
Analysing Normative Influences on the Prevalence of Female Genital Mutilation/Cutting among 0–14 Years Old Girls in Senegal: A Spatial Bayesian Hierarchical Regression Approach


 , ,
, ,
Abstract
:1. Introduction
- (1)
- Assessment of the trends of FGM/C prevalence among Senegalese girls aged 0–14 years focusing on the roles of social norms in the persistence of the practice.
- (2)
- Assessment of the unobserved effects of geographical location as well as time and space-time interaction on the likelihood of FGM/C among 0–14 years old Senegalese girls.
2. Materials and Methods
2.1. Data
2.2. Outcome Variable
2.3. Exposure Variables
3. Statistical Analysis
3.1. Bivariate Data Analysis
3.2. Bayesian Hierarchical Spatial and Space-Time Modelling
4. Results
4.1. Descriptive Analysis
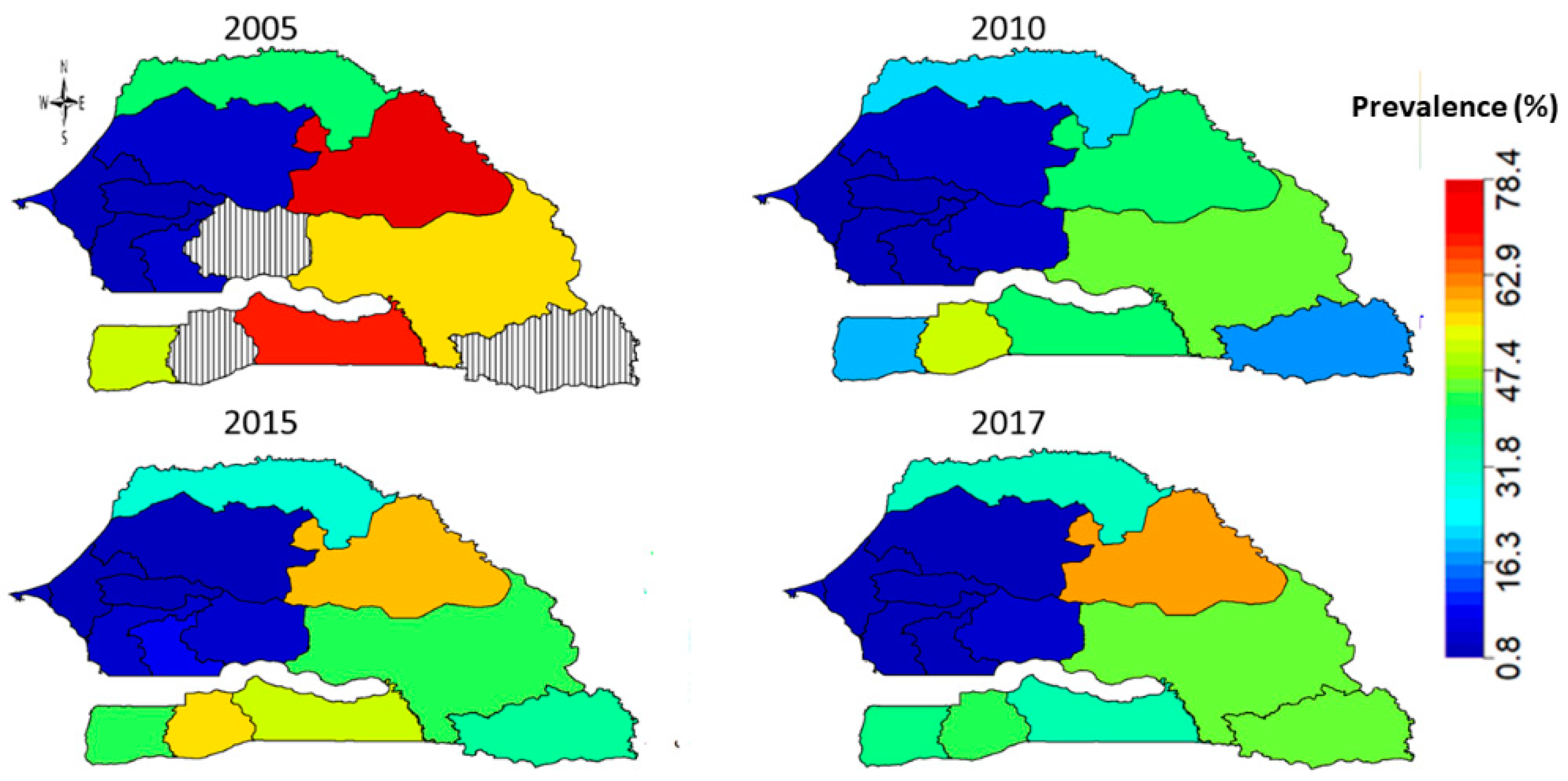
4.2. Regional Evolution of FGM/C Prevalence among 0–14 Years Old Girls in Senegal
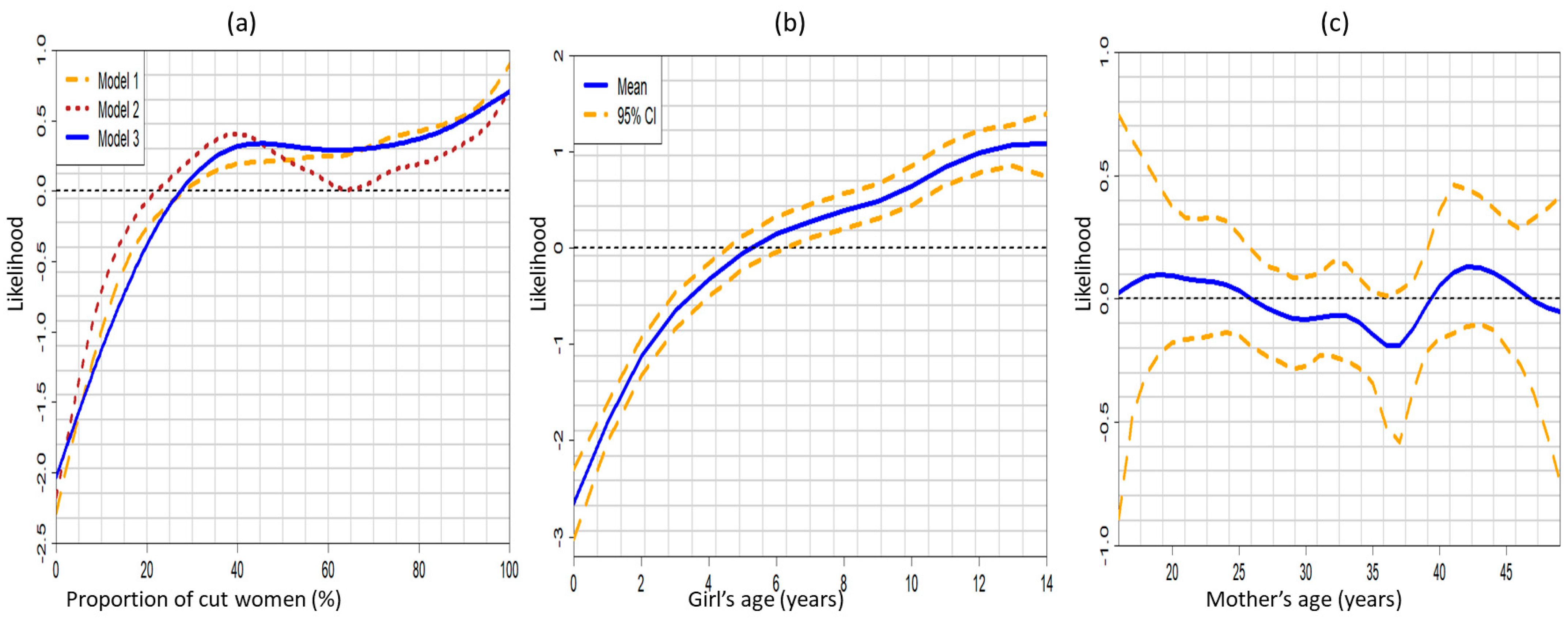
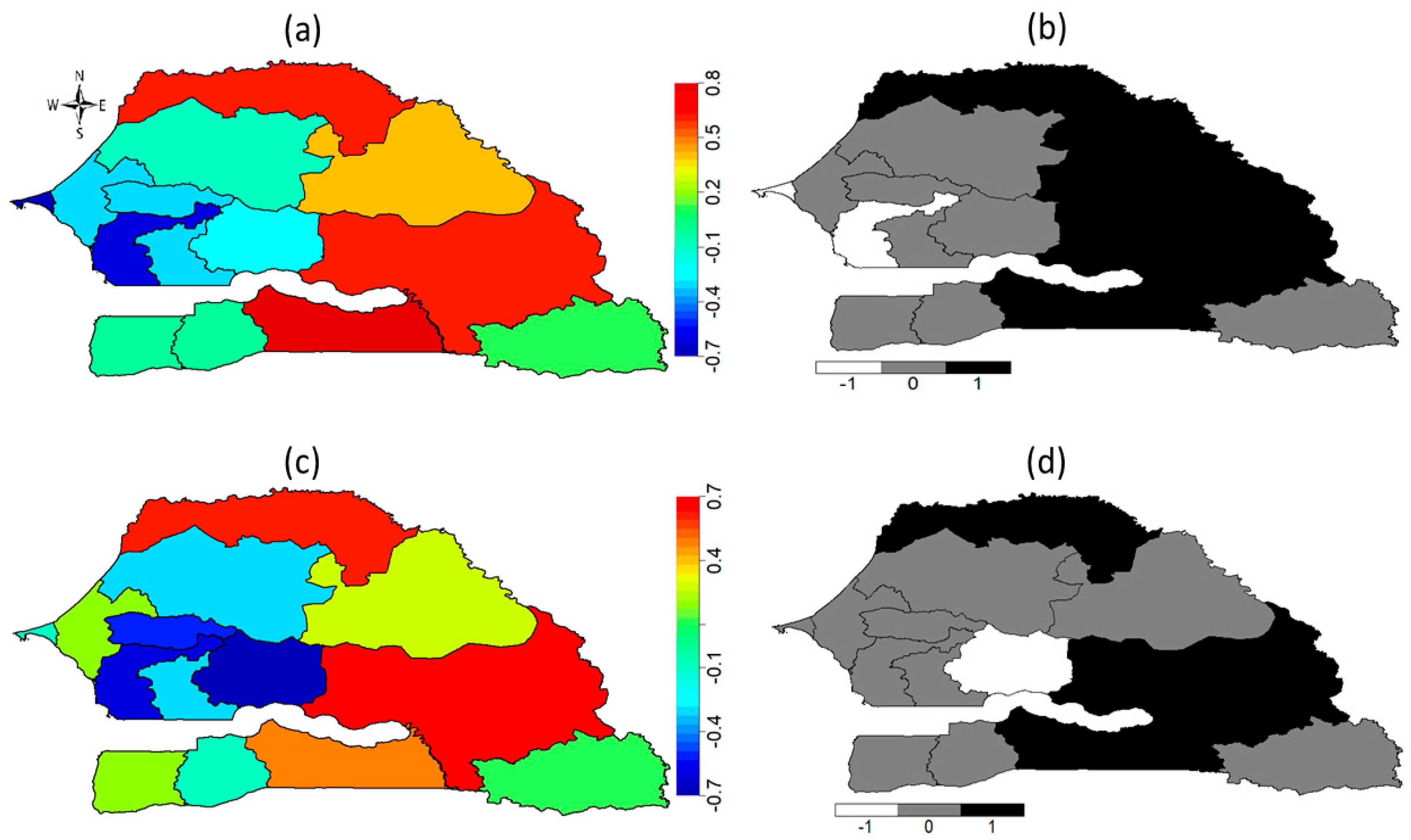
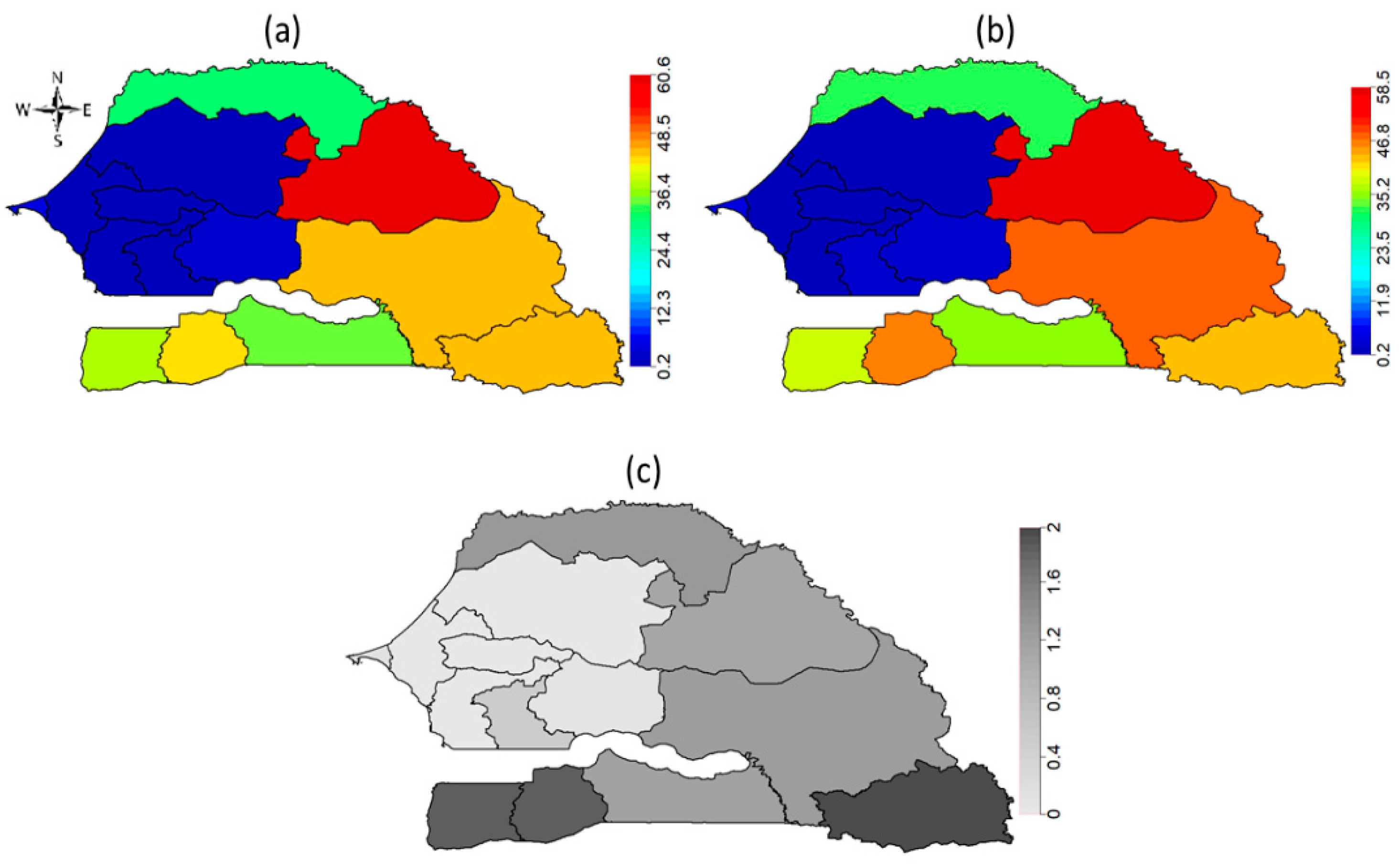
4.3. Bayesian Hierarchical Geo-Additive Logistic Regression
4.4. 2017 Senegal Demographic and Health Surveys (SDHS)
4.5. Pooled 2010 to 2017 SDHS Data
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | 2005 DHS | 2010–2011 DHS | 2015 DHS | 2017 DHS | ||||
|---|---|---|---|---|---|---|---|---|
| 20.4% | N = 11,878 | 11.9% | N = 9740 | 14.6% | N = 7529 | 14.0% | N = 14,008 | |
| Demographic | ||||||||
| Girl’s age | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | ||||
| 0–4 | 15.8 | 4749 | 8.1 | 5325 | 9 | 3047 | 9.6 | 5244 |
| 5–9 | 22.4 | 3960 | 16.5 | 4415 | 17.3 | 2606 | 15.5 | 5098 |
| 10–14 | 24.9 | 3169 | na | na | 20.1 | 1876 | 18.1 | 3667 |
| Mother’s age | p < 0.001 | p = 0.068 | p = 0.011 | p < 0.001 | ||||
| 15–19 | 10.3 | 300 | 14.2 | 295 | 11.7 | 138 | 13.5 | 254 |
| 20–24 | 15.9 | 1322 | 12.7 | 1466 | 10.6 | 694 | 13 | 1196 |
| 25–29 | 16.2 | 2320 | 11.1 | 2431 | 14.1 | 1676 | 14.9 | 2614 |
| 30–34 | 21.8 | 2865 | 11.7 | 2327 | 17 | 1773 | 13.7 | 3646 |
| 35–39 | 22.8 | 492 | 10.8 | 1852 | 12.3 | 1684 | 14.1 | 2901 |
| 40–44 | 23.5 | 1656 | 12 | 989 | 16.1 | 1122 | 13.7 | 2192 |
| 45–49 | 24.6 | 924 | 18.4 | 380 | 19.9 | 442 | 14 | 1205 |
| Mother’s marital status | p = 0.02 | p = 0.118 | p = 0.007 | p = 0.003 | ||||
| Never married | 2.3 | 74 | 5.2 | 201 | 9.9 | 104 | 4.7 | 203 |
| Currently married/in union | 20.7 | 11,214 | 12.1 | 9186 | 14.8 | 7122 | 14.1 | 13,149 |
| Formerly married | 17.6 | 590 | 10.3 | 353 | 13.7 | 302 | 15 | 656 |
| Mother’s age difference with husband/partner (currently married women only) | p < 0.001 | p = 0.36 | p = 0.326 | p = 0.103 | ||||
| Wife is older | 25.9 | 152 | 14.6 | 183 | 16.2 | 217 | 5.9 | 385 |
| Wife is same age | 11.6 | 76 | 11.1 | 123 | 7.2 | 91 | 11.1 | 105 |
| Wife is 1–4 years younger | 14.6 | 1176 | 12.3 | 1013 | 13.3 | 668 | 11.4 | 1617 |
| Wife is 5–9 years younger | 15.6 | 2544 | 11.1 | 2043 | 15.1 | 1737 | 14.4 | 3123 |
| Wife is 10+ years younger | 22.8 | 7930 | 12 | 6378 | 14.8 | 4816 | 14.7 | 8778 |
| Mother’s type of union | p = 0.016 | p = 0.008 | p = 0.007 | p = 0.011 | ||||
| Monogamous | 19.5 | 6251 | 10.9 | 5818 | 13.6 | 4507 | 13.2 | 8219 |
| Polygamous | 22.5 | 4821 | 14.2 | 3367 | 16.8 | 2612 | 15.5 | 4919 |
| Residence | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | ||||
| Urban | 11.7 | 4452 | 7.6 | 3733 | 7.5 | 2824 | 6.2 | 5321 |
| Rural | 25.7 | 7426 | 14.6 | 6007 | 19 | 4704 | 18.7 | 8687 |
| Region | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | ||||
| Dakar | 7.1 | 2302 | 5.6 | 1888 | 2.1 | 1322 | 3.8 | 2752 |
| Diourbel | 0.8 | 1364 | 0.2 | 1216 | 0 | 931 | 0.2 | 1822 |
| Fatick | 2.9 | 737 | 0.5 | 563 | 2.8 | 436 | 1.1 | 754 |
| Kaolack | 4 | 1569 | 0.2 | 821 | 7.1 | 647 | 1.6 | 938 |
| Kolda | 68.8 | 1054 | 40.9 | 506 | 51.8 | 466 | 34.6 | 753 |
| Louga | 3.2 | 832 | 3.4 | 709 | 0 | 578 | 1.6 | 956 |
| Matam | 78.4 | 482 | 41.4 | 409 | 57.1 | 278 | 60.6 | 610 |
| Saint-Louis | 41.1 | 785 | 20.6 | 637 | 29.6 | 477 | 31.8 | 897 |
| Tambacounda | 54.8 | 840 | 44.1 | 561 | 41.8 | 418 | 44 | 875 |
| Thios | 2.6 | 1503 | 0.6 | 1214 | 0.3 | 963 | 1.2 | 1757 |
| Zuguinchor | 51.9 | 411 | 19.1 | 315 | 42.3 | 251 | 38.5 | 464 |
| Kaffrine | na | na | 2.7 | 466 | 2.6 | 403 | 2.4 | 770 |
| Kedougou | na | na | 17.3 | 96 | 35.7 | 76 | 45.4 | 165 |
| Sedhiou | na | na | 50.3 | 340 | 54.8 | 283 | 43 | 494 |
| Mother’s education | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | ||||
| No education | 23.7 | 8796 | 14 | 7134 | 17.4 | 5270 | 16.3 | 9313 |
| Primary | 13.5 | 2215 | 7.1 | 1905 | 9.8 | 1574 | 11 | 3053 |
| Secondary | 5 | 801 | 3.5 | 654 | 5.6 | 601 | 7 | 1400 |
| Higher | 1.4 | 66 | 0 | 47 | 0.8 | 83 | 0.9 | 241 |
| Husband’s/partner’s education | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | ||||
| No education | 23.3 | 8111 | 13.7 | 6848 | 17.9 | 5164 | 17.2 | 8630 |
| Primary | 16.5 | 1275 | 9 | 1068 | 7.1 | 767 | 8 | 1715 |
| Secondary | 12 | 1121 | 7.8 | 699 | 5.2 | 501 | 7.2 | 1185 |
| Higher | 7 | 319 | 5.7 | 223 | 4.5 | 241 | 4.8 | 521 |
| Mother’s religion | p = 0.177 | p < 0.001 | p = 0.232 | p = 0.051 | ||||
| Christian | 8.1 | 389 | 2.2 | 302 | 7.2 | 237 | 3.1 | 394 |
| Muslim | 20.8 | 11,467 | 12.2 | 9385 | 14.8 | 7236 | 14.3 | 13,605 |
| Mother’s ethnicity | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | ||||
| Wolof | 0.7 | 4461 | 0.3 | 3596 | 0.5 | 2901 | 0.3 | 5052 |
| Poular | 46.2 | 3301 | 28 | 2794 | 31.1 | 2254 | 31.1 | 3949 |
| Serer | 0.8 | 1992 | 0.5 | 1514 | 0.5 | 1126 | 0.1 | 2500 |
| Mandingue | 50.1 | 557 | 31.7 | 475 | 36.8 | 446 | 39 | 871 |
| Diola | 34.8 | 524 | 13.5 | 297 | 37.5 | 170 | 26.2 | 452 |
| Soninke | 54.3 | 309 | 18.5 | 169 | 38.7 | 66 | 32.3 | 185 |
| Other Senegalese | 26.8 | 508 | 13.5 | 657 | 13.9 | 333 | 31.5 | 320 |
| Non-Senegalese | 38.8 | 220 | 19.2 | 239 | 35.5 | 233 | 13.5 | 679 |
| Woman from mixed ethnicity household (husband/partner from a different ethnic group; currently married women only) | p = 0.238 | p = 0.544 | p = 0.089 | p < 0.001 | ||||
| Yes | 20.2 | 378 | 8.7 | 527 | 9.7 | 409 | 9.3 | 754 |
| No | 22.6 | 1445 | 12.1 | 1.343 | 16.7 | 1494 | 17.3 | 2575 |
| Wealth Quintile | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | ||||
| Lowest | 26.8 | 2639 | 21.2 | 2292 | 25.4 | 1777 | 25.8 | 3291 |
| Second | 31.6 | 2669 | 13.7 | 2125 | 19.2 | 1636 | 18.3 | 3122 |
| Middle | 21.2 | 2492 | 11.3 | 1898 | 15.3 | 1531 | 11.5 | 2821 |
| Higher | 12.6 | 2201 | 6.8 | 1909 | 5 | 1359 | 5.3 | 2564 |
| Highest | 3.5 | 1877 | 2.4 | 1516 | 2.8 | 1225 | 3.5 | 2211 |
| Mother’s Beliefs | ||||||||
| Women’s attitudes toward FGM/C | ||||||||
| Should be continued | 69.8 | 2299 | 53.6 | 1740 | 57.3 | 1412 | 62.3 | 2522 |
| Should be discontinued | 8.6 | 8175 | 2.7 | 6775 | 5.2 | 5194 | 3.3 | 10,324 |
| Depends/Don’t know | 12.8 | 885 | 8.4 | 469 | 11.3 | 211 | 9 | 482 |
| Women’s beliefs about FGM/C | ||||||||
| FGM/C is required by religion | 67.4 | 2220 | 46.6 | 1719 | 54.1 | 1010 | 59.2 | 2052 |
| FGM/C is not required by religion | 9.2 | 8151 | 4.5 | 6707 | 9.3 | 5465 | 6.3 | 10,553 |
| Mother’s gender norms | ||||||||
| Husband is justified in hitting or beating his wife if she: | ||||||||
| Burns the food | ||||||||
| Yes | 19.8 | 3012 | 16.3 | 2717 | 17 | 2025 | 18.9 | 3883 |
| No | 20.8 | 8729 | 10.2 | 6994 | 13.8 | 5500 | 12.1 | 10,101 |
| Neglects children | ||||||||
| Yes | 20.3 | 6269 | 15.3 | 4462 | 18.2 | 3899 | 18.4 | 5940 |
| No | 20.7 | 5504 | 9 | 5254 | 11 | 3627 | 10.7 | 8044 |
| Argues with him | ||||||||
| Yes | 21.5 | 6312 | 14.9 | 4869 | 17.4 | 3940 | 19.2 | 6098 |
| No | 19.6 | 5381 | 8.9 | 4818 | 11.6 | 3584 | 9.9 | 7879 |
| Goes out without telling him | ||||||||
| Yes | 21.8 | 6588 | 15.8 | 4554 | 19.1 | 3826 | 18.7 | 5834 |
| No | 18.7 | 5138 | 8.4 | 5142 | 10 | 3698 | 10.5 | 8147 |
| Refuses to have sex with him | ||||||||
| Yes | 20.7 | 6156 | 14.5 | 5221 | 17.2 | 3955 | 18.3 | 6424 |
| No | 20.6 | 5532 | 8.6 | 4452 | 11.8 | 3568 | 10.2 | 7553 |
| Final say in making decisions on women’s own health care | ||||||||
| Self only | 25.2 | 1784 | 23.3 | 1053 | 20.1 | 405 | 14.6 | 1015 |
| Jointly with husband/someone else | 22 | 804 | 26.9 | 1696 | 38.3 | 1071 | 22.2 | 2527 |
| Husband/someone else only | 19.4 | 9261 | 30.2 | 6407 | 27.8 | 5618 | 30.7 | 9567 |
| Mother’s opportunities | ||||||||
| Mother’s occupation | ||||||||
| Formal | 15.6 | 3932 | 8.5 | 3366 | 9.8 | 2169 | 8 | 4881 |
| Informal | 31.3 | 2301 | 19.2 | 1444 | 20.9 | 2787 | 17.3 | 4579 |
| Not working | 19.5 | 5606 | 12.1 | 4919 | 12 | 2517 | 17 | 4426 |
| Mother’s employment | ||||||||
| All year | 15.9 | 2936 | 9.2 | 2521 | 10.1 | 2696 | 8 | 5489 |
| Seasonal/once in a while | 26.1 | 3312 | 14.3 | 2316 | 22.8 | 2316 | 18.5 | 4112 |
| Mother works for cash (cash only/cash and kind) | ||||||||
| Yes | 18.6 | 4845 | 9.5 | 4124 | 12.2 | 3909 | 9.9 | 7568 |
| No | 30.5 | 1413 | 23.8 | 712 | 29.2 | 1102 | 22.4 | 2033 |
| Mother’s number of trips away from the community (slept away) in the last 12 months | ||||||||
| 0 | 14.7 | 4350 | 21.1 | 2752 | ||||
| 1–25 | 9.7 | 5281 | 10.7 | 4673 | ||||
| 26–50 | 11.5 | 58 | 20.5 | 69 | ||||
| 51 or more | 0.7 | 52 | 20 | 34 | ||||
| Mother’s frequency of reading newspaper or magazine | ||||||||
| Not at all | 22.2 | 10,500 | 12.9 | 8644 | 15.6 | 6915 | 15.4 | 12,240 |
| Less than once a week | 6.6 | 705 | 6.1 | 567 | 5 | 283 | 5.2 | 1097 |
| At least once a week | 6.5 | 631 | 2.2 | 529 | 3.9 | 331 | 2.7 | 671 |
| Mother’s frequency of listening to the radio | ||||||||
| Not at all | 33.1 | 1104 | 12.5 | 1874 | 18 | 1344 | 19.2 | 2173 |
| Less than once a week | 13.9 | 1365 | 15.5 | 2223 | 15.5 | 2065 | 16.3 | 4618 |
| At least once a week | 17.9 | 2397 | 10.3 | 5644 | 13.1 | 4120 | 10.9 | 7217 |
| Mother’s frequency of watching television | ||||||||
| Not at all | 29 | 4083 | 17 | 3399 | 21.3 | 2670 | 23.7 | 3957 |
| Less than once a week | 17.7 | 1750 | 15.6 | 1382 | 19.3 | 1203 | 19.3 | 2798 |
| At least once a week | 19.3 | 1708 | 7.3 | 4959 | 8.2 | 3655 | 6.6 | 7253 |
References
- World Health Organization. Fact Sheets on Female Genital Mutilation. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/female-genital-mutilation (accessed on 18 July 2019).
- Shetty, P. Slow progress in ending female genital mutilation. Bull. World Health Organ. 2014, 92, 6–7. [Google Scholar] [CrossRef]
- WHO. Eliminating Female Genital Mutilatio. An Interagency Statement. (WHO, UNFPA, UNICEF, UNIFEM, UNHCHR, UNHCR, UNECA, UNESCO, UNDP, UNAIDS); World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Muteshi, J.K.; Miller, S.; Belizan, J.M. The ongoing violence against women: Female Genital Mutilation/Cutting. Reprod. Health 2016, 18, 44. [Google Scholar] [CrossRef] [Green Version]
- Rymer, J. Female genital mutilation. Curr. Obs. Gynecol. 2003, 13, 185–190. [Google Scholar] [CrossRef]
- Toubia, N. Female circumcision as a public health issue. N. Engl. J. Med. 1994, 331, 712–716. [Google Scholar] [CrossRef]
- Dirie, M.; Lindmark, G. The risk of medical complications after female circumcision. East Afr. Med. J. 1992, 69, 479–482. [Google Scholar] [PubMed]
- Abd El-Naser, T.; Farouk, A.; El-Nashar, A.E.-R.; Mostafa, T. Sexual side effects of female genital mutilation/cutting May Be type dependent: A hospital-based study. J. Obstet. Gynecol. 2011, 1, 65–74. [Google Scholar]
- Alsibiani, S.A.; Rouzi, A.A. Sexual function in women with female genital mutilation. Fertil. Steril. 2010, 93, 722–724. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Female Genital Mutilation/Cutting; A Global Concern; UNICEF: New York, NY, USA, 2016. [Google Scholar]
- ANSD. Senegal: Facteurs Socio-Demographiques, Agence Nationale de Statistique et de la Démographie. 2019. Available online: http://www.ansd.sn/ (accessed on 15 July 2019).
- 28 TooMany Country Profile: FGM in Senegal. 2015. Available online: https://www.28toomany.org/static/media/uploads/ (accessed on 19 July 2019).
- Standard DHS. 2010–2011. The DHS Program. Available online: https://dhsprogram.com/ (accessed on 19 July 2019).
- Kandala, N.-B.; Komba, P.N. Geographical Variation in Female Genital Mutilation and Legal Enforcement in sub-Saharan Africa: A case Study of Senegal. Am. J. Trop. Med. Hyg. 2015, 92, 838–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kandala, N.-B.; Shell-Duncan, B. Trends in female genital mutilation/cutting in Senegal: What can we learn from successive household surveys in sub-Saharan African countries? Int. J. Equity Health 2019, 18, 25. [Google Scholar] [CrossRef] [Green Version]
- Matanda, D.; Atilola, G.; Moore, Z.; Komba, P.; Mavatikua, L.; Nnanatu, C.C.; Kandala, N.-B. Female Genital Mutilation/Cutting in Senegal: Is the Practice Declining? Descriptive Analysis of Demographic and Health Declining? Descriptive Analysis of Demographic and Health Surveys, 2005–2017 Surveys. Available online: https://knowledgecommons.popcouncil.org/cgi/viewcontent.cgi?article=2080&context=departments_sbsr-rh (accessed on 13 February 2021).
- Mackie, G.; LeJeune, J. Social Dynamics of Abandonment of Harmful Practices. A New Look at the Theory; Innocenti Working Paper No. 2009-06; UNICEF Innocenti Research Centre: Florence, KY, USA, 2009. [Google Scholar]
- Mackie, G. Ending footbinding and infibulation A convention account. Am. Sociol. Rev. 1996, 61, 999–1017. [Google Scholar] [CrossRef]
- Shell-Duncan, B.; Wander, K.; Hernlund, Y.; Moreau, A. Dynamics of change in the practice of female genital cutting in Senegambia: Testing predictions of social convention theory. Soc. Sci. Med. 2011, 73, 1275–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cislaghi, B.; Heise, L. Using social norms theory for health promotion in low-income countries. Health Promot. Int. 2018, 37, 562–573. [Google Scholar] [CrossRef] [PubMed]
- LiselottDellenborg. A Reflection on the Cultural Meanings of Female Genital Cutting: Experiences from Fieldwork in Casamance, Southern Senegal. 2000. Available online: https://gup.ub.gu.se/publication/74446 (accessed on 4 May 2018).
- Utazi, C.E.; Afuecheta, A.O.; Nnanatu, C.C. Bayesian latent process spatiotemporal regression model for areal count data. Spat. Spatio-Temporal Epidemiol. 2018, 25, 25–37. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.; Rushworth, A.; Shahu, S.K. A Bayesian localized conditional auroregressive model for estimating the health effects of air pollution. Biometrics 2014, 70, 419–429. [Google Scholar] [CrossRef] [Green Version]
- Kandala, N.-B.; Nwakeze, N.; Ngianga, S.; Kandala, I.I. Spatial distribution of female genital mutilation in Nigeria. Am. J. Trop. Med. Hyg. 2009, 81, 784–792. [Google Scholar] [CrossRef] [Green Version]
- Nnanatu, C.C.; Atilola, G.; Komba, P.; Mavatikua, L.; Moore, Z.; Matanda, D.; Kandala, N.-B. Evaluating changes in the prevalence of female genital mutilation/cutting among 0-14 years old girls in Nigeria using data from multiple surveys: A novel Bayesian hierarchical spatio-temporal model. PLoS ONE 2021, 16, e0246661. [Google Scholar] [CrossRef]
- Stata Statistical Software. Sata Corp 2009. Available online: https://www.stata.com/URL (accessed on 3 May 2018).
- Brezger, A.L. Generalized Structured Additive Regression Based on Bayesian P-Splines. Comput. Stat. Data Anal. 2006, 50, 947–991. [Google Scholar] [CrossRef] [Green Version]
- Kneib, T.; Fahrmeir, L. Structured Additive Regression for Multicategorical Space-Time Data: A Mixed Model Approach. Biometrics 2006, 62, 109. [Google Scholar] [CrossRef] [Green Version]
- Kamman, E.E.; Wand, M.P. Geoadditive Models. J. R. Stat. Soc. Ser. C 2003, 52, 1–18. [Google Scholar] [CrossRef]
- Lang, B. Bayesian P-splines. Sonderforschungsberelch 2001, 386, 236. [Google Scholar] [CrossRef] [Green Version]
- Eilers, P.; Marx, B. Flexible Smoothing using B-splines and Penalized Likelihood (with comments and rejoinder). Statist. Math. 1996, 53, 11–30. [Google Scholar]
- Umlauf, N.; Adler, D.; Kneib, T. Structured Additive Regression Models: An R Interface to BayesX. J. Stat. Softw. 2015, 63, 21. [Google Scholar] [CrossRef] [Green Version]
- Gilks, W.R.; Wild, P. Adaptive Rejection Sampling for Gibbs Sampling. J. R. Stat. Soc. Ser. C 1992, 41, 337–348. [Google Scholar] [CrossRef]
- Spiegelhalter, D.J.; Best, N.G.; Carlin, B.P.; Van Der Linde, A. Bayesian measures of model complexity and fit. J. R. Stat. Soc. Ser. B 2002, 64, 583–639. [Google Scholar] [CrossRef] [Green Version]
- Hongfei, L.I.; Calder, C.A.; Cressie, N. Beyond Moran’s I: Testing for Spatial Dependence Based on the Spatial Autoregressive Model. Geogr. Anal. 2007, 39, 357–375. [Google Scholar]
- Mackie, G. Unprogrammed abandonment of female genital mutilation/cutting. World Dev. 2021, in press. [Google Scholar]
- Shell-Duncan, B.; Moreau, A.; Wander, K.; Smith, S. The role of older women in contesting norms associated with female genital mutilation/cutting: A factorial focus group analysis. PLoS ONE 2018, 13, e0199217. [Google Scholar] [CrossRef]









| Survey | Girls 0–14 Years | National Prevalence (%) |
|---|---|---|
| 2005 SDHS | 11,878 | 20.4 |
| 2010–2011 SDHS | 9740 | 11.9 |
| 2015 SDHS | 7529 | 14.6 |
| 2017 SDHS | 14,008 | 14.0 |
| Data | Model | Description | DIC |
|---|---|---|---|
| 2017 SDHS | Model 1 | Normative influence variables only | 6427 |
| Model 2 | Normative influence variables and total space | 6329 | |
| Model 3 | Normative influence variables, space and other individual-level covariates | 3542 | |
| 2010 to 2017 pooled data | Model 4 | Normative influence variables only. | 15,300 |
| Model 5 | Normative influence variables, space without time and space-time interaction. | 15,160 | |
| Model 6 | Normative influence variables, space and time, space-time interaction and other individual-level covariates | 12,324 |
| Predictor | Level | Model 1 POR (95% CI) | Model 2 POR (95% CI) | Model 3 POR (95% CI) |
|---|---|---|---|---|
| DEMOGRAPHIC | ||||
| Place of residence | Rural (ref) | 1.00 | ||
| Urban | 0.52 (0.39, 0.68) | |||
| Religion | ||||
| Christian (ref) | 1.00 | |||
| Muslim | 0.78 (0.33, 1.97) | |||
| Wealth index | ||||
| Middle (ref) | 1.00 | |||
| lower | 0.89 (0.65, 1.20) | |||
| lowest | 0.94 (0.68, 1.31) | |||
| Higher | 1.40 (0.93, 2.00) | |||
| Highest | 0.81 (0.39, 1.63) | |||
| Ethnicity | ||||
| Wolof (ref) | 1.00 | |||
| Idiola | 5.97 (2.46, 16.59) | |||
| Mandingue | 3.84 (1.88, 9.47) | |||
| Non-Senegalese | 2.15 (0.95, 5.16) | |||
| Other | 4.25 (1.86, 11.13) | |||
| Poular | 3.50 (1.76, 8.25) | |||
| Serer | 0.49 (0.10, 2.02) | |||
| Soninke | 3.74 (1.61, 10.47) | |||
| SOCIAL NORMS | ||||
| (SOCIAL NORMS) Mother cut | ||||
| No (ref) | 1.00 | 1.00 | 1.00 | |
| Yes | 14.05 (10.73,18.3) | 14.19 (10.93, 19.01) | 14.74 (10.01, 21.31) | |
| Support continuation | ||||
| Be stopped (ref) | 1.00 | 1.00 | 1.00 | |
| Continued | 3.82 (3.32, 4.51) | 3.88 (3.40, 4.49) | 5.28 (4.36, 6.55) | |
| Depends | 1.27 (0.90, 1.81) | 1.29 (0.85, 1.80) | 0.99 (0.55, 1.76) | |
| FGM/C is required by religion | ||||
| No (ref) | 1.00 | 1.00 | 1.00 | |
| Yes | 1.69 (1.43, 1.96) | 1.72 (1.48, 2.03) | 1.94 (1.51, 2.39) | |
| WOMEN’S AGENCY | ||||
| Mother’s education | ||||
| Higher (ref) | 1.00 | |||
| No education | 0.77 (0.29, 2.46) | |||
| Primary | 0.87 (0.34, 2.70) | |||
| Secondary | 1.30 (0.47, 4.21) | |||
| WOMEN’S OPPORTUNITIES | ||||
| Mother’s occupation | ||||
| Formal (ref) | 1.00 | |||
| Informal | 1.20 (0.93, 1.54) | |||
| Not working | 1.53 (0.97, 2.49) | |||
| Who decides? | ||||
| husband’s expenditure | Alone (ref) | 1.00 | ||
| Husband has no earning | 3.85 (1.12, 12.12) | |||
| hus/partner/someone else | 0.81 (0.36, 1.61) | |||
| With hus/partner/someone else | 1.29 (0.57, 2.88) | |||
| GENDER NORMS | ||||
| Female positive attitude to wife beating: | ||||
| Wife beating for going out | ||||
| No (ref) | 1.00 | |||
| Yes | 0.90 (0.65, 1.26) | |||
| Wife beating for neglecting the children | ||||
| No (ref) | 1.00 | |||
| Yes | 1.40 (0.96, 2.04) | |||
| Wife beating for arguing with the husband | ||||
| No (ref) | 1.00 | |||
| Yes | 0.76 (0.49, 1.12) | |||
| Wife beating for denying husband sex | ||||
| No (ref) | 1.00 | |||
| Yes | 1.54 (1.12, 2.12) | |||
| Wife beating for denying husband food | ||||
| No (ref) | 1.00 | |||
| Yes | 0.74 (0.57, 0.96) | |||
| Who makes large household purchases | Alone (ref) | 1.00 | ||
| Husband/partner | 0.37 (0.17, 0.74) | |||
| With husband/par | 0.28 (0.13, 0.56) | |||
| Who makes decision on mother’s health | Alone(ref) | 1.00 | ||
| Husband/partner | 1.81 (1.00, 3.32) | |||
| With husband/par | 1.10 (0.58, 2.17) | |||
| MEDIA INFORMATION | ||||
| Read Newspaper | Not at all (ref) | 1.00 | ||
| Less than once a week | 0.36 (0.19, 0.67) | |||
| At least once a week | 0.57 (0.20, 1.53) | |||
| Listen to Radio | Not at all (ref) | 1.00 | ||
| Less than once a week | 1.18 (0.92, 1.49) | |||
| At least once a week | 1.19 (0.92, 1.60) | |||
| Watch Television | Not at all (ref) | 1.00 | ||
| Less than once a week | 0.76 (0.60, 0.96) | |||
| At least once a week | 0.76 (0.59, 1.01) |
| Predictor | Level | Model 4 POR (95% CI) | Model 5 POR (95% CI) | Model 6 POR (95% CI) |
|---|---|---|---|---|
| DEMOGRAPHIC | ||||
| Place of residence | Rural (ref) | 1.00 | ||
| Urban | 0.63 (0.56, 0.73) | |||
| Religion | ||||
| Christian (ref) | 1.00 | |||
| Muslim | 0.95 (0.69, 1.33) | |||
| Wealth index | ||||
| Middle (ref) | 1.00 | |||
| lower | 0.93(0.79, 1.12) | |||
| lowest | 0.91 (0.76, 1.11) | |||
| Higher | 1.17 (0.88, 1.52) | |||
| Highest | 0.84 (0.56, 1.20) | |||
| Ethnicity | ||||
| Wolof (ref) | 1.00 | |||
| Idiola | 3.27 (1.95, 5.65) | |||
| Mandingue | 2.75 (1.74, 4.66) | |||
| Non-Senegalese | 2.35 (1.50, 4.03) | |||
| Other | 2.84 (1.83, 4.79) | |||
| Poular | 3.19 (2.08, 5.21) | |||
| Serer | 0.86 (0.42, 1.88) | |||
| Soninke | 4.24 (2.57, 7.70) | |||
| SOCIAL NORMS | ||||
| Mother cut | ||||
| No (ref) | 1.00 | 1.00 | 1.00 | |
| Yes | 13.69 (11.04, 17.13) | 13.63 (11.19, 16.57) | 13.38(10.56, 17.17) | |
| Support continuation | ||||
| Be stopped (ref) | 1.00 | 1.00 | 1.00 | |
| Continued | 3.55 (3.24, 3.89) | 3.59 (3.29, 3.95) | 4.96 (4.43, 5.59) | |
| Depends | 1.25 (0.99, 1.61) | 1.22 (0.97, 1.56) | 1.25 (0.91, 1.68) | |
| FGM/C is required by religion | ||||
| No (ref) | 1.00 | 1.00 | 1.00 | |
| Yes | 1.39 (1.26, 1.54) | 1.40 (1.27, 1.54) | 1.64 (1.43, 1.89) | |
| WOMEN’S AGENCY | ||||
| Mother’s education | ||||
| Higher (ref) | 1.00 | |||
| No education | 0.85 (0.62, 1.19) | |||
| Primary | 0.78 (0.57, 1.07) | |||
| Secondary | 0.31 (0.05, 1.38) | |||
| Highest educational level of mother’s husband | Higher (ref) | 1.00 | ||
| No education | 1.52 (0.95, 2.49) | |||
| Primary | 1.05 (0.64, 1.70) | |||
| Secondary | 0.97 (0.57, 1.57) | |||
| WOMEN’S OPPORTUNITIES | ||||
| Mother’s occupation | ||||
| Formal (ref) | 1.00 | |||
| Informal | 1.35 (1.17, 1.59) | |||
| Not working | 1.38 (1.13, 1.76) | |||
| Partner’s occupation | Formal (ref) | 1.00 | ||
| Informal | 0.98 (0.85, 1.11) | |||
| Not working | 0.69 (0.50, 0.97) | |||
| Woman currently employed | ||||
| No (ref) | 1.00 | |||
| Yes | 0.75 (0.63, 0.90) | |||
| Who decides? | ||||
| husband’s expenditure | Alone (ref) | 1.00 | ||
| Husband has no earning | 1.69 (0.70, 4.84) | |||
| hus/partner/someone else | 0.66 (0.45, 0.96) | |||
| With hus/partner/someone else | 0.76 (0.48, 1.16) | |||
| GENDER NORMS | ||||
| Female positive attitude to wife beating: | ||||
| Wife beating for going out | ||||
| No (ref) | 1.00 | |||
| Yes | 1.08 (0.90, 1.28) | |||
| Wife beating for neglecting the children | ||||
| No (ref) | 1.00 | |||
| Yes | 1.02 (0.86, 1.24) | |||
| Wife beating for arguing with the husband | ||||
| No (ref) | 1.00 | |||
| Yes | 0.95 (0.79, 1.14) | |||
| Wife beating for denying husband sex | ||||
| No (ref) | 1.00 | |||
| Yes | 1.38 (1.17, 1.62) | |||
| Wife beating for denying husband food | ||||
| No (ref) | 1.00 | |||
| Yes | 0.92 (0.80, 1.05) | |||
| Who makes large household purchases | Alone (ref) | 1.00 | ||
| Husband/partner | 0.96 (0.67, 1.36) | |||
| With husband/partner | 0.87 (0.62, 1.27) | |||
| Who makes decision on mother’s health | Alone(ref) | 1.00 | ||
| Husband/partner | 1.25 (0.92, 1.68) | |||
| With husband/partner | 0.96 (0.67, 1.30) | |||
| MEDIA INFORMATION | ||||
| Read Newspaper | Not at all (ref) | 1.00 | ||
| Less than once a week | 0.74 (0.52, 1.05) | |||
| At least once a week | 0.96 (0.56, 1.67) | |||
| Listen to Radio | Not at all (ref) | 1.00 | ||
| Less than once a week | 1.31 (1.13, 1.53) | |||
| At least once a week | 1.37 (1.19, 1.57) | |||
| Watch Television | Not at all (ref) | 1.00 | ||
| Less than once a week | 1.01 (0.80, 1.14) | |||
| At least once a week | 0.96 (0.80, 1.14) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kandala, N.-B.; Nnanatu, C.C.; Atilola, G.; Komba, P.; Mavatikua, L.; Moore, Z.; Matanda, D. Analysing Normative Influences on the Prevalence of Female Genital Mutilation/Cutting among 0–14 Years Old Girls in Senegal: A Spatial Bayesian Hierarchical Regression Approach. Int. J. Environ. Res. Public Health 2021, 18, 3822. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073822
Kandala N-B, Nnanatu CC, Atilola G, Komba P, Mavatikua L, Moore Z, Matanda D. Analysing Normative Influences on the Prevalence of Female Genital Mutilation/Cutting among 0–14 Years Old Girls in Senegal: A Spatial Bayesian Hierarchical Regression Approach. International Journal of Environmental Research and Public Health. 2021; 18(7):3822. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073822
Chicago/Turabian StyleKandala, Ngianga-Bakwin, Chibuzor Christopher Nnanatu, Glory Atilola, Paul Komba, Lubanzadio Mavatikua, Zhuzhi Moore, and Dennis Matanda. 2021. "Analysing Normative Influences on the Prevalence of Female Genital Mutilation/Cutting among 0–14 Years Old Girls in Senegal: A Spatial Bayesian Hierarchical Regression Approach" International Journal of Environmental Research and Public Health 18, no. 7: 3822. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073822