
The Impact of the COVID-19 Pandemic on the Cognition of People with Dementia



Abstract
:1. Introduction
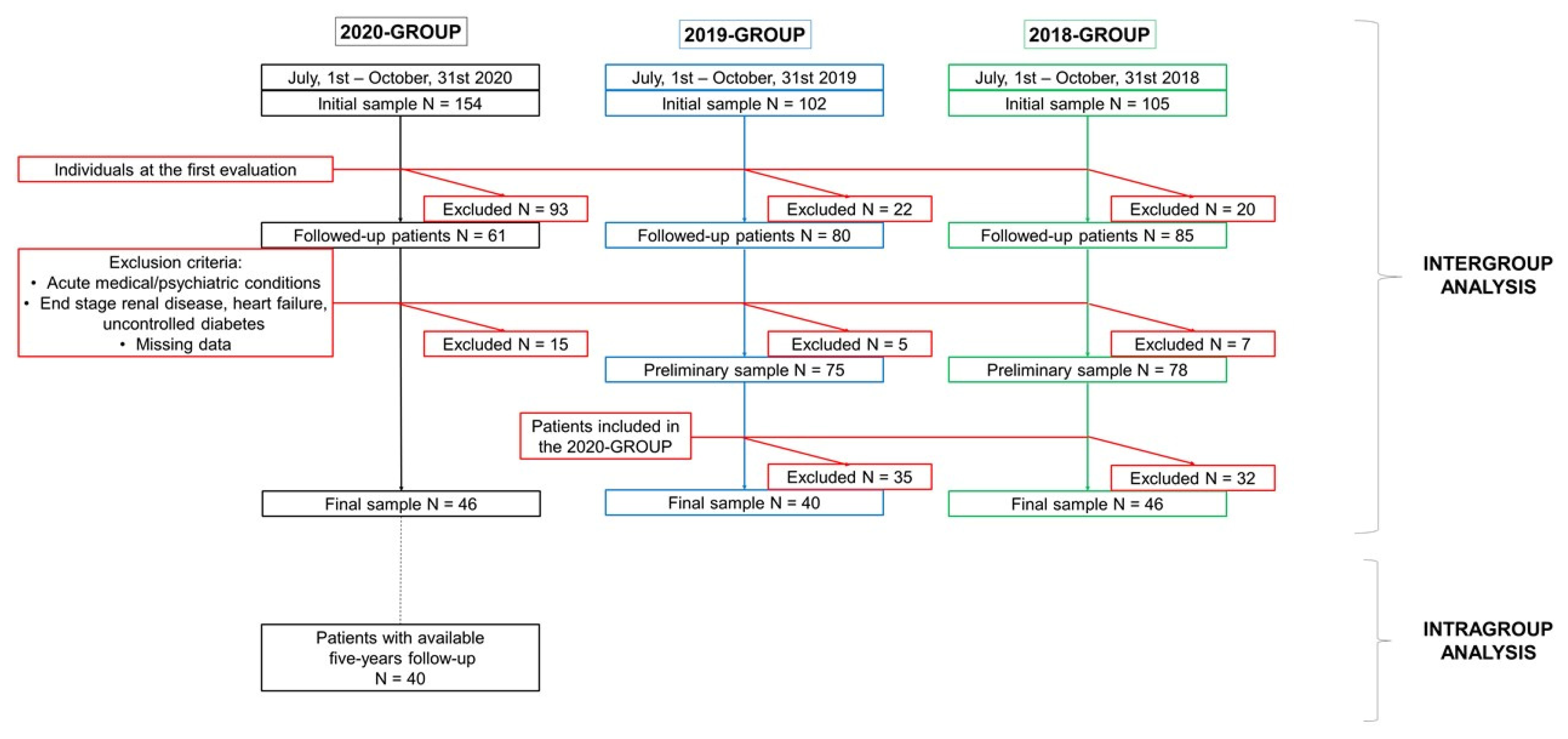
2. Materials and Methods
2.1. Subjects
2.2. Data Collection
2.3. Statistical Analysis
3. Results
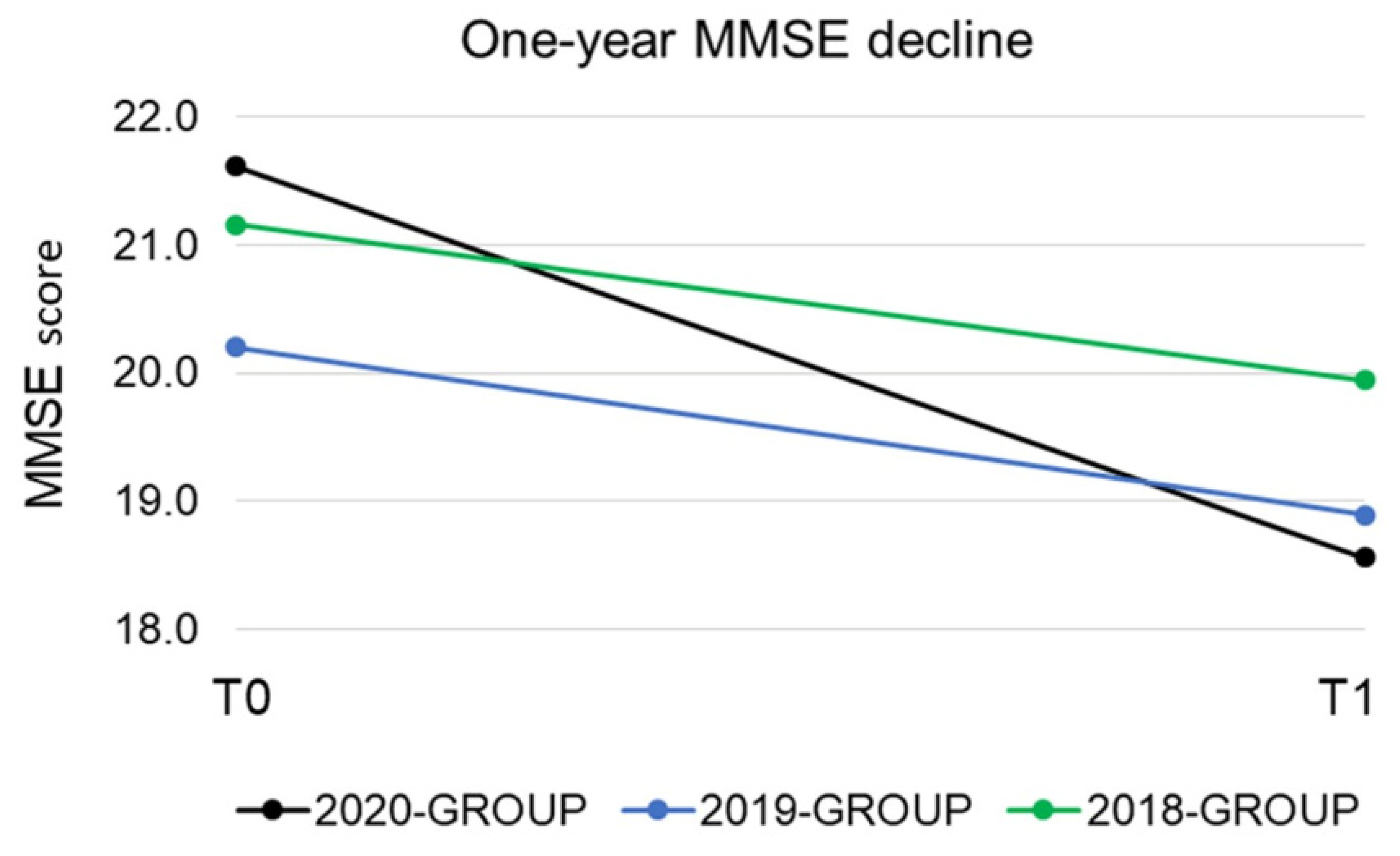
3.1. Intergroup Analysis
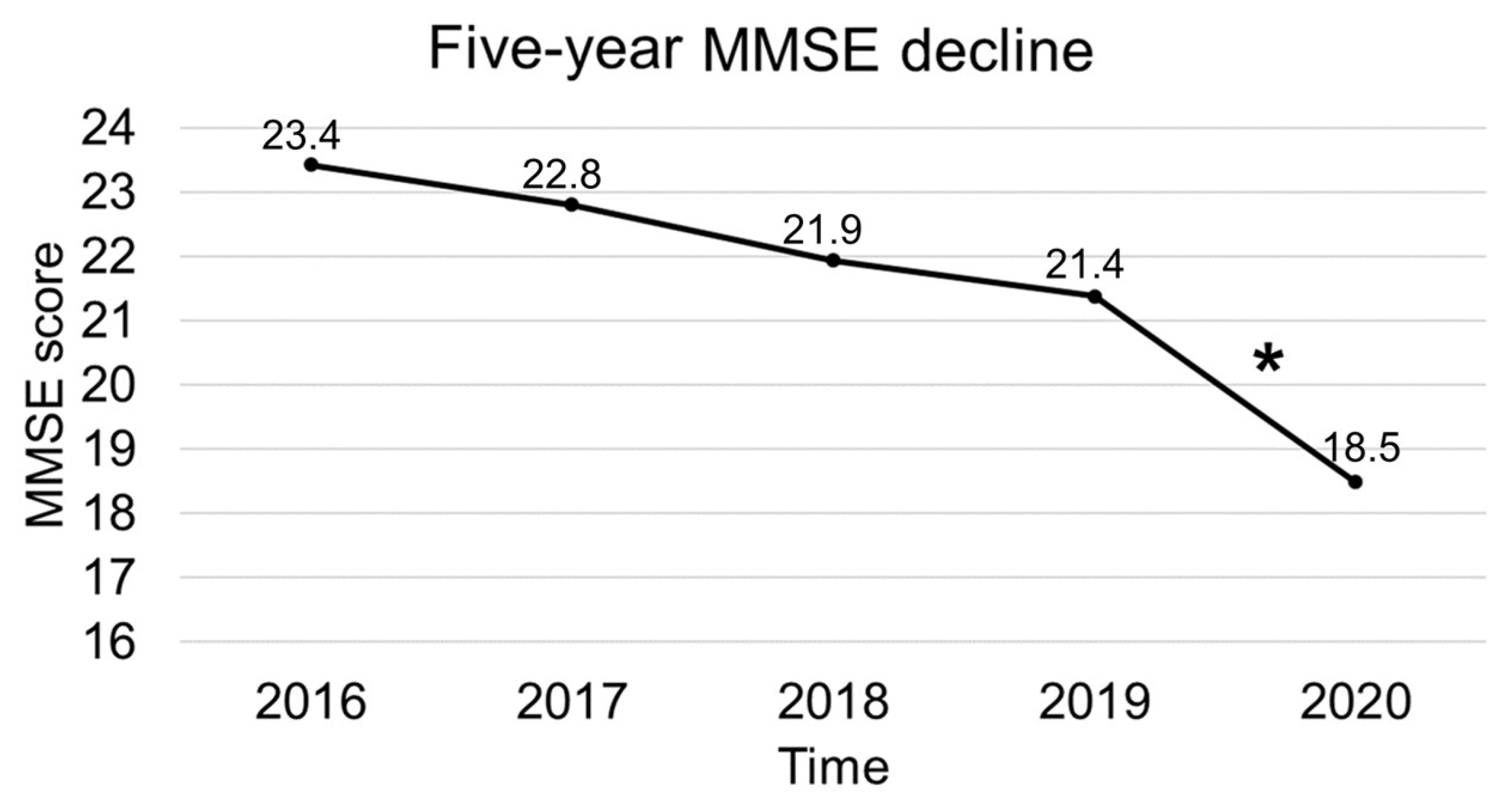
3.2. Intragroup Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Italian Ministry of Health. COVID-19 Italy, Daily Situation Report. Italian Ministry of Health, 2020. Available online: http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?lingua=italiano&id=5351&area=nuovoCoronavirus&menu=vuoto (accessed on 15 February 2021).
- Gallo, O.; Locatello, L.G.; Orlando, P.; Martelli, F.; Bruno, C.; Cilona, M.; Fancello, G.; Mani, R.; Vitali, D.; Bianco, G. The clinical consequences of the COVID-19 lockdown: A report from an Italian referral ENT department. Laryngoscope Investig. Otolaryngol. 2020, 5, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Torzilli, G.; Vigano, L.; Galvanin, J.; Castoro, C.; Quagliuolo, V.; Spinelli, A.; Zerbi, A.; Donadon, M.; Montorsi, M. A snapshot of elective oncological surgery in Italy during COVID-19 emergency: Pearls, pitfalls, and perspectives. Ann. Surg. 2020, 272, e112. [Google Scholar] [CrossRef] [PubMed]
- Randelli, P.S.; Compagnoni, R. Management of Orthopaedic and Traumatology Patients during the Coronavirus Disease (COVID-19) Pandemic in Northern Italy. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 1683–1689. [Google Scholar]
- Bonanad, C.; García-Blas, S.; Tarazona-Santabalbina, F.J.; Díez-Villanueva, P.; Ayesta, A.; Forés, J.S.; Vidán-Austiz, M.T.; Formiga, F.; Ariza-Solé, A.; Martínez-Sellés, M. Coronavirus: The geriatric emergency of 2020. Joint document of the Section on Geriatric Cardiology of the Spanish Society of Cardiology and the Spanish Society of Geriatrics and Gerontology. Rev. Española Cardiol. (Engl. Ed.) 2020, 73, 569–576. [Google Scholar] [CrossRef]
- Numbers, K.; Brodaty, H. The effects of the COVID-19 pandemic on people with dementia. Nat. Rev. Neurol. 2021, 17, 69–70. [Google Scholar] [CrossRef] [PubMed]
- Canevelli, M.; Palmieri, L.; Raparelli, V.; Lo Noce, C.; Colaizzo, E.; Tiple, D.; Vaianella, L.; Vanacore, N.; Brusaferro, S.; Onder, G. Prevalence and clinical correlates of dementia among COVID-19-related deaths in Italy. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2020, 12, e12114. [Google Scholar] [CrossRef] [PubMed]
- Bianchetti, A.; Rozzini, R.; Guerini, F.; Boffelli, S.; Ranieri, P.; Minelli, G.; Bianchetti, L.; Trabucchi, M. Clinical presentation of COVID19 in dementia patients. J. Nutr. Health Aging 2020, 24, 560–562. [Google Scholar] [CrossRef]
- Covino, M.; De Matteis, G.; Santoro, M.; Sabia, L.; Simeoni, B.; Candelli, M.; Ojetti, V.; Franceschi, F. Clinical characteristics and prognostic factors in COVID-19 patients aged≥ 80 years. Geriatr. Gerontol. Int. 2020, 20, 704–708. [Google Scholar] [CrossRef]
- Prete, G.; Fontanesi, L.; Porcelli, P.; Tommasi, L. The psychological impact of COVID-19 in Italy: Worry leads to protective behavior, but at the cost of anxiety. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 pandemic and lockdown measures impact on mental health among the general population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef]
- Fiorillo, A.; Sampogna, G.; Giallonardo, V.; Del Vecchio, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B. Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: Results from the COMET collaborative network. Eur. Psychiatry 2020, 63. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, D.; Fontanesi, L.; Mazza, C.; Di Giandomenico, S.; Roma, P.; Verrocchio, M.C. Parenting-related exhaustion during the italian COVID-19 lockdown. J. Pediatr. Psychol. 2020, 45, 1114–1123. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental health outcomes among frontline and second-line health care workers during the coronavirus disease 2019 (COVID-19) pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef] [PubMed]
- Naldi, A.; Vallelonga, F.; Di Liberto, A.; Cavallo, R.; Agnesone, M.; Gonella, M.; Sauta, M.D.; Lochner, P.; Tondo, G.; Bragazzi, N.L. COVID-19 pandemic-related anxiety, distress and burnout: Prevalence and associated factors in healthcare workers of North-West Italy. BJPsych Open 2021, 7. [Google Scholar] [CrossRef] [PubMed]
- Marelli, S.; Castelnuovo, A.; Somma, A.; Castronovo, V.; Mombelli, S.; Bottoni, D.; Leitner, C.; Fossati, A.; Ferini-Strambi, L. Impact of COVID-19 lockdown on sleep quality in university students and administration staff. J. Neurol. 2021, 268, 8–15. [Google Scholar] [CrossRef]
- Altieri, M.; Santangelo, G. The psychological impact of COVID-19 pandemic and lockdown on caregivers of people with dementia. Am. J. Geriatr. Psychiatry 2021, 29, 27–34. [Google Scholar] [CrossRef]
- Cagnin, A.; Di Lorenzo, R.; Marra, C.; Bonanni, L.; Cupidi, C.; Laganà, V.; Rubino, E.; Vacca, A.; Provero, P.; Isella, V. Behavioral and psychological effects of coronavirus disease-19 quarantine in patients with dementia. Front. Psychiatry 2020, 11, 916. [Google Scholar] [CrossRef]
- Manca, R.; De Marco, M.; Venneri, A. The impact of COVID-19 infection and enforced prolonged social isolation on neuropsychiatric symptoms in older adults with and without dementia: A review. Front. Psychiatry 2020, 11, 1086. [Google Scholar] [CrossRef]
- di Giacomo, E.; Bellelli, G.; Peschi, G.; Scarpetta, S.; Colmegna, F.; de Girolamo, G.; Clerici, M. Management of older people during the COVID-19 outbreak: Recommendations from an Italian experience. Int. J. Geriatr. Psychiatry 2020, 35, 803–805. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKeith, I.G.; Boeve, B.F.; DIckson, D.W.; Halliday, G.; Taylor, J.P.; Weintraub, D.; Aarsland, D.; Galvin, J.; Attems, J.; Ballard, C.G.; et al. Diagnosis and management of dementia with Lewy bodies. Neurology 2017, 89, 88–100. [Google Scholar] [CrossRef] [Green Version]
- Rascovsky, K.; Hodges, J.R.; Knopman, D.; Mendez, M.F.; Kramer, J.H.; Neuhaus, J.; Van Swieten, J.C.; Seelaar, H.; Dopper, E.G.P.; Onyike, C.U.; et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain 2011, 134, 2456–2477. [Google Scholar] [CrossRef]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Román, G.C.; Tatemichi, T.K.; Erkinjuntti, T.; Cummings, J.L.; Masdeu, J.C.; Garcia, J.H.; Amaducci, L.; Orgogozo, J.-M.; Brun, A.; Hofman, A. Vascular dementia: Diagnostic criteria for research studies: Report of the NINDS-AIREN International Workshop. Neurology 1993, 43, 250. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Caroli, A.; Prestia, A.; Galluzzi, S.; Ferrari, C.; Van Der Flier, W.M.; Ossenkoppele, R.; Van Berckel, B.; Barkhof, F.; Teunissen, C.; Wall, A.E. Mild cognitive impairment with suspected nonamyloid pathology (SNAP): Prediction of progression. Neurology 2015, 84, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Varatharaj, A.; Thomas, N.; Ellul, M.A.; Davies, N.W.S.; Pollak, T.A.; Tenorio, E.L.; Sultan, M.; Easton, A.; Breen, G.; Zandi, M. Neurological and neuropsychiatric complications of COVID-19 in 153 patients: A UK-wide surveillance study. Lancet Psychiatry 2020, 7, 875–882. [Google Scholar] [CrossRef]
- Arnold, C. Could COVID delirium bring on dementia? Nature 2020, 588, 22–24. [Google Scholar] [CrossRef]
- Marshall, M. How COVID-19 can damage the brain. Nature 2020, 585, 342–343. [Google Scholar] [CrossRef] [PubMed]
- Wijeratne, T.; Crewther, S. COVID-19 and long-term neurological problems: Challenges ahead with Post-COVID-19 Neurological Syndrome. Aust. J. Gen. Pract. 2021, 50. [Google Scholar] [CrossRef]
- Thyrian, J.R.; Kracht, F.; Nikelski, A.; Boekholt, M.; Schumacher-Schönert, F.; Rädke, A.; Michalowsky, B.; Vollmar, H.C.; Hoffmann, W.; Rodriguez, F.S. The situation of elderly with cognitive impairment living at home during lockdown in the Corona-pandemic in Germany. BMC Geriatr. 2020, 20, 1–15. [Google Scholar] [CrossRef]
- Roach, P.; Zwiers, A.; Cox, E.; Fischer, K.; Charlton, A.; Josephson, C.B.; Patten, S.B.; Seitz, D.; Ismail, Z.; Smith, E.E. Understanding the impact of the COVID-19 pandemic on well-being and virtual care for people living with dementia and care partners living in the community. Dementia 2020. [Google Scholar] [CrossRef]
- Borges-Machado, F.; Barros, D.; Ribeiro, Ó.; Carvalho, J. The Effects of COVID-19 Home Confinement in Dementia Care: Physical and Cognitive Decline, Severe Neuropsychiatric Symptoms and Increased Caregiving Burden. Am. J. Alzheimer’s Dis. Other Dementias® 2020, 35. [Google Scholar] [CrossRef]
- Tsapanou, A.; Papatriantafyllou, J.D.; Yiannopoulou, K.; Sali, D.; Kalligerou, F.; Ntanasi, E.; Zoi, P.; Margioti, E.; Kamtsadeli, V.; Hatzopoulou, M. The impact of COVID-19 pandemic on people with mild cognitive impairment/dementia and on their caregivers. Int. J. Geriatr. Psychiatry 2020. [Google Scholar] [CrossRef]
- Van Maurik, I.S.; Bakker, E.D.; van den Buuse, S.; Gillissen, F.; Van De Beek, M.; Lemstra, E.; Mank, A.; Van Den Bosch, K.A.; Van Leeuwenstijn, M.; Bouwman, F.H. Psychosocial effects of corona measures on patients with dementia, mild cognitive impairment and subjective cognitive decline. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Mazzi, M.C.; Iavarone, A.; Musella, C.; De Luca, M.; de Vita, D.; Branciforte, S.; Coppola, A.; Scarpa, R.; Raimondo, S.; Sorrentino, S. Time of isolation, education and gender influence the psychological outcome during COVID-19 lockdown in caregivers of patients with dementia. Eur. Geriatr. Med. 2020, 11, 1095–1098. [Google Scholar] [CrossRef] [PubMed]
- Barguilla, A.; Fernández-Lebrero, A.; Estragués-Gázquez, I.; García-Escobar, G.; Navalpotro-Gómez, I.; Manero, R.M.; Puente-Periz, V.; Roquer, J.; Puig-Pijoan, A. Effects of COVID-19 Pandemic Confinement in Patients With Cognitive Impairment. Front. Neurol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Fong, T.G.; Jones, R.N.; Shi, P.; Marcantonio, E.R.; Yap, L.; Rudolph, J.L.; Yang, F.M.; Kiely, D.K.; Inouye, S.K. Delirium accelerates cognitive decline in Alzheimer disease. Neurology 2009, 72, 1570–1575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, D.H.J.; Muniz Terrera, G.; Keage, H.; Rahkonen, T.; Oinas, M.; Matthews, F.E.; Cunningham, C.; Polvikoski, T.; Sulkava, R.; MacLullich, A.M.J. Delirium is a strong risk factor for dementia in the oldest-old: A population-based cohort study. Brain 2012, 135, 2809–2816. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; Speechley, M. Falls in cognitively impaired older adults: Implications for risk assessment and prevention. J. Am. Geriatr. Soc. 2018, 66, 367–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lombardo, F.L.; Salvi, E.; Lacorte, E.; Piscopo, P.; Mayer, F.; Ancidoni, A.; Remoli, G.; Bellomo, G.; Losito, G.; D’Ancona, F. Adverse events in Italian nursing homes during the COVID-19 epidemic: A national survey. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef]
- Howard, R.; Burns, A.; Schneider, L. Antipsychotic prescribing to people with dementia during COVID-19. Lancet Neurol. 2020, 19, 892. [Google Scholar] [CrossRef]
- Baker, E.; Iqbal, E.; Johnston, C.; Broadbent, M.; Shetty, H.; Stewart, R.; Howard, R.; Newhouse, S.; Khondoker, M.; Dobson, R.J.B. Trajectories of dementia-related cognitive decline in a large mental health records derived patient cohort. PLoS ONE 2017, 12, e0178562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkosz, P.A.; Seltman, H.J.; Devlin, B.; Weamer, E.A.; Lopez, O.L.; DeKosky, S.T.; Sweet, R.A. Trajectories of cognitive decline in Alzheimer’s disease. Int. Psychogeriatr. IPA 2010, 22, 281. [Google Scholar] [CrossRef] [Green Version]
- Pilon, M.-H.; Poulin, S.; Fortin, M.-P.; Houde, M.; Verret, L.; Bouchard, R.W.; Laforce, R. Differences in rate of cognitive decline and caregiver burden between Alzheimer’s disease and vascular dementia: A retrospective study. Neurology 2016, 2, 278. [Google Scholar]
- Giil, L.M.; Aarsland, D. Greater Variability in Cognitive Decline in Lewy Body Dementia Compared to Alzheimer’s Disease. J. Alzheimer’s Dis. 2020, 73, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Binetti, G.; Locascio, J.J.; Corkin, S.; Vonsattel, J.P.; Growdon, J.H. Differences between Pick disease and Alzheimer disease in clinical appearance and rate of cognitive decline. Arch. Neurol. 2000, 57, 225–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Small, B.J.; Viitanen, M.; Backman, L. Mini-Mental State Examination item scores as predictors of Alzheimer’s disease: Incidence data from the Kungsholmen Project, Stockholm. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1997, 52, M299–M304. [Google Scholar] [CrossRef] [Green Version]
- Wilson, R.S.; Leurgans, S.E.; Boyle, P.A.; Bennett, D.A. Cognitive decline in prodromal Alzheimer disease and mild cognitive impairment. Arch. Neurol. 2011, 68, 351–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paterniti, S.; Verdier-Taillefer, M.-H.; Dufouil, C.; Alpérovitch, A. Depressive symptoms and cognitive decline in elderly people: Longitudinal study. Br. J. Psychiatry 2002, 181, 406–410. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, F.C.; Ashley, A.V.; Endeshaw, Y.; Hanfelt, J.; Lah, J.J.; Levey, A.I. Effects of hypertension and hypercholesterolemia on cognitive functioning in patients with Alzheimer’s disease. Alzheimer Dis. Assoc. Disord. 2008, 22, 336. [Google Scholar] [CrossRef] [PubMed]
- Singh-Manoux, A.; Sabia, S.; Lajnef, M.; Ferrie, J.E.; Nabi, H.; Britton, A.R.; Marmot, M.G.; Shipley, M.J. History of coronary heart disease and cognitive performance in midlife: The Whitehall II study. Eur. Heart J. 2008, 29, 2100–2107. [Google Scholar] [CrossRef] [PubMed]
- Marzona, I.; O’Donnell, M.; Teo, K.; Gao, P.; Anderson, C.; Bosch, J.; Yusuf, S. Increased risk of cognitive and functional decline in patients with atrial fibrillation: Results of the ONTARGET and TRANSCEND studies. Cmaj 2012, 184, E329–E336. [Google Scholar] [CrossRef] [Green Version]
- Hogervorst, E.; Huppert, F.; Matthews, F.E.; Brayne, C. Thyroid function and cognitive decline in the MRC Cognitive Function and Ageing Study. Psychoneuroendocrinology 2008, 33, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Roselli, F.; Tartaglione, B.; Federico, F.; Lepore, V.; Defazio, G.; Livrea, P. Rate of MMSE score change in Alzheimer’s disease: Influence of education and vascular risk factors. Clin. Neurol. Neurosurg. 2009, 111, 327–330. [Google Scholar] [CrossRef] [PubMed]
- Tondo, G.; De Marchi, F.; Terazzi, E.; Prandi, P.; Sacchetti, M.; Comi, C.; Cantello, R. Chronic obstructive pulmonary disease may complicate Alzheimer’s disease: A comorbidity problem. Neurol. Sci. 2018, 39, 1585–1589. [Google Scholar] [CrossRef]
- De Girolamo, G.; Bellelli, G.; Bianchetti, A.; Starace, F.; Zanetti, O.; Zarbo, C.; Micciolo, R. Older People Living in Long-Term Care Facilities and Mortality Rates During the COVID-19 Pandemic in Italy: Preliminary Epidemiological Data and Lessons to Learn. Front. Psychiatry 2020, 11, 1032. [Google Scholar] [CrossRef]
- Reyes-Bueno, J.A.; Mena-Vázquez, N.; Ojea-Ortega, T.; Gonzalez-Sotomayor, M.M.; Cabezudo-Garcia, P.; Ciano-Petersen, N.L.; Pons-Pons, G.; Castro-Sánchez, M.V.; Serrano-Castro, P.J. Case fatality of COVID-19 in patients with neurodegenerative dementia. Neurol. (Engl. Ed.) 2020, 35, 639–645. [Google Scholar] [CrossRef]
- Palsetia, D.; Rao, G.P.; Tiwari, S.C.; Lodha, P.; De Sousa, A. The clock drawing test versus mini-mental status examination as a screening tool for dementia: A clinical comparison. Indian J. Psychol. Med. 2018, 40, 1–10. [Google Scholar] [CrossRef]
- Evans, I.E.M.; Martyr, A.; Collins, R.; Brayne, C.; Clare, L. Social isolation and cognitive function in later life: A systematic review and meta-analysis. J. Alzheimer’s Dis. 2019, 70, S119–S144. [Google Scholar] [CrossRef] [Green Version]
- Enache, D.; Winblad, B.; Aarsland, D. Depression in dementia: Epidemiology, mechanisms, and treatment. Curr. Opin. Psychiatry 2011, 24, 461–472. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2020-GROUP N = 46 | 2019-GROUP N = 40 | 2018-GROUP N = 46 | p Value | |
|---|---|---|---|---|
| Age | 78.78 ± 8.82 | 79.58 ± 6.20 | 79.30 ± 6.21 | 0.919 |
| Sex (f/m) | 32/14 | 25/15 | 28/18 | 0.654 |
| Education in years | 6.96 ± 3.63 | 6.25 ± 2.69 | 6.43 ± 3.59 | 0.671 |
| Follow-up in years | 0.93 ± 0.15 | 0.95 ± 0.16 | 0.94 ± 0.15 | 0.912 |
| Disease duration in years | 4.33 ± 2.24 | 4.10 ± 1.98 | 3.96 ± 1.80 | 0.838 |
| MMSE T0 | 21.61 ± 4.75 | 20.20 ± 4.68 | 21.15 ± 3.36 | 0.370 |
| MMSE T1 | 18.56 ± 5.03 | 18.89 ± 5.24 | 19.94 ± 3.37 | 0.380 |
| Index of progression | −3.25 | −1.39 | −1.33 | 0.021 |
| Diagnosis N (%) | 0.836 | |||
| AD | 21 (46%) | 21 (53%) | 26 (57%) | |
| DLB | 1 (2%) | 2 (5%) | 1 (2%) | |
| FTD | 5 (11%) | 2 (5%) | 2 (4%) | |
| MCI | 10 (22%) | 7 (18%) | 6 (13%) | |
| VAD | 9 (20%) | 8 (20%) | 11 (24%) | |
| Therapy N (%) | 0.945 | |||
| None | 13 (28%) | 14 (35%) | 16 (35%) | |
| Donepezil | 14 (30%) | 8 (20%) | 11 (24%) | |
| Rivastigmine | 7 (15%) | 7 (18%) | 6 (13%) | |
| Donepezil + Memantine | 4 (9%) | 5 (13%) | 6 (13%) | |
| Other | 8 (17%) | 6 (15%) | 7 (15%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tondo, G.; Sarasso, B.; Serra, P.; Tesser, F.; Comi, C. The Impact of the COVID-19 Pandemic on the Cognition of People with Dementia. Int. J. Environ. Res. Public Health 2021, 18, 4285. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084285
Tondo G, Sarasso B, Serra P, Tesser F, Comi C. The Impact of the COVID-19 Pandemic on the Cognition of People with Dementia. International Journal of Environmental Research and Public Health. 2021; 18(8):4285. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084285
Chicago/Turabian StyleTondo, Giacomo, Barbara Sarasso, Paola Serra, Fabiana Tesser, and Cristoforo Comi. 2021. "The Impact of the COVID-19 Pandemic on the Cognition of People with Dementia" International Journal of Environmental Research and Public Health 18, no. 8: 4285. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084285