
Observational Study Regarding the Relationship between Nutritional Status, Dental Caries, Mutans Streptococci, and Lactobacillus Bacterial Colonies

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
- -
- Children wearing orthodontic appliances;
- -
- children taking medication;
- -
- children with systemic conditions (gastroesophageal reflux disease, seizure, cancer, celiac disease).
3. Results
4. Discussion
4.1. Practical Application
4.2. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eman, K.C.; Qasim, A. Nutritional status in relation to oral health status among patients attending dental hospital. J. Bagh. Coll. Dent. 2013, 25, 114–119. [Google Scholar]
- Ridhi, N.; Sabyasachi, S.; Jagannath, G.V. Nutritional status and caries experience among 12 to 15 years old school going children of Lucknow. J. Int. Dent. Med. Res. 2012, 5, 30–35. [Google Scholar]
- Alshehri, Y.; Park, J.S.; Kruger, E.; Tennant, M. Association between body mass index and dental caries in the Kingdom of Saudi Arabia: Systematic review. Saudi Dent. J. 2020, 32, 171–180. [Google Scholar] [CrossRef]
- Alshihri, A.A.; Rogers, H.J.; Alqahtani, M.A.; Aldossary, M.S. Association between Dental Caries and Obesity in Children and Young People: A Narrative Review. Int. J. Dent. 2019, 2019, 1–8. [Google Scholar] [CrossRef]
- Alm, A.; Fahraeus, C.; Wendt, L.K. Body adiposity status in teenagers and snacking habits in early childhood in relation to aproximal caries at 15 years of age. Int. J. Paediatr. Dent. 2008, 18, 189–196. [Google Scholar] [CrossRef]
- Bhayat, A.A.; Tamer, M.H.; Al-Shorman, M.; Abu-Naba’a, H.; Bakeer, L.H. Correlating dental caries with oral bacteria and the buffering capacity of saliva in children in Madinah, Saudi Arabia. J. Int. Soc. Prev. Community Dent. 2016, 3, 38–43. [Google Scholar] [CrossRef] [Green Version]
- Köhler, B.; Pettersson, B.-M.; Bratthall, D. Streptococcus mutans in plaque and saliva and the development of caries. Eur. J. Oral Sci. 1981, 89, 19–25. [Google Scholar] [CrossRef]
- Holbrook, W.P.; De Soet, J.J.; De Graaff, J. Prediction of Dental Caries in Pre-School Children. Caries Res. 1993, 27, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, R.J. Mutansstreptococci: Acquistion and transmission. Pediatr. Dent. 2006, 28, 106–109. [Google Scholar] [PubMed]
- Krishnan, K.; Chen, T.; Paster, B.J. A practical guide to the oral microbiome and its relation to health and disease. Oral Dis. 2017, 23, 276–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemos, J.; Palmer, S.; Zeng, L.; Wen, Z.T.; Kajfasz, J.K.; Freires, I.; Abranches, J.; Brady, L. The Biology of Streptococcus mutans. Microbiol. Spectr. 2019, 7, 101128. [Google Scholar] [CrossRef] [PubMed]
- Sansone, C.; Van Houte, J.; Joshipura, K.; Kent, R.; Margolis, H.C. The Association of Mutans Streptococci and Non-Mutans Streptococci Capable of Acidogenesis at a Low pH with Dental Caries on Enamel and Root Surfaces. J. Dent. Res. 1993, 72, 508–516. [Google Scholar] [CrossRef]
- Kolawole, K.A.; Folayan, M.O. Association between malocclusion, caries and oral hygiene in children 6 to 12 years old resident in suburban Nigeria. BMC Oral Health 2019, 19, 262. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Laino, L.; Herford, A.S.; Lauritano, F.; Giudice, G.L.; Famà, F.; Santoro, R.; Troiano, G.; Iannello, G.; et al. Oral Health Impact Profile in Celiac Patients: Analysis of Recent Findings in a Literature Review. Gastroenterol. Res. Pract. 2018, 2018, 7848735. [Google Scholar] [CrossRef]
- Sambataro, S.; Bocchieri, S.; Cervino, G.; La Bruna, R.; Cicciù, A.; Innorta, M.; Torrisi, B.; Cic-ciù, M. Correlations between Malocclusion and Postural Anomalies in Children with Mixed Denti-tion. J. Funct. Morphol. Kinesiol. 2019, 4, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization—Oral Health Surveyes: Basic Methods, France. WHO Libr. Cat. Publ. Data 2013, 5, 1–125.
- Chen, D.; Zhi, Q.; Zhou, Y.; Tao, Y.; Wu, L.; Lin, H. Association between Dental Caries and BMI in Children: A Systematic Review and Meta-Analysis. Caries Res. 2018, 52, 230–245. [Google Scholar] [CrossRef] [PubMed]
- Mummolo, S.; Marchetti, E.; Giuca, M.R.; Gallusi, G.; Tecco, S.; Gatto, R.; Marzo, G. In-office bacteria test for a microbial monitoring during the conventional and self-ligating orthodontic treatment. Head Face Med. 2013, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Arvidsson, L.; Birkhed, D.; Hunsberger, M.; Lanfer, A.; Lissner, L.; Mehlig, K.; Mårild, S.; Eiben, G.; IDEFICS Consortium. BMI, eating habits and sleep in relation to salivary counts of mutans streptococci in children—The IDEFICS Sweden study. Public Health Nutr. 2016, 19, 1088–1092. [Google Scholar] [CrossRef] [Green Version]
- Pannu, P.; Gambhir, R.; Sujlana, A. Correlation between the salivary Streptococcus mutans levels and dental caries experience in adult population of Chandigarh, India. Eur. J. Dent. 2013, 7, 191–195. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention (CDC). BMI Percentile Calculator for Child and Teen. Available online: https://www.cdc.gov/healthyweight/bmi/calculator.html (accessed on 2 January 2021).
- Farsi, D.E.; Heba, M.; Leena, F.; Najat, A.; Sumer, A.; Najlaa, B.; Haneen, M. Prevalence of obesity in elementary school children and its association with dental caries. Saudi Med. J. 2016, 37, 1378–1385. [Google Scholar] [CrossRef] [PubMed]
- Paisi, M.; Kay, E.; Kaimi, I.; Witton, R.; Nelder, R.; Christophi, C.; Lapthorne, D. Obesity and Dental Caries in Young Children in Plymouth, United Kingdom: A Spatial Analysis. Community Dent. Health 2018, 35, 58–64. [Google Scholar] [PubMed]
- Davidson, K.; Schroth, R.J.; Levi, J.A.; Yaffe, A.B.; Mittermuller, B.-A.; Sellers, E.A.C. Higher body mass index associated with severe early childhood caries. BMC Pediatr. 2016, 16, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahraki, T.; Shahraki, M.; Mehr, S.O. Association between Body Mass Index and Caries Frequency among Zahedan Elementary School Children. Int. J. High Risk Behav. Addict. 2013, 2, 122–125. [Google Scholar] [CrossRef] [Green Version]
- Hong, L.; Ahmed, A.; McCunniff, M.; Overman, P.; Mathew, M. Obesity and Dental Caries in Children Aged 2–6 Years in the United States: National Health and Nutrition Examination Survey 1999–2002. J. Public Health Dent. 2008, 68, 227–233. [Google Scholar] [CrossRef]
- Gerdin, E.W.; Angbratt, M.; Aronsson, K.; Eriksson, E.; Johansson, I. Dental caries and body mass index by socio-economic status in Swedish children. Community Dent. Oral Epidemiol. 2008, 36, 459–465. [Google Scholar] [CrossRef]
- Powell, J.C.; Koroluk, L.D.; Phillips, C.L.; Roberts, M.W. Relationship between adjusted body mass index percentile and decayed, missing, and filled primary teeth. J. Dent. Child. 2013, 80, 115–120. [Google Scholar]
- Yao, Y.; Ren, X.; Song, X.; He, L.; Jin, Y.; Chen, Y.; Lu, W.; Guo, D.; Ding, L.; Tang, H.; et al. The relationship between dental caries and obesity among primary school children aged 5 to 14 years. Nutr. Hosp. 2014, 30, 60–65. [Google Scholar] [PubMed]
- Tilinca, M.C.; Barabas-Hajdu, E.C.; Ferencz, G.T.; Nemes-Nagy, E. Involvement of inflammatory cytokines in obesity and its complications. Rev. Romana Med. Lab. 2018, 26, 359–371. [Google Scholar] [CrossRef] [Green Version]
- Elangovan, A.; Mungara, J.; Joseph, E. Exploring the relation between body mass index, diet, and dental caries among 6-12-year-old children. J. Indian Soc. Pedod. Prev. Dent. 2012, 30, 293–300. [Google Scholar] [CrossRef]
- Bimstein, E.; Katz, J. Obesity in Children: A Challenge that Pediatric Dentistry Should not Ignore—Review of the Literature. J. Clin. Pediatr. Dent. 2009, 34, 103–106. [Google Scholar] [CrossRef]
- Köksal, E.; Tekçiçek, M.; Yalçın, S.S.; Tuğrul, B.; Yalçın, S.; Pekcan, G. Association between anthropometric measurements and dental caries in Turkish school children. Cent. Eur. J. Public Health 2011, 19, 147–151. [Google Scholar] [CrossRef] [Green Version]
- Sudhakar, K.; Shanthi, P.R.; Fareed, N.; Sudhir, K.M. Relationship between Dentition Status and Body Mass Index among 5 to 15 year old group of children of an orphanage in Nellore city. J. Indian Assoc. Public Health Dent. 2010, 15, 45–49. [Google Scholar]
- Sheller, B.; Churchill, S.S.; Williams, B.J.; Davidson, B. Body mass index of children with severe early childhood caries. Pediatr. Dent. 2009, 31, 216–221. [Google Scholar]
- Benzian, H.; Monse, B.; Heinrich-Weltzien, R.; Hobdell, M.; Mulder, J.; Helderman, W.V.P. Untreated severe dental decay: A neglected determinant of low Body Mass Index in 12-year-old Filipino children. BMC Public Health 2011, 11, 558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bafti, L.S.; Hashemipour, M.A.; Poureslami, H.; Hoseinian, Z. Relationship between Body Mass Index and Tooth Decay in a Population of 3–6-Year-Old Children in Iran. Int. J. Dent. 2015, 2015, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Perez, L.; Irigoyen, M.E.; Zepeda, M. Dental caries, tooth eruption timing and obesity: A longitudinal study in a group of Mexican school children. Acta Odontol. Scand. 2010, 68, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Araujo, D.S.; Klein, M.I.; Scudine, K.G.D.O.; Leite, L.D.S.; Parisotto, T.M.; Ferreira, C.M.; Fonseca, F.L.A.; Perez, M.M.; Castelo, P.M. Salivary Microbiological and Gingival Health Status Evaluation of Adolescents With Overweight and Obesity: A Cluster Analysis. Front. Pediatr. 2020, 8, 429. [Google Scholar] [CrossRef] [PubMed]
- Freitas, C.N.; Castelo, P.M.; Sousa, K.G.; Alonso, G.C.; Fonseca, F.; Klein, M.; Barbosa, T. Educational strategies and atraumatic restorative treatment effect on salivary characteristics: A controlled clinical trial. Oral Dis. 2017, 23, 1116–1126. [Google Scholar] [CrossRef]
- Goodson, J.M.; Groppo, D.; Halem, S.; Carpino, E. Is Obesity an Oral Bacterial Disease? J. Dent. Res. 2009, 88, 519–523. [Google Scholar] [CrossRef]
- Barkeling, B.; Linné, Y.; Lindroos, A.K.; Birkhed, D.; Rooth, P.; Rössner, S. Intake of sweet foods and counts of cariogenic microorganisms in relation to body mass index and psychometric variables in women. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 1239–1244. [Google Scholar] [CrossRef] [Green Version]
- Lalloo, R.; Tadakamadla, S.K.; Kroon, J.; Tut, O.; Kularatna, S.; Boase, R.; Kapellas, K.; Gilchrist, D.; Cobbledick, E.; Rogers, J.; et al. Salivary characteristics and dental caries experience in remote Indigenous children in Australia: A cross-sectional study. BMC Oral Health 2019, 19, 21. [Google Scholar] [CrossRef] [PubMed]
- Ndanu, T.A.; Aryeetey, R.; Sackeyfio, J.; Otoo, G.; Lartey, A. Streptococcus mutans and Lactobacillus Species Infection in Obese and Non-Obese School Children in Accra, Ghana. J. Obes. Overweight 2015, 1, 1. [Google Scholar] [CrossRef]
- Raju, S.C.; Lagström, S.; Ellonen, P.; De Vos, W.M.; Eriksson, J.G.; Weiderpass, E.; Rounge, T.B. Gender-Specific Associations Between Saliva Microbiota and Body Size. Front. Microbiol. 2019, 10, 767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nur, L.H.; Jain, R.K.; Duraisamy, R. Prevalence and associated factors for dental caries in school children with malloclussion. Eur. J. Mol. Clin. Med. 2020, 7, 1952–1963. [Google Scholar]
- Jürgensen, N.; Petersen, P.E. Oral health and the impact of socio-behavioural factors in a cross-sectional survey of 12-year old school children in Laos. BMC Oral Health 2009, 9, 29. [Google Scholar] [CrossRef] [Green Version]
- Masmoudi Baccouche, F.; Sebai, A.; Ouanane, M.A.; Baaziz, M.; Maatouk, F. Relationship between Dental Caries and Body Mass Index in Tunisian Children. Int. Ann. Med. 2017, 1. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nutritional Status | BMI Percentile Range |
|---|---|
| Obesity | BMI ≥ percentile 95 |
| Overweight | 85 ≤ BMI < percentile 95 |
| Normal weigh | 5 ≤ BMI< percentile 85 |
| Underweight | BMI < percentile 5 |
| Group 1 <5th Percentile, n = 10 | Group 2 5th to 85th Percentile, n = 117 | Group 3 85th to 95th Percentile, n = 27 | p-Value | ||
|---|---|---|---|---|---|
| Sex | M | 2 | 53 | 11 | 0.29 |
| F | 8 | 64 | 16 | ||
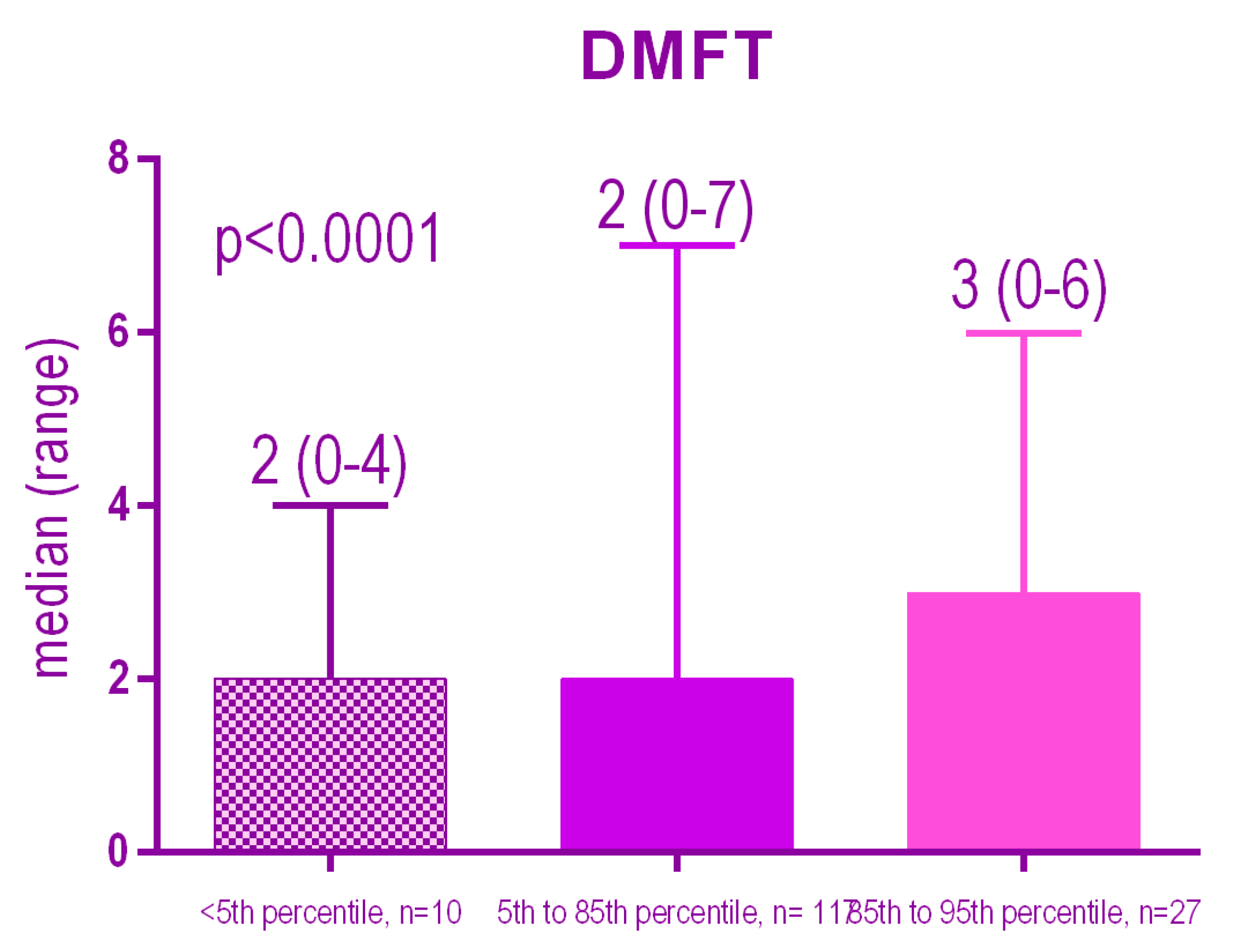
| DMFT | 0 | 0 | 39 | 1 | <0.0001 |
| 1–3 | 7 | 73 | 15 | ||
| 4–6 | 2 | 5 | 11 | ||
| >6 | 0 | 2 | 6 | ||
| Total | 21 | 165 | 86 | <0.0001 | |
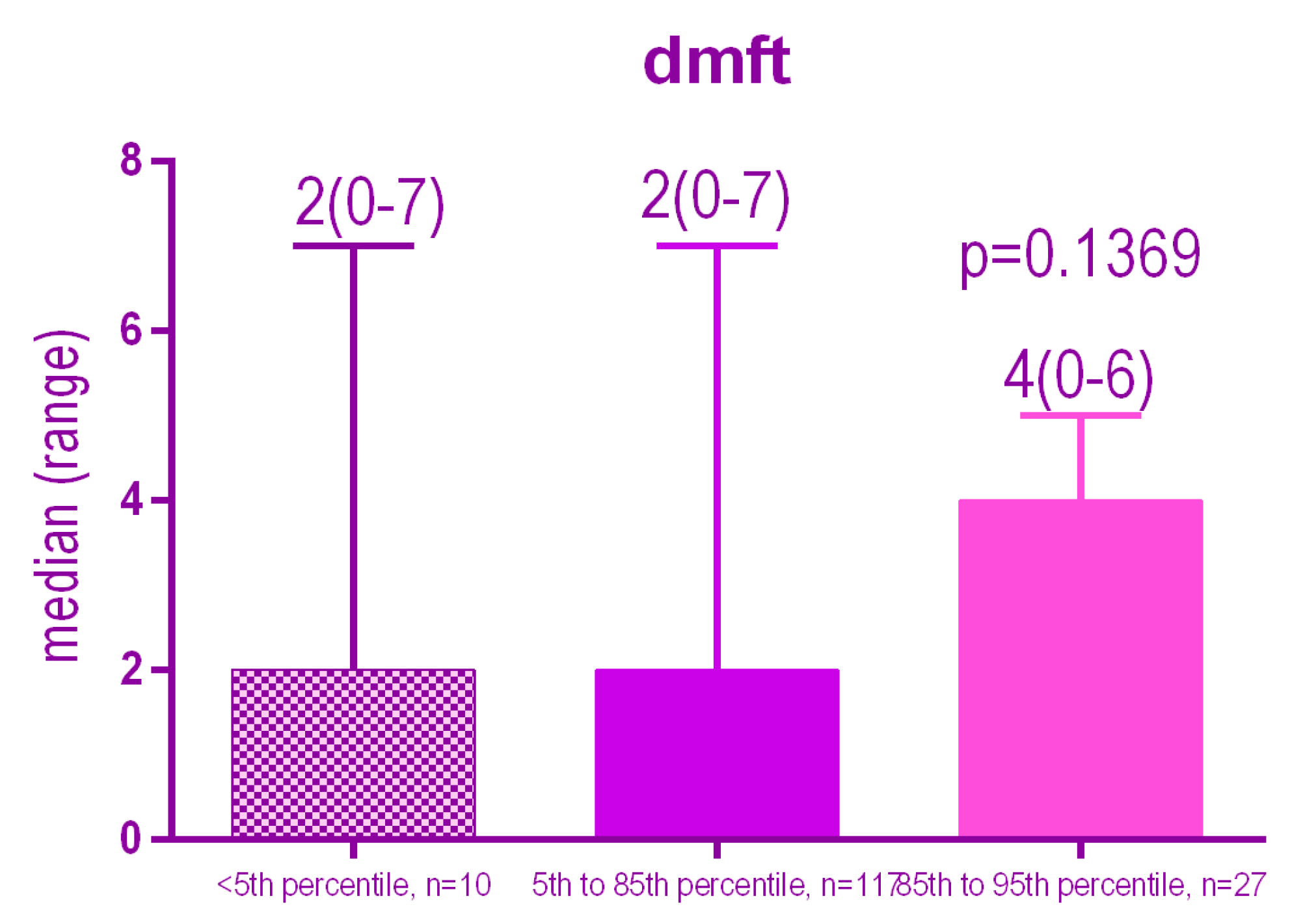
| Dmft | 0 | 2 | 34 | 4 | <0.0001 |
| 1–3 | 6 | 66 | 5 | ||
| 4–6 | 1 | 15 | 18 | ||
| >6 | 1 | 2 | 0 | ||
| Total | 24 | 214 | 31 | 0.1369 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bud, E.S.; Bica, C.I.; Stoica, O.E.; Vlasa, A.; Eșian, D.; Bucur, S.-M.; Bud, A.; Chibelean, M.; Păcurar, M. Observational Study Regarding the Relationship between Nutritional Status, Dental Caries, Mutans Streptococci, and Lactobacillus Bacterial Colonies. Int. J. Environ. Res. Public Health 2021, 18, 3551. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073551
Bud ES, Bica CI, Stoica OE, Vlasa A, Eșian D, Bucur S-M, Bud A, Chibelean M, Păcurar M. Observational Study Regarding the Relationship between Nutritional Status, Dental Caries, Mutans Streptococci, and Lactobacillus Bacterial Colonies. International Journal of Environmental Research and Public Health. 2021; 18(7):3551. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073551
Chicago/Turabian StyleBud, Eugen Silviu, Cristina Ioana Bica, Oana Elena Stoica, Alexandru Vlasa, Daniela Eșian, Sorana-Maria Bucur, Anamaria Bud, Manuela Chibelean, and Mariana Păcurar. 2021. "Observational Study Regarding the Relationship between Nutritional Status, Dental Caries, Mutans Streptococci, and Lactobacillus Bacterial Colonies" International Journal of Environmental Research and Public Health 18, no. 7: 3551. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073551