
Comparison of the Effectiveness of an Abbreviated Program versus a Standard Program in Mindfulness, Self-Compassion and Self-Perceived Empathy in Tutors and Resident Intern Specialists of Family and Community Medicine and Nursing in Spain

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Study Participants and Recruitment
2.3. Sample Size
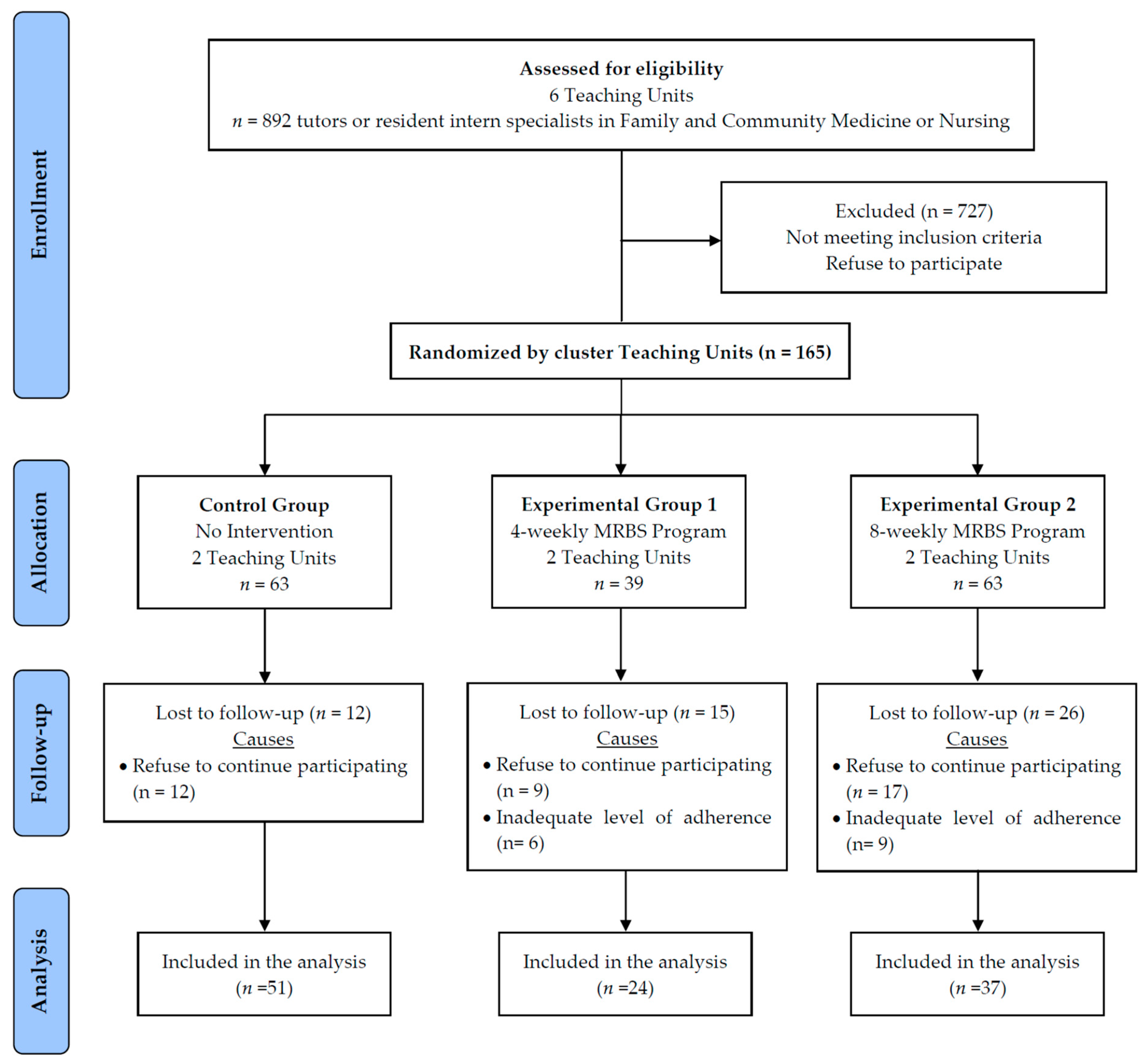
2.4. Procedure and Randomisation
2.5. Intervention
2.6. Main Outcomes
2.7. Data Collection Procedure, Data Management and Monitoring
2.8. Ethical Considerations
2.9. Statistical Analyses
3. Results
3.1. Baseline Characterists of the Study Participants
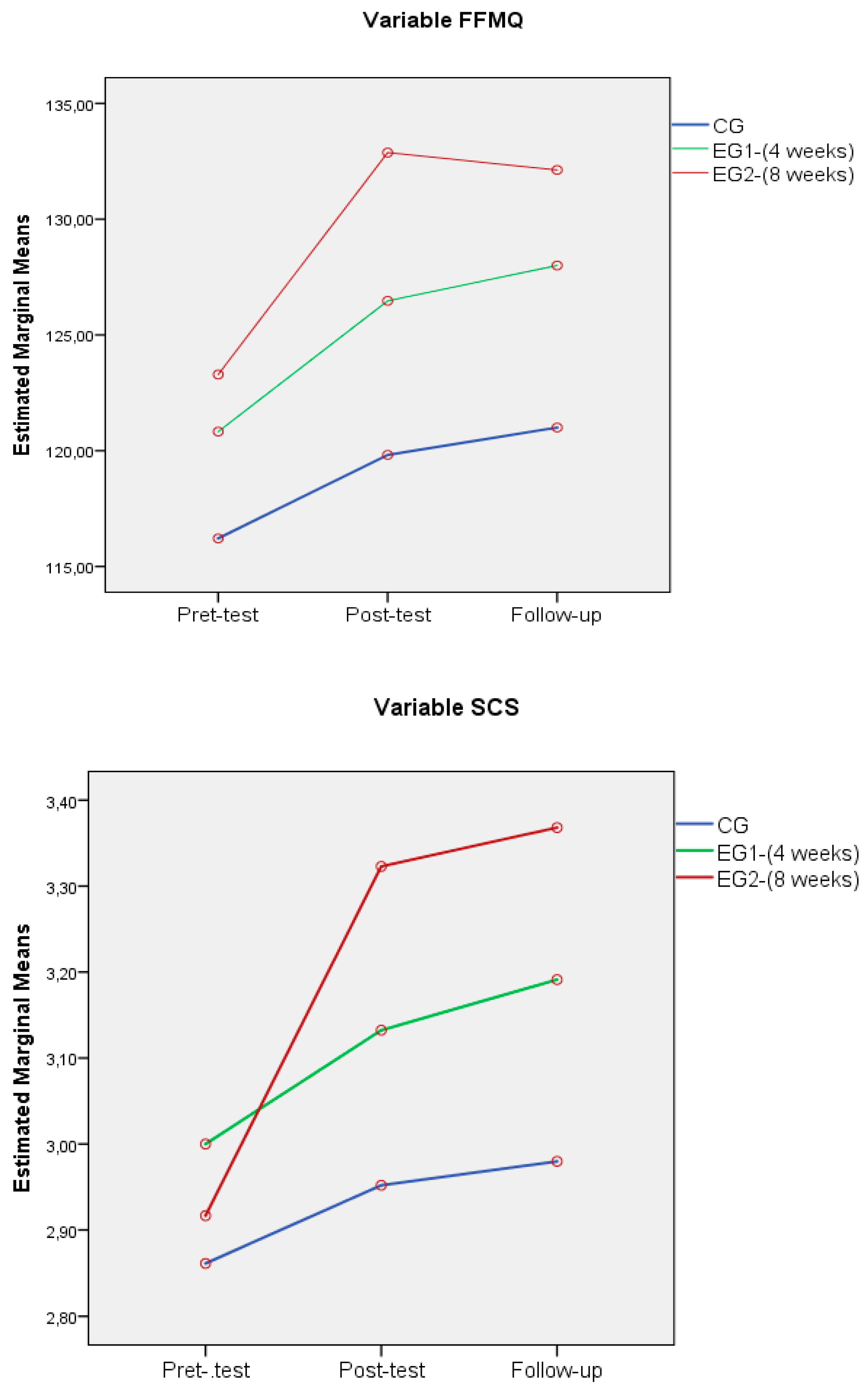
3.2. Mindfulness, Self-Compassion and Self-Perceived Empathy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Vilnius, M.; Cross, C.; Orfila, F.; Creixell, J.; Gonzalez, M.P.; Davins, J. Burnout and Teamwork at Primary Care Health Professionals. Aten. Primaria 2015, 47, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Spence Laschinger, H.K.; Finegan, J. Situational and Dispositional Predictors of Nurse Manager Burnout: A Time-Lagged Analysis. J. Nurs. Manag. 2008, 16, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Schinler, B.A.; Novack, D.H.; Cohen, D.G.; Yager, J.; Wang, D.; Saheen, N.J.; Guze, P.; Wilkerson, L.A.; Drossman, D.A. The Impact of the Changing Care Environment on the Health and Well-Being of Faculty at Four Medical Schools. Acad. Med. 2006, 81, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, V.J.; Cooper, C.L. Identifying Distress among General Practitioner: Predictors or Psycological Ill-Healt and Job Dissatisfaction. Soc. Sci. Med. 1993, 37, 575–581. [Google Scholar] [CrossRef]
- Benito, E.; Arranz, P.; Cancio, H. Tools for Self-Care of the Professional Caring for People Who Suffer. FMC 2011, 18, 59–65. [Google Scholar] [CrossRef]
- Van Mol, M.M.; Kompanje, E.J.; Benoit, D.D.; Bakker, J.; Nijkamp, M.D. The Prevalence of Compassion Fatigue and Burnout among Healthcare Professionals in Intensive Care Units: A Systematic Review. PLoS ONE 2015, 10, e0136955. [Google Scholar] [CrossRef] [PubMed]
- Chuang, C.H.; Tseng, P.C.; Lin, C.Y.; Lin, K.H.; Chen, Y.Y. Burnout in the Intensive Care Unit Professionals: A Systematic Review. Medicine 2016, 95, e5629. [Google Scholar] [CrossRef]
- Grossman, P.; Niemann, L.; Schmidt, S.; Walach, H. Mindfulness-Based Stress Reduction and Health Benefits. A Metaanalysis. J. Psychosom. Res. 2004, 57, 35–43. [Google Scholar] [CrossRef]
- Escuriex, B.F.; Labbe, E.E. Healthcare Providers’ Mindfulness and Treatment Outcomes: A Critical Review of the Research literature. Mindfulness 2011, 2, 242–253. [Google Scholar] [CrossRef]
- Awa, W.L.; Plaumann, M.; Walter, U. Burnout prevention: A review of intervention programs. Patient Educ. Couns. 2002, 78, 184–190. [Google Scholar] [CrossRef]
- Morgan, P.; Simpson, J.; Smith, A. Healthcare Workers’ Experiences of Mindfulness training: A Qualitative Review. Mindfulness 2014, 6, 744–758. [Google Scholar] [CrossRef]
- Smith, S.A. Mindfulness-Based Stress Reduction: An Intervention to Enhance Effectiveness of Nurses’ Coping with Work-Related Stress. Int. J. Nurs. Knowl. 2014, 25, 119–130. [Google Scholar] [CrossRef]
- Spinelli, C.; Wisener, M.; Khoury, B. Mindfulness Training for Healthcare Professionals and Trainees: A Meta-Analysis of Randomized Controlled Trials. J. Psychosom. Res. 2019, 120, 29–38. [Google Scholar] [CrossRef]
- Pérula Jiménez, C.; Pérula de Torres, C.; Pérula de Torres, L.A.; Jiménez García, C.; Vaquero Abellán, M. Mindfulness in Family and Community Nursing and its Relationship with Work Stress. Nure Inv. 2017, 14, 1–9. [Google Scholar]
- Brand, S.L.; Thompson Coon, J.; Fleming, L.E.; Carroll, L.; Bethel, A.; Wyatt, K. Whole-System Approaches to Improving the Health and Wellbeing of Healthcare Workers: A Systematic Review. PLoS ONE 2017, 12, e0188418. [Google Scholar] [CrossRef] [Green Version]
- Zafra-Ramirez, N.; Perez-Milena, A.; Valverde-Bolívar, F.J.; Rodriguez-Bayon, A.; Delgado-Rodríguez, M. Accomplishment of preventive activities proposed by resident doctors of Family Medicine in Primary Care and its relationship with communication skills. Aten. Primaria 2019, 51, 562–570. [Google Scholar] [CrossRef] [PubMed]
- García Campayo, J. The Practice of “Being Aware” (Mindfulness) in Medicine. Impact on Patients and Professionals. Aten Primaria 2008, 40, 363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.; Yin., J.; Wang, D.; Rahman, A.; Li, X. Urgent Need to Develop Evidence-Based Self-Help Interventions for Mental Health of Healthcare Workers in COVID-19 pandemic. Psychol. Med. 2020, 1–2. [Google Scholar] [CrossRef]
- Shaw, S.C. Hopelessness, Helplessness and Resilience: The Importance of Safeguarding Our Trainees’ Mental Wellbeing during the COVID-19 Pandemic. Nurse Educ. Pract. 2020, 44, 102780. [Google Scholar] [CrossRef]
- Behan, C. The Benefits of Meditation and Mindfulness Practices during Times of Crisis such as Covid-19. Irish J. Psychol. Med. 2020, 1–3. [Google Scholar] [CrossRef]
- Polizzi, C.; Lynn, S.J.; Perry, A. Stress and Coping in the Time of Covid-19: Pathways to Resilience and Recovery. Clin. Neuropsychiatry 2020, 17, 59–62. [Google Scholar] [CrossRef]
- Atanes, A.C.; Andreoni, S.; Hirayama, M.S.; Montero-Marin, J.; Barros, V.V.; Ronzani, T.M.; Kozasa, E.H.; Soler, J.; Cebolla, A.; Garcia-Campayo, J.; et al. Mindfulness, Perceived Stress, and Subjective Well-being: A Correlational Study in Primary Care Health Professionals. BMC Complement. Altern. Med. 2015, 15, 303. [Google Scholar] [CrossRef] [Green Version]
- Shanafelt, T.D.; Balch, C.M.; Bechamps, G.J.; Russell, T.; Dyrbye, L.; Satele, D.; Collicott, P.; Novotny, P.J.; Sloan, J.; Freischlag, J.A. Burnout and Career Satisfaction among American Surgeons. Ann. Surg. 2009, 250, 463–471. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. An Outpatient Program in Behavioral Medicine for Chronic Pain Patients based on the Practice of Mindfulness Meditation: Theoretical Considerations and Preliminary Results. Gen. Hosp. Psychiatry 1982, 4, 33–47. [Google Scholar] [CrossRef]
- Demarzo, M.M.; Montero Marin, J.; Cuijpers, P.; Zabaleta del Olmo, E.; Mahtani, K.R.; Vellinga, A.; Vicens, C.; López del Hoyo, Y.; García Campayo, J. The Efficacy of Mindfulness-Based Interventions in Primary Care: A Meta-Analytic Review. Ann. Fam. Med. 2015, 13, 573–582. [Google Scholar] [CrossRef]
- García Campayo, J.; Demarzo, M. What Do We Know about Mindfulness? 1st ed.; Kairos: Barcelona, Spain, 2018. [Google Scholar]
- Martín-Asuero, A.; García de la Banda, G. The Advantages of Being Present: Developing Full Awareness to Reduce Psychological Distress. Int. J. Clin. Health Psychol. 2007, 7, 369–384. [Google Scholar]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of your Body and Mind to Face Stress, Pain, and Illness, 1st ed.; Delacorte: New York, NY, USA, 1990. [Google Scholar]
- Kabat-Zinn, J.; Torrijos, F.; Skillings, A.H.; Blacker, M.; Mumford, G.T.; Levi-Alvares, D.; Santorelli, S.; Rosal, M.C. Delivery and Effectiveness of a Dual Language (English/Spanish). Mindfulness-based stress reduction (MBI). Program in the Inner City -A Seven-Year Experience: 1992–1999. Mindfulness 2016, 1, 213. [Google Scholar] [CrossRef]
- Lloyd, A.; White, R.; Eames, C.; Crane, R. The Utility of Home-Practice in Mindfulness-Based Group Interventions: A Systematic Review. Mindfulness 2018, 9, 673–692. [Google Scholar] [CrossRef] [Green Version]
- Fortney, L.; Luchterhand, C.; Zakletskaia, L.; Zgierska, A.; Rakel, D. Abbreviated Mindfulness Intervention for Job Satisfaction, Quality of Life, and Compassion in Primary Care Clinicians: A Pilot Study. Ann. Fam. Med. 2013, 11, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Braden, B.B.; Pipe, T.B.; Smith, R.; Glaspy, T.K.; Deatherage, B.R.; Baxter, L.C. Brain and Behavior Changes Associated with an Abbreviated 4-week Mindfulness Based Stress Reduction Course in Back Pain Patients. Brain Behav. 2016, 6, e00443. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, D.A.; Stephens, E.; Colgan, D.; Hunsinger, M.; Rubin, D.; Christopher, M.S. A Brief Mindfulness-Based Intervention for Primary Care Physicians: A Pilot Randomized Controlled Trial. Am. J. Lifestyle Med. 2016, 12, 83–91. [Google Scholar] [CrossRef] [Green Version]
- Brintz, C.E.; Roth, I.; Faurot, K.; Rao, S.; Gaylord, S.A. Feasibility and Acceptability of an Abbreviated, Four-Week Mindfulness Program for Chronic Pain Management. Pain Med. 2020, 21, 2799–2810. [Google Scholar] [CrossRef]
- Pipe, T.B.; Bortz, J.J.; Duek, A. Nurse Leader Mindfulness Meditation Program for Stress Management: A Randomized Controlled Trial. J. Nurs. Adm. 2009, 39, 130–137. [Google Scholar] [CrossRef]
- Manotas, M.; Segura, C.; Eraso, M.; Oggins, J.; McGovern, K. Association of Brief Mindfulness Training with Reductions in Perceived Stress and Distress in Colombian Healthcare Professionals. Int. J. Stress Manag. 2014, 21, 207–225. [Google Scholar] [CrossRef]
- Martin-Asuero, A.; Queralto, J.M.; Pujol-Ribera, E.; Berenguera, A.; Rodriguez-Blanco, T.; Epstein, R.M. Effectiveness of a Mindfulness Education Program in Primary Health Care Professionals: A Pragmatic Controlled Trial. J. Contin. Educ. Health Prof. 2014, 34, 4–12. [Google Scholar] [CrossRef]
- Simon, V. Mindfulness and Psychology; present and future. Psychol. Inform. 2010, 100, 162–170. [Google Scholar]
- Singer, T.; Klimecki, O.M. Empathy and Compassion. Curr. Biol. 2014, 24, R875–R878. [Google Scholar] [CrossRef] [Green Version]
- Ashar, Y.K.; Andrews-Hanna, J.R.; Dimidjian, S.; Wager, T.D. Empathic Care and Distress: Predictive Brain Markers and Dissociable Brain Systems. Neuron 2017, 94, 1263–1273. [Google Scholar] [CrossRef] [Green Version]
- Leiberg, S.; Klimecki, O.; Singer, T. Short-Term Compassion Training Increases Prosocial Behavior in a Newly Developed Prosocial Game. PLoS ONE 2011, 6, e17798. [Google Scholar] [CrossRef]
- Neff, K.D.; Germer, C.K. A Pilot Study and Randomized Controlled Trial of the Mindful Self-Compassion Program. J. Clin. Psychol. 2013, 69, 28–44. [Google Scholar] [CrossRef] [PubMed]
- Demarzo, M.; Montero-Marin, J.; Puebla-Guedea, M.; Navarro-Gil, M.; Herrera-Mercadal, P.; Moreno-González, S.; Calvo-Carrión, S.; Bafaluy-Franch, L.; Garcia- Campayo, J. Efficacy of 8- and 4-Session Mindfulness-Based Interventions in a Non-Clinical Population: A Controlled Study. Front. Psychol. 2017, 8, 1343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérula de Torres, L.A.; Atalaya, J.C.V.M.; García Campayo, J.; Roldán Villalobos, A.; Magallón Botaya, R.; Bartolomé Moreno, C.; Moreno Martos, H.; Melús Palazón, E.; Liétor Villajos, N.; Valverde Bolívar, F.J.; et al. Controlled Clinical Trial Comparing The Effectiveness of a Mindfulness and Self-Compassion 4-Session Programme Versus an 8-Session Programme to Reduce Work Stress and Burnout in Family and Community Medicine Physicians and Nurses: MINDUUDD Study Protocol. BMC Fam. Pract. 2019, 20, 24. [Google Scholar] [CrossRef]
- Dobkin, P.L.; Irving, J.A.; Amar, S. For Whom May Participation in a Mindfulness-Based Stress Reduction Program Be Contraindicated? Mindfulness 2012, 3, 44–50. [Google Scholar] [CrossRef]
- Silva, L.C. Sampling for Research in Health Sciences, 1st ed.; Diaz de Santos: Madrid, Spain, 1993. [Google Scholar]
- Campbell, M.; Grimshaw, J.; Steen, N. Sample Size Calculations for Cluster Randomised Trials. J. Health Serv. Res. Policy 2000, 5, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Brito, G. Secular Compassion Training: An Empirical Review. J. Transpersonal Res. 2014, 6, 61–71. [Google Scholar]
- Gilbert, P. Therapy Centered on Compassion. Distinctive Features, 1st ed.; Desclée de Brouwer, S.A.: Bilbao, Spain, 2015. [Google Scholar]
- Tirch, D.D. Mindfulness as a Context for the Cultivation of Compassion. Int. J. Cogn. Ther. 2010, 3, 113–123. [Google Scholar] [CrossRef] [Green Version]
- Cebolla, A.; García-Palacios, A.; Soler, J.; Guillen, V.; Baños, R.; Botella, C. Psychometric Properties of the Spanish Validation of the Five Facets of Mindfulness Questionnaire (FFMQ). Rev. Eur. J. Psychiat. 2012, 26, 118–126. [Google Scholar] [CrossRef] [Green Version]
- Aguado, J.; Luciano, J.V.; Cebolla, A.; Serrano-Blanco, A.; Soler, J.; García-Campayo, J. Bifactor Analysis and Construct Validity of the Five Facet Mindfulness Questionnaire (FFMQ) in Non-Clinical Spanish samples. Front. Psicol. 2015, 6, 404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using Self-Report Assessment Methods to Explore Facets of Mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef] [Green Version]
- Baer, R.A.; Smith, G.T.; Lykins, E.; Button, D.; Krietemeyer, J.; Sauer, S.; Walsh, E.; Duggan, D.; Williams, J.M.G. Construct Validity of the Five Facet Mindfulness Questionnaire in Meditating and Nonmeditating Samples. Assessment 2008, 15, 329–342. [Google Scholar] [CrossRef]
- Neff, K.D. Development and Validation of a Scale to Measure Self-Compassion. Self. Identity 2003, 2, 223–250. [Google Scholar] [CrossRef]
- García Campayo, J.; Navarro Gil, M.; Andrés, E.; Montero Marín, J.; López Artal, L.; Demarzo, M. Validation of the Spanish Versions of the Long (26 items) and Short (12 items) Forms of the Self-Compassion Scale (SCS). Health Qual. Life Outcomes 2014, 12, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcorta Garza, A.; González Guerrero, J.F.; Tavitas Herrera, S.E.; Rodríguez Lara, F.J.; Hojat, M. Validation of the Jefferson Scale for Physician Empathy in Mexican Medical Students. Salud Ment. 2005, 28, 57–63. [Google Scholar]
- Blanco, J.M.; Caballero, F.; García, F.J.; Lorenzo, F.; Monge, D. Validation of the Jefferson Scale of Physician Empathy in Spanish Medical Students Who Participated in an Early Clerkship Immersion Programme. BMC Med. Educ. 2018, 18, 209. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, C.J. An Effect Size Primer: A Guide for Clinicians and Researchers. Prof. Psychol. Res. Pr. 2009, 40, 532–538. [Google Scholar] [CrossRef] [Green Version]
- Montero-Marin, J.; Garcia-Campayo, J.; Pérez-Yus, M.C.; Zabaleta-Del-Olmo, E.; Cuijpers, P. Meditation Techniques v. Relaxation Therapies when Treating Anxiety: A Meta-Analytic Review. Psychol. Med. 2019, 49, 2118–2133. [Google Scholar] [CrossRef]
- Khusid, M.A.; Vythilingam, M. The Emerging Role of Mindfulness Meditation as Effective Self-Management Strategy, Part 1: Clinical Implications for Depression, Post-Traumatic Stress Disorder, and Anxiety. Mil. Med. 2016, 181, 961–968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juul, L.; Pallesen, K.J.; Bjerggaard, M.; Nielsen, C.; Fjorback, L.O. A Pilot Randomised Trial Comparing a Mindfulness-Based Stress Reduction Course, a Locally-Developed Stress Reduction Intervention and a Waiting List Control Group in a Real-Life Municipal Health Care Setting. BMC Public Health 2020, 20, 409. [Google Scholar] [CrossRef]
- Lomas, T.; Medina, J.C.; Ivtzan, I.; Rupprecht, S.; Eiroa-Orosa, F.J. A Systematic Review of the Impact of Mindfulness on the Well-Being of Healthcare Professionals. J. Clin. Psychol. 2018, 74, 319–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, K.T.; Dunbar, M.; Speelman, D.L. Effectiveness of Using a Meditation App in Reducing Anxiety and Improving Well-Being during the COVID-19 Pandemic: A Structured Summary of a Study Protocol for a Randomized Controlled Trial. Trials 2020, 21, 1006. [Google Scholar] [CrossRef]
- Reyes, A.T. A Mindfulness Mobile App for Traumatized COVID-19 Healthcare Workers and Recovered Patients: A Response to “The Use of Digital Applications and COVID-19”. Community Ment. Health J. 2020, 56, 1204–1205. [Google Scholar] [CrossRef]
- Shapiro, S.L.; Astin, J.A.; Bishop, S.R.; Cordova, M. Mindfulness-Based Stress Reduction for Health Care Professionals: Results from a Randomized Trial. Int. J. Stress Manag. 2005, 12, 164–176. [Google Scholar] [CrossRef] [Green Version]
- Keng, S.L.; Smoski, M.J.; Robins, C.J.; Ekblad, A.G.; Brantley, J.G. Mechanisms of Change in Mindfulness-Based Stress Reduction: Self-Compassion and Mindfulness as Mediators of Intervention Outcomes. J. Cogn. Psychother. 2012, 26, 270–280. [Google Scholar] [CrossRef]
- Krasner, M.S.; Epstein, R.M.; Beckman, H.; Suchman, A.L.; Chapman, B.; Mooney, C.J.; Quill, T.E. Association of an Educational Program in Mindful Communication with Burnout, Empathy, and Attitudes among Primary Care Physicians. JAMA 2009, 302, 1284–1293. [Google Scholar] [CrossRef] [Green Version]
- Neff, K.D. Self-Compassion: An Alternative Conceptualization of a Healthy Attitude Toward Oneself. Self Identity 2003, 2, 85–101. [Google Scholar] [CrossRef] [Green Version]
- Gracia Gozalo, R.M.; Ferrer Tarrés, J.M.; Ayora Ayora, A.; Alonso Herrero, M.; Amutio Kareaga, A.; Ferrer Roca, R. Application of a Mindfulness Program among Healthcare Professionals in an Intensive Care Unit: Effect on Burnout, Empathy and Self-Compassion. Med. Intensiva 2019, 43, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Conversano, C.; Ciacchini, R.; Orrù, G.; Di Giuseppe, M.; Gemignani, A.; Poli, A. Mindfulness, Compassion, and Self-Compassion Among Health Care Professionals: What’s New? A Systematic Review. Front. Psychol. 2020, 11, 1683. [Google Scholar] [CrossRef] [PubMed]
- Wasson, R.S.; Barratt, C.; O’Brien, W.H. Effects of Mindfulness-Based Interventions on Self-Compassion in Health Care Professionals: A Meta-Analysis. Mindfulness 2020, 11, 1914–1934. [Google Scholar] [CrossRef] [Green Version]
- Irving, J.A.; Dobkin, P.L.; Park, J. Cultivating Mindfulness in Health Care Professionals: A Review of Empirical Studies of Mindfulness-Based Stress Seduction (MBSR). Complement. Ther. Clin. Pract. 2009, 15, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Amutio, A.; Martínez-Taboada, C.; Delgado, L.C.; Hermosilla, D.; Mozaz, M.J. Acceptability and Effectiveness of a Long-Term Educational Intervention to Reduce Physicians’ Stress-Related Conditions. J. Contin. Educ. Health Prof. 2015, 35, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Galantino, M.L.; Baime, M.; Maguire, M.; Szapary, P.O.; Farrar, J.T. Association of Psychological and Physiological Measures of Stress in Health-Care Professionals During an 8-Week Mindfulness Meditation Program: Mindfulness in Practice. Stress Health 2005, 21, 255–261. [Google Scholar] [CrossRef]
- Raab, K. Mindfulness, Self-Compassion, and Empathy among Health Care Professionals: A Review of the Literature. J. Health Care Chaplain. 2014, 20, 95–108. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total (n = 112) | CG (n = 51) | EG1 (n = 24) | EG2 (n = 37) | p-Value |
|---|---|---|---|---|---|
| Age (years) | 41.61 ± 12.61 | 40.34 ± 13.22 | 47.66 ± 13.67 | 35.73 ± 12.04 | <0.001 |
| Sex | |||||
| Male | 26 (23.21) | 11 (21.57) | 6 (25.00) | 9 (24.32) | 0.978 |
| Female | 86 (76.79) | 40 (78.43) | 18 (75.00) | 28 (75.68) | |
| Occupation | |||||
| Physician | 95 (84.82) | 41 (80.39) | 20 (83.33) | 34 (91.89) | 0.165 |
| Nurse | 17 (15.18) | 10 (19.61) | 4 (16.67) | 3 (8.11) | |
| Professional type | |||||
| Tutor | 50 (44.64) | 24 (47.06) | 15 (62.50) | 11 (29.73) | <0.001 |
| Resident | 62 (55.36) | 27 (52.94) | 9 (37.50) | 26 (70.27) | |
| Work-place | |||||
| Health Center | 95 (84.82) | 40 (78.43) | 22 (91.67) | 33 (89.19) | 0.217 |
| Hospital | 17 (15.18) | 11 (21.57) | 2 (8.33) | 4 (10.81) | |
| Work experiences (years) | 12.88 ± 13.15 | 13.13 ± 12.95 | 19.49 ± 13.91 | 8.91 ± 11.06 | <0.001 |
| Evaluation | Variable | CG | EG1 | EG2 | F | p-Value | η2 | |||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |||||
| Pre-test | FFMQ | 118.17 | 13.32 | 117.71 | 16.76 | 119.26 | 15.11 | 0.153 | 0.858 | 0.002 |
| SCS | 2.88 | 0.73 | 2.97 | 0.88 | 2.82 | 0.93 | 0.381 | 0.683 | 0.005 | |
| JSPE | 124.14 | 8.53 | 120.12 | 15.98 | 122.44 | 12.72 | 1.281 | 0.281 | 0.016 | |
| Post-test | FFMQ | 119.28 * | 17.79 | 124.07 | 22.60 | 131.65 * | 18.03 | 5.004 | 0.008 | 0.076 |
| SCS | 2.98 * | 0.89 | 3.15 | 0.98 | 3.47 * | 0.74 | 3.789 | 0.025 | 0.058 | |
| JSPE | 124.35 | 8.40 | 120.85 | 15.74 | 126.85 | 9.06 | 2.634 | 0.076 | 0.041 | |
| Follow-up | FFMQ | 121.03 * | 18.29 | 125.04 | 22.62 | 131.97 * | 18.22 | 3.461 | 0.035 | 0.060 |
| SCS | 2.96 * | 0.90 | 3.21 | 1.04 | 3.46 * | 0.78 | 3.289 | 0.041 | 0.057 | |
| JSPE | 123.96 | 8.06 | 125.50 | 12.39 | 124.35 | 18.23 | 0.113 | 0.893 | 0.002 | |
| Group | Variable | Pre-Test | Post-Test | Follow-Up | MS | F | p-Value | η2 | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | ||||||
| CG | FFMQ | 118.17 | 13.32 | 119.28 | 17.79 | 121.03 | 18.29 | 205.283 | 2.009 | 0.143 | 0.059 |
| SCS | 2.88 | 0.73 | 2.98 | 0.89 | 2.96 | 0.90 | 0.127 | 0.971 | 0.384 | 0.029 | |
| JSPE | 124.14 | 8.53 | 124.35 | 8.40 | 123.96 | 8.06 | 23.303 | 0.578 | 0.564 | 0.018 | |
| EG1 | FFMQ | 117.71 | 16.76 | 124.07 | 22.60 | 125.04 | 22.62 | 242.902 | 2.736 | 0.080 | 0.146 |
| SCS | 2.97 | 0.88 | 3.15 | 0.98 | 3.21 | 1.04 | 0.163 | 1.160 | 0.326 | 0.068 | |
| JSPE | 120.12 * | 15.98 | 120.85 | 15.74 | 125.50 * | 12.39 | 240.137 | 4.584 | 0.018 | 0.223 | |
| EG2 | FFMQ | 119.26 *,$ | 15.11 | 131.65 $ | 18.03 | 131.97 * | 18.22 | 681.722 | 8.473 | 0.001 | 0.269 |
| SCS | 2.82 *,$ | 0.93 | 3.47 $ | 0.74 | 3.46 * | 0.78 | 1.483 | 9.356 | <0.001 | 0.289 | |
| JSPE | 122.44 | 12.72 | 126.85 | 9.06 | 124.35 | 18.23 | 245.847 | 1.596 | 0.214 | 0.065 | |
| Variable | Source | Type III Sum of Square | df | MS | F | p-Value | η2 |
|---|---|---|---|---|---|---|---|
| FFMQ | FFMQ pre-test | 10,240.20 | 1 | 10,240.21 | 46.396 | <0.001 | 0.338 |
| CG/EG1/EG2 | 1443.94 | 2 | 721.97 | 3.271 | 0.042 | 0.067 | |
| Error | 20,084.98 | 91 | 220.71 | ||||
| SCS | SCS pre-test | 38.90 | 1 | 38.09 | 101.675 | <0.001 | 0.528 |
| CG/EG1/EG2 | 4.53 | 2 | 2.26 | 6.046 | 0.003 | 0.117 | |
| Error | 34.09 | 91 | 0.37 | ||||
| JSPE | JSPE pre-test | 3400.18 | 1 | 3400.18 | 39.316 | 0.001 | 0.302 |
| CG/EG1/EG2 | 328.79 | 2 | 164.39 | 1.901 | 0.155 | 0.040 | |
| Error | 7870.04 | 91 | 86.48 |
| Variable | Source | Type III Sum of Square | df | MS | F | p-Value | η2 |
|---|---|---|---|---|---|---|---|
| FFMQ | FFMQ pre-test | 13,867.36 | 1 | 13,867.36 | 66.304 | <0.001 | 0.456 |
| CG/EG1/EG2 | 687.25 | 2 | 343.63 | 1.643 | 0.200 | 0.040 | |
| Error | 16,522.68 | 79 | 209.15 | ||||
| SCS | SCS pre-test | 37.15 | 1 | 37.15 | 114.242 | <0.001 | 0.591 |
| CG/EG1/EG2 | 2.52 | 2 | 1.26 | 3.880 | 0.025 | 0.089 | |
| Error | 25.69 | 79 | 0.32 | ||||
| JSPE | JSPE pre-test | 3259.28 | 1 | 3259.29 | 20.553 | <0.001 | 0.206 |
| CG/EG1/EG2 | 732.76 | 2 | 366.38 | 2.310 | 0.106 | 0.055 | |
| Error | 12,527.60 | 79 | 158.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérula-de Torres, L.Á.; Verdes-Montenegro-Atalaya, J.C.; Melús-Palazón, E.; García-de Vinuesa, L.; Valverde, F.J.; Rodríguez, L.A.; Lietor-Villajos, N.; Bartolomé-Moreno, C.; Moreno-Martos, H.; García-Campayo, J.; et al. Comparison of the Effectiveness of an Abbreviated Program versus a Standard Program in Mindfulness, Self-Compassion and Self-Perceived Empathy in Tutors and Resident Intern Specialists of Family and Community Medicine and Nursing in Spain. Int. J. Environ. Res. Public Health 2021, 18, 4340. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084340
Pérula-de Torres LÁ, Verdes-Montenegro-Atalaya JC, Melús-Palazón E, García-de Vinuesa L, Valverde FJ, Rodríguez LA, Lietor-Villajos N, Bartolomé-Moreno C, Moreno-Martos H, García-Campayo J, et al. Comparison of the Effectiveness of an Abbreviated Program versus a Standard Program in Mindfulness, Self-Compassion and Self-Perceived Empathy in Tutors and Resident Intern Specialists of Family and Community Medicine and Nursing in Spain. International Journal of Environmental Research and Public Health. 2021; 18(8):4340. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084340
Chicago/Turabian StylePérula-de Torres, Luis Ángel, Juan Carlos Verdes-Montenegro-Atalaya, Elena Melús-Palazón, Leonor García-de Vinuesa, Francisco Javier Valverde, Luis Alberto Rodríguez, Norberto Lietor-Villajos, Cruz Bartolomé-Moreno, Herminia Moreno-Martos, Javier García-Campayo, and et al. 2021. "Comparison of the Effectiveness of an Abbreviated Program versus a Standard Program in Mindfulness, Self-Compassion and Self-Perceived Empathy in Tutors and Resident Intern Specialists of Family and Community Medicine and Nursing in Spain" International Journal of Environmental Research and Public Health 18, no. 8: 4340. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084340