, A.; Chew-Graham, C. Talking about depression: A qualitative study of barriers to managing depression in people with long term conditions in primary care. BMC Fam. Pr. 2011, 12, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratcliff, C.G.; Barrera, T.L.; Petersen, N.J.; Sansgiry, S.; Kauth, M.R.; Kunik, M.E.; Stanley, M.A.; Cully, J.A. Recognition of anxiety, depression, and PTSD in patients with COPD and CHF: Who gets missed? Gen. Hosp. Psychiatry 2017, 47, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Benze, G.; Nauck, F.; Alt-Epping, B.; Gianni, G.; Bauknecht, T.; Ettl, J.; Munte, A.; Kretzschmar, L.; Gaertner, J. PROutine: A feasibility study assessing surveillance of electronic patient reported outcomes and adherence via smartphone app in advanced cancer. Ann. Palliat. Med. 2019, 8, 104–111. [Google Scholar] [CrossRef] [PubMed]
- van der Willik, E.M.; Hemmelder, M.H.; Bart, H.A.J.; van Ittersum, F.J.; Hoogendijk-van den Akker, J.M.; Bos, W.J.W.; Dekker, F.W.; Meuleman, Y. Routinely measuring symptom burden and health-related quality of life in dialysis patients: First results from the Dutch registry of patient-reported outcome measures. Clin. Kidney J. 2020, sfz192. [Google Scholar] [CrossRef] [Green Version]
- Ferwerda, M.; van Beugen, S.; van Burik, A.; van Middendorp, H.; de Jong, E.M.; van de Kerkhof, P.C.; van Riel, P.L.; Evers, A.W. What patients think about E-health: Patients’ perspective on internet-based cognitive behavioral treatment for patients with rheumatoid arthritis and psoriasis. Clin. Rheumatol. 2013, 32, 869–873. [Google Scholar] [CrossRef]
- Shen, H.; van der Kleij, R.M.J.J.; van der Boog, P.J.M.; Chang, X.; Chavannes, N.H. Electronic health self-management interventions for patients with chronic kidney disease: Systematic review of quantitative and qualitative evidence. J. Med. Internet Res. 2019, 21, e12384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, S.; Peynenburg, V.A.; Hadjistavropoulos, H.D. Internet-delivered cognitive behaviour therapy for chronic health conditions: A systematic review and meta-analysis. J. Behav. Med. 2019, 42, 169–187. [Google Scholar] [CrossRef] [Green Version]
- van Beugen, S.; Ferwerda, M.; Hoeve, D.; Rovers, M.M.; Spillekom-van Koulil, S.; van Middendorp, H.; Evers, A.W. Internet-based cognitive behavioral therapy for patients with chronic somatic conditions: A meta-analytic review. J. Med. Internet Res. 2014, 16, e88. [Google Scholar] [CrossRef]
- van Beugen, S.; Ferwerda, M.; Spillekom-van Koulil, S.; Smit, J.V.; Zeeuwen-Franssen, M.E.; Kroft, E.B.; de Jong, E.M.; Otero, M.E.; Donders, A.R.; van de Kerkhof, P.C.; et al. Tailored therapist-guided internet-based cognitive behavioral treatment for psoriasis: A randomized controlled trial. Psychother. Psychosom. 2016, 85, 297–307. [Google Scholar] [CrossRef]
- Ferwerda, M.; van Beugen, S.; van Middendorp, H.; Spillekom-van Koulil, S.; Donders, A.R.T.; Visser, H.; Taal, E.; Creemers, M.C.W.; van Riel, P.C.L.M.; Evers, A.W.M. A tailored-guided internet-based cognitive-behavioral intervention for patients with rheumatoid arthritis as an adjunct to standard rheumatological care: Results of a randomized controlled trial. Pain 2017, 158, 868–878. [Google Scholar] [CrossRef]
- Beerthuizen, T.; Rijssenbeek-Nouwens, L.H.; van Koppen, S.M.; Khusial, R.J.; Snoeck-Stroband, J.B.; Sont, J.K. Internet-based self-management support after high-altitude climate treatment for severe asthma: Randomized controlled trial. J. Med. Internet Res. 2020, 22, e13145. [Google Scholar] [CrossRef]
- Tommel, J.; Evers, A.W.M.; Van Hamersvelt, H.W.; Jordens, R.; Van Dijk, S.; Hilbrands, L.B.; Hermans, M.M.H.; Hollander, D.A.M.J.; Van de Kerkhof, J.J.; Ten Dam, M.A.G.J.; et al. “What Matters to You?”—The Relevance of Patient Priorities in Dialysis Care for Assessment and Clinical Practice. Manuscript in preparation. Unpublished.
- Little, B.R. Personal Projects—A rationale and method for investigation. Environ. Behav. 1983, 15, 273–309. [Google Scholar] [CrossRef]
- Melville, L.L.; Baltic, T.A.; Bettcher, T.W.; Nelson, D.L. Patients’ perspectives on the self-identified goals assessment. Am. J. Occup. 2002, 56, 650–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tugwell, P.; Bombardier, C.; Buchanan, W.W.; Goldsmith, C.H.; Grace, E.; Hanna, B. The Mactar Patient Preference Disability Questionnaire—An individualized functional priority approach for assessing improvement in physical disability in clinical trials in rheumatoid arthritis. J. Rheumatol. 1987, 14, 446–451. [Google Scholar]
- Willis, G. Cognitive Interviewing: A Tool for Improving Questionnaire Design; Sage: Thousand Oaks, CA, USA, 2005. [Google Scholar]
- Slok, A.H.; Kotz, D.; van Breukelen, G.; Chavannes, N.H.; Rutten-van Molken, M.P.; Kerstjens, H.A.; van der Molen, T.; Asijee, G.M.; Dekhuijzen, P.N.; Holverda, S.; et al. Effectiveness of the Assessment of Burden of COPD (ABC) tool on health-related quality of life in patients with COPD: A cluster randomised controlled trial in primary and hospital care. BMJ Open 2016, 6, e011519. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel: A Guide to Designing Interventions; Silverback Publishing: London, UK, 2014. [Google Scholar]
- Meuleman, Y.; Hoekstra, T.; Dekker, F.W.; Navis, G.; Vogt, L.; van der Boog, P.J.; Bos, W.J.; van Montfrans, G.A.; van Dijk, S.; Group, E.S. Sodium restriction in patients with CKD: A randomized controlled trial of self-management support. Am. J. Kidney Dis. 2016, 69, 576–586. [Google Scholar] [CrossRef] [Green Version]
- Janssen, V.; De Gucht, V.; van Exel, H.; Maes, S. A self-regulation lifestyle program for post-cardiac rehabilitation patients has long-term effects on exercise adherence. J. Behav. Med. 2014, 37, 308–321. [Google Scholar] [CrossRef]
- Wang, Y.L.; Fadhil, A.; Lange, J.P.; Reiterer, H. Integrating taxonomies into theory-based digital health interventions for behavior change: A holistic framework. JMIR Res. Protoc. 2019, 8, e8055. [Google Scholar] [CrossRef]
- Dalgetty, R.; Miller, C.B.; Dombrowski, S.U. Examining the theory-effectiveness hypothesis: A systematic review of systematic reviews. Br. J. Health Psychol. 2019, 24, 334–356. [Google Scholar] [CrossRef]
- Varsi, C.; Nes, L.S.; Kristjansdottir, O.B.; Kelders, S.M.; Stenberg, U.; Zangi, H.A.; Borosund, E.; Weiss, K.E.; Stubhaug, A.; Asbjornsen, R.A.; et al. Implementation strategies to enhance the implementation of eHealth programs for patients with chronic illnesses: Realist systematic review. J. Med. Internet Res. 2019, 21, e14255. [Google Scholar] [CrossRef] [PubMed]
- Schreiweis, B.; Pobiruchin, M.; Strotbaum, V.; Suleder, J.; Wiesner, M.; Bergh, B. Barriers and Facilitators to the implementation of eHealth services: Systematic literature analysis. J. Med. Internet Res. 2019, 21, e14197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.L.; Mishra, G.D.; Jones, M. Evidence on multimorbidity from definition to intervention: An overview of systematic reviews. Ageing Res. Rev. 2017, 37, 53–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sisti, L.G.; Dajko, M.; Campanella, P.; Shkurti, E.; Ricciardi, W.; de Waure, C. The effect of multifactorial lifestyle interventions on cardiovascular risk factors: A systematic review and meta-analysis of trials conducted in the general population and high risk groups. Prev. Med. 2018, 109, 82–97. [Google Scholar] [CrossRef] [PubMed]
- Boslooper-Meulenbelt, K.; Patijn, O.; Battjes-Fries, M.C.E.; Haisma, H.; Pot, G.K.; Navis, G.J. Barriers and facilitators of fruit and vegetable consumption in renal transplant recipients, family members and healthcare professionals-a focus group study. Nutrients 2019, 11, 2427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hudson, J.L.; Moss-Morris, R. Treating illness distress in chronic illness integrating mental health approaches with illness self-management. Eur. Psychol. 2019, 24, 26–37. [Google Scholar] [CrossRef] [Green Version]
- Brettschneider, C.; Kohlmann, S.; Gierk, B.; Lowe, B.; Konig, H.H. Depression screening with patient-targeted feedback in cardiology: The cost-effectiveness of DEPSCREEN-INFO. PLoS ONE 2017, 12, e181021. [Google Scholar] [CrossRef] [Green Version]
- Senteio, C.R.; Adler-Milstein, J.; Richardson, C.; Veinot, T. Psychosocial information use for clinical decisions in diabetes care. J. Am. Med. Inf. Assoc. 2019, 26, 813–824. [Google Scholar] [CrossRef] [Green Version]
- Knudsen, M.D.; Hjartaker, A.; Robb, K.A.; de Lange, T.; Hoff, G.; Berstad, P. Improving cancer preventive behaviors: A randomized trial of tailored lifestyle feedback in colorectal cancer screening. Cancer Epidemiol. Prev. Biomark. 2018, 27, 1442–1449. [Google Scholar] [CrossRef] [Green Version]
- White, V.; Linardon, J.; Stone, J.E.; Holmes-Truscott, E.; Olive, L.; Mikocka-Walus, A.; Hendrieckx, C.; Evans, S.; Speight, J. Online psychological interventions to reduce symptoms of depression, anxiety, and general distress in those with chronic health conditions: A systematic review and meta-analysis of randomized controlled trials. Psychol. Med. 2020, 1–26. [Google Scholar] [CrossRef]
- Sangrar, R.; Docherty-Skippen, S.M.; Beattie, K. Blended face-to-face and online/computer-based education approaches in chronic disease self-management: A critical interpretive synthesis. Patient Educ. Couns. 2019, 102, 1822–1832. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, S.; Cabral, C.; Hay, A.; Lucas, P.J. Health equity in the effectiveness of web-based health interventions for the self-care of people with chronic health conditions: Systematic review. J. Med. Internet Res. 2020, 22, e17849. [Google Scholar] [CrossRef] [PubMed]
- Armaou, M.; Araviaki, E.; Musikanski, L. eHealth and mHealth interventions for ethnic minority and historically underserved populations in developed countries: An umbrella review. Int. J. Com. WB 2020, 3, 193–221. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Key Behavioral Problem | Unhealthy Lifestyle Behaviors (Leading to Poor Health Outcomes) |
|---|---|
| What (target behavior) | Physical activity: moderate-to-vigorous intensity ≥150 min per week in multiple sessions Healthy weight: BMI 18.5 to 24.9 Healthy diet: Adherence to dietary prescriptions (e.g., low sodium) Smoking: No tobacco smoking Medication: Adherence to medication prescriptions |
| Who (target group) | Individuals with lifestyle-related chronic diseases |
| When/where/how often | Regularly, i.e., on a weekly to daily basis, embedded in daily schedule |
| With whom | With support from health professionals and social environment |
| COM-B Component (Step 4) | Main TDF Barriers and Facilitators (Step 4) | Selected Intervention Functions (Step 5) | Selected BCTs (Step 7) | Description of BCTs within the Intervention | Lifestyle iCBT Module (Based on Stages of Behavior Change) |
|---|---|---|---|---|---|
| Capability | Knowledge (How to engage in a healthy lifestyle) | Education, Persuasion | Instruction on how to perform the behavior; Information about antecedents; Information about health consequences; Feedback on behavior | Guidelines on what, how, and why to engage in healthy lifestyle behaviors; Instruction to keep a record of (unhealthy) behaviors and of events, emotions, and cognitions occurring prior to it; Information about advantages of healthy behaviors; Evaluative feedback on monitored behavior. | 1: Goals Exploration (contemplation and decision) |
| Opportunity | Social influences (Support by professionals and social environment) | Enablement | Social support (unspecified); social support (practical); social support (emotional) | Exercise to discuss personal strengths with important others and how to implement them in behavior change; Exercise to think about ways in which social support is received and about emotional and practical support the person would (not) like to receive; Prompt to ask for support. | 3: Goals Persistence (evaluation and maintenance) |
| Environmental context and resources (Disease symptoms and material support tools) | Enablement | Restructuring the physical environment; Avoidance/changing exposure to cues for the behavior | Advice and prompt to think about how to avoid exposure to environmental cues for unhealthy behavior and to make adaptations to the environment that facilitate the wanted behavior. | 2: Goals in Action (planning and action) | |
| Motivation | Role and identity (Personality characteristics) | Persuasion | Valued self-identity | Exercise to list personal strengths. | 3: Goals Persistence (evaluation and maintenance) |
| Beliefs about capabilities (Self-efficacy, locus of control) | Persuasion | Focus on past success | Exercise to list previous successes in behavior change. | 3: Goals Persistence (evaluation and maintenance) | |
| Optimism (Acceptance, focusing on possibilities vs. limitations) | Persuasion | Problem solving | Exercise to identify barriers for behavior change and explore ways to overcome them. | 1: Goals Exploration (contemplation and decision) | |
| Emotion (Depression, stress, anxiety) | Education, Persuasion, Enablement | Education, Persuasion: Information on emotional consequences; Self-assessment of affective consequences Enablement: Reduce negative emotions | Information about emotional advantages of healthy lifestyle behaviors; Instruction to keep a record of feelings after performing unhealthy vs. healthy behaviors; Exercise to identify positive self-talk and images to promote positive emotions that facilitate maintenance of the wanted behavior; Exercise to identify ways to reduce negative and stressful emotions. | 1: Goals Exploration (contemplation and decision) 3: Goals Persistence (evaluation and maintenance) | |
| Reinforcement (Noticeable effects of healthy behavior, rewards) | Incentivization | Self-reward, material reward | Prompt to use a personally relevant reward if there has been progress in the wanted behavior. | 2: Goals in Action (planning and action) | |
| Intentions (Intrinsic motivation, joy, higher-order purposes) | Incentivization, Enablement | Pros and cons; Commitment | Exercise to identify and compare reasons for wanting and not wanting to change behavior; Exercise to link the wanted behavior to personally relevant higher-order values; Instruction to write down a decision statement indicating commitment to change behavior. | 1: Goals Exploration (contemplation and decision) | |
| Goals (Concrete and feasible goals) | Enablement | Goal setting (outcome); Goal setting (behavior); Review of outcome goals; Review of behavior goals; Action planning | Exercise to set weekly goals; Instruction to create a daily action (implementation intentions); Prompt to reflect on behavior and correspondence with goals and action plans, leading to re-setting or adapting. | 2: Goals in Action (planning and action) 3: Goals Persistence (evaluation and maintenance) | |
| Beliefs about Consequences (Beliefs about and experiences with consequences of behavior) | Enablement | Pros and cons | Exercise to identify and compare reasons for wanting and not wanting to change behavior. | 1: Goals Exploration (contemplation and decision) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardol, C.K.; Tommel, J.; van Middendorp, H.; Ciere, Y.; Sont, J.K.; Evers, A.W.M.; van Dijk, S. Detecting and Treating Psychosocial and Lifestyle-Related Difficulties in Chronic Disease: Development and Treatment Protocol of the E-GOAL eHealth Care Pathway. Int. J. Environ. Res. Public Health 2021, 18, 3292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063292
Cardol CK, Tommel J, van Middendorp H, Ciere Y, Sont JK, Evers AWM, van Dijk S. Detecting and Treating Psychosocial and Lifestyle-Related Difficulties in Chronic Disease: Development and Treatment Protocol of the E-GOAL eHealth Care Pathway. International Journal of Environmental Research and Public Health. 2021; 18(6):3292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063292
Chicago/Turabian StyleCardol, Cinderella K., Judith Tommel, Henriët van Middendorp, Yvette Ciere, Jacob K. Sont, Andrea W. M. Evers, and Sandra van Dijk. 2021. "Detecting and Treating Psychosocial and Lifestyle-Related Difficulties in Chronic Disease: Development and Treatment Protocol of the E-GOAL eHealth Care Pathway" International Journal of Environmental Research and Public Health 18, no. 6: 3292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063292