
Effectiveness of an Intervention Aimed at Improving Information for Patients with High Cardiovascular Risk: INFORISK Clinical Trial

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Description of Baseline Characteristics
3.2. End of Follow-Up Analysis
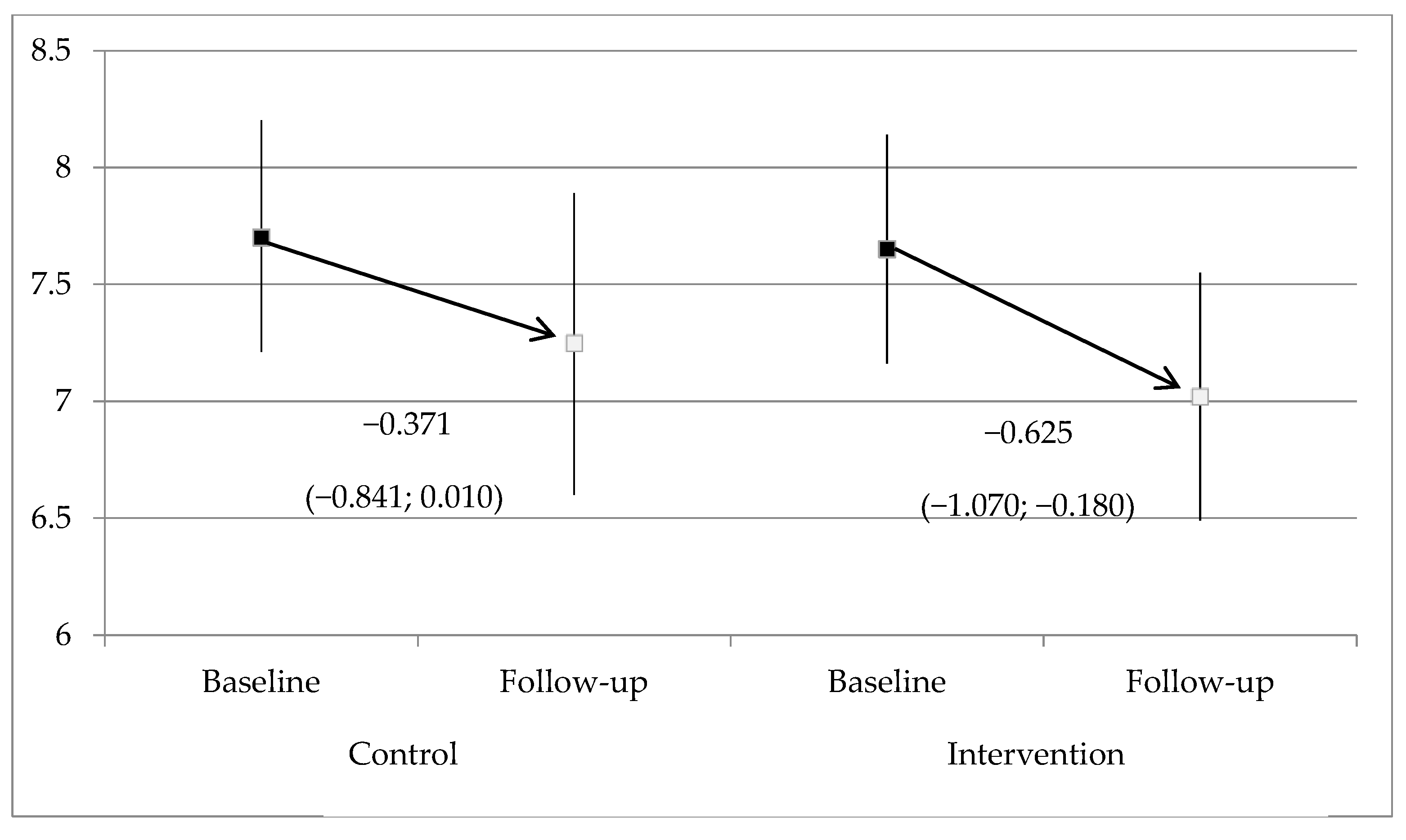
3.3. Impact of the Intervention
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 74, e177–e232. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Abreu, A.; Albus, C.; Ambrosetti, M.; Brotons, C.; Catapano, A.L.; Corra, U.; Cosyns, B.; Deaton, C.; Graham, I.; et al. Update on cardiovascular prevention in clinical practice: A position paper of the European Association of Preventive Cardiology of the European Society of Cardiology. Eur. J. Prev. Cardiol. 2020, 27, 181–205. [Google Scholar] [CrossRef] [Green Version]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2889–2934, Erratum in 2015, 66, 2812. [Google Scholar] [CrossRef] [Green Version]
- Conroy, R.M.; Pyörälä, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetière, P.; Jousilahti, P.; Keil, U.; et al. SCORE project group. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.C., Jr.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129 (Suppl. S2), S49–S73, Erratum in 2014, 129, S74–S75. [Google Scholar] [CrossRef] [Green Version]
- Wilson, P.W.F.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of coronary heart disease using risk factor categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef] [Green Version]
- Marrugat, J.; Solanas, P.; D’Agostino, R.; Sullivan, L.; Ordovas, J.; Cordón, F.; Ramos, R.; Sala, J.; Masià, R.; Rohlfs, I.; et al. Estimación del riesgo coronario en España mediante la ecuación de Framingham calibrada Coronary risk estimation in Spain using a calibrated Framingham function. Rev. Esp. Cardiol. 2003, 56, 253–261. [Google Scholar] [CrossRef]
- Cooney, M.T.; Dudina, A.; D’agostino, R.; Graham, I.M. Risk Prediction in Cardiovascular Medicine Cardiovascular Risk-Estimation Systems in Primary Prevention Do They Differ? Do They Make a Difference? Can We See the Future? The Rationale for CVD Risk Estimation A Comparison of Current CVD Risk-Estimation Systems. Published online 2010. Circulation 2010, 122, 300–310. [Google Scholar]
- Neuner-Jehle, S.; Senn, O.; Wegwarth, O.; Rosemann, T.; Steurer, J. How do family physicians communicate about cardiovascular risk? Frequencies and determinants of different communication formats. BMC Fam. Pract. 2011, 12, 15. [Google Scholar] [CrossRef] [Green Version]
- Overview Cardiovascular Disease: Risk Assessment and Reduction, Including Lipid Modification Guidance NICE. Available online: https://www.nice.org.uk/guidance/cg181 (accessed on 30 November 2020).
- Brotons, C.; Lobos, J.M.; Royo-Bordonada, M.Á.; Maiques, A.; de Santiago, A.; Castellanos, Á.; Diaz, S.; Obaya, J.C.; Pedro-Botet, J.; Moral, I.; et al. Implementation of Spanish adaptation of the European guidelines on cardiovascular disease prevention in primary care. BMC Fam. Pract. 2013, 14, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipkus, I.M.; Samsa, G.; Rimer, B.K. General performance on a numeracy scale among highly educated samples. Med. Decis. Mak. 2001, 21, 37–44. [Google Scholar] [CrossRef]
- Samsa, G.P.; Cohen, S.J.; Goldstein, L.B.; Bonito, A.J.; Duncan, P.W.; Enarson, C.; DeFriese, G.H.; Horner, R.D.; Matchar, D.B. Knowledge of risk among patients at increased risk for stroke. Stroke 1997, 28, 916–921. [Google Scholar] [CrossRef]
- van der Weijden, T.; van Steenkiste, B.; Stoffers, H.E.J.H.; Timmermans, D.R.M.; Grol, R. Primary Prevention of Cardiovascular Diseases in General Practice: Mismatch between Cardiovascular Risk and Patients’ Risk Perceptions. Med. Decis. Mak. 2007, 27, 754–761. [Google Scholar] [CrossRef] [PubMed]
- Koelewijn-van Loon, M.S.; van der Weijden, T.; Ronda, G.; van Steenkiste, B.; Winkens, B.; Elwyn, G.; Grol, R. Improving lifestyle and risk perception through patient involvement in nurse-led cardiovascular risk management: A cluster-randomized controlled trial in primary care. Prev. Med. 2010, 50, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Edwards, A.; Thomas, R.; Williams, R.; Ellner, A.L.; Brown, P.; Elwyn, G. Presenting risk information to people with diabetes: Evaluating effects and preferences for different formats by a web-based randomised controlled trial. Patient Educ. Couns. 2006, 63, 336–349. [Google Scholar] [CrossRef] [PubMed]
- Krones, T.; Keller, H.; Sönnichsen, A.; Sadowski, E.M.; Baum, E.; Wegscheider, K.; Rochon, J.; Donner-Banzhoff, N. Absolute cardiovascular disease risk and shared decision making in primary care: A randomized controlled trial. Ann. Fam. Med. 2008, 6, 218–227. [Google Scholar] [CrossRef] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Hippisley-Cox, J.; Coupland, C.; Brindle, P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: Prospective cohort study. BMJ 2017, 357, j2099. [Google Scholar] [CrossRef] [Green Version]
- Hwang, W.J.; Kang, S.J. Interventions to Reduce the Risk of Cardiovascular Disease among Workers: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 2267. [Google Scholar] [CrossRef] [Green Version]
- Byrne, J.L.; Dallosso, H.M.; Rogers, S.; Gray, L.J.; Waheed, G.; Patel, P.; Gupta, P.; Doherty, Y.; Davies, M.J.; Khunti, K. Effectiveness of the Ready to Reduce Risk (3R) complex intervention for the primary prevention of cardiovascular disease: A pragmatic randomised controlled trial. BMC Med. 2020, 18, 198. [Google Scholar] [CrossRef]
- Sheridan, S.L.; Viera, A.J.; Krantz, M.J.; Ice, C.L.; Steinman, L.E.; Peters, K.E.; Kopin, L.A.; Lungelow, D. Cardiovascular Health Intervention Research and Translation Network Work Group on Global Coronary Heart Disease Risk. The effect of giving global coronary risk information to adults: A systematic review. Arch. Intern. Med. 2010, 170, 230–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zipkin, D.A.; Umscheid, C.A.; Keating, N.L.; Allen, E.; Aung, K.; Beyth, R.; Kaatz, S.; Mann, D.M.; Sussman, J.B.; Korenstein, D.; et al. Evidence-based risk communication: A systematic review. Ann. Intern. Med. 2014, 161, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Gonzalez, A.A.; Aguilo, A.; Frontera, M.; Bennasar-Veny, M.; Campos, I.; Vicente-Herrero, T.; Tomas-Salva, M.; De Pedro-Gomez, J.; Tauler, P. Effectiveness of the Heart Age tool for improving modifiable cardiovascular risk factors in a Southern European population: A randomized trial. Eur. J. Prev. Cardiol. 2015, 22, 389–396. [Google Scholar] [CrossRef]


{kind=link}
| KERRYPNX | Study Group | Total (n = 464) | p-Value | |
|---|---|---|---|---|
| Control (n = 236) | Intervention (n = 228) | |||
| Education level, n (%) | 0.775 | |||
| No studies | 4 (1.69%) | 3 (1.32%) | 7 (1.51%) | |
| Primary | 63 (26.69%) | 68 (29.82%) | 131 (28.23%) | |
| Secondary | 91 (38.56%) | 81 (35.53%) | 172 (37.07%) | |
| University/higher degree | 77 (32.63%) | 76 (33.33%) | 153 (32.97%) | |
| Employment status, n (%) | 0.902 | |||
| Self-employed | 28 (11.86%) | 22 (9.65%) | 50 (10.78%) | |
| Employed worker | 69 (29.24%) | 72 (31.58%) | 141 (30.39%) | |
| Unemployed | 18 (7.63%) | 14 (6.14%) | 32 (6.90%) | |
| Retired | 99 (41.95%) | 97 (42.54%) | 196 (42.24%) | |
| Others | 20 (8.47%) | 22 (9.65%) | 42 (9.05%) | |
| Hypertension, n (%) | 173 (73.31%) | 161 (70.61%) | 334 (71.98%) | 0.374 |
| Antihypertensive treatment, n (%) | 157 (66.53%) | 147 (64.47%) | 304 (65.52%) | 0.642 |
| Dyslipidemia, n (%) | 171 (72.46%) | 175 (76.75%) | 346 (74.57%) | 0.112 |
| Lipid-lowering treatment, n (%) | 139 (58.90%) | 138 (60.53%) | 277 (59.70%) | 0.721 |
| Type 2 diabetes, n (%) | 160 (67.80%) | 160 (70.18%) | 320 (68.97%) | 0.242 |
| Hypoglycemic agents, n (%) | 146 (61.86%) | 145 (63.60%) | 291 (62.72%) | 0.700 |
| Antiplatelet, n (%) | 43 (18.22%) | 29 (12.72%) | 72 (15.52%) | 0.102 |
| Mean (SD) [n] | Group | Inter-Group p-Value | |||
|---|---|---|---|---|---|
| Control | Intervention | ||||
| Baseline | End of Follow-Up | Baseline | End of Follow-Up | ||
| SBP (mmHg) | 138.08 (15.23) [n = 235] | 136.80 (14.99) [n = 185] | 138.16 (15.14) [n = 228] | 135.04 (14.42) [n = 192] | 0.139 |
| Intra-group p-value | 0.328 | 0.003 | |||
| DBP (mmHg) | 81.49 (10.42) [n = 235] | 79.64 (8.99) [n = 182] | 81.79 (10.23) [n = 228] | 80.06 (9.12) [n = 191] | 0.721 |
| Intra-group p-value | 0.021 | 0.023 | |||
| BMI (kg/m2) | 31.05 (5.32) [n = 233] | 31.09 (5.92) [n = 164] | 31.06 (5.99) [n = 227] | 30.72 (5.80) [n = 183] | 0.361 |
| Intra-group p-value | 0.364 | 0.047 | |||
| Abdominal circumference (cm) | 107.29 (13.39) [n = 233] | 106.68 (13.50) [n = 167] | 107.13 (13.62) [n = 227] | 105.89 (13.61) [n = 178] | 0.317 |
| Intra-group p-value | 0.381 | 0.001 | |||
| Total cholesterol (mg/dL) | 206.88 (43.20) [n = 234] | 197.38 (44.23) [n = 201] | 203.77 (40.41) [n = 223] | 199.75 (41.83) [n = 204] | 0.356 |
| Intra-group p-value | <0.001 | 0.190 | |||
| HDL-c (mg/dL) | 55.31 (19.52) [n = 231] | 53.29 (17.91) [n = 199] | 53.27 (15.63) [n = 215] | 50.69 (14.44) [n = 203] | 0.192 |
| Intra-group p-value | 0.018 | 0.024 | |||
| LDL-c (mg/dL) | 121.48 (39.30) [n = 229] | 115.37 (37.42) [n = 194] | 119.67 (35.23) [n = 213] | 118.79 (35.58) [n = 195] | 0.300 |
| Intra-group p-value | 0.010 | 0.748 | |||
| Triglycerides (mg/dL) | 181.43 (111.67) [n = 232] | 175.55 (149.35) [n = 195] | 188.88 (139.06) [n = 219] | 164.83 (118.30) [n = 197] | 0.454 |
| Intra-group p-value | 0.930 | 0.094 | |||
| Blood glucose (mg/dL) | 134.05 (56.58) [n = 234] | 130.85 (55.17) [n = 194] | 128.96 (46.32) [n = 222] | 128.38 (43.14) [n = 191] | 0.641 |
| Intra-group p-value | 0.388 | 0.845 | |||
| [N] n (%) | Study Group | Inter-Group p-Value | |||
|---|---|---|---|---|---|
| Control | Intervention | ||||
| Baseline | Follow-Up | Baseline | Follow-Up | ||
| Adherence to the Mediterranean diet Low Moderate High | [N = 235] 47 (20.00%) 160 (68.09%) 28 (11.91%) | [N = 170] 24 (14.12%) 128 (75.29%) 18 (10.59%) | [N = 227] 47 (20.70%) 161 (70.93%) 19 (8.37%) | [N = 181] 21 (11.60%) 131 (72.38%) 29 (16.02%) | 0.115 |
| Intra-group p-value | 0.463 | <0.001 | |||
| Degree of physical activity Low Moderate Vigorous | [N = 235] 84 (35.74%) 125 (53.19%) 26 (11.06%) | [N = 170] 66 (38.82%) 84 (49.41%) 20 (11.76%) | [N = 227] 80 (35.24%) 116 (51.10%) 31 (13.66%) | [N = 181] 74 (40.88%) 84 (46.41%) 23 (12.71%) | 0.827 |
| Intra-group p-value | 0.636 | 0.151 | |||
| Adherence to treatment High Moderate-high Moderate-low Low-moderate Low | [N = 226] 143 (63.27%) 70 (30.97%) 8 (3.54%) 4 (1.77%) 1 (0.44%) | [N = 156] 126 (80.77%) 21 (13.46%) 4 (2.56%) 1 (0.64%) 4 (2.56%) | [N = 218] 129 (59.17%) 68 (31.19%) 17 (7.80%) 3 (1.38%) 1 (0.46%) | [N = 163] 133 (81.60%) 24 (14.72%) 5 (3.07%) 0 (0%) 1 (0.61%) | 0.689 |
| Intra-group p-value | 0.002 | <0.001 | |||
| Smoking habit, n (%) Non-smoker Former smoker (<1 year) Former smoker (≥1 year) Smoker | 93 (39.41%) 5 (2.12%) 64 (27.12%) 74 (31.36%) | 78 (42.16%) 3 (1.62%) 48 (25.95%) 56 (30.27%) | 63 (27.63%) 8 (3.52%) 77 (33.92%) 79 (34.80%) | 55 (28.80%) 5 (2.62%) 71 (37.17%) 60 (31.41%) | 0.609 |
| Intra-group p-value | 0.206 | 0.131 | |||
| Alcohol intake, n (%) | 120 (50.85%) | 78 (45.88%) | 134 (59.03%) | 82 (44.57%) | 0.979 |
| Intra-group p-value | 0.052 | <0.001 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brotons, C.; Moral, I.; Fernández, D.; Puig, M.; Vilella, M.T.; Puig, T.; Cuixart, L.; Férriz, G.; Pedro, A.M.; Codinachs, R.; et al. Effectiveness of an Intervention Aimed at Improving Information for Patients with High Cardiovascular Risk: INFORISK Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 3621. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073621
Brotons C, Moral I, Fernández D, Puig M, Vilella MT, Puig T, Cuixart L, Férriz G, Pedro AM, Codinachs R, et al. Effectiveness of an Intervention Aimed at Improving Information for Patients with High Cardiovascular Risk: INFORISK Clinical Trial. International Journal of Environmental Research and Public Health. 2021; 18(7):3621. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073621
Chicago/Turabian StyleBrotons, Carlos, Irene Moral, Diana Fernández, Mireia Puig, M. Teresa Vilella, Teresa Puig, LLuís Cuixart, Gemma Férriz, Anna M. Pedro, Roger Codinachs, and et al. 2021. "Effectiveness of an Intervention Aimed at Improving Information for Patients with High Cardiovascular Risk: INFORISK Clinical Trial" International Journal of Environmental Research and Public Health 18, no. 7: 3621. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073621