
Psychometric Properties of the POAGTS: A Tool for Understanding Parents’ Perceptions Regarding Autism Spectrum Disorder Genetic Testing


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
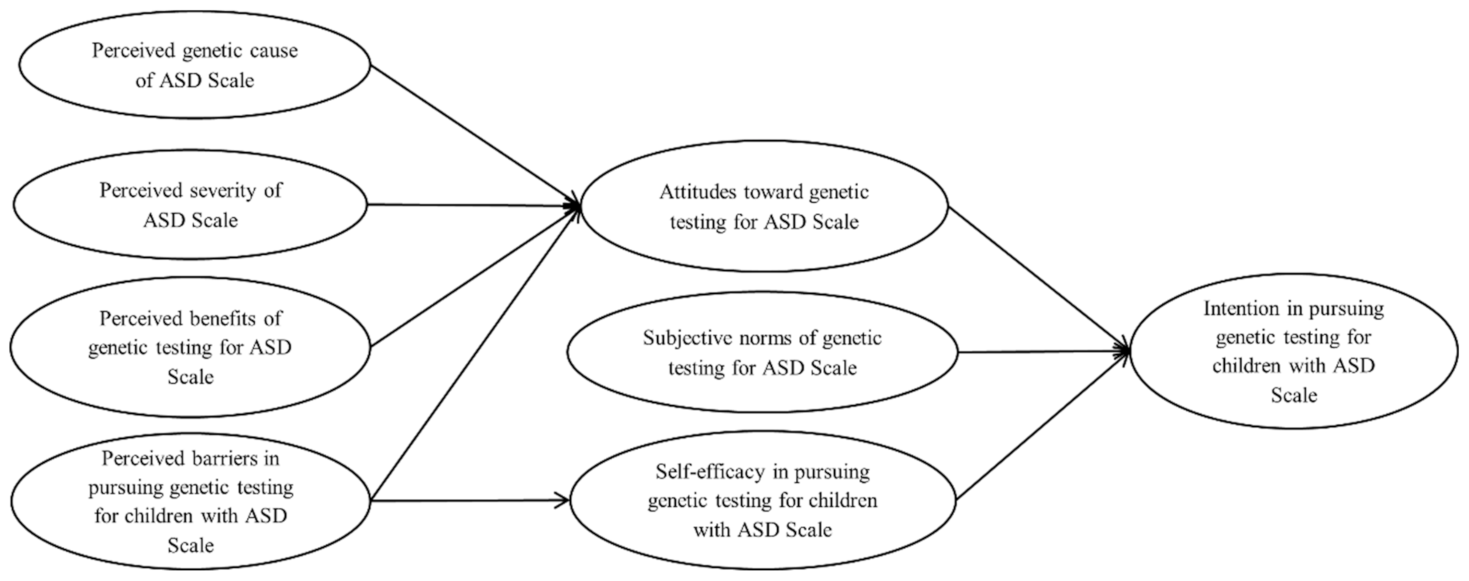
2.1. Theoretical Framework
2.2. Measurement
2.3. Pretesting the POAGTS
2.4. Formal Testing
2.4.1. Data Collection
2.4.2. Participants
2.4.3. Statistical Analyses
3. Results
3.1. Reliability
3.2. Exploratory Factor Analysis (EFA)
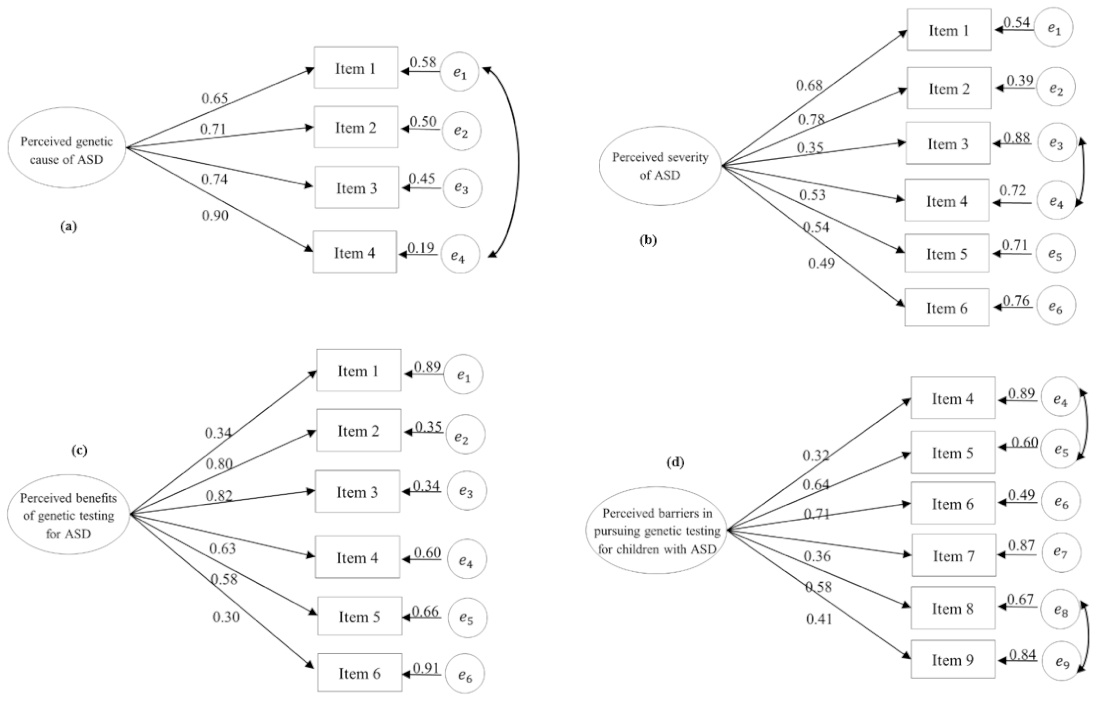
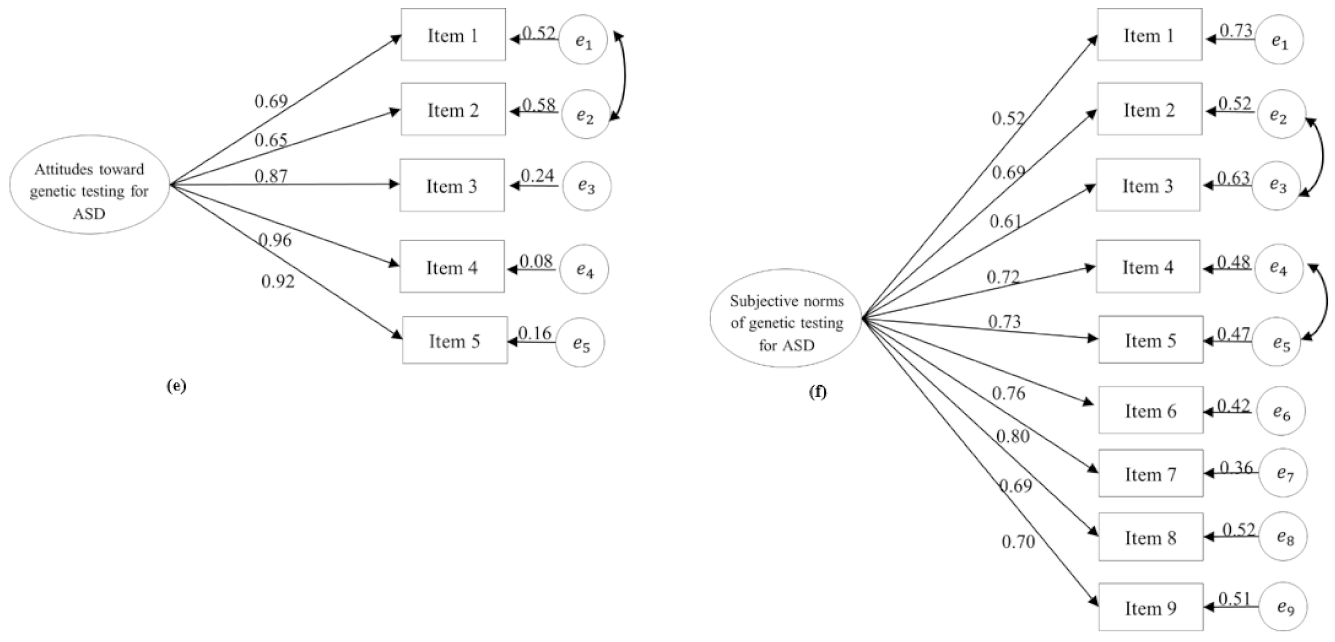
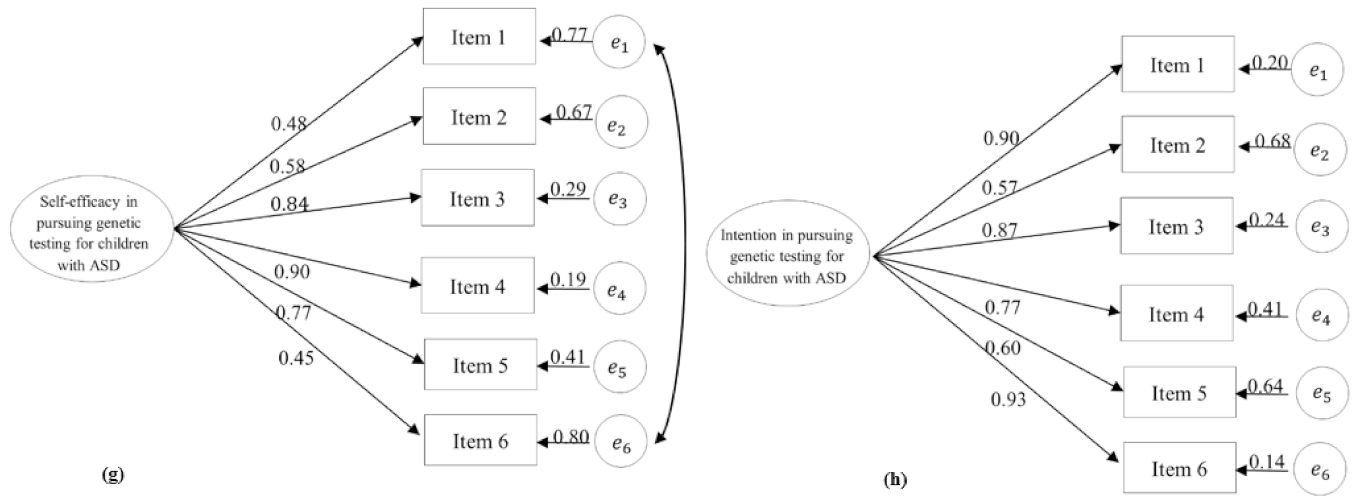
3.3. Confirmatory Factor Analysis (CFA)
3.4. Structural Equation Modeling (SEM)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Neurodevelopmental Disorders. In Diagnostic and Statistical Manual of Mental Disorders DSM-5, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Centers for Disease Control and Prevention. Data & Statistics on Autism Spectrum Disorder. Available online: https://www.cdc.gov/ncbddd/autism/data.html (accessed on 5 January 2021).
- Šestan, N. The emerging biology of autism spectrum disorders. Science 2012, 337, 1301–1303. [Google Scholar]
- Devlin, B.; Scherer, S.W. Genetic architecture in autism spectrum disorder. Curr. Opin. Genet. Dev. 2012, 22, 229–237. [Google Scholar] [CrossRef]
- Betancur, C. Etiological heterogeneity in autism spectrum disorders: More than 100 genetic and genomic disorders and still counting. Brain Res. 2011, 1380, 42–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torre-Ubieta, L.; Won, H.; Stein, J.L.; Geschwind, D.H. Advancing the understanding of autism disease mechanisms through genetics. Nat. Med. 2016, 22, 345. [Google Scholar] [CrossRef]
- Jeste, S.S.; Geschwind, D.H. Disentangling the heterogeneity of autism spectrum disorder through genetic findings. Nat. Rev. Neurol. 2014, 10, 74–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, C.P.; Myers, S.M. Identification and evaluation of children with autism spectrum disorders. Pediatrics 2007, 120, 1183–1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moeschler, J.B.; Shevell, M. Comprehensive evaluation of the child with intellectual disability or global developmental delays. Pediatrics 2014, 134, e903–e918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volkmar, F.; Siegel, M.; Woodbury-Smith, M.; King, B.; McCracken, J.; State, M. Practice parameter for the assessment and treatment of children and adolescents with autism spectrum disorder. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 237–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michelson, D.; Shevell, M.; Sherr, E.; Moeschler, J.; Gropman, A.; Ashwal, S. Evidence report: Genetic and metabolic testing on children with global developmental delay: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2011, 77, 1629–1635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefer, G.B.; Mendelsohn, N.J. Clinical genetics evaluation in identifying the etiology of autism spectrum disorders: 2013 guideline revisions. Genet. Med. 2013, 15, 399–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefer, G.B. Clinical genetic aspects of autism spectrum disorders. Int. J. Mol. Sci. 2016, 17, 180. [Google Scholar] [CrossRef] [Green Version]
- Shen, Y.; Dies, K.A.; Holm, I.A.; Bridgemohan, C.; Sobeih, M.M.; Caronna, E.B.; Miller, K.J.; Frazier, J.A.; Silverstein, I.; Picker, J.; et al. Clinical genetic testing for patients with autism spectrum disorders. Pediatrics 2010, 125, e727–e735. [Google Scholar] [CrossRef] [Green Version]
- Howsmon, D.P.; Kruger, U.; Melnyk, S.; James, S.J.; Hahn, J. Classification and adaptive behavior prediction of children with autism spectrum disorder based upon multivariate data analysis of markers of oxidative stress and DNA methylation. PLoS Comput. Biol. 2017, 13, e1005385. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.-H.; Wang, Y.; Xiu, X.; Choy, K.W.; Pursley, A.N.; Cheung, S.W. Genetic diagnosis of autism spectrum disorders: The opportunity and challenge in the genomics era. Crit. Rev. Clin. Lab. Sci. 2014, 51, 249–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, P.; Elsabbagh, M.; Bolton, P.; Singh, I. In search of biomarkers for autism: Scientific, social and ethical challenges. Nat. Rev. Neurosci. 2011, 12, 603. [Google Scholar] [CrossRef]
- Rabba, A.S.; Dissanayake, C.; Barbaro, J. Parents’ experiences of an early autism diagnosis: Insights into their needs. Res. Autism Spectr. Disord. 2019, 66, 101415. [Google Scholar] [CrossRef]
- Downes, N.; Lichtlé, J.; Lamore, K.; Orêve, M.-J.; Cappe, E. Couples’ experiences of parenting a child after an autism diagnosis: A qualitative study. J. Autism Dev. Disord. 2020, 1–14. [Google Scholar] [CrossRef]
- Fernańdez-Alcántara, M.; García-Caro, M.P.; Pérez-Marfil, M.N.; Hueso-Montoro, C.; Laynez-Rubio, C.; Cruz-Quintana, F. Feelings of loss and grief in parents of children diagnosed with autism spectrum disorder (ASD). Res. Dev. Disabil. 2016, 55, 312–321. [Google Scholar] [CrossRef]
- Lewis, S.; Curnow, L.; Ross, M.; Massie, J. Parental attitudes to the identification of their infants as carriers of cystic fibrosis by newborn screening. J. Paediatr. Child Health 2006, 42, 533–537. [Google Scholar] [CrossRef]
- Moran, J.; Quirk, K.; Duff, A.J.; Brownlee, K.G. Newborn screening for CF in a regional paediatric centre: The psychosocial effects of false-positive IRT results on parents. J. Cyst. Fibros. 2007, 6, 250–254. [Google Scholar] [CrossRef] [Green Version]
- Aatre, R.D.; Day, S.M. Psychological issues in genetic testing for inherited cardiovascular diseases. Circ. Cardiovasc. Genet. 2011, 4, 81–90. [Google Scholar] [CrossRef]
- Dinc, L.; Terzioglu, F. The psychological impact of genetic testing on parents. J. Clin. Nurs. 2006, 15, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Janz, N.K.; Becker, M.H. The health belief model: A decade later. Health Educ. Behav. 1984, 11, 1–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenstock, I.M. Historical origins of the health belief model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory, 1st ed.; Prentice-Hall, Inc.: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Bunn, J.Y.; Bosompra, K.; Ashikaga, T.; Flynn, B.S.; Worden, J.K. Factors influencing intention to obtain a genetic test for colon cancer risk: A population-based study. Prev. Med. 2002, 34, 567–577. [Google Scholar] [CrossRef]
- Sagi, M.; Shiloh, S.; Cohen, T. Application of the health belief model in a study on parents’ intentions to utilize prenatal diagnosis of cleft lip and/or palate. Am. J. Med. Genet. Part A 1992, 44, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Levine, F.R.; Coxworth, J.E.; Stevenson, D.A.; Tuohy, T.; Burt, R.W.; Kinney, A.Y. Parental attitudes, beliefs, and perceptions about genetic testing for FAP and colorectal cancer surveillance in minors. J. Genet. Couns. 2010, 19, 269–279. [Google Scholar] [CrossRef] [Green Version]
- Gooding, H.C.; Organista, K.; Burack, J.; Biesecker, B.B. Genetic susceptibility testing from a stress and coping perspective. Soc. Sci. Med. 2006, 62, 1880–1890. [Google Scholar] [CrossRef] [PubMed]
- Doukas, D.J.; Localio, A.R.; Li, Y. Attitudes and beliefs concerning prostate cancer genetic screening. Clin. Genet. 2004, 66, 445–451. [Google Scholar] [CrossRef]
- Miller, S.M.; Shoda, Y.; Hurley, K. Applying cognitive-social theory to health-protective behavior: Breast self-examination in cancer screening. Psychol. Bull. 1996, 119, 70. [Google Scholar] [CrossRef]
- Lagos, V.I.; Perez, M.A.; Ricker, C.N.; Blazer, K.R.; Santiago, N.M.; Feldman, N.; Viveros, L.; Weitzel, J.N. Social-cognitive aspects of underserved Latinas preparing to undergo genetic cancer risk assessment for hereditary breast and ovarian cancer. Psycho-Oncology 2008, 17, 774–782. [Google Scholar] [CrossRef]
- Armitage, C.J.; Conner, M. Social cognition models and health behaviour: A structured review. Psychol. Health 2000, 15, 173–189. [Google Scholar] [CrossRef] [Green Version]
- Godin, G.; Gagnon, H.; Alary, M.; Noël, L.; Morissette, M.R. Correctional officers’ intention of accepting or refusing to make HIV preventive tools accessible to inmates. AIDS Educ. Prev. 2001, 13, 462–473. [Google Scholar] [CrossRef]
- Calsbeek, H.; Morren, M.; Bensing, J.; Rijken, M. Knowledge and attitudes towards genetic testing: A two year follow-up study in patients with asthma, diabetes mellitus and cardiovascular disease. J. Genet. Couns. 2007, 16, 493–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behavior and Health Education: Theory, Research, and Practice, 5th ed.; John Wiley & Sons: San Francisco, CA, USA, 2015. [Google Scholar]
- Dillman, D.A.; Smyth, J.D.; Christian, L.M. Internet, Phone, Mail, and Mixed-Mode Surveys: The Tailored Design Method, 4th ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014. [Google Scholar]
- DeVellis, R.F. Scale Development: Theory and Applications, 4th ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Lee, H.; Marvin, A.R.; Watson, T.; Piggot, J.; Law, J.K.; Law, P.A.; Constantino, J.N.; Nelson, S.F. Accuracy of phenotyping of autistic children based on internet implemented parent report. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2010, 153, 1119–1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marvin, A.; Law, P.; Law, J.; Arthur, R.; Mortenson, E.; Abbacchi, A.; Constantino, J. Non-verbal children with ASD (NV-ASD): Validating a registry and characterizing a population. In Proceedings of the International Meeting for Autism Research, Atlanta, GA, USA, 14–17 May 2014. [Google Scholar]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Field, A. Discovering Statistics Using SPSS, 3rd ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Hendrickson, A.E.; White, P.O. Promax: A quick method for rotation to oblique simple structure. Br. J. Math. Stat. Psychol. 1964, 17, 65–70. [Google Scholar] [CrossRef]
- Henson, R.K.; Roberts, J.K. Use of exploratory factor analysis in published research: Common errors and some comment on improved practice. Educ. Psychol. Meas. 2006, 66, 393–416. [Google Scholar] [CrossRef] [Green Version]
- Kline, P. An Easy Guide to Factor Analysis; Routledge: New York, NY, USA, 1994. [Google Scholar]
- Muthén, L.; Muthén, B. Mplus User’s Guide; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; The Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Hutcheson, G.D.; Sofroniou, N. The Multivariate Social Scientist: Introductory Statistics Using Generalized Linear Models, 1st ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1999. [Google Scholar]
- Giarelli, E.; Reiff, M. Mothers’ appreciation of chromosomal microarray analysis for autism spectrum disorder. J. Spec. Pediatr. Nurs. 2015, 20, 244–258. [Google Scholar] [CrossRef]
- Reiff, M.; Giarelli, E.; Bernhardt, B.A.; Easley, E.; Spinner, N.B.; Sankar, P.L.; Mulchandani, S. Parents’ perceptions of the usefulness of chromosomal microarray analysis for children with autism spectrum disorders. J. Autism Dev. Disord. 2015, 45, 3262–3275. [Google Scholar] [CrossRef]
- Hayeems, R.; Babul-Hirji, R.; Hoang, N.; Weksberg, R.; Shuman, C. Parents’ experience with pediatric microarray: Transferrable lessons in the era of genomic counseling. J. Genet. Couns. 2016, 25, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Harrington, J.W.; Emuren, L.; Restaino, K.; Schrier Vergano, S. Parental perception and participation in genetic testing among children with autism spectrum disorders. Clin. Pediatr. 2018, 57, 1642–1655. [Google Scholar] [CrossRef] [PubMed]
- Asparouhov, T.; Muthén, B.; Morin, A.J. Bayesian structural equation modeling with cross-loadings and residual covariances: Comments on Stromeyer et al. J. Manag. 2015, 41, 1561–1577. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research, 2nd ed.; Guilford Publications: New York, NY, USA, 2015. [Google Scholar]
- Lohmöller, J.-B. Latent Variable Path Modeling with Partial Least Squares; Springer: Berlin, Germany, 1989. [Google Scholar]
- Wydeven, K.V.; Kwan, A.; Hardan, A.Y.; Bernstein, J.A. Underutilization of genetics services for autism: The importance of parental awareness and provider recommendation. J. Genet. Couns. 2012, 21, 803–813. [Google Scholar] [CrossRef]
- Narcisa, V.; Discenza, M.; Vaccari, E.; Rosen-Sheidley, B.; Hardan, A.Y.; Couchon, E. Parental interest in a genetic risk assessment test for autism spectrum disorders. Clin. Pediatr. 2013, 52, 139–146. [Google Scholar] [CrossRef]
- Farmer, J.E.; Clark, M.J.; Mayfield, W.A.; Cheak-Zamora, N.; Marvin, A.R.; Law, J.K.; Law, P.A. The relationship between the medical home and unmet needs for children with autism spectrum disorders. Matern. Child Health J. 2014, 18, 672–680. [Google Scholar] [CrossRef]
- Masino, S.A.; Kawamura, M., Jr.; Plotkin, L.M.; Svedova, J.; DiMario, F.J., Jr.; Eigsti, I.-M. The relationship between the neuromodulator adenosine and behavioral symptoms of autism. Neurosci. Lett. 2011, 500, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Interactive Autism Network. IAN Survey Results Viewer—Birth and ASD Diagnosis History Questionnaire. Available online: https://dashboards.ianservices.org/Dashboards/Codebook/Build/IANCommunity/ICXUVX (accessed on 25 July 2020).
- Millsap, R.E.; Kwok, O.-M. Evaluating the impact of partial factorial invariance on selection in two populations. Psychol. Methods 2004, 9, 93–115. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Mean | SD | Item Total r |
|---|---|---|---|
| Perceived Genetic Cause of ASD Scale (4 items) | |||
| Response Scale: (1) Strongly Disagree, (2) Disagree, (3) Agree, (4) Strongly Agree | |||
| How much do you agree or disagree with the following statements? | |||
| 1. ASD has a genetic factor | 3.31 | 0.61 | 0.52 |
| 2. ASD is caused by genes | 2.85 | 0.66 | 0.67 |
| 3. ASD is associated with family history | 2.92 | 0.63 | 0.68 |
| 4. ASD is an inherited disorder | 2.75 | 0.68 | 0.70 |
| Scale (total score) | 11.82 | 2.07 | |
| Internal Consistency (Cronbach’s α) | 0.82 | ||
| Perceived Severity of ASD Scale (6 items) | |||
| Response Scale: (1) Strongly Disagree, (2) Disagree, (3) Agree, (4) Strongly Agree | |||
| How much do you agree or disagree with the following statements? | |||
| 1. ASD is a severe disorder | 3.00 | 0.77 | 0.53 |
| 2. Individuals with ASD have problems living independently | 3.04 | 0.70 | 0.63 |
| 3. The public discriminates against individuals with ASD | 3.19 | 0.66 | 0.36 |
| 4. Individuals with ASD have fewer job opportunities | 3.46 | 0.63 | 0.49 |
| 5. Compared to a child without ASD, it’s hard to raise a child with ASD | 3.51 | 0.64 | 0.48 |
| 6. Health problems associated with ASD are severe | 2.50 | 0.76 | 0.42 |
| Scale (total score) | 18.69 | 2.76 | |
| Internal Consistency (Cronbach’s α) | 0.74 | ||
| Perceived Benefits of Genetic Testing for ASD Scale (6 items) | |||
| Response Scale: (1) Strongly Disagree, (2) Disagree, (3) Agree, (4) Strongly Agree | |||
| How much do you agree or disagree with the following statements? | |||
| 1. ASD genetic testing identifies the cause of children’s ASD | 2.37 | 0.69 | 0.33 |
| 2. ASD genetic testing promotes early detection and intervention for children with ASD | 2.93 | 0.63 | 0.65 |
| 3. ASD genetic testing helps develop treatment plans targeting ASD-associated medical conditions for affected children | 2.89 | 0.62 | 0.65 |
| 4. ASD genetic testing helps children with ASD make informed family planning decisions | 2.80 | 0.70 | 0.54 |
| 5. ASD genetic testing helps children with ASD get more social support | 2.56 | 0.76 | 0.54 |
| 6. Taking children with ASD to undergo ASD genetic testing contributes to ASD research | 3.35 | 0.54 | 0.25 |
| Scale (total score) | 16.90 | 2.63 | |
| Internal Consistency (Cronbach’s α) | 0.75 | ||
| Perceived Barriers in Pursuing Genetic Testing for Children with ASD Scale (9 items) | |||
| Response Scale: (1) Strongly Disagree, (2) Disagree, (3) Agree, (4) Strongly Agree | |||
| How much do you agree or disagree with the following statements? | |||
| 1. ASD is not caused by genes | 2.03 | 0.62 | 0.07 |
| 2. ASD genetic testing cannot improve the current situation of my child(ren) diagnosed with ASD | 2.53 | 0.81 | 0.26 |
| 3. My child(ren) has/have already been diagnosed with ASD, so there’s no need to undergo this testing | 2.10 | 0.73 | 0.46 |
| 4. Taking my child(ren) with ASD to undergo ASD genetic testing contradicts with my religious or cultural beliefs. | 1.34 | 0.49 | 0.29 |
| 5. ASD genetic testing does more harm than good | 1.59 | 0.61 | 0.56 |
| 6. ASD genetic testing can cause family conflicts | 2.06 | 0.79 | 0.42 |
| 7. The procedure of undergoing ASD genetic testing is uncomfortable for my child (i.e., drawing blood) | 2.76 | 0.90 | 0.28 |
| 8. The results of ASD genetic testing can cause public discrimination against my child(ren) with ASD | 2.02 | 0.78 | 0.52 |
| 9. The results of ASD genetic testing can put the health insurance status of my child(ren) with ASD in jeopardy | 2.22 | 0.87 | 0.46 |
| Scale (total score) | 18.65 | 3.58 | |
| Internal Consistency (Cronbach’s α) | 0.69 | ||
| Attitudes Toward Genetic Testing for ASD Scale—Product of Belief (5 items) and Value (5 items) | |||
| 1. Taking a child with ASD to undergo ASD genetic testing is a good thing | 8.71 | 3.33 | 0.78 |
| 2. Taking a child with ASD to undergo ASD genetic testing is beneficial | 9.06 | 3.32 | 0.74 |
| 3. Taking a child with ASD to undergo ASD genetic testing is necessary | 6.00 | 3.65 | 0.83 |
| 4. All children diagnosed with ASD should undergo ASD genetic testing | 6.16 | 3.72 | 0.86 |
| 5. All children with ASD characteristics or traits should undergo ASD genetic testing | 6.19 | 3.64 | 0.82 |
| Scale (total score) | 36.12 | 15.52 | |
| Internal Consistency (Cronbach’s α) | 0.93 | ||
| Subjective Norms of Genetic Testing for ASD Scale—Product of Normative Belief (9 items) and Motivation to Comply (9 items) | |||
| 1. Spouse | 5.92 | 4.36 | 0.51 |
| 2. Your family members on your side | 4.49 | 3.47 | 0.68 |
| 3. Your family members on your spouse’s side | 3.12 | 2.60 | 0.61 |
| 4. Physicians | 6.01 | 3.65 | 0.75 |
| 5. Health care professionals other than physicians (e.g., nurses, social workers, occupational/physical/speech therapists, psychologists) | 5.82 | 3.72 | 0.74 |
| 6. School teachers | 3.94 | 3.34 | 0.71 |
| 7. Your friends | 3.31 | 2.76 | 0.72 |
| 8. Other parents of children with ASD | 5.13 | 3.70 | 0.61 |
| 9. General public | 2.79 | 2.29 | 0.62 |
| Scale (total score) | 40.54 | 22.14 | |
| Internal Consistency (Cronbach’s α) | 0.89 | ||
| Self-efficacy in Pursuing Genetic Testing for Children with ASD Scale (6 items) | |||
| Response Scale: From 0 (I am not confident at all) to 10 (I am 100% confident) | |||
| How confident are you… | |||
| 1. in finding a time to take your child(ren) with ASD for ASD genetic testing? | 6.34 | 3.08 | 0.50 |
| 2. that you are able to afford to take your child(ren) with ASD for ASD genetic testing? | 3.57 | 3.18 | 0.54 |
| 3. in finding a suitable hospital or doctor to take your child(ren) with ASD for ASD genetic testing? | 4.94 | 3.13 | 0.72 |
| 4. that you can make an appointment with an ASD genetic testing provider to take your child(ren) with ASD for ASD genetic testing? | 4.76 | 3.12 | 0.77 |
| 5. that you can figure out the health insurance for ASD genetic testing | 3.72 | 3.22 | 0.69 |
| 6. that your family members will support you in taking your child(ren) with ASD to undergo genetic testing for ASD? | 6.57 | 2.95 | 0.49 |
| Scale (total score) | 29.91 | 13.91 | |
| Internal consistency (Cronbach’s α) | 0.84 | ||
| Intention in Pursuing Genetic Testing for Children with ASD Scale (6 items) | |||
| Response Scale: (1) Extremely unlikely, (2) Unlikely, (3) Likely, (4) Extremely likely | |||
| How likely are you to… | |||
| 1. organize your time to take your child(ren) with ASD to undergo ASD genetic testing? | 2.67 | 0.92 | 0.83 |
| 2. pay out-of-pocket for ASD genetic testing for your child(ren) with ASD? | 1.80 | 0.83 | 0.54 |
| 3. make an appointment with an ASD genetic testing provider to take your child(ren) with ASD for ASD genetic testing? | 2.36 | 0.86 | 0.81 |
| 4. contact the health insurance company about the cost of ASD genetic testing for your child(ren) with ASD? | 2.39 | 0.95 | 0.75 |
| 5. obtain your family members’ support to take your child(ren) with ASD to undergo ASD genetic testing? | 2.28 | 0.93 | 0.58 |
| 6. take your child(ren) with ASD to undergo ASD genetic testing? | 2.44 | 0.88 | 0.85 |
| Scale (total score) | 13.93 | 4.39 | |
| Internal Consistency (Cronbach’s α) | 0.90 | ||
| Item | Factor 1 | Factor 2 |
|---|---|---|
| Perceived Genetic Cause of ASD Scale (4 items) | ||
| 1. ASD has a genetic factor | 0.70 | |
| 2. ASD is caused by genes | 0.82 | |
| 3. ASD is associated with family history | 0.84 | |
| 4. ASD is an inherited disorder | 0.85 | |
| Total variance explained = 64.80% | 64.80% | |
| Perceived Severity of ASD Scale (6 items) | ||
| 1. ASD is a severe disorder | 0.71 | |
| 2. Individuals with ASD have problems living independently | 0.80 | |
| 3. The public discriminates against individuals with ASD | 0.53 | |
| 4. Individuals with ASD have fewer job opportunities | 0.68 | |
| 5. Compared to a child without ASD, it’s hard to raise a child with ASD | 0.66 | |
| 6. Health problems associated with ASD are severe | 0.60 | |
| Total variance explained = 44.43% | 44.43% | |
| Perceived Benefits of Genetic Testing for ASD Scale (6 items) | ||
| 1. ASD genetic testing identifies the cause of children’s ASD | 0.48 | |
| 2. ASD genetic testing promotes early detection and intervention for children with ASD | 0.82 | |
| 3. ASD genetic testing helps develop treatment plans targeting ASD-associated medical conditions for affected children | 0.83 | |
| 4. ASD genetic testing helps children with ASD make informed family planning decisions | 0.73 | |
| 5. ASD genetic testing helps children with ASD get more social support | 0.71 | |
| 6. Taking children with ASD to undergo ASD genetic testing contributes to ASD research | 0.39 | |
| Total variance explained = 46.14% | 46.14% | |
| Perceived Barriers in Pursuing Genetic Testing for Children with ASD Scale (9 items) | ||
| 1. ASD is not caused by genes | - | - |
| 2. ASD genetic testing cannot improve the current situation of my child(ren) diagnosed with ASD | - | 0.93 |
| 3. My child(ren) has/have already been diagnosed with ASD, so there’s no need to undergo this testing | - | 0.81 |
| 4. Taking my child(ren) with ASD to undergo ASD genetic testing contradicts with my religious or cultural beliefs. | 0.57 | - |
| 5. ASD genetic testing does more harm than good | 0.69 | - |
| 6. ASD genetic testing can cause family conflicts | 0.73 | - |
| 7. The procedure of undergoing ASD genetic testing is uncomfortable for my child (i.e., drawing blood) | 0.48 | - |
| 8. The results of ASD genetic testing can cause public discrimination against my child(ren) with ASD | 0.76 | - |
| 9. The results of ASD genetic testing can put the health insurance status of my child(ren) with ASD in jeopardy | 0.65 | - |
| Total variance explained = 47.29% | 31.16% | 16.13% |
| Attitudes Toward Genetic Testing for ASD Scale (5 items) | ||
| 1. Taking a child with ASD to undergo ASD genetic testing is a good thing | 0.86 | |
| 2. Taking a child with ASD to undergo ASD genetic testing is beneficial | 0.83 | |
| 3. Taking a child with ASD to undergo ASD genetic testing is necessary | 0.89 | |
| 4. All children diagnosed with ASD should undergo ASD genetic testing | 0.92 | |
| 5. All children with ASD characteristics or traits should undergo ASD genetic testing | 0.89 | |
| Total variance explained = 77.12% | 77.12% | |
| Subjective Norms of Genetic Testing for ASD Scale—(9 items) | ||
| 1. Spouse | 0.60 | |
| 2. My family members on my side | 0.76 | |
| 3. My family members on my spouse’s side | 0.69 | |
| 4. Physicians | 0.81 | |
| 5. Health care professionals other than physicians (e.g., nurses, social workers, occupational/physical/speech therapists, psychologists) | 0.81 | |
| 6. School teachers | 0.78 | |
| 7. My friends | 0.80 | |
| 8. Other parents of children with ASD | 0.71 | |
| 9. General public | 0.71 | |
| Total variance explained = 55.37% | 55.37% | |
| Self-efficacy Scale in Pursuing Genetic Testing for Children with ASD (6 items) | ||
| 1. in finding a time to take your child(ren) with ASD for ASD genetic testing? | 0.63 | |
| 2. that you are able to afford to take your child(ren) with ASD for ASD genetic testing? | 0.69 | |
| 3. in finding a suitable hospital or doctor to take your child(ren) with ASD for ASD genetic testing? | 0.84 | |
| 4. that you can make an appointment with an ASD genetic testing provider to take your child(ren) with ASD for ASD genetic testing? | 0.87 | |
| 5. that you can figure out the health insurance for ASD genetic testing | 0.82 | |
| 6. that your family members will support you in taking your child(ren) with ASD to undergo genetic testing for ASD? | 0.62 | |
| Total variance explained = 56.06% | 56.06% | |
| Intention in Pursuing Genetic Testing for Children with ASD Scale (6 items) | ||
| 1. organize your time to take your child(ren) with ASD to undergo ASD genetic testing? | 0.90 | |
| 2. pay out-of-pocket for ASD genetic testing for your child(ren) with ASD? | 0.66 | |
| 3. make an appointment with an ASD genetic testing provider to take your child(ren) with ASD for ASD genetic testing? | 0.89 | |
| 4. contact the health insurance company about the cost of ASD genetic testing for your child(ren) with ASD? | 0.83 | |
| 5. obtain your family members’ support to take your child(ren) with ASD to undergo ASD genetic testing? | 0.69 | |
| 6. take your child(ren) with ASD to undergo ASD genetic testing? | 0.91 | |
| Total variance explained = 67.19% | 67.19% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, S.; Chen, W.-J.; Kwok, O.-M.; Dhar, S.U.; Eble, T.N.; Tseng, T.-S.; Chen, L.-S. Psychometric Properties of the POAGTS: A Tool for Understanding Parents’ Perceptions Regarding Autism Spectrum Disorder Genetic Testing. Int. J. Environ. Res. Public Health 2021, 18, 3323. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063323
Zhao S, Chen W-J, Kwok O-M, Dhar SU, Eble TN, Tseng T-S, Chen L-S. Psychometric Properties of the POAGTS: A Tool for Understanding Parents’ Perceptions Regarding Autism Spectrum Disorder Genetic Testing. International Journal of Environmental Research and Public Health. 2021; 18(6):3323. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063323
Chicago/Turabian StyleZhao, Shixi, Wei-Ju Chen, Oi-Man Kwok, Shweta U. Dhar, Tanya N. Eble, Tung-Sung Tseng, and Lei-Shih Chen. 2021. "Psychometric Properties of the POAGTS: A Tool for Understanding Parents’ Perceptions Regarding Autism Spectrum Disorder Genetic Testing" International Journal of Environmental Research and Public Health 18, no. 6: 3323. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063323