
Measuring Attitudes toward Suicide Prevention among Occupational Staff Frequently Exposed to Suicidal Individuals: Psychometric Evaluation and Validation


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Items
3. Procedures
3.1. The First Study
3.1.1. Cross-Validations
3.1.2. Tests of the Hypothesized Measurement Models
3.2. The Second Study
Reliability Tests
4. Data Analyses
5. Results
5.1. Cross-Validations
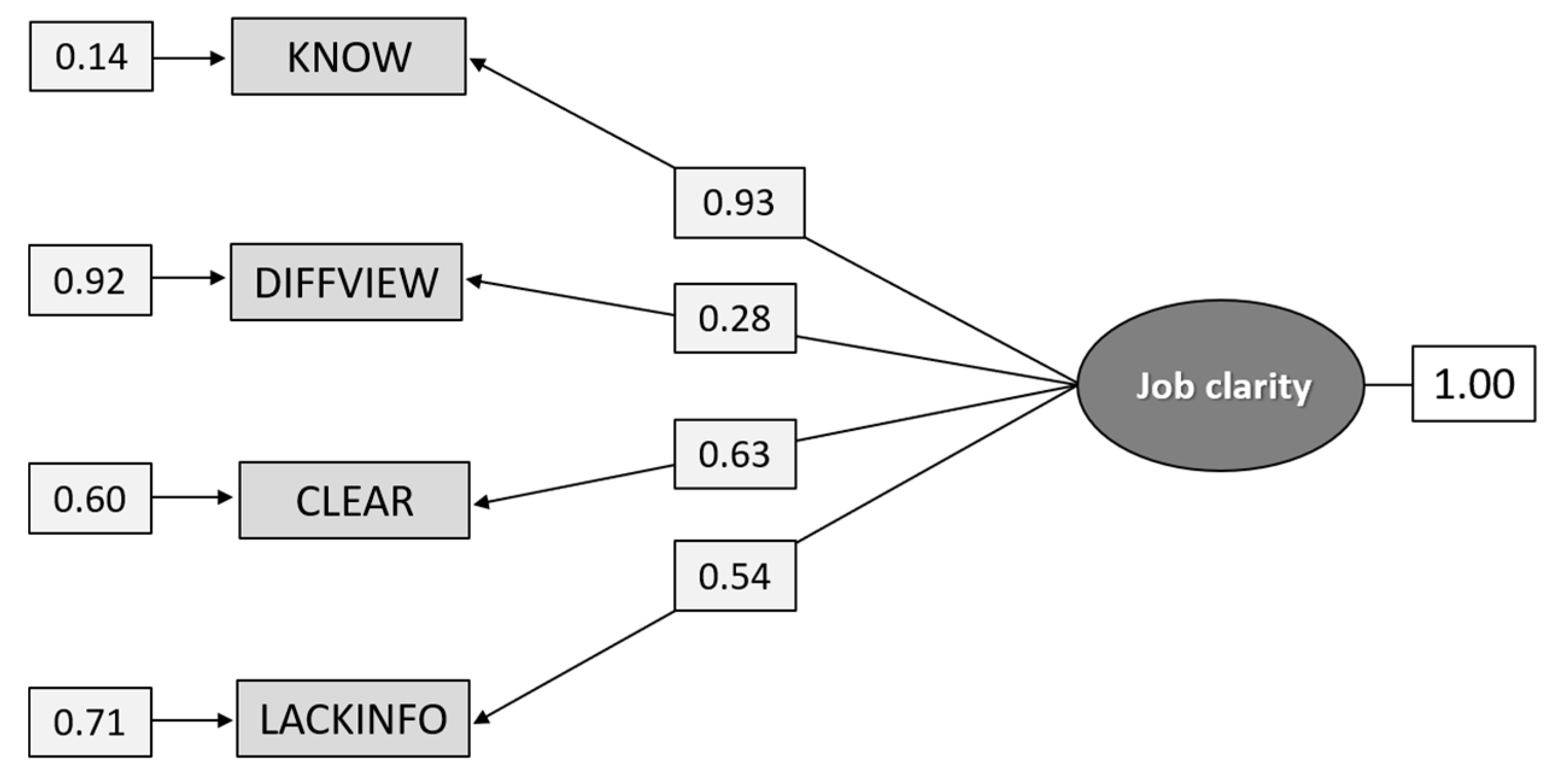
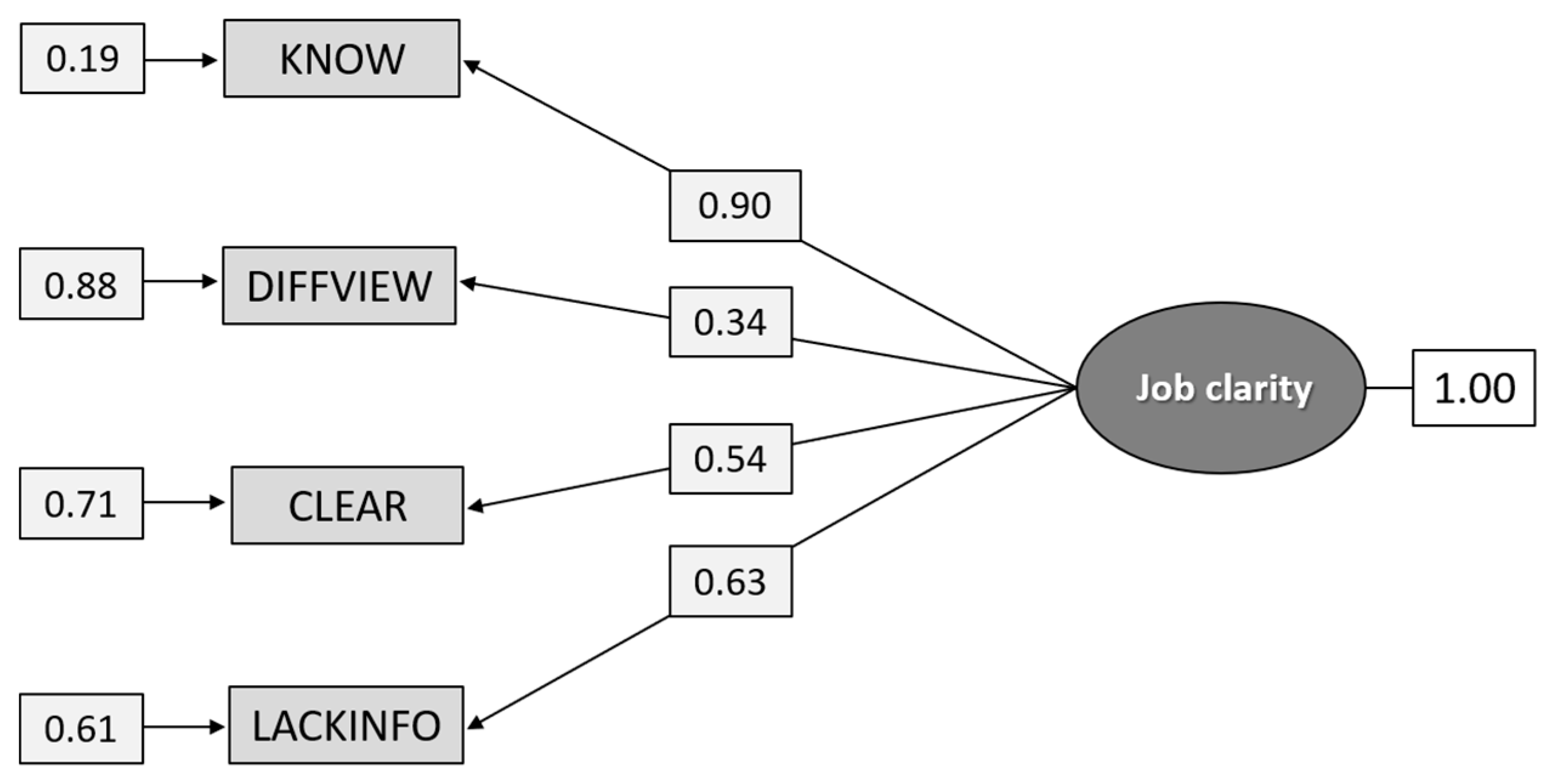
5.1.1. Construct A: Job Clarity
5.1.2. Construct B: Job Confidence
5.1.3. Construct C: Attitudes toward the Possibility to Prevent Suicides
5.1.4. Summary of Cross-Validation Results
5.2. Testing New Hypothesized Measurement Models
5.2.1. Construct D: Job Support
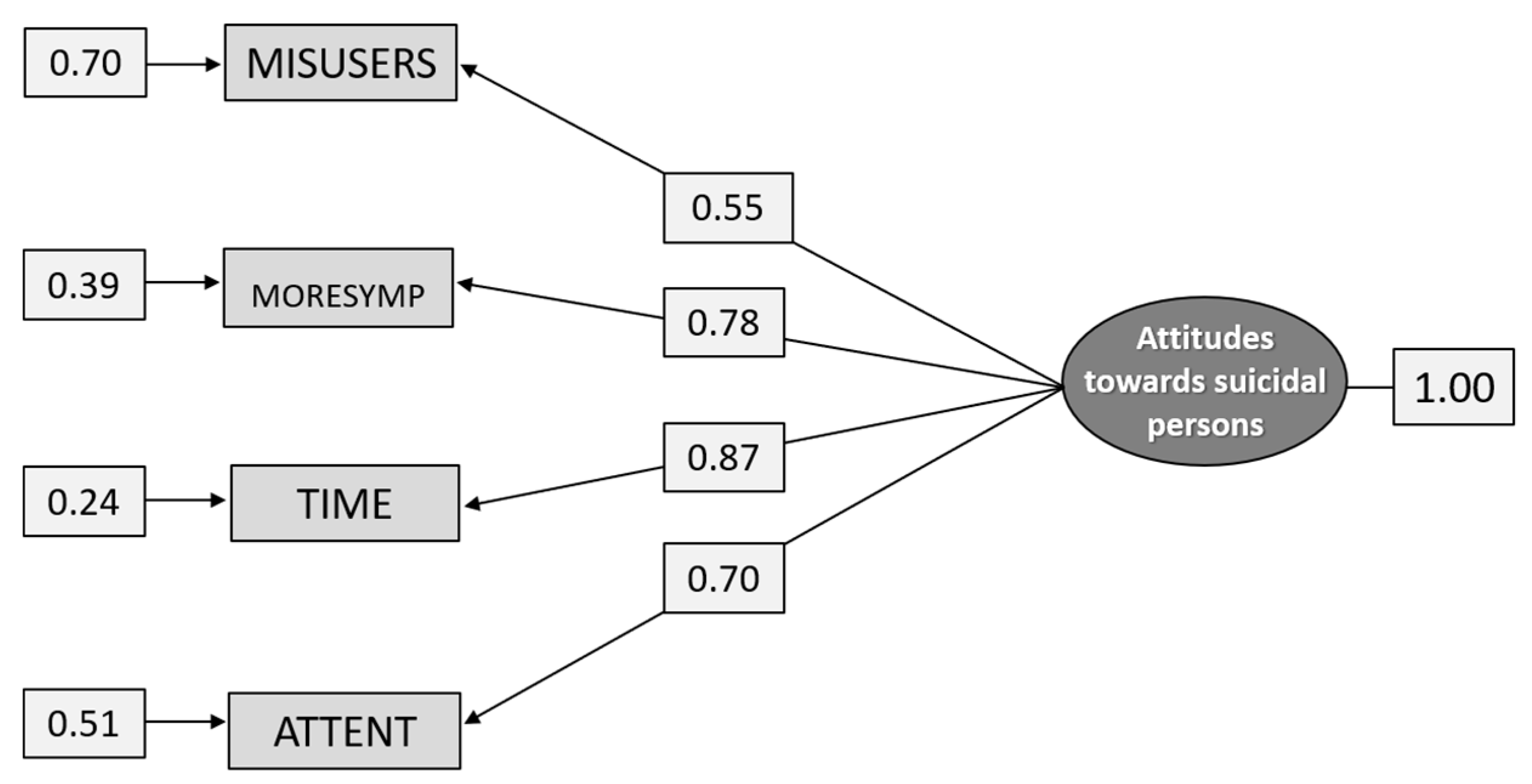
5.2.2. Construct E: Attitudes toward Suicidal Persons
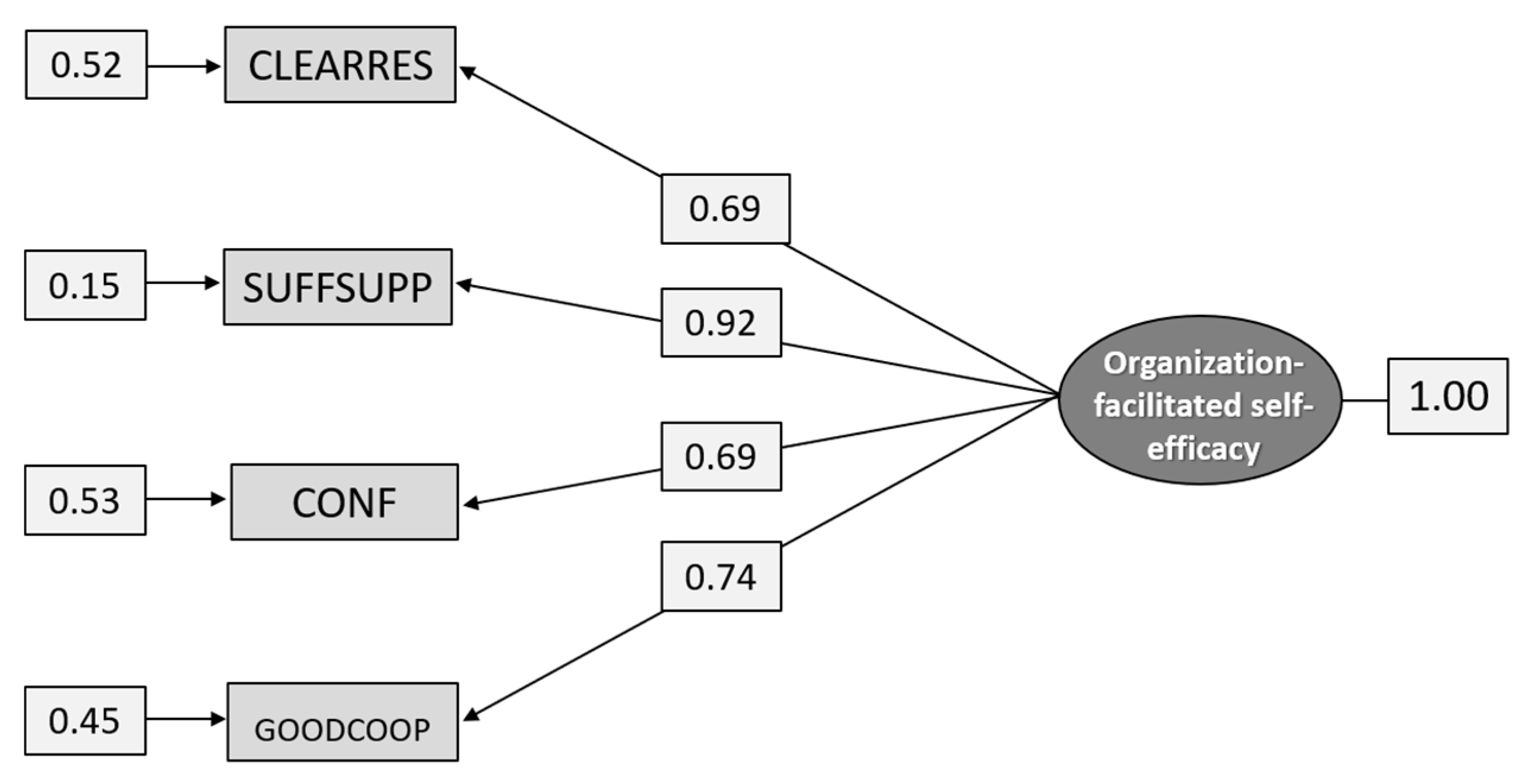
5.3. Reliability Tests of Job Clarity, Organization-Facilitated Self-Efficacy, Attitudes toward Prevention, and Attitudes towards Suicidal Persons
6. Discussion
6.1. Cross-Validations
6.2. Tests of New Measurement Models
6.3. Summary and Scale Development
6.4. Limitations and Future Research
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hegerl, U.; Althaus, D.; Schmidtke, A.; Niklewski, G. The alliance against depression: 2-year evaluation of a community-based intervention to reduce suicidality. Psychol. Med. 2006, 36, 1225–1233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szanto, K.; Kalmar, S.; Hendin, H.; Rihmer, Z.; Mann, M.M. A suicide prevention program in a region with av very high suicide rate. Arch. Gen. Psychiatry 2007, 64, 914–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sueci, H. The relationship between attitudes toward suicide and willingness to pay for suicide prevention: A cross-sectional study in Japan. Psychol. Health Med. 2017, 22, 1072–1081. [Google Scholar]
- Beautrais, A.; Fergusson, D.; Coggan, C. Effective Strategies for suicide prevention in New Zeeland: A review of the evidence. N. Z. Med. J. 2007, 120, U2459. [Google Scholar]
- Maltsberger, J.T.; Buie, D.H. Countertransference hate in the treatment of suicidal patients. Arch. Gen. Psychiat. 1973, 30, 625–633. [Google Scholar] [CrossRef]
- Wolk-Wasserman, D. Some problems connected with the treatment of suicide attempt patients, transference and countertransference aspects. Crisis 1987, 1, 69–82. [Google Scholar]
- McKinley, A.; Couston, M.; Cowan, S. Nurses’ behavioural intentions towards self-poisoning patients: A theory of reasoned action, comparison of attitudes and subjective norms as predictive variables. J. Adv. Nurs. 2001, 34, 107–116. [Google Scholar] [CrossRef]
- Talseth, A.-G. Psychiatric Care of People at Risk for Committing Suicide: Narrative Interviews with Registered Nurses, Physicians, Patients and Their Relatives. Ph.D. Thesis, Umeå University, Umeå, Sweden, 2001. [Google Scholar]
- Wasserman, D. A stress-vulnerability model and the development of the suicidal process. In Suicide—An Unnecessary Death; Wasserman, D., Ed.; Martin Dunitz: London, UK, 2001; pp. 13–27. [Google Scholar]
- Goldblatt, M.J.; Maltsberger, J.T. Countertransference in the treatment of suicidal patients. In Oxford Textbook of Suicidology and Suicide Prevention. A Global Perspective, 2nd ed.; Wasserman, D., Wasserman, C., Eds.; Oxford University Press: Oxford, UK, 2013; pp. 389–393. [Google Scholar]
- Titelman, D.; Wasserman, D. Suicide prevention by education and the moulding of attitudes. In Oxford Textbook of Suicidology and Suicide Prevention. A Global Perspective, 2nd ed.; Wasserman, D., Wasserman, C., Eds.; Oxford University Press: Oxford, UK, 2013; pp. 509–514. [Google Scholar]
- Rokeach, M. Beliefs, Attitudes and Values. In A Theory of Organization and Change; Ossey-Bas: San Francisco, CA, USA, 1968. [Google Scholar]
- Manstead, A.S.R. Attitudes and behavior. In Applied Social Psychology; Semin, G.R., Fiedler, K., Eds.; SAGE Publications Ltd.: London, UK, 1996; pp. 3–29. [Google Scholar]
- Ramberg, I.-L.; Di Lucca, M.A.; Hadlaczky, G. The Impact of Knowledge of Suicide Prevention and Work Experience among Clinical Staff on Attitudes towards Working with Suicidal Patients and Suicide Prevention. Int. J. Environ. Res. Public Health 2016, 13, 195. [Google Scholar] [CrossRef] [Green Version]
- Domino, G.; Moore, D.; Westlake, L.; Gibson, L. Attitudes toward suicide: A factor analytic approach. J. Clin. Psychol. 1982, 38, 257–262. [Google Scholar] [CrossRef]
- Diekstra, R.F.W.; Kerkhof, A.J.F.M. Attitudes towards suicide. The development of a suicide-attitude questionnaire [SUIATT]. In Current Issues of Suicidology; Möller, H.-J., Schmidke, A., Welz, R., Eds.; Springer: Berlin/Heidelberg, Germany, 1988; pp. 466–472. [Google Scholar] [CrossRef]
- Renberg Salander, E.; Jakobsson, L. Development of a Questionnaire on Attitudes Towards Suicide [ATTS] and Its Application in a Swedish Population. Suicide Life-Threat. Behav. 2003, 33, 52–64. [Google Scholar] [CrossRef]
- Boukouvalas, E.; El-Den, S.; Murphy, A.L.; Salvador-Carulla, L.; O’Reilly, C.L. Exploring Health Care Professionals’ Knowledge of, Attitudes Towards, and Confidence in Caring for People at Risk of Suicide: A Systematic Review. Arch. Suicide Res. 2020, 20, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Samuelsson, M.; Åsberg, M.; Gustavsson, J.P. Attitudes of psychiatric nursing personnel towards patients who have attempted suicide. Acta Psychiatr. Scand. 1997, 95, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Hernández, J.A.; Navarro-Ruíz, J.M.; Torrente, G.; Rodríguez, A. Construcción de un cuestionario de creencias actitudinales sobre el comportamiento suicida: El CCCS-18. Psicothema 2005, 17, 684–690. (In Spanish) [Google Scholar]
- Batterham, P.J.; Calear, A.L.; Christensen, H. The Stigma of Suicide Scale. Psychometric properties and correlates of the stigma of suicide. Crisis 2013, 34, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Li, X.Y.; Phillips, M.R.; Niu, Y.J.; Wang, Z.Q.; Tong, Y.S.; Zhang, Y.L.; Xu, D.; Wang, S.L.; Yang, P.D.; Li, C. Development and application of the Scale of Public Attitudes about Suicide among community members and college students. CMHJ 2011, 25, 468–475. (In Chinese) [Google Scholar]
- Botega, N.J.; Reginato, D.G.; da Silva, S.V.; da Silva Cais, C.F.; Rapeli, C.B.; Mauro, M.L.F.; Cecconi, J.P.; Stefanello, S. Nursing personnel attitudes towards suicide: The development of a measure scale. Rev. Bras. Psiquitr. 2005, 27, 315–318. [Google Scholar] [CrossRef] [Green Version]
- Herron, J.; Ticehurst, H.; Appleby, L.; Perry, A.; Cordingley, L. Attitudes toward suicide prevention in front line health staff. Suicide Life-Threat. Behav. 2001, 31, 342–347. [Google Scholar] [CrossRef]
- Griffiths, K.M.; Christensen, H.; Jorm, A.F.; Evans, K.; Groves, C. Effect of web-based depression literacy and cognitive-behavioural therapy interventions on stigmatizing attitudes to depression. Br. J. Psychiatry 2004, 185, 342–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, E.; Kim, S. Cronbach’s coefficient alpha: Well known but poorly understood. ORM 2015, 18, 207–230. [Google Scholar] [CrossRef]
- Fabrigar, L.R.; Wegener, D.T.; MacCallum, R.C.; Strahan, E.J. Evaluating the use of exploratory factor analysis in psychological research. Psychol. Methods 1999, 4, 272–299. [Google Scholar] [CrossRef]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; The Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Aish, A.-M.; Ramberg, I.-L.; Wasserman, D. Measuring attitudes of mental health-care staff towards suicidal patients. Arch. Suicide Res. 2002, 6, 309–323. [Google Scholar] [CrossRef]
- Spector, P.E. Summated Rating Scale Constructions: An Introduction; Sage University Paper Series on Quantitative Applications in the Social Sciences; Sage: Newbury Park, CA, USA, 1992. [Google Scholar]
- Cwik, J.C.; Till, B.; Bieda, A.; Blackwell, S.E.; Walter, C.; Teismann, T. Measuring attitudes towards suicide: Preliminary evaluation of an attitude towards suicide scale. Compr. Psychiatry 2017, 72, 56–65. [Google Scholar] [CrossRef]
- Biblarz, A.; Brown, R.M.; Biblarz, D.N.; Pilgrim, M.P.; Baldree, B.F. Media influence on attitudes toward suicide. Suicide Life-Threat. Behav. 1991, 21, 374–384. [Google Scholar]
- VanSickle, M.; Tucker, J.; Daruwala, S.; Ghahramanlou-Holloway, M. Development and psychometric evaluation of the Military Suicide Attitudes Questionnaire [MSAQ]. J. Affect. Disord. 2016, 203, 158–165. [Google Scholar] [CrossRef] [Green Version]
- Ji, N.-J.; Hong, Y.-P.; Lee, W.-Y. Comprehensive psychometric examination of the attitudes towards suicide [ATTS] in South Korea. Int. J. Ment. Health Syst. 2016, 10, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Sandford, D.M.; Kirtley, O.J.; Lafit, G.; Thwaites, R. An Investigation into the Factor Structure of the Attitudes to Suicide Prevention Scale. Crisis 2020, 41, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Steiger, J.H. Understanding the limitations of global fit assessment in structural equation modeling. Pers. Individ. Diff. 2007, 42, 893–898. [Google Scholar] [CrossRef]
- Jöreskog, K.G.; Sörbom, D. Analysis of Linear Structural Relationships by Maximum Likelihood and Least Square Methods; Report No. 81–88; Department of Statistics, University of Uppsala: Uppsala, Sweden, 1981. [Google Scholar]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Med. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Hayduk, L.; Cummings, G.G.; Boadu, K.; Pazderka-Robinson, H.; Boulianne, S. Testing! Testing! One, Two, Three—Testing the theory in structural equation models. Pers. Individ. Differ. 2007, 42, 841–850. [Google Scholar] [CrossRef]
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting Structural Equation Modeling and Confirmatory Factor Analysis: A Review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Jackson, D.I.; Purc-Stephenson, R. Reporting Practices in Confirmatory Factor Analysis: An Overview and some Recommendations. Psychol. Methods 2009, 14, 6–23. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M. Structural Equation Modelling: Guidelines for Determining Model Fit. EJBRM 2008, 6, 53–60. [Google Scholar]
- Jöreskog, K.G. Structural Equation Modeling with Ordinal Variables using LISREL. IMS Lecture Notes-Monograph Series. 24; Scientific Software International: Skokie, IL, USA, 2002; revised 2005; Available online: https://ssicentral.com/wp-content/uploads/2020/07/lis_ordinal.pdf (accessed on 16 August 2020). [CrossRef]
- Özdemir, H.F.; Çetin, T.; Ömer, K. The use of polycoric and Pearson correlation matrices in the determination of construct validity of Likert type scales. Turk. J. Educ. 2019, 8, 180–195. [Google Scholar] [CrossRef] [Green Version]
- Ahlberg-Hultén, G.; Theorell, T. Combined somatic and psychiatric care–Effects on personnel treating drug addicts with infectious diseases. J. Occup. Health Psychol. 1997, 3, 263–272. [Google Scholar] [CrossRef]
- Jöreskog, K.G.; Sörbom, D. LISREL 9.30; Scientific Software International, Inc.: Skokie, IL, USA, 2017. [Google Scholar]
- Jöreskog, K.G.; Sörbom, D. LISREL8: Structural Equation Modeling with the SIMPLIS Command Language; Scientific Software International, Inc.: Chicago, IL, USA, 1993. [Google Scholar]
- Satorra, A.; Bentler, P.M. Corrections to test statistics and standard errors in covariance structure analysis. In Latent Variables Analysis: Applications for Developmental Research; von Eye, A., Clogg, C.C., Eds.; Sage: Thousand Oaks, CA, USA, 1994; pp. 339–419. [Google Scholar]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. In Testing Structural Equation Models; Bollen, K.A., Long, J.S., Eds.; Sage: Newbury Park, CA, USA, 1993; pp. 136–162. [Google Scholar]
- Marsh, H.W.; Hau, K.T. Assessing goodness of fit: Is parsimony always desirable? J. Exp. Educ. 1996, 64, 364–390. [Google Scholar] [CrossRef]
- MacCallum, R.C.; Browne, M.W.; Sugawara, H.M. Power Analysis and Determination of Sample Size for Covariance Structure Modeling. Psychol. Methods 1996, 1, 130–149. [Google Scholar] [CrossRef]
- Karasek, R.; Theorell, T. Healthy Work: Stress, Productivity, and the Reconstruction of Working Life; Basic Books: New York, NY, USA, 1990. [Google Scholar]
- Hox, J.J.; Bechger, T.M. An Introduction to Structural Equation Modeling. Fam. Sci. Rev. 1998, 11, 354–373. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Constructs | Items |
|---|---|
| A. Job clarity (The items that define the construct of Job clarity emanate originally from a study of Ahlberg-Hultén and Theorell [46].) | I know what is expected of me in work with suicidal individuals |
| Different superiors have varying views on how and what I shall do in work with suicidal individuals | |
| I get clear and good instructions concerning management of care of suicidal individuals | |
| I lack knowledge and information about what is important in work with suicidal individuals | |
| B. Job confidence | The division of responsibilities for risk assessment is clear and distinct |
| I feel confident when working with suicidal individuals | |
| I have no one with whom I can share the responsibility for the suicidal individuals | |
| The co-operation concerning the suicidal individuals is well functioning | |
| C. Possibility to prevent suicides | It is possible to prevent suicides |
| It makes no difference what is done for suicidal individuals—they succeed sooner or later anyway | |
| If people really want to kill themselves, they will succeed despite receiving the best treatment | |
| Once people have made up their minds to commit suicide, you cannot stop them |
| Constructs | Items/Items |
|---|---|
| D. Job support | I have enough support in work with suicidal individuals |
| I do not know what to do if somebody tells me that he/she want to kill himself/herself | |
| There are enough resources for me to do what is expected of me when I encounter suicidal persons | |
| Due to the ambiguous description of my responsibilities, I’m uncertain as to whether I should find out whether persons are suicidal or not | |
| I feel free to ask for help when I am not sure what to do in my work with suicidal individuals | |
|
E. Attitudes toward suicidal persons | Some suicidal individuals are abusing the health-care system |
| I feel more sympathy for first time suicide attempters than for those who have made several attempts | |
| Suicidal persons often steal time from other persons with greater need for support and help | |
| Those who have made several suicide attempts do not really want to kill themselves | |
| Those who use non-lethal methods to attempt suicide only seek attention |
| Fit Index | Good Fit Values | Acceptable Fit Values |
|---|---|---|
| RMSEA | <0.05 | <0.08 |
| CFI | >0.97 | >0.95 |
| SRMR | <0.05 | <0.08 |
| Item | Factor 1 | Unique Var |
|---|---|---|
| The division of responsibilities for risk assessment is clear and distinct [CLEARRES] | 0.675 | 0.545 |
| I feel confident when working with suicidal individuals [CONF] | 0.714 | 0.490 |
| I have no one with whom I can share the responsibility for the suicidal individuals [ALLRESP] | 0.433 | 0.813 |
| The co-operation concerning the suicidal individuals is well functioning [GOODCOOP] | 0.769 | 0.409 |
| I have enough support in work with suicidal individuals [SUFFSUPP] | 0.902 | 0.186 |
| I do not know what to do if somebody tells me that he/she want to kill himself/herself [NOTKNOW] | 0.367 | 0.865 |
| There are enough resources for me to do what is expected of me when I encounter suicidal persons [SUFFRES] | 0.619 | 0.617 |
| Due to the ambiguous description of my responsibilities, I’m uncertain as to find out whether persons are suicidal or not [UNCLEAR] | 0.416 | 0.827 |
| I feel free to ask for help when I am not sure what to do in my work with suicidal individuals [ASKHELP] | 0.408 | 0.833 |
| Items | Validity | Reliability |
|---|---|---|
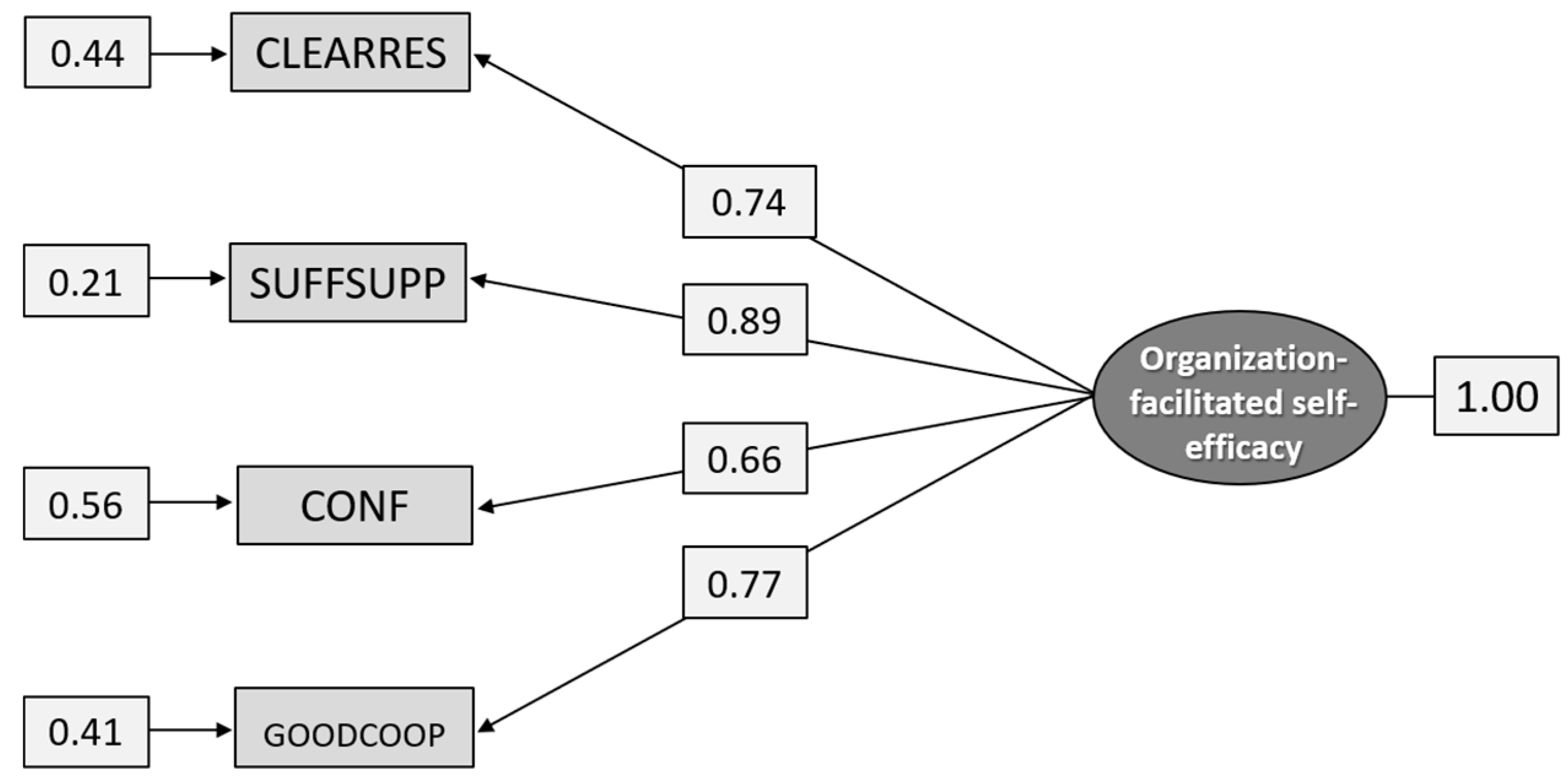
| The division of responsibilities for risk assessment is clear and distinct [CLEARRES] | 0.71 | 0.51 |
| I have enough support in work with suicidal individuals [SUFFSUPP] | 0.90 | 0.82 |
| I feel confident when working with suicidal individuals [CONF] | 0.65 | 0.42 |
| The co-operation concerning the suicidal individuals is well functioning [GOODCOOP] | 0.72 | 0.52 |
| Model fit: χ2 = 0.216 [2], p = 0.8976, RMSEA = 0.0, p = 0.943, CI = 0.0–0.05, CFI = 1.00, SRMR = −0.00453 | ||
| Items | Validity | Reliability |
|---|---|---|
| Some suicidal individuals are abusing the health-care system [MISUSERS] | 0.52 | 0.27 |
| I feel more sympathy for first time suicide attempters than for those who have made several attempts [MORESYMP] | 0.81 | 0.65 |
| Suicidal persons often steal time from other persons with greater need for support and help [TIME] | 0.85 | 0.72 |
| Those who use non-lethal methods to attempt suicide only seek attention [ATTENT] | 0.73 | 0.53 |
| Model fit: χ2[df = 2] = 2.964, p = 0.2272, RMSEA = 0.0793, p = 0.126, [CI 0.0346–0.132], CFI = 0.999, SRMR = 0.0216 | ||
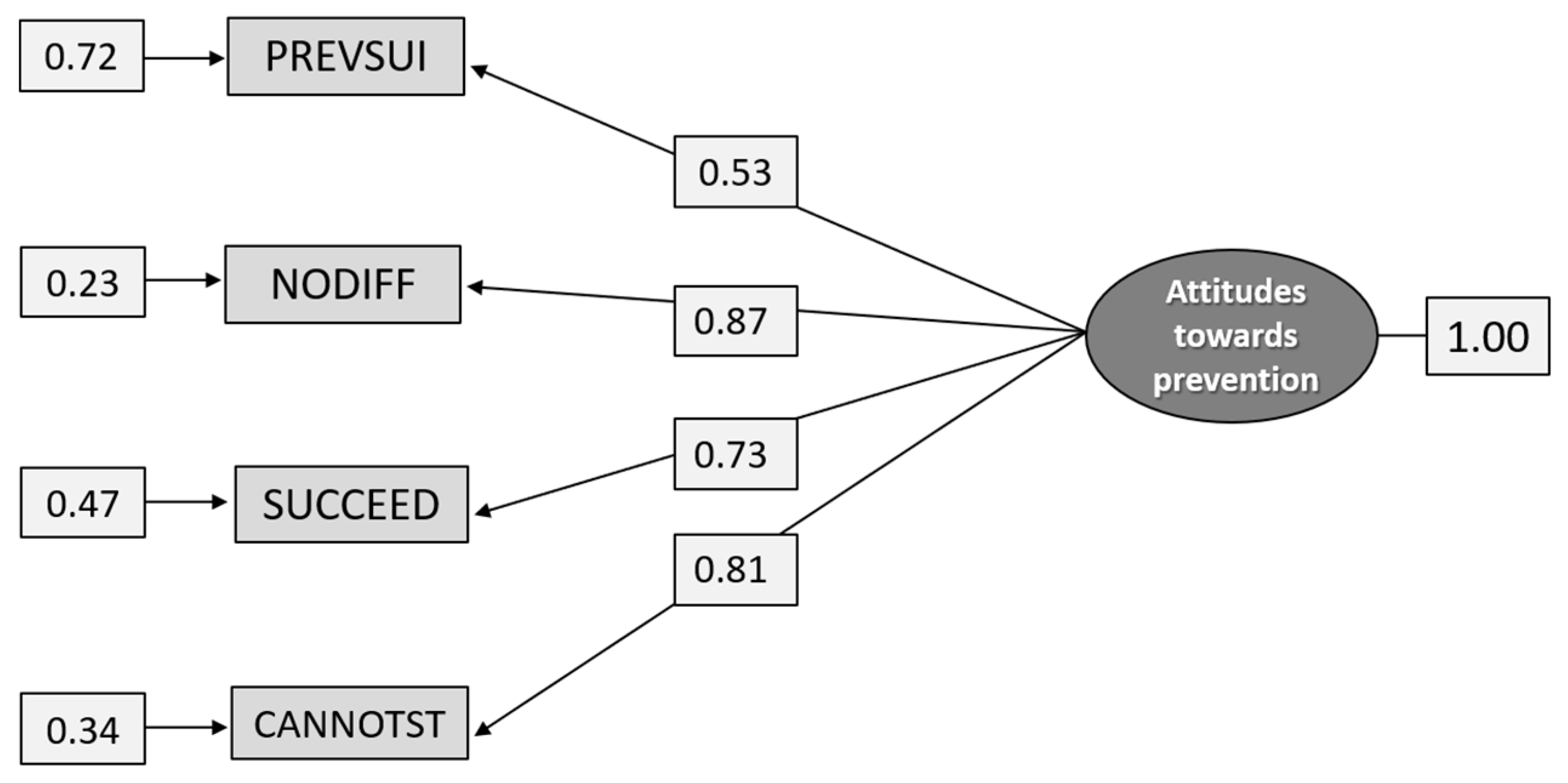
| Attitudes toward prevention |
|
| Attitudes toward suicidal persons |
|
| Organization-facilitated self-efficacy |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramberg, I.-L.; Hökby, S.; Karlsson, L.; Hadlaczky, G. Measuring Attitudes toward Suicide Prevention among Occupational Staff Frequently Exposed to Suicidal Individuals: Psychometric Evaluation and Validation. Int. J. Environ. Res. Public Health 2021, 18, 4001. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084001
Ramberg I-L, Hökby S, Karlsson L, Hadlaczky G. Measuring Attitudes toward Suicide Prevention among Occupational Staff Frequently Exposed to Suicidal Individuals: Psychometric Evaluation and Validation. International Journal of Environmental Research and Public Health. 2021; 18(8):4001. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084001
Chicago/Turabian StyleRamberg, Inga-Lill, Sebastian Hökby, Linda Karlsson, and Gergö Hadlaczky. 2021. "Measuring Attitudes toward Suicide Prevention among Occupational Staff Frequently Exposed to Suicidal Individuals: Psychometric Evaluation and Validation" International Journal of Environmental Research and Public Health 18, no. 8: 4001. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084001