
An IoT Framework for Screening of COVID-19 Using Real-Time Data from Wearable Sensors



Abstract
:1. Introduction
1.1. Importance of Remote Screening
1.2. Detection of COVID-19 Using Wearable Devices
1.3. Novel Contributions of this Work
2. Background and Related Work
2.1. The Difference between the Symptoms of the New Coronavirus (SARS-CoV-2) and Influenza
2.2. Techniques Currently Used for the Detection of COVID-19
2.3. Using Rules for COVID-19 Detection
2.4. Other Proposed Alternatives (Under Investigation) for the Detection of COVID-19
- Use of electrochemical sensors [40]: Traditionally, respiratory infections have been identified by a range of methodologies [41] such as staining, direct fluorescence antibody, etc. Such techniques require costly chemicals and materials, time-consuming preparation of samples, and skilled staff. To tackle these disadvantages, methods like surface plasmon resonance [42], interferometry [43], and field effect transistor [44] were adopted for virus detection. All these methods depend on specialized devices.
- Use of Smartphone Sensors A new mechanism was proposed for detecting COVID-19 using smartphone sensors in [45]. The proposal offers a cheaper solution, as most radiologists already have smart phones available for various everyday purposes. Not only this, but normal individuals can use the system for virus detection purposes on their phones.
- Use of Smart Thermometers: In [46], the authors compared smart thermometers and mobile device data to regional influenza and “influenza-like illness” (ILI) monitoring. Similarly in [47], a group of researchers proposed a methodology to identify anomalously high levels of ILI in real-time, at the scale of US counties. Using data from a geospatial network of thermometers involving more than one million users across the US, they identified anomalies by producing precise, county-specific predictions of seasonal ILI from a point before a possible outbreak. Anomalies are strongly correlated with COVID-19 case counts and could provide an early-warning mechanism for locating the epicenters of future possible outbreaks.
- Wearable Medical Sensors (WMS): A WMS based solution called EasyBand [48] has recently been proposed to restrict the growth of new positive cases by tracking auto-contact and supporting critical social distancing. In an other recent work [49,50], the authors proposed a solution called CovidDeep which uses commercial WMSs for the detection of the COVID-19 virus. Similarly, the authors of [51] developed an application that gathers self-reported symptoms as well as smartwatch and activity tracker data in order to differentiate between COVID-19 negative and positive cases in symptomatic persons.
- Use of Cough Recognition Techniques: Cough [52] is a characteristic of varied respiratory infections from a common cold to the latest coronavirus infection. Not only does cough exist in humans, but it has been equally found to exist in many species [53]. In the work presented in [54], the authors presented a new technique which detects coughs using a “K-band continuous-wave Doppler radar”. Similarly in [55], a group of scientists have developed an AI model which detects the COVID-19 virus from a forced cough.
- Use of Arduino and IoT: Magesh et al. [56] used sensors to monitor the temperature and respiratory rate of the COVID-19 cases to develop the mathematical model called the epidemic Susceptible, Infected and Recovered (SIR) to classify the COVID-19 cases in one of the three SIR categories. However, as we describe earlier, temperature and respiratory rates are not sufficient to detect COVID-19 cases. On the same pattern, Al-Shalabi used the temperature sensor to detect COVID-19 [57], which is not an accurate and reliable solution. Ref. [58] proposed an IoT-based solution aiming to increase COVID-19 indoor safety by analysing contactless temperature sensing, mask detection, social distancing check. The temperature sensing relied on Arduino using an infrared sensor or a thermal camera, while mask detection and social distancing checks were performed by leveraging computer vision techniques. The solution could only be helpful in prevention of COVID-19 but could not support COVID-19 diagnosis.
3. IoT Framework for Remote Screening of COVID-19
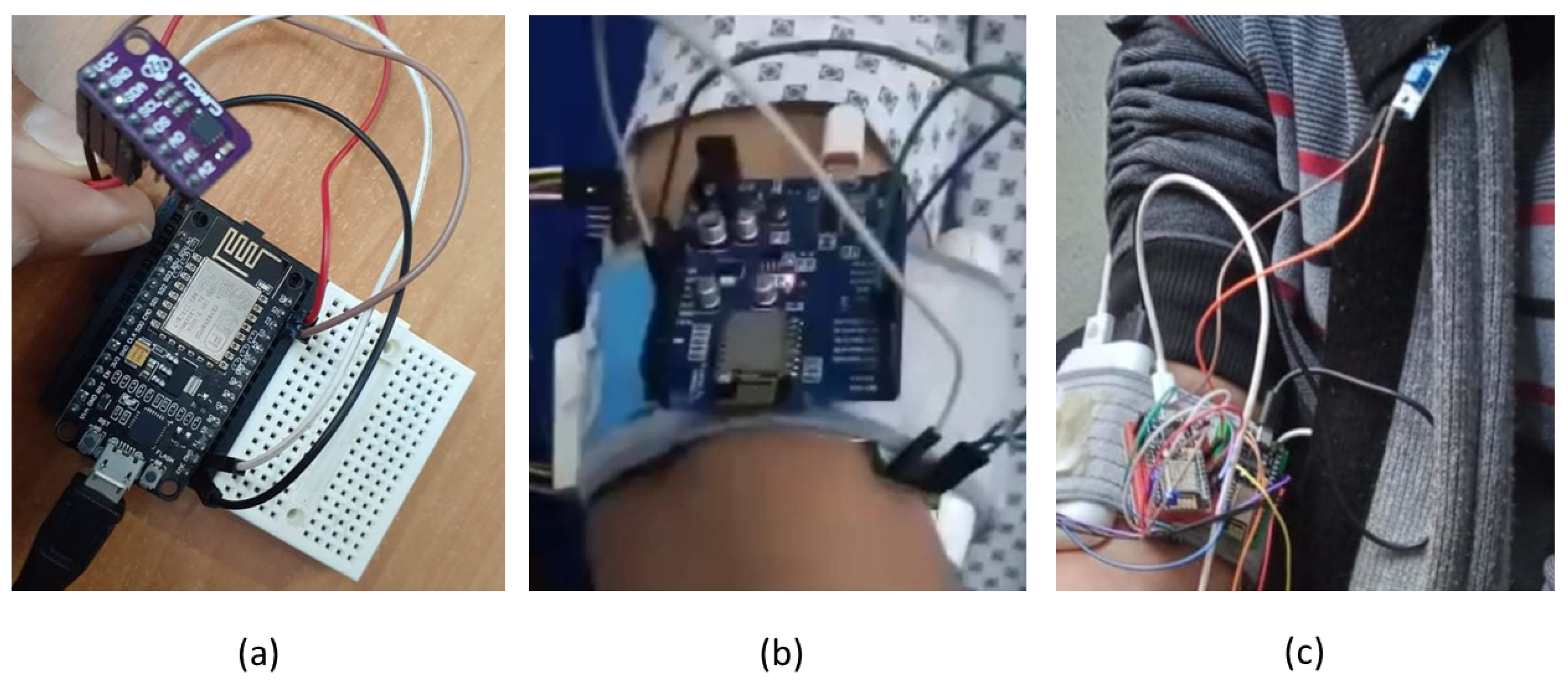
3.1. The COVID-19 Screening Device
3.2. The Rule-Based Analysis of COVID-19
- Class 0: Non-symptomatic
- -
- SpO ;
- -
- Cough Rate: NIL;
- -
- Heartbeat Rate bpm;
- -
- Temperature ≤ 37.2 C;
- -
- No headache and pains.
- -
- No comorbidities.
- Class 1: Mild symptoms
- -
- SpO;
- -
- Cough Rate min;
- -
- Heartbeat Rate bpm;
- -
- 36 C ≤ Temperature ≤ 38 C;
- -
- No shortness of breath.
- -
- No comorbidities
- Class 2: Moderate clinical symptoms
- -
- SpO ;
- -
- 5/min ≤ Cough Rate min;
- -
- Heartbeat Rate > 100 bpm;
- -
- Temperature ≥ 38 C.
- Class 3: Serious clinical symptoms
- -
- SpO ;
- -
- Cough Rate ≥ 30/min;
- -
- Heartbeat Rate bpm;
- -
- Temperature > 38 C.
- -
- Occurrence of comorbidities.
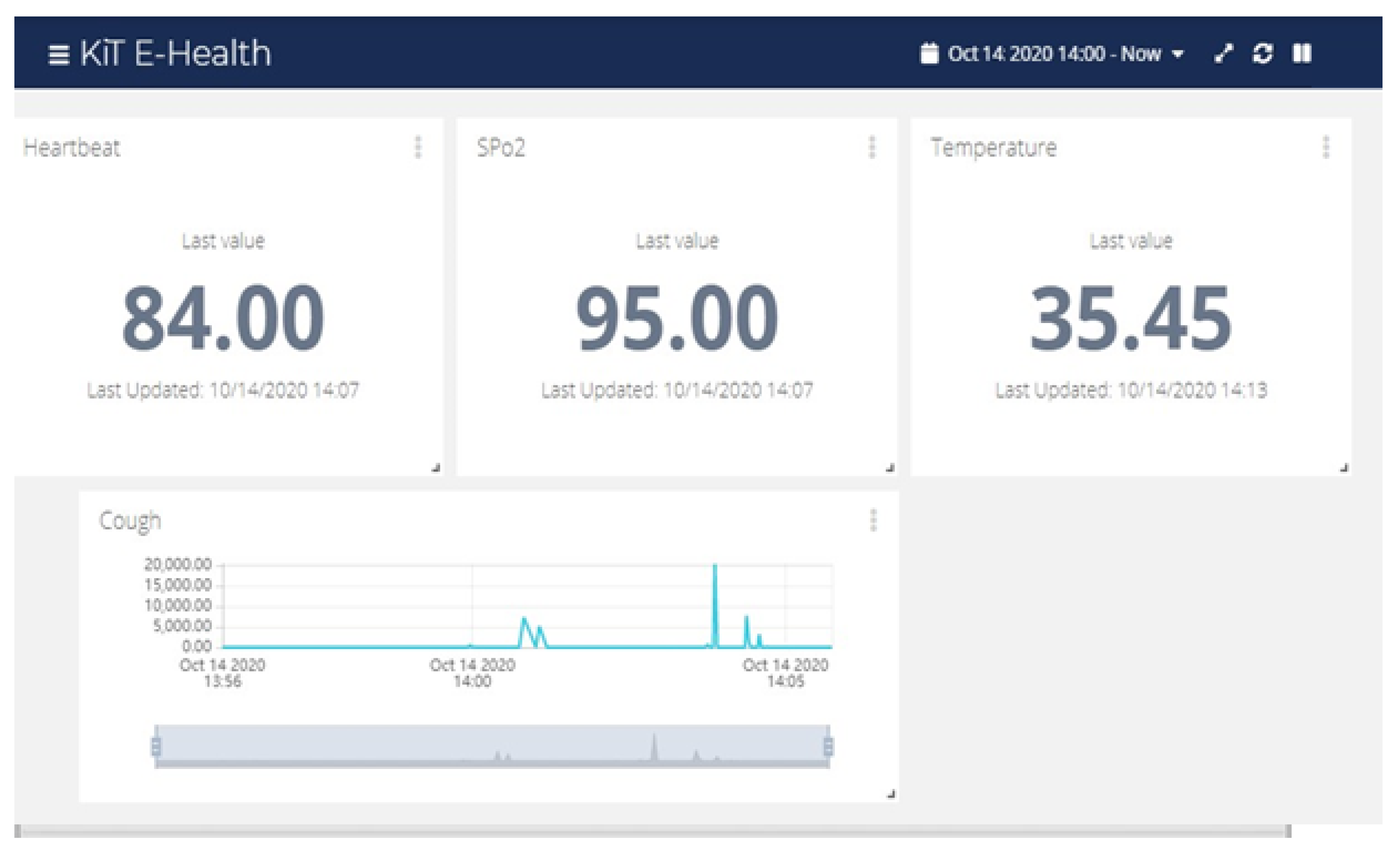
3.3. Real-Time Screening: Analysis and Visualization
4. The Hardware and Software Architectural Components
4.1. The Hardware Components
4.2. The Software Components
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lescure, F.X.; Bouadma, L.; Nguyen, D.; Parisey, M.; Wicky, P.H.; Behillil, S.; Gaymard, A.; Bouscambert-Duchamp, M.; Donati, F.; Le Hingrat, Q.; et al. Clinical and virological data of the first cases of COVID-19 in Europe: A case series. Lancet Infect. Dis. 2020, 20, 697–706. [Google Scholar] [CrossRef] [Green Version]
- CDC (Centers for Diseases Control and Prevention). About Variants of the Virus That Causes COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/transmission/variant.html (accessed on 3 April 2021).
- Anchordoqui, L.A.; Dent, J.B.; Weiler, T.J. A physics modeling study of SARS-CoV-2 transport in air. arXiv 2020, arXiv:2007.05410. [Google Scholar]
- Bahl, P.; Doolan, C.; de Silva, C.; Chughtai, A.A.; Bourouiba, L.; MacIntyre, C.R. Airborne or droplet precautions for health workers treating COVID-19? J. Infect. Dis. 2020. review. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, C.; Zhai, Z. The efficacy of social distance and ventilation effectiveness in preventing COVID-19 transmission. Sustain. Cities Soc. 2020, 62, 102390. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.M.; Vinetz, J.M. Dexamethasone in the management of covid-19. BMJ 2020. [Google Scholar] [CrossRef]
- Gottlieb, S.; Rivers, C.; McClellan, M.B.; Silvis, L.; Watson, C. National coronavirus response: A road map to reopening. In AEI Paper & Studies; GALE: Farmington Hills, Michigan, 2020. [Google Scholar]
- Zhu, Y.; Chen, L.; Ji, H.; Xi, M.; Fang, Y.; Li, Y. The risk and prevention of novel coronavirus pneumonia infections among inpatients in psychiatric hospitals. Neurosci. Bull. 2020, 36, 299–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.; Liu, J.Q.; Wen, H.J.; Liu, H.; Hu, W.D.; Han, X.; Li, C.X.; Wang, X.J. The unsynchronized changes of CT image and nucleic acid detection in COVID-19: Reports the two cases from Gansu, China. Respir. Res. 2020, 21, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Gyorfi, A.H. Relapse of coronavirus disease-2019 following misuse of prednisolone: Case report. Reactions 1816, 278, 2020. [Google Scholar]
- Jiang, F.; Deng, L.; Zhang, L.; Cai, Y.; Cheung, C.W.; Xia, Z. Review of the clinical characteristics of coronavirus disease 2019 (COVID-19). J. Gen. Int. Med. 2020, 35, 1545–1549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singhal, T. A review of coronavirus disease-2019 (COVID-19). Indian J. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Hu, Z.; Song, C.; Xu, C.; Jin, G.; Chen, Y.; Xu, X.; Ma, H.; Chen, W.; Lin, Y.; Zheng, Y.; et al. Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci. China Life Sci. 2020, 63, 706–711. [Google Scholar] [CrossRef] [Green Version]
- Gavriatopoulou, M.; Korompoki, E.; Fotiou, D.; Ntanasis-Stathopoulos, I.; Psaltopoulou, T.; Kastritis, E.; Terpos, E.; Dimopoulos, M.A. Organ-specific manifestations of COVID-19 infection. Clin. Exp. Med. 2020, 20, 493–506. [Google Scholar] [CrossRef]
- Qiu, P.; Zhou, Y.; Wang, F.; Wang, H.; Zhang, M.; Pan, X.; Zhao, Q.; Liu, J. Clinical characteristics, laboratory outcome characteristics, comorbidities, and complications of related COVID-19 deceased: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2020, 32, 1869–1878. [Google Scholar] [CrossRef]
- Bhagat, S.; Yadav, N.; Shah, J.; Dave, H.; Swaraj, S.; Tripathi, S.; Singh, S. Novel coronavirus (COVID-19) pandemic: Current status and possible strategies for detection and treatment of the disease. Expert Rev. Anti Infect. Ther. 2020. [Google Scholar] [CrossRef] [PubMed]
- Barh, D.; Tiwari, S.; Andrade, B.S.; Weener, M.E.; Goes-Neto, A.; Azevedo, V.; Ghosh, P.; Ganguly, N.K. A novel multi-omics-based identification of symptoms, comorbid conditions, and possible long-term complications in COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Hejaz, H.A. Treatments And Management Of Coronavirus Disease 2019 (COVID-19). Int. J. Med. Sci. Diagn. Res. 2020, 4, 7. [Google Scholar]
- De Angelis, G.; Posteraro, B.; Biscetti, F.; Ianiro, G.; Dal Verme, L.Z.; Cattani, P.; Franceschi, F.; Sanguinetti, M.; Gasbarrini, A. Confirmed or unconfirmed cases of 2019 novel coronavirus pneumonia in Italian patients: A retrospective analysis of clinical features. BMC Infect. Dis. 2020, 20, 775. [Google Scholar] [CrossRef]
- Shorfuzzaman, M.; Masud, M. On the detection of covid-19 from chest X-ray images using cnn-based transfer learning. Comput. Mater. Contin. 2020, 64. [Google Scholar] [CrossRef]
- Maia Chagas, A.; Molloy, J.C.; Prieto-Godino, L.L.; Baden, T. Leveraging open hardware to alleviate the burden of COVID-19 on global health systems. PLoS Biol. 2020, 18, e3000730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belhouideg, S. Impact of 3D printed medical equipment on the management of the Covid 19 pandemic. Int. J. Health Plan. Manag. 2020, 35, 1014–1022. [Google Scholar] [CrossRef] [PubMed]
- Rabiee, N.; Bagherzadeh, M.; Ghasemi, A.; Zare, H.; Ahmadi, S.; Fatahi, Y.; Dinarvand, R.; Rabiee, M.; Ramakrishna, S.; Shokouhimehr, M.; et al. Point-of-use rapid detection of sars-cov-2: Nanotechnology-enabled solutions for the covid-19 pandemic. Int. J. Mol. Sci. 2020, 21, 5126. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, R.; Bastin, G.; Chrzanowski, A. ALERT-A fully automated real time monitoring system. In Proceedings of the 11th FIG Symposium on Deformation Measurements, Santorini, Greece, 25–28 May 2003; pp. 25–28. [Google Scholar]
- Stonebraker, M.; Çetintemel, U.; Zdonik, S. The 8 requirements of real-time stream processing. ACM Sigmod Rec. 2005, 34, 42–47. [Google Scholar] [CrossRef] [Green Version]
- Sun, S.; Cao, Z.; Zhu, H.; Zhao, J. A survey of optimization methods from a machine learning perspective. IEEE Trans. Cybern. 2019, 50, 3668–3681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Struyf, T.; Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Leeflang, M.M.; Spijker, R.; Hooft, L.; Emperador, D.; Dittrich, S.; et al. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19 disease. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef]
- Qu, J.M.; Wang, C.; Cao, B. Guidance for the management of adult patients with coronavirus disease 2019. Chin. Med. J. 2020, 133, 1575. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Kumar, M.; Kumar Dubey, A. Effect of pre-existing diseases on COVID-19 infection and role of new sensors and biomaterials for its detection and treatment. Med. Dev. Sens. 2020, 4, e10140. [Google Scholar] [CrossRef]
- Wan, Z.; Zhang, Y.; He, Z.; Liu, J.; Lan, K.; Hu, Y.; Zhang, C. A melting curve-based multiplex RT-qPCR assay for simultaneous detection of four human coronaviruses. Int. J. Mol. Sci. 2016, 17, 1880. [Google Scholar] [CrossRef] [Green Version]
- Tahamtan, A.; Ardebili, A. Real-time RT-PCR in COVID-19 detection: Issues affecting the results. Expert Rev. Mol. Diagn. 2020, 20, 453–454. [Google Scholar] [CrossRef] [Green Version]
- Bælum, J.; Jacobsen, C.S. TaqMan probe-based real-time PCR assay for detection and discrimination of class I, II, and III tfdA genes in soils treated with phenoxy acid herbicides. Appl. Environ. Microbiol. 2009, 75, 2969–2972. [Google Scholar] [CrossRef] [Green Version]
- Yu, Y.; Bu, F.; Zhou, H.; Wang, Y.; Cui, J.; Wang, X.; Nie, G.; Xiao, H.H. Biosafety Materials: An Emerging New Research Direction of Materials Science from COVID-19 Outbreak. Mater. Chem. Front. 2020, 4, 1903–1953. [Google Scholar] [CrossRef]
- Taylor, S.C.; Laperriere, G.; Germain, H. Droplet Digital PCR versus qPCR for gene expression analysis with low abundant targets: From variable nonsense to publication quality data. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Park, S.R.; Yoon, Y.J.; Pham, J.V.; Yilma, M.A.; Feliz, A.; Majid, M.T.; Maffetone, N.; Walker, J.R.; Kim, E.; Reynolds, J.M.; et al. A review of the microbial production of bioactive natural products and biologics. Front. Microbiol. 2019, 10, 1404. [Google Scholar]
- Banjar, H.R.; Alkhatabi, H.; Alganmi, N.; Almouhana, G.I. Prototype Development of an Expert System of Computerized Clinical Guidelines for COVID-19 Diagnosis and Management in Saudi Arabia. Int. J. Environ. Res. Pub. Health 2020, 17, 8066. [Google Scholar] [CrossRef] [PubMed]
- Salman, F.M.; Abu-Naser, S.S. Expert System for COVID-19 Diagnosis. Int. J. Acad. Inf. Syst. Res. IJAISR 2020, 4, 1–13. [Google Scholar]
- Chakraborty, C.; Banerjee, A.; Garg, L.; Rodrigues, J.J. Internet of Medical Things for Smart Healthcare. In Studies in Big Data; Springer: Cham, Switzerland, 2020; Volume 80. [Google Scholar]
- Manta, C.; Jain, S.S.; Coravos, A.; Mendelsohn, D.; Izmailova, E.S. An Evaluation of Biometric Monitoring Technologies for Vital Signs in the Era of COVID-19. Clin. Transl. Sci. 2020, 13, 1034–1044. [Google Scholar] [CrossRef] [PubMed]
- Santhanam, K.S.V. Electrochemical approaches towards sensing viruses: A mini review. Med. Dev. Sens. 2020, 4, e10148. [Google Scholar] [CrossRef]
- Jartti, T.; Söderlund-Venermo, M.; Hedman, K.; Ruuskanen, O.; Mäkelä, M.J. New molecular virus detection methods and their clinical value in lower respiratory tract infections in children. Paediatr. Respir. Rev. 2013, 14, 38–45. [Google Scholar] [CrossRef]
- Yakes, B.J.; Papafragkou, E.; Conrad, S.M.; Neill, J.D.; Ridpath, J.F.; Burkhardt, W., III; Kulka, M.; DeGrasse, S.L. Surface plasmon resonance biosensor for detection of feline calicivirus, a surrogate for norovirus. Int. J. Food Microbiol. 2013, 162, 152–158. [Google Scholar] [CrossRef]
- Auer, S.; Koho, T.; Uusi-Kerttula, H.; Vesikari, T.; Blazevic, V.; Hytönen, V.P. Rapid and sensitive detection of norovirus antibodies in human serum with a biolayer interferometry biosensor. Sens. Actuators B Chem. 2015, 221, 507–514. [Google Scholar] [CrossRef] [Green Version]
- Xiang, L.; Wang, Z.; Liu, Z.; Weigum, S.E.; Yu, Q.; Chen, M.Y. Inkjet-printed flexible biosensor based on graphene field effect transistor. IEEE Sens. J. 2016, 16, 8359–8364. [Google Scholar] [CrossRef]
- Maghded, H.S.; Ghafoor, K.Z.; Sadiq, A.S.; Curran, K.; Rawat, D.B.; Rabie, K. A Novel AI-enabled Framework to Diagnose Coronavirus COVID-19 using Smartphone Embedded Sensors: Design Study. In Proceedings of the 2020 IEEE 21st International Conference on Information Reuse and Integration for Data Science (IRI), Las Vegas, NV, USA, 11–13 August 2020; pp. 180–187. [Google Scholar] [CrossRef]
- Ackley, S.F.; Pilewski, S.; Petrovic, V.S.; Worden, L.; Murray, E.; Porco, T.C. Assessing the utility of a smart thermometer and mobile application as a surveillance tool for influenza and influenza-like illness. Health Inf. J. 2020, 26, 2148–2158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamberlain, S.; Singh, I.; Ariza, C.; Daitch, A.; Philips, P.; Dalziel, B.D. Real-time detection of COVID-19 epicenters within the United States using a network of smart thermometers. medRxiv 2020. [Google Scholar] [CrossRef]
- Tripathy, A.K.; Mohapatra, A.G.; Mohanty, S.P.; Kougianos, E.; Joshi, A.M.; Das, G. EasyBand: A Wearable for Safety-Aware Mobility During Pandemic Outbreak. IEEE Consum. Electron. Mag. 2020, 9, 57–61. [Google Scholar] [CrossRef]
- Hassantabar, S.; Stefano, N.; Ghanakota, V.; Ferrari, A.; Nicola, G.N.; Bruno, R.; Marino, I.R.; Hamidouche, K.; Jha, N.K. CovidDeep: SARS-CoV-2/COVID-19 Test Based on Wearable Medical Sensors and Efficient Neural Networks. arXiv 2020, arXiv:2007.10497. [Google Scholar]
- Karthickraja, R.; Kumar, R.; Kirubakaran, S.; Manikandan, R.; Marcilin, J.A.L. COVID-19 prediction and symptom analysis using wearable sensors and IoT. Int. J. Pervasive Comput. Commun. 2020. [Google Scholar] [CrossRef]
- Quer, G.; Radin, J.M.; Gadaleta, M.; Baca-Motes, K.; Ariniello, L.; Ramos, E.; Kheterpal, V.; Topol, E.J.; Steinhubl, S.R. Passive monitoring of physiological data and self-reported symptoms to detect clusters of people with COVID-19. Nat. Med. 2021, 27, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Preethi, S.; Revathi, A.; Murugan, M. Exploration of Cough Recognition Technologies Grounded on Sensors and Artificial Intelligence. In Internet of Medical Things for Smart Healthcare; Springer: Berlin, Germany, 2020; pp. 193–214. [Google Scholar]
- Carpentier, L.; Berckmans, D.; Youssef, A.; Berckmans, D.; van Waterschoot, T.; Johnston, D.; Ferguson, N.; Earley, B.; Fontana, I.; Tullo, E.; et al. Automatic cough detection for bovine respiratory disease in a calf house. Biosyst. Eng. 2018, 173, 45–56. [Google Scholar] [CrossRef]
- Chuma, E.L.; Iano, Y. A Movement Detection System Using Continuous-Wave Doppler Radar Sensor and Convolutional Neural Network to Detect Cough and Other Gestures. IEEE Sens. J. 2020. [Google Scholar] [CrossRef]
- Laguarta, J.; Hueto, F.; Subirana, B. COVID-19 Artificial Intelligence Diagnosis using only Cough Recordings. IEEE Open J. Eng. Med. Biol. 2020, 1, 275–281. [Google Scholar] [CrossRef]
- Magesh, S.; Niveditha, V.; Rajakumar, P.; Natrayan, L. Pervasive computing in the context of COVID-19 prediction with AI-based algorithms. Int. J. Pervasive Comput. Commun. 2020, 16, 477–487. [Google Scholar]
- Al-Shalabi, M. COVID-19 Symptoms Monitoring Mechanism using Internet of Things and Wireless Sensor Networks. IJCSNS 2020, 20, 16. [Google Scholar]
- Petrović, N.; Kocić, Đ. IoT-based System for COVID-19 Indoor Safety Monitoring. IcETRAN Belgrade 2020. preprint. [Google Scholar]
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Pub. Health 2020, 20, 1193. [Google Scholar] [CrossRef]
- Ontario Ministry of Health, Canada. COVID-19 Patient Screening Guidance Document. Available online: https://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/2019_patient_screening_guidance.pdf (accessed on 3 April 2021).
- Ubidots. Ubidots Homepage. 2021. Available online: https://ubidots.com/ (accessed on 3 April 2021).
- Arduino. Arduino Homepage. 2021. Available online: https://arduino.cc/ (accessed on 3 April 2021).
- Schwartz, M. Internet of Things with ESP8266; Packt Publishing Ltd.: Birmingham, UK, 2016; ISBN 1786466678. [Google Scholar]
- Xuedan, P.; Kai, Z.; Lili, W.; Yujie, F.; Shufen, C. Research on Blood Oxygen Saturation Measurement System Based on Reflective Signal. In Proceedings of the 2019 IEEE International Conference on Consumer Electronics—Taiwan (ICCE-TW), Yilan, Taiwan, 20–22 May 2019; pp. 1–2. [Google Scholar] [CrossRef]
- Jubran, A. Pulse Oximetry: Review. Crit. Care 2015, 272. [Google Scholar] [CrossRef] [Green Version]
- Yamanoor, N.S.; Yamanoor, S. Low-Cost Contact Thermometry for Screening and Monitoring during the COVID-19 Pandemic. In Proceedings of the 2020 IEEE International IOT, Electronics and Mechatronics Conference (IEMTRONICS), Vancouver, BC, Canada, 9–12 September 2020; pp. 1–6. [Google Scholar] [CrossRef]
- Enciso, L.; Vargas, A. Interface with Ubidots for a fire alarm system using WiFi. In Proceedings of the 2018 13th Iberian Conference on Information Systems and Technologies (CISTI), Caceres, Spain, 13–16 June 2018; pp. 1–6. [Google Scholar] [CrossRef]
- Garcia, J. Security: Is Ubidots Secure? 2020. Available online: https://help.ubidots.com/en/articles/889691-security-is-ubidots-secure (accessed on 24 February 2021).
- Ghubaish, A.; Salman, T.; Zolanvari, M.; Unal, D.; Al-Ali, A.K.; Jain, R. Recent Advances in the Internet of Medical Things (IoMT) Systems Security. IEEE Internet Things J. 2020. [Google Scholar] [CrossRef]
- Grillet, F.; Behr, J.; Calame, P.; Aubry, S.; Delabrousse, E. Acute pulmonary embolism associated with COVID-19 pneumonia detected with pulmonary CT angiography. Radiology 2020, 296, E186–E188. [Google Scholar] [CrossRef] [Green Version]
- Maâlej, A.J.; Krichen, M. A Model Based Approach to Combine Load and Functional Tests for Service Oriented Architectures. In Proceedings of the 10th International Workshop on Verification and Evaluation of Computer and Communication Systems VECoS, Sfax, Tunisia, 6–7 October 2016; pp. 123–140. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Purpose | Sensor | Technology | Composition | Performance/Calibration |
|---|---|---|---|---|
| Measuring human body temperature | MAX30205 | Converts the temperature measurements to digital form using a high-resolution, sigma-delta, analog-to-digital converter (ADC) | USB-to- controller along with display units | Meets clinical thermometry specification of the ASTM E1112 (0.1 C) |
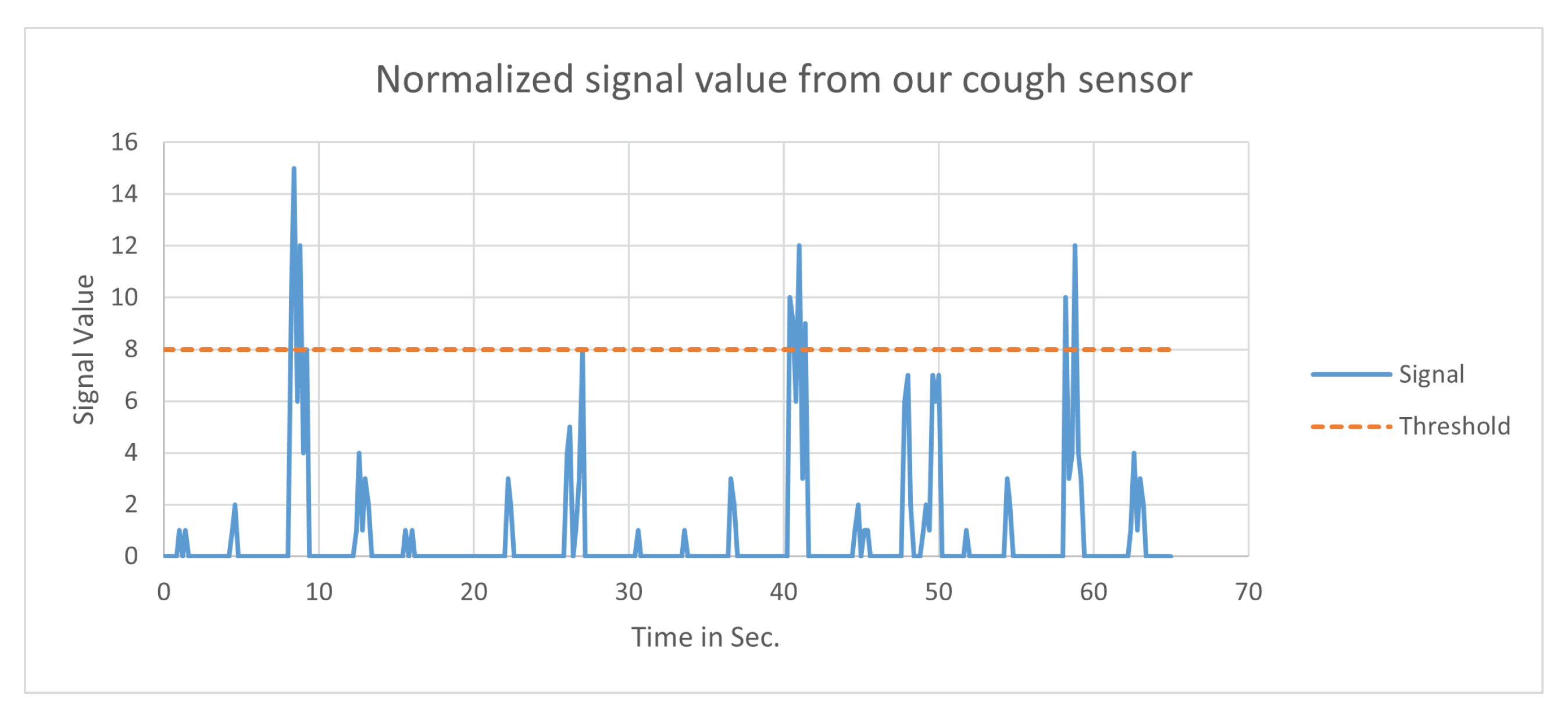
| Cough detection and variation | SW-420 | Doppler radar, continuous-wave (CW) radar, vibration detection | Breakout board that includes comparator LM393 | Adjustable on-board potentiometer for sensitivity threshold selection |
| Pulse/heart-rate | MAX30100 | Uses red and infrared frequency of light to determine the percentage of hemoglobin in the blood | Two LEDs, a photo detector, enhanced optics, and low-noise analog signal processing | Programmable from 200 s to 1.6 ms to optimize measurement accuracy |
| Wi-Fi connectivity | ESP8266 | Integrated TR switch, PLL, regulators, 32-bit CPU | Full TCP/IP stack and microcontroller capability | Wake up and transmit packets in <2 ms |
| Software Application | Objective | Usage | Characteristics |
|---|---|---|---|
| Google Firebase | Application creation | For creating client-server architecture | Cross-platform rapid development |
| Ubidots | IoT data analytics and visualization | To analyse and visualize data from mobile and other computing devices with support for device, app, and resource organization in IoT and cloud infrastructure | Encryption, secure authorization, privacy-aware protocols |
| Arduino IDE | Sensors connectivity | For programming and customizing the sensors used in the project | Open-source, easy-to-use hardware and software |
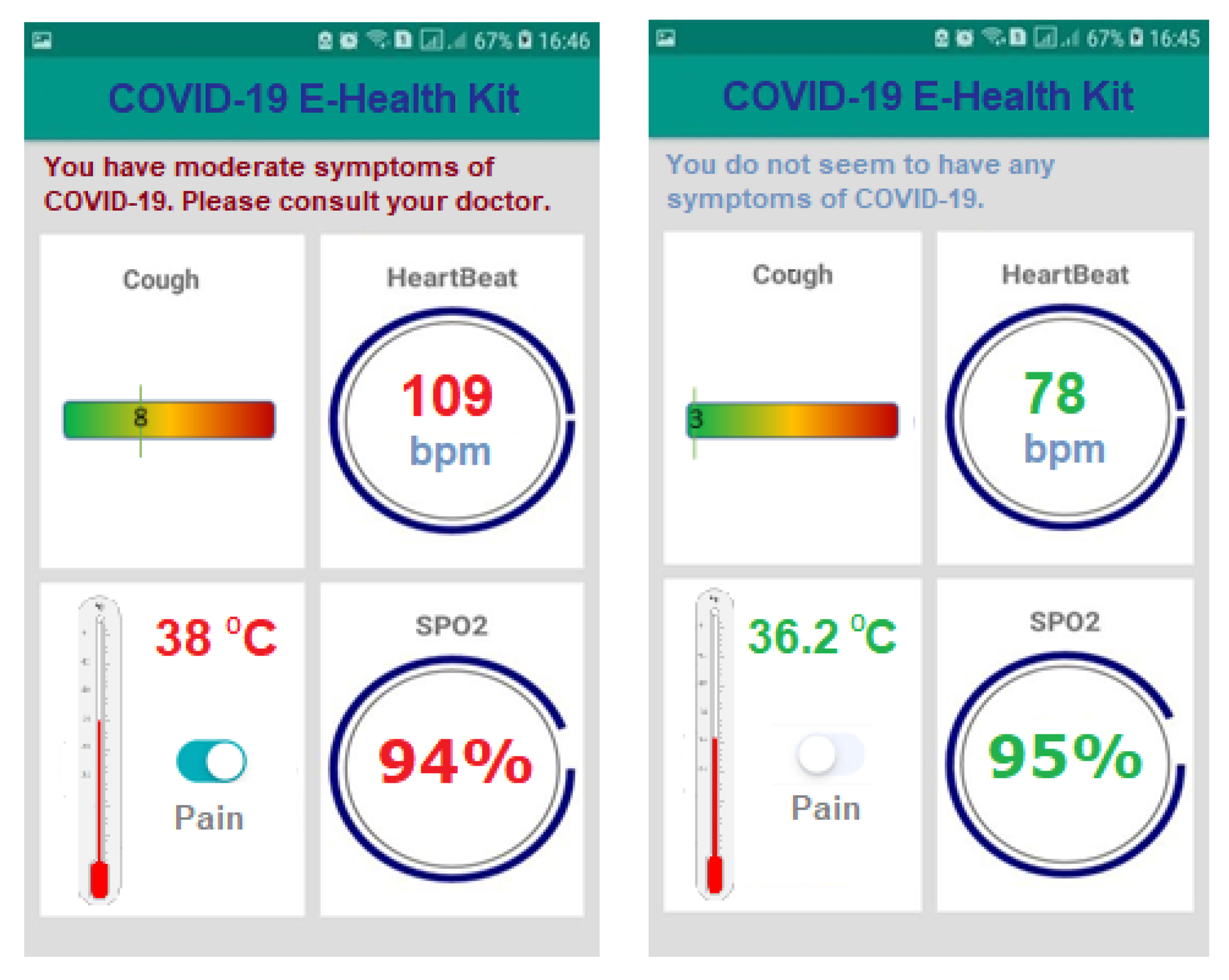
| Android Studio | Android app development | For developing Android-based application interface (Figure 4) and connectivity with the server | Unified environment, structured code modules |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mukhtar, H.; Rubaiee, S.; Krichen, M.; Alroobaea, R. An IoT Framework for Screening of COVID-19 Using Real-Time Data from Wearable Sensors. Int. J. Environ. Res. Public Health 2021, 18, 4022. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084022
Mukhtar H, Rubaiee S, Krichen M, Alroobaea R. An IoT Framework for Screening of COVID-19 Using Real-Time Data from Wearable Sensors. International Journal of Environmental Research and Public Health. 2021; 18(8):4022. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084022
Chicago/Turabian StyleMukhtar, Hamid, Saeed Rubaiee, Moez Krichen, and Roobaea Alroobaea. 2021. "An IoT Framework for Screening of COVID-19 Using Real-Time Data from Wearable Sensors" International Journal of Environmental Research and Public Health 18, no. 8: 4022. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084022