
Effects of Internet-Based Support Program on Parenting Outcomes for Primiparous Women: A Pilot Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Intervention
2.4. Outcomes
2.4.1. Primary Outcomes
2.4.2. Secondary Outcomes
2.4.3. Other Outcomes
2.5. Data Collection
2.6. Data Analysis
3. Results
3.1. Baseline Characteristics
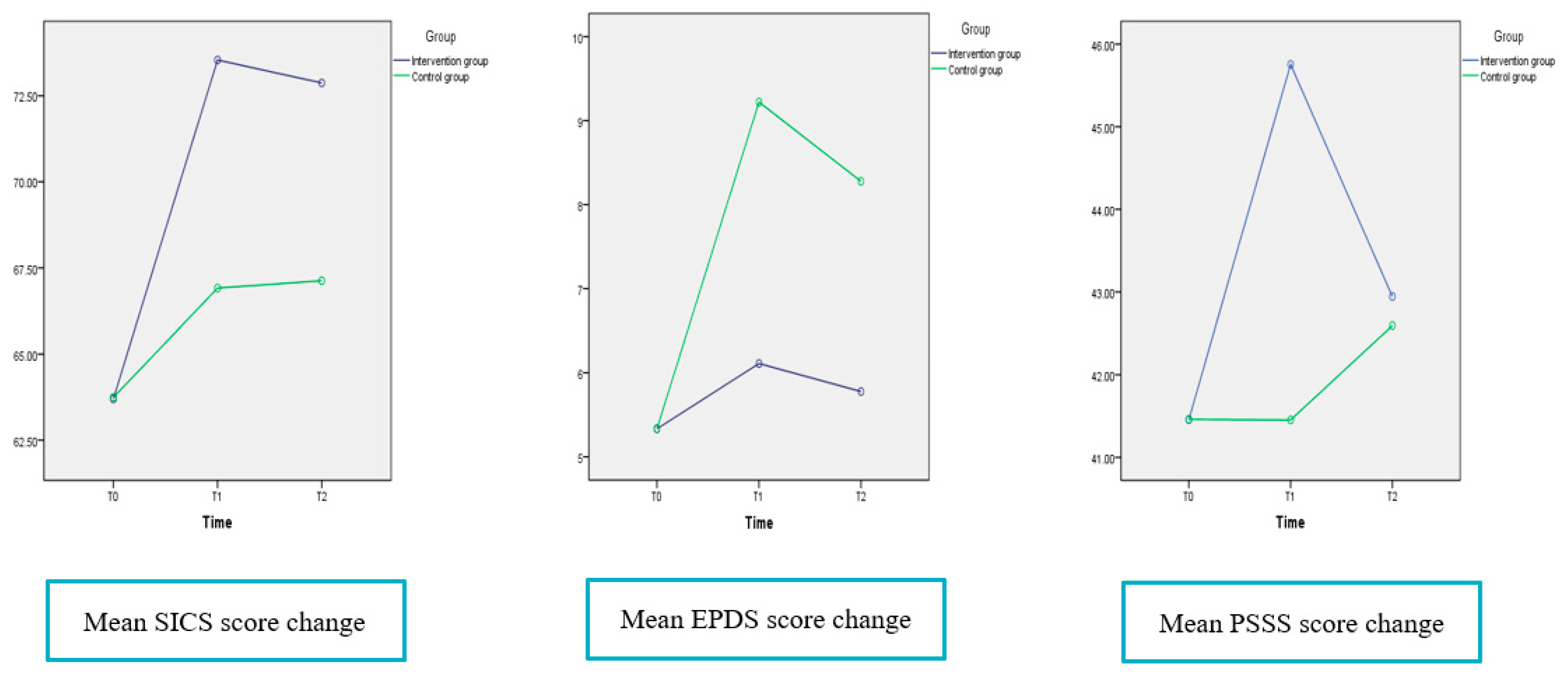
3.2. Effectiveness of the ISP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zheng, X.J.; Morrell, J.; Watts, K. An Exploration of Factors Which Influence Maternal Self-Efficacy in Primiparous Women in China during the Initial Postnatal Period. Ph.D. Thesis, The University of Nottingham, Nottingham, UK, 2015. [Google Scholar]
- Zheng, X.J.; Morrell, J.; Watts, K. Changes in maternal self-efficacy, postnatal depression symptoms and social support among Chinese primiparous women during the initial postpartum period: A longitudinal study. Midwifery 2018, 62, 151–160. [Google Scholar] [CrossRef] [Green Version]
- Li, X.W.; Liu, Y. Parent-Grandparent Coparenting Relationship, maternal parenting self-efficacy, and young children’s social competence in Chinese urban families. J. Child Fam. Stud. 2019, 28, 1145–1153. [Google Scholar] [CrossRef]
- Montigny, F.; Lacharite, C. Perceived parental self-efficacy: Concept analysis. J. Adv. Nurs. 2005, 49, 387–396. [Google Scholar] [CrossRef]
- Fulton, J.M.; Mastergeorge, A.M.; Steele, J.S.; Hansen, R. Maternal perceptions of the infant: Relationship to maternal self-efficacy during this first six week’s postpartum. Infant. Ment. Health J. 2012, 33, 329–338. [Google Scholar] [CrossRef]
- Whittaker, K.A.; Cowley, S. A survey of parental self-efficacy experiences: Maximising potential through health visiting and universal parenting support. J. Clin. Nurs. 2012, 21, 3276–3286. [Google Scholar] [CrossRef] [PubMed]
- Pierce, T.; Boivin, M.; Frenettea, E.; Forget-Duboisa, N.; Dionnea, G.; Tremblayb, R.E. Maternal self-efficacy and hostile-reactive parenting from infancy to toddlerhood. Infant Behav. Dev. 2010, 33, 149–158. [Google Scholar] [CrossRef]
- Salonen, A.H.; Kaunonen, M.; Astedt-Kurkip, P.; Järvenpää, A.L.; Isoaho, H.; Tarkka, M.T. Parenting self-efficacy after childbirth. J. Adv. Nurs. 2009, 65, 2324–2336. [Google Scholar] [CrossRef]
- Salonen, A.H.; Kaunonen, M.; Astedt-Kurki, P.; Järvenpää, A.L.; Isoaho, H.; Tarkka, M.T. Effectiveness of an internet-based intervention enhancing Finnish parents’ parenting satisfaction and parenting self-efficacy during the postnatal period. Midwifery 2011, 27, 832–841. [Google Scholar] [CrossRef]
- Zheng, X.J.; Huang, L.L.; Fang, Q.Y.; Zhang, Y.; Zhang, Y.; Li, X.L.; Ye, Z.W.; Wang, Q. Internet-based support program on parenting outcomes for Chinese primiparous women: Study protocol for a randomized controlled trial. J. Adv. Nurs. 2020, 76, 1–9. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, Y.; Li, X.L.; Ye, Z.W.; Huang, L.L.; Zhang, Y.; Zheng, X.J. Exploring maternal self-efficacy of first-time mothers among rural-to-urban floating women: A quantitative longitudinal study in China. Int. J. Environ. Res. Public Health 2021, 18, 2793. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.L.; Chan, S.W.; Sun, K. Effects of an interpersonal-psychotherapy-oriented childbirth education program for Chinese first-time childbearing women at 3-month follow-up: Randomized controlled trial. Int. J. Nurs. Stud. 2012, 49, 274–281. [Google Scholar] [CrossRef]
- Zheng, X.J.; Morrell, J.; Watts, K. A quantitative longitudinal study to explore factors which influence maternal self-efficacy among Chinese primiparous women during the initial postpartum period. Midwifery 2018, 59, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Perez-Blasco, J.; Viguer, P.; Rodrigo, M.F. Effects of a mindfulness-based intervention on psychological distress, well-being, and maternal self-efficacy in breast-feeding mothers: Results of a pilot study. Arch. Women Ment. Health 2013, 16, 227–236. [Google Scholar] [CrossRef]
- Gao, L.L.; Sun, K.; Chan, S.W. Social support and parenting self-efficacy among Chinese women in the perinatal period. Midwifery 2014, 30, 532–538. [Google Scholar] [CrossRef]
- Zhu, J.M.; Ebert, L.; Liu, X.Y.; Chan, W.C. A mobile application of breast cancer e-support program versus routine care in the treatment of Chinese women with breast cancer undergoing chemotherapy: Study protocol for a randomized controlled trial. BMC Cancer 2017, 17, 291. [Google Scholar] [CrossRef] [Green Version]
- Van den Berg, S.W.; Gielissen, M.F.; Ottevanger, P.B.; Prins, J.B. Rationale of the BREAst cancer e-healTH [BREATH] multicentre randomised controlled trial: An internet-based self-management intervention to foster adjustment after curative breast cancer by decreasing distress and increasing empowerment. BMC Cancer 2012, 12, 394. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.Y.; Tse, M.; Tang, A. The effectiveness of a dyadic pain management program for community-dwelling older adults with chronic pain: A pilot randomized controlled trial. Int. J. Environ. Res. Public Health 2020, 17, 4966. [Google Scholar] [CrossRef]
- Friesen, N.L.; Hadjistavropoulos, D.H.; Schneider, H.L.; Alberts, M.N.; Titov, F.N.; Dear, F.B. Examination of an internet-delivered cognitive behavioural pain management course for adults with fibromyalgia: A randomized controlled trial. PAIN 2017, 158, 593–604. [Google Scholar] [CrossRef]
- Natalie, K.; Jessica, S.; Shivani, U.; Mathew, A.J.; Adrian, R.A.; Gavin, A.; Jill, M.N. Transdiagnostic internet-delivered CBT and mindfulness-based treatment for depression and anxiety: A randomized controlled trial. Internet Interv. 2020, 20, 100310. [Google Scholar]
- Lee, C.S.; Vellone, E.; Lyons, K.S.; Cocchieri, A.; Bidwell, J.T.; D’Agostino, F.; Hiatt, S.O.; Alvaro, R.; Buck, H.G.; Riegel, B. Patterns and predictors of patient and caregiver engagement in heart failure care: A multi-level dyadic study. Int. J. Nurs. Stud. 2015, 52, 588–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- China News 2020. Big Data of Chinese Netizens’ Behavior. Available online: https://news.sina.cn/2019-02-20/detail-ihqfskcp7055720.d.html (accessed on 7 March 2021). (In Chinese).
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2011, 9, 672–677. [Google Scholar] [CrossRef] [Green Version]
- Prasopkittikun, T.; Tilokskulchai, F. Self-efficacy in Infant Care Scale: Revision and further. Nurs. Health Sci. 2010, 12, 450–455. [Google Scholar] [CrossRef]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression: Development of the 10-item Edinburgh postnatal depression scale. Br. J. Psychiatry. 1987, 150, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.Q.; Guo, X.J.; Lau, Y.; Chan, K.S.; Yin, L.; Chen, J. Psychometric evaluation of the Mainland Chinese version of the Edinburgh postnatal depression scale. Int. J. Nurs. Stud. 2009, 46, 813–823. [Google Scholar] [CrossRef]
- Lu, H.; Zheng, X.X. The relationship between social support and postnatal depression of primiparous women. Chin. J. Nurs. 2001, 36, 731–733. (In Chinese) [Google Scholar]
- Bandura, A. Self-Efficacy: The Exercise of Control, 1st ed.; Freeman and Co.: New York, NY, USA, 1997. [Google Scholar]
- Zang, S.M.; Sheng, Y. Study on influencing factors of maternal self-efficacy in primiparous women. Chin. J. Mod. Nurs. 2010, 16, 2980–2982. (In Chinese) [Google Scholar]
- Porter, C.H.; Hsu, H.C. First-time mothers ’perceptions of efficacy during the transition to motherhood: Links to infant temperament. J. Fam. Psychol. 2003, 17, 54–64. [Google Scholar] [CrossRef]
- Gavin, N.I.; Gaynes, B.N.; Lohr, K.N.; Meltzer-Brody, S.; Gartlehner, G.; Swinson, T. Perinatal depression: A systematic review of prevalence and incidence. Obstet. Gynecol. 2005, 106, 1071–1083. [Google Scholar] [CrossRef]
- Hewitt, C.; Gilbody, S.; Brealey, S.M.; Paulden, M.; Palmer, S.; Mann, R.; Green, J.; Morrell, J.; Barkham, M.; Light, K.; et al. Methods to identify postnatal depression in primary care: An integrated evidence synthesis and value of information analysis. Health Technol. Assess. 2009, 13, 1–145. [Google Scholar] [CrossRef] [Green Version]
- Zhu, J.M.; Ebert, L.; Liu, X.Y.; Wei, D.; Chan, W.C. Mobile Breast Cancer e-Support Program for Chinese Women With Breast Cancer Undergoing Chemotherapy (Part 2): Multicenter Randomized Controlled Trial. JMIR mHealth uHealth 2018, 6, e104. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Components | Functions | Contents |
|---|---|---|
| Learning forum | Educational function |
|
| Communication forum | Social function |
|
| Ask-the-expert forum | Answering function |
|
| Baby home forum | Recording function |
|
| Reminder forum | Reminder function |
|
| Variables | Total (n = 40) | Intervention Group (n = 20) | Control Group (n = 20) | t/χ2 Value | p-Value |
|---|---|---|---|---|---|
| Maternal age, mean (SD) | 27.25 (3.04) | 27.15 (3.15) | 27.35 (3.00) | 0.013 | 0.908 |
| Marital status, n (%) | |||||
| Married | 40 (100) | 20 (100) | 20 (100) | 0.000 | 1.000 |
| Divorced | 0 (0) | 0 (0) | 0 (0) | ||
| Single | 0 (0) | 0 (0) | 0 (0) | ||
| Education, n (%) | 0.178 | 0.915 | |||
| Middle school or lower | 9 (22.5) | 5 (25) | 4 (20) | ||
| High school | 15 (37.5) | 7 (35) | 8 (40) | ||
| University or higher | 16 (40.0) | 8 (40) | 8 (40) | ||
| Occupation, n (%) | 0.443 | 0.931 | |||
| Professional | 15 (37.5) | 8 (40) | 7 (35) | ||
| Skilled | 7 (17.5) | 3 (15) | 4 (20) | ||
| Unskilled | 11 (27.5) | 6 (30) | 5 (25) | ||
| Unemployed | 7 (17.5) | 3 (15) | 4 (20) | ||
| Monthly family income, n (%) | 0.503 | 0.778 | |||
| <3000 yuan (US$420) | 5 (12.5) | 3 (15) | 2 (10) | ||
| 3001–5000 yuan (US$420–700) | 16 (40.0) | 7 (35) | 9 (45) | ||
| >5000 yuan (US$700) | 19 (47.5) | 10 (50) | 9 (45) | ||
| Delivery mode, n (%) | 0.582 | 0.748 | |||
| Natural childbirth | 22 (55) | 12 (60%) | 10 (50) | ||
| Assisted childbirth | 10 (25) | 4 (20%) | 6 (30) | ||
| C-section | 8 (20) | 4 (20%) | 4 (20) | ||
| Whether attending parenting train, n (%) | 0.000 | 1.000 | |||
| Yes | 18 (45) | 9 (45) | 9 (45) | ||
| No | 22 (55) | 11(55) | 11(55) | ||
| Baby gender, n (%) | 0.100 | 0.752 | |||
| Boy | 21 (52.5) | 10 (50) | 11 (55) | ||
| Girl | 19 (47.5) | 10 (50) | 9 (45) | ||
| Baby health, mean (SD) | 61.42 (18.13) | 61.70 (16.76) | 61.15 (19.83) | 0.701 | 0.408 |
| Baby fussiness, mean (SD) | 49.57 (12.68) | 50.20 (12.60) | 48.95 (13.05) | 1.636 | 0.209 |
| SICS, mean (SD) | 63.61 (7.13) | 63.49 (7.17) | 63.72 (7.27) | 0.023 | 0.880 |
| EPDS, mean (SD) | 5.15 (2.33) | 5.05 (2.54) | 5.25 (2.15) | 0.001 | 0.982 |
| PSSS, mean (SD) | 41.43 (2.78) | 41.43 (2.78) | 41.43 (2.86) | 0.309 | 0.581 |
| ISP Effect | Mean (SD) Intervention Group (n = 18) | Mean (SD) Control Group (n = 18) | Mean Difference (95% CI) | p-Value a |
|---|---|---|---|---|
| Outcomes | ||||
| MSE (SICS) | ||||
| T1 | 73.54 (6.38) | 66.91 (7.52) | 6.63 (1.90 to 11.35) | 0.007 |
| T2 | 72.87 (6.97) | 67.12 (7.10) | 5.75 (0.98 to 10.51) | 0.020 |
| Postpartum depression (EPDS) | ||||
| T1 | 6.11 (2.54) | 9.22 (3.30) | −3.11 (−5.11 to −1.12) | 0.003 |
| T2 | 5.78 (2.23) | 8.28 (2.66) | −2.50 (−4.17 to −0.83) | 0.005 |
| Social support (PSSS) | ||||
| T1 | 45.76 (3.85) | 41.45(2.92) | 4.30 (1.99 to 6.62) | 0.001 |
| T2 | 42.94 (3.39) | 42.59 (3.13) | 0.35 (−1.80 to 2.50) | 0.743 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, L.; Shen, Q.; Fang, Q.; Zheng, X. Effects of Internet-Based Support Program on Parenting Outcomes for Primiparous Women: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 4402. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094402
Huang L, Shen Q, Fang Q, Zheng X. Effects of Internet-Based Support Program on Parenting Outcomes for Primiparous Women: A Pilot Study. International Journal of Environmental Research and Public Health. 2021; 18(9):4402. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094402
Chicago/Turabian StyleHuang, Lingling, Qu Shen, Qiyu Fang, and Xujuan Zheng. 2021. "Effects of Internet-Based Support Program on Parenting Outcomes for Primiparous Women: A Pilot Study" International Journal of Environmental Research and Public Health 18, no. 9: 4402. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094402