
Arthroscopic Rotator Cuff Repair Improves Sleep Disturbance and Quality of Life: A Prospective Study

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Piper, C.C.; Hughes, A.J.; Ma, Y.; Wang, H.; Neviaser, A.S. Operative versus nonoperative treatment for the management of full-thickness rotator cuff tears: A systematic review and meta-analysis. J. Shoulder Elb. Surg. 2018, 27, 572–576. [Google Scholar] [CrossRef] [PubMed]
- Teunis, T.; Lubberts, B.; Reilly, B.T.; Ring, D. A systematic review and pooled analysis of the prevalence of rotator cuff disease with increasing age. J. Shoulder Elb. Surg. 2014, 23, 1913–1921. [Google Scholar] [CrossRef] [PubMed]
- Serbest, S.; Tiftikçi, U.; Askın, A.; Yaman, F.; Alpua, M. Preoperative and post-operative sleep quality evaluation in rotator cuff tear patients. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 2109–2113. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Salvatore, G.; Rizzello, G.; Berton, A.; Ciuffreda, M.; Candela, V.; Denaro, V. The burden of rotator cuff surgery in Italy: A nationwide registry study. Arch. Orthop. Trauma Surg. 2017, 137, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef] [PubMed]
- Khazzam, M.S.; Mulligan, E.P.; Brunette-Christiansen, M.; Shirley, Z. Sleep Quality in Patients With Rotator Cuff Disease. J. Am. Acad. Orthop. Surg. 2018, 26, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Kunze, K.N.; Movasagghi, K.; Rossi, D.M.; Polce, E.M.; Cohn, M.R.; Karhade, A.V.; Chahla, J. Systematic Review of Sleep Quality Before and After Arthroscopic Rotator Cuff Repair: Are Improvements Experienced and Maintained? Orthop. J. Sports Med. 2020, 8, 2325967120969224. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Facchinetti, G.; Marchetti, A.; Candela, V.; Risi Ambrogioni, L.; Faldetta, A.; De Marinis, M.G.; Denaro, V. Sleep Disturbance and Rotator Cuff Tears: A Systematic Review. Medicina (Kaunas) 2019, 55, 453. [Google Scholar] [CrossRef] [Green Version]
- Somerson, J.S.; Hsu, J.E.; Gorbaty, J.D.; Gee, A.O. Classifications in Brief: Goutallier Classification of Fatty Infiltration of the Rotator Cuff Musculature. Clin. Orthop. Relat. Res. 2016, 474, 1328–1332. [Google Scholar] [CrossRef] [Green Version]
- Lädermann, A.; Burkhart, S.S.; Hoffmeyer, P.; Neyton, L.; Collin, P.; Yates, E.; Denard, P.J. Classification of full-thickness rotator cuff lesions: A review. EFORT Open Rev. 2016, 1, 420–430. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; King, J.B.; Denaro, V.; Maffulli, N. Double-bundle arthroscopic reconstruction of the anterior cruciate ligament: Does the evidence add up? J. Bone Jt. Surg. Br. 2008, 90, 995–999. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Buchmann, S.; Franceschetti, E.; Maffulli, N.; Denaro, V. A systematic review of single-bundle versus double-bundle anterior cruciate ligament reconstruction. Br. Med. Bull. 2012, 103, 147–168. [Google Scholar] [CrossRef]
- Berton, A.; De Salvatore, S.; Candela, V.; Cortina, G.; Lo Presti, D.; Massaroni, C.; Petrillo, S.; Denaro, V. Delayed Rehabilitation Protocol after Rotator Cuff Repair. Osteology 2021, 1, 29–38. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Curcio, G.; Tempesta, D.; Scarlata, S.; Marzano, C.; Moroni, F.; Rossini, P.M.; Ferrara, M.; De Gennaro, L. Validity of the Italian version of the Pittsburgh Sleep Quality Index (PSQI). Neurol. Sci. 2013, 34, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Apolone, G.; Mosconi, P. The Italian SF-36 Health Survey: Translation, validation and norming. J. Clin. Epidemiol. 1998, 51, 1025–1036. [Google Scholar] [CrossRef]
- Godfrey, J.; Hamman, R.; Lowenstein, S.; Briggs, K.; Kocher, M. Reliability, validity, and responsiveness of the simple shoulder test: Psychometric properties by age and injury type. J. Shoulder Elb. Surg. 2007, 16, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Michener, L.A.; McClure, P.W.; Sennett, B.J. American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, patient self-report section: Reliability, validity, and responsiveness. J. Shoulder Elb. Surg. 2002, 11, 587–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawson, J.; Rogers, K.; Fitzpatrick, R.; Carr, A. The Oxford shoulder score revisited. Arch. Orthop. Trauma Surg. 2009, 129, 119–123. [Google Scholar] [CrossRef]
- Cho, C.H.; Song, K.S.; Hwang, I.; Warner, J.J. Does Rotator Cuff Repair Improve Psychologic Status and Quality of Life in Patients With Rotator Cuff Tear? Clin. Orthop. Relat. Res. 2015, 473, 3494–3500. [Google Scholar] [CrossRef] [Green Version]
- Horneff, J.G.; Tjoumakaris, F.; Wowkanech, C.; Pepe, M.; Tucker, B.; Austin, L. Long-term Correction in Sleep Disturbance Is Sustained After Arthroscopic Rotator Cuff Repair. Am. J. Sports Med. 2017, 45, 1670–1675. [Google Scholar] [CrossRef] [PubMed]
- Austin, L.; Pepe, M.; Tucker, B.; Ong, A.; Nugent, R.; Eck, B.; Tjoumakaris, F. Sleep disturbance associated with rotator cuff tear: Correction with arthroscopic rotator cuff repair. Am. J. Sports Med. 2015, 43, 1455–1459. [Google Scholar] [CrossRef] [PubMed]
- Maestroni, L.; Marelli, M.; Gritti, M.; Civera, F.; Rabey, M. Is rotator cuff related shoulder pain a multidimensional disorder? An exploratory study. Scand. J. Pain 2020, 20, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Werner, C.M.; Ossendorf, C.; Meyer, D.C.; Blumenthal, S.; Gerber, C. Subacromial pressures vary with simulated sleep positions. J. Shoulder Elb. Surg. 2010, 19, 989–993. [Google Scholar] [CrossRef] [PubMed]
- Holdaway, L.A.; Hegmann, K.T.; Thiese, M.S.; Kapellusch, J. Is sleep position associated with glenohumeral shoulder pain and rotator cuff tendinopathy: A cross-sectional study. BMC Musculoskelet. Disord. 2018, 19, 408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gumina, S.; Candela, V.; Passaretti, D.; Venditto, T.; Mariani, L.; Giannicola, G. Sleep quality and disturbances in patients with different-sized rotator cuff tear. Musculoskelet. Surg. 2016, 100, 33–38. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preoperative | One Month | Three Months | Six Months | p-Value | |
|---|---|---|---|---|---|
| PSQI | 7.19 ± 3.91 | 6.34 ± 4.01 | 4.67 ± 3.31 | 3.81 ± 3.32 | <0.001 * |
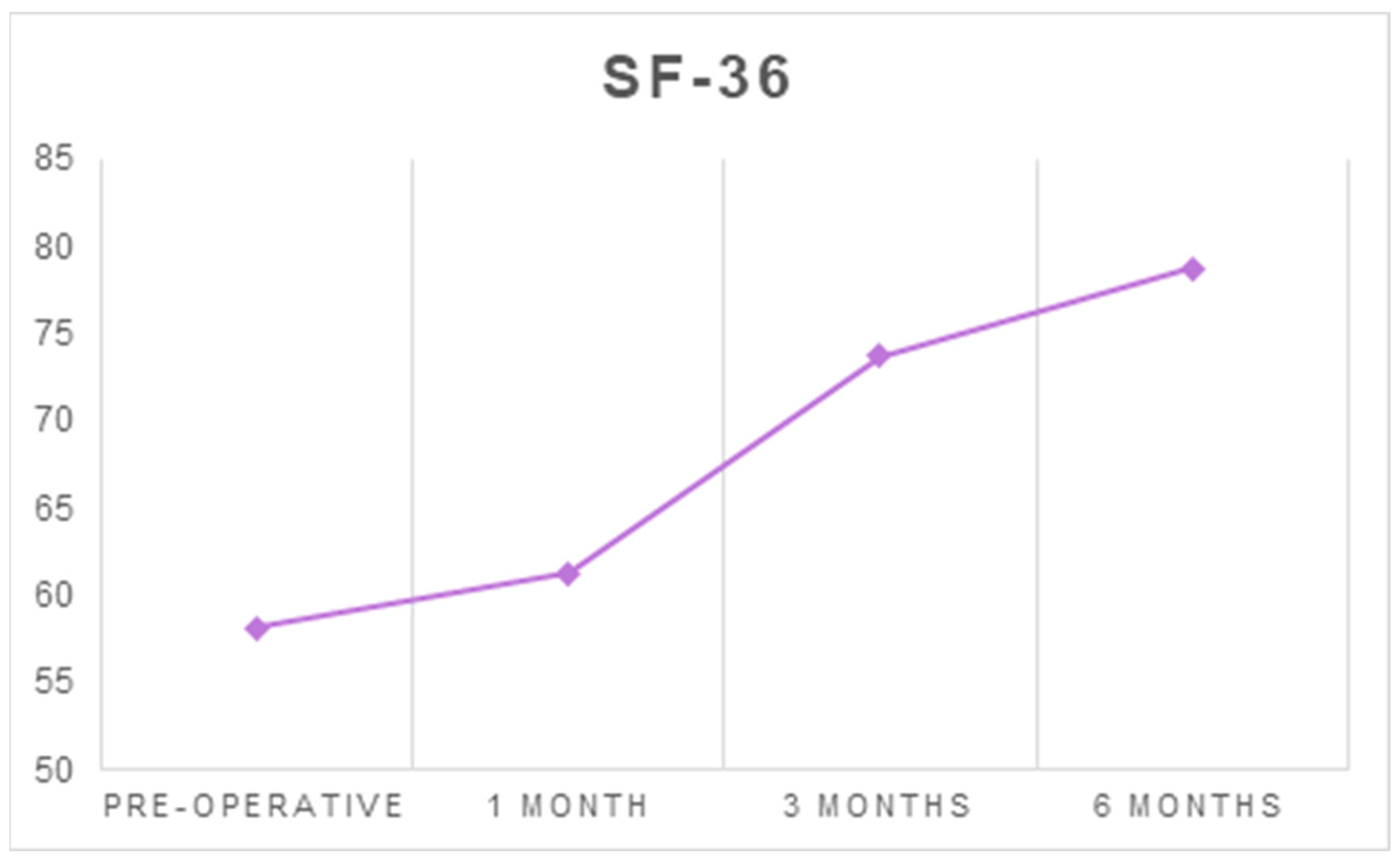
| SF-36 | 58.15 ± 17.35 | 61.26 ± 14.69 | 73.68 ± 15.01 | 78.75 ± 14.9 | <0.001 * |
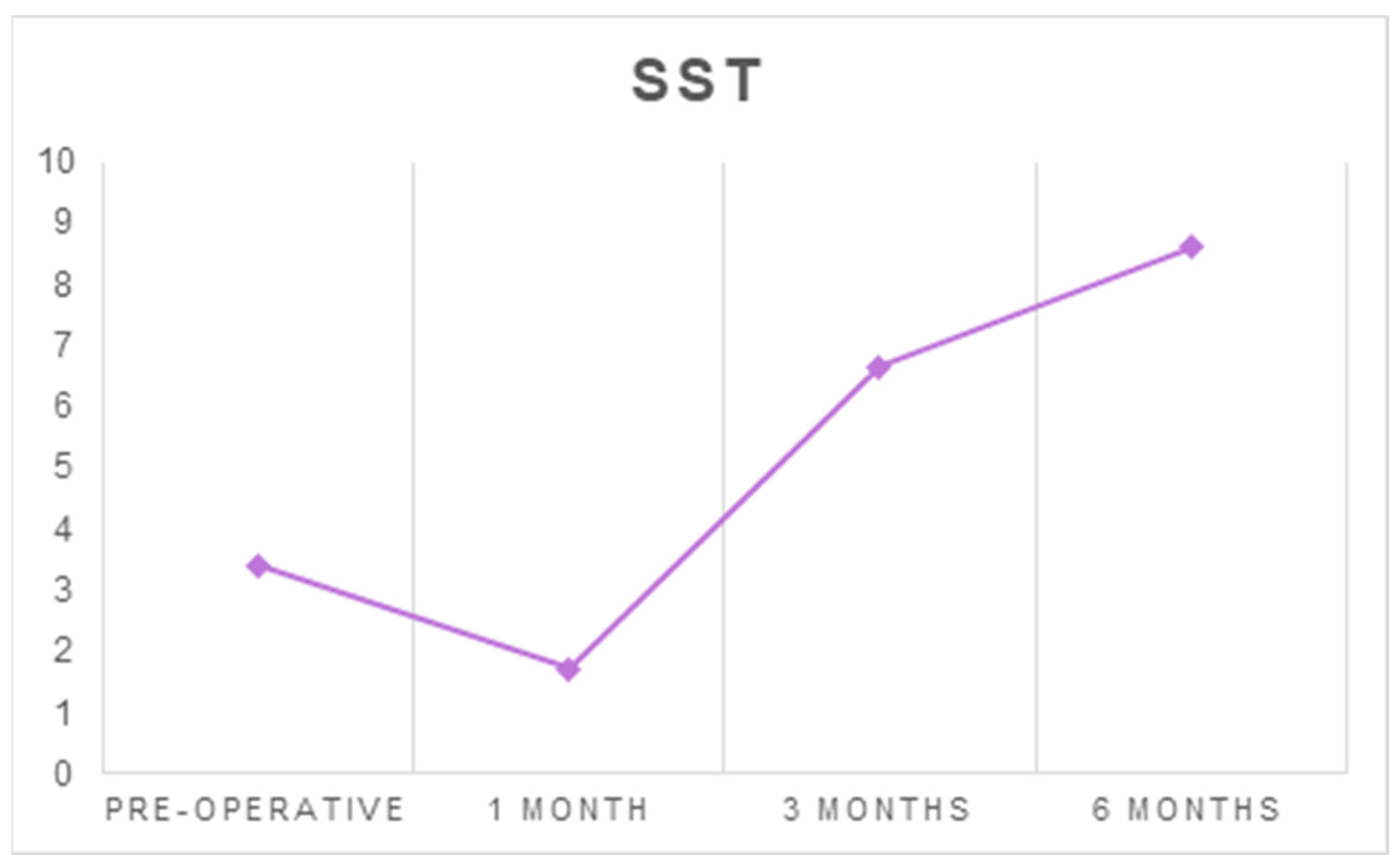
| SST | 3.41 ± 2.73 | 1.71 ± 1.97 | 6.67 ± 2.21 | 8.62 ± 2.65 | <0.001 * |
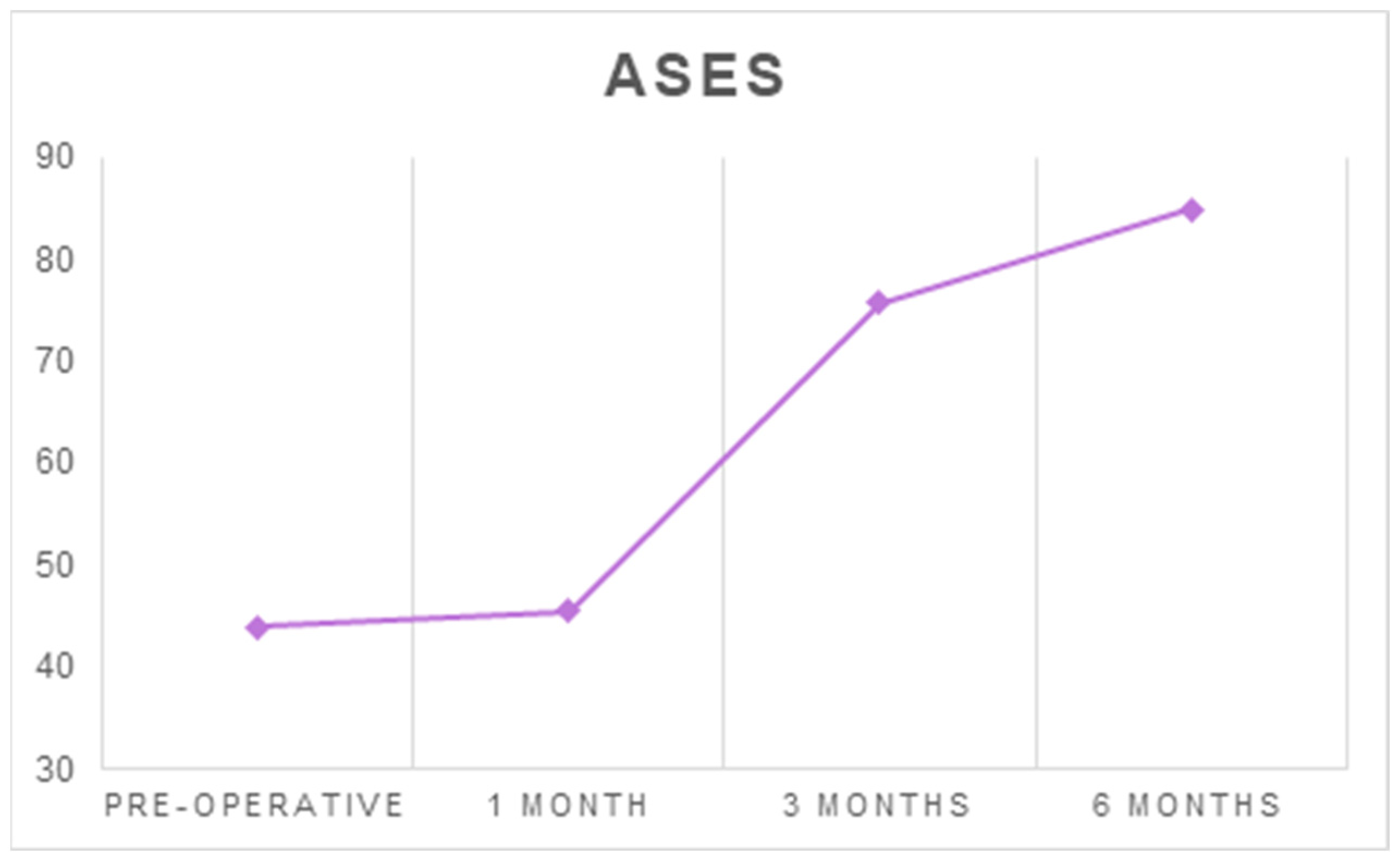
| ASES | 43.94 ± 20.4 | 45.52 ± 16.92 | 75.74 ± 17.09 | 84.95 ± 13.27 | <0.001 * |
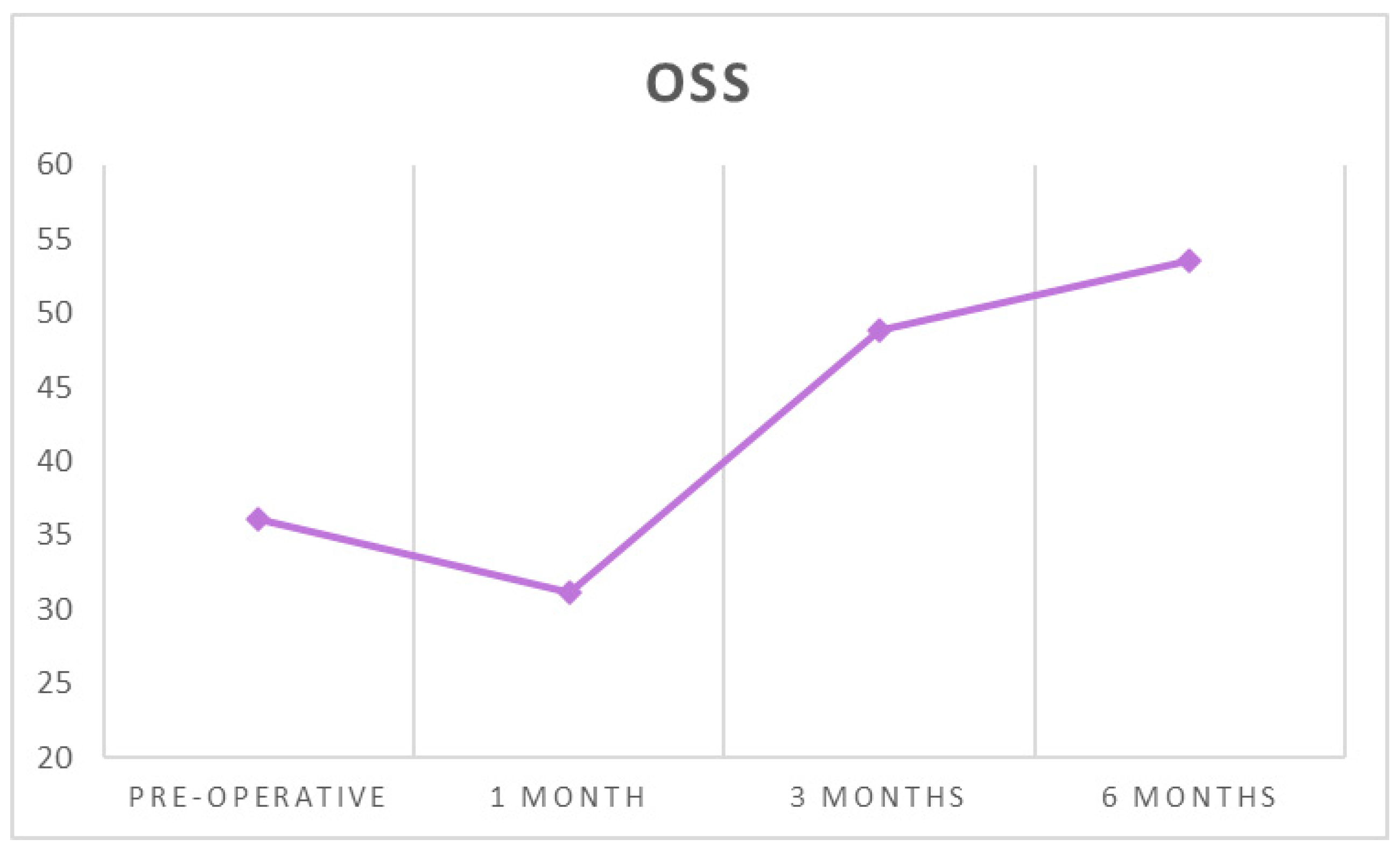
| OSS | 36.09 ± 10.96 | 31.09 ± 8.18 | 48.88 ± 7.72 | 53.60 ± 5.79 | <0.001 * |
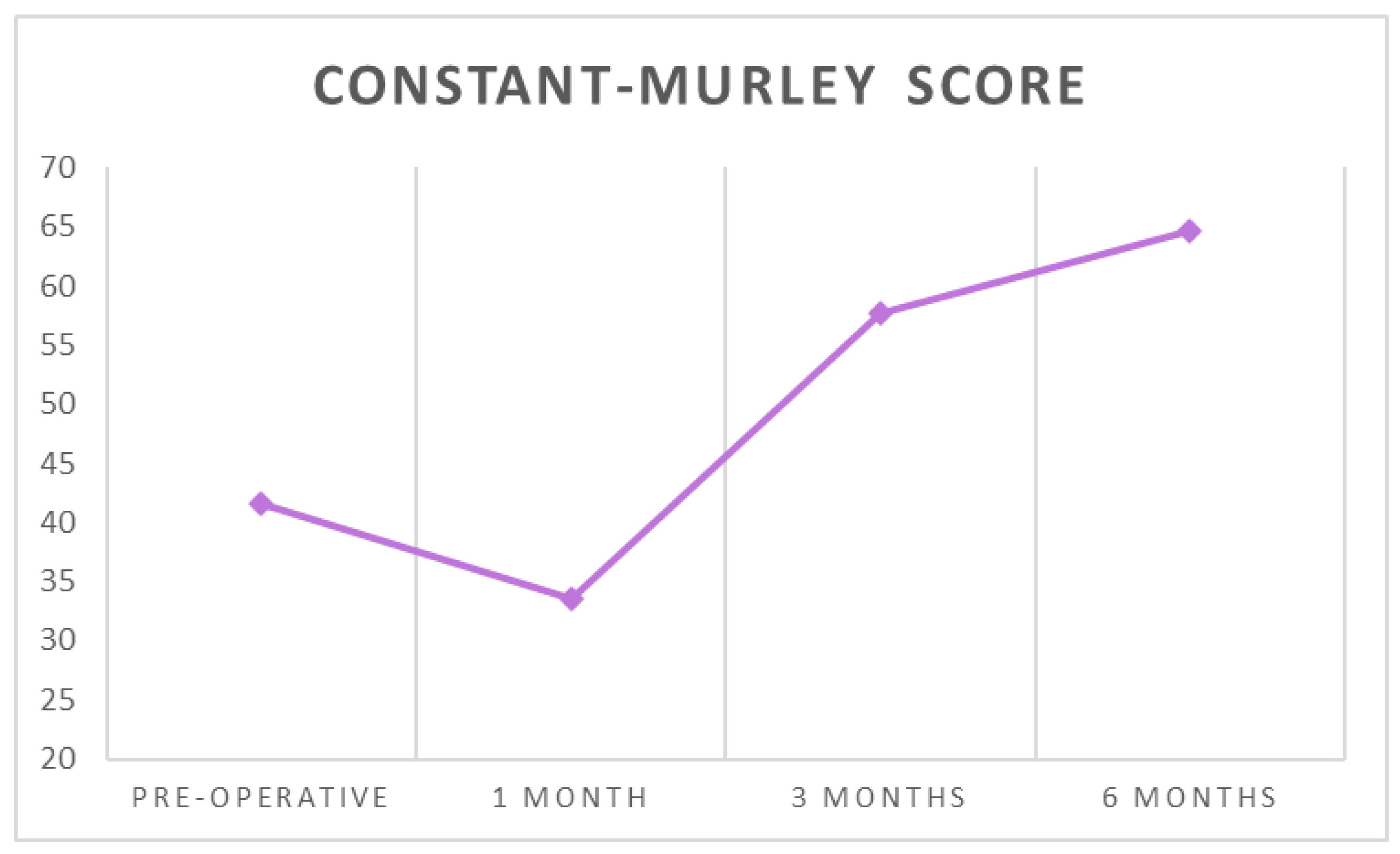
| Constant score | 41.6 ± 15.58 | 33.56 ± 10.46 | 57.66 ± 11.87 | 64.59 ± 9.85 | <0.001 * |
| Pre–One Month | Pre–Three Months | Pre–Six Months | One Month–Three Months | One Month–Six Months | Three Months–Six Months | |
|---|---|---|---|---|---|---|
| PSQI | 0.098 | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| SF-36 | 0.05 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | 0.01 * |
| SST | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| ASES | 0.533 | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| OSS | 0.02 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| Constant score | 0.002 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| Preoperative PSQI | PSQI, One Month | PSQI, Three Months | PSQI, Six Months | ||
|---|---|---|---|---|---|
| SF-36 | rho | −0.570 | −0.594 | −0.577 | −0.538 |
| p-value | <0.001 * | <0.001 * | <0.001 * | <0.001 * | |
| SST | rho | −0.585 | −0.604 | −0.359 | −0.498 |
| p-value | <0.001 * | < 0.001 * | 0.006 * | <0.001 * | |
| ASES | rho | −0.505 | −0.544 | −0.547 | −0.393 |
| p-value | <0.001 * | <0.001 * | <0.001 * | 0.002 * | |
| OSS | rho | −0.071 | −0.317 | −0.136 | −0.195 |
| p-value | 0.598 | 0.015 * | 0.308 | 0.142 | |
| Constant score | rho | −0.527 | −0.504 | −0.302 | −0.383 |
| p-value | < 0.001 | <0.001 | 0.021 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longo, U.G.; Candela, V.; De Salvatore, S.; Piergentili, I.; Panattoni, N.; Casciani, E.; Faldetta, A.; Marchetti, A.; De Marinis, M.G.; Denaro, V. Arthroscopic Rotator Cuff Repair Improves Sleep Disturbance and Quality of Life: A Prospective Study. Int. J. Environ. Res. Public Health 2021, 18, 3797. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073797
Longo UG, Candela V, De Salvatore S, Piergentili I, Panattoni N, Casciani E, Faldetta A, Marchetti A, De Marinis MG, Denaro V. Arthroscopic Rotator Cuff Repair Improves Sleep Disturbance and Quality of Life: A Prospective Study. International Journal of Environmental Research and Public Health. 2021; 18(7):3797. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073797
Chicago/Turabian StyleLongo, Umile Giuseppe, Vincenzo Candela, Sergio De Salvatore, Ilaria Piergentili, Nicolò Panattoni, Erica Casciani, Aurora Faldetta, Anna Marchetti, Maria Grazia De Marinis, and Vincenzo Denaro. 2021. "Arthroscopic Rotator Cuff Repair Improves Sleep Disturbance and Quality of Life: A Prospective Study" International Journal of Environmental Research and Public Health 18, no. 7: 3797. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073797