
Effect of Myofascial Therapy on Pain and Functionality of the Upper Extremities in Breast Cancer Survivors: A Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registry
2.2. Search and Information Sources
2.3. Inclusion and Exclusion Criteria
2.3.1. Types of Studies
2.3.2. Types of Participants
2.3.3. Types of Interventions
2.3.4. Types of Outcome Measures
2.4. Study Selection
2.5. Data Extraction and Management
2.6. Risk of Bias Assessment
2.7. Statistical Analysis
3. Results
3.1. Selection of Studies
3.2. Characteristics of Studies Included
3.3. Characteristics of the Participants
3.4. Characteristics of the Interventions
3.5. Outcome Measures
3.5.1. Primary Measures
3.5.2. Secondary Measures
3.6. Follow-Up
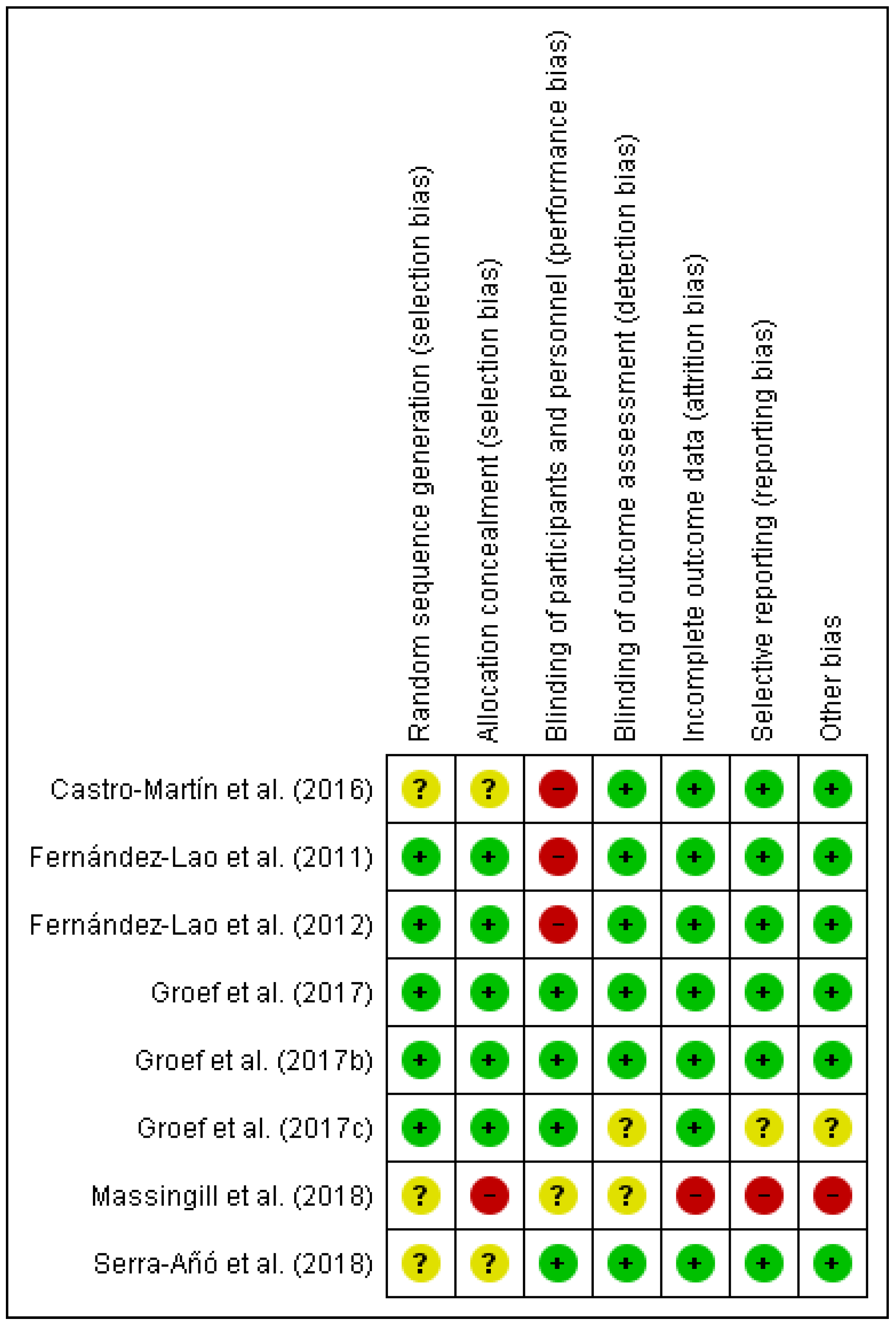
3.7. Risk of Bias in the Studies Included
3.8. Effects of the Interventions
3.8.1. Myofascial Therapy vs. Placebo Treatment or Other Intervention at Post-Immediate
- Pain Intensity
- 2.
- Functionality
- 3.
- Range of motion
3.8.2. Myofascial Therapy vs. Placebo Treatment or Minimal Intervention at Post-Immediate
- Pain intensity
- 2.
- Range of motion
- 3.
- Mood state
3.8.3. Myofascial Technique (Physical Therapy and Myofascial Therapy) vs. Other Interventions (Physical Therapy and Placebo) at Post-Immediate, Medium Term and Long Term
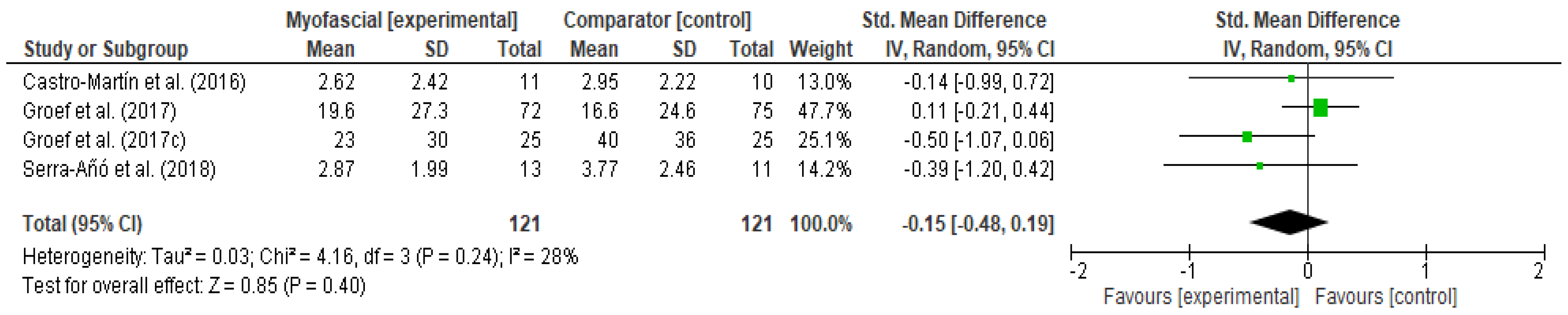
- Pain Intensity
- 2.
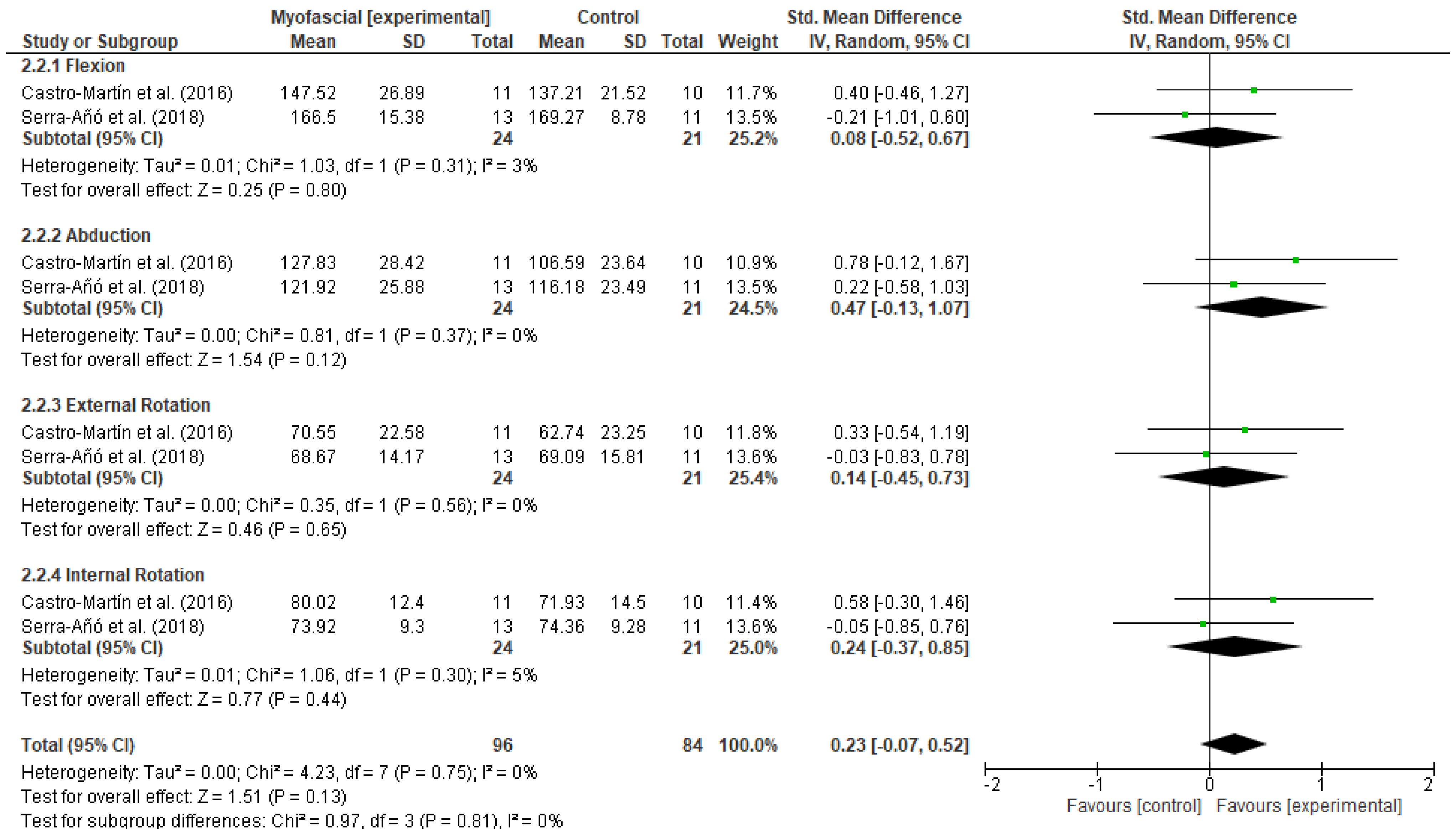
- Functionality
- 3.
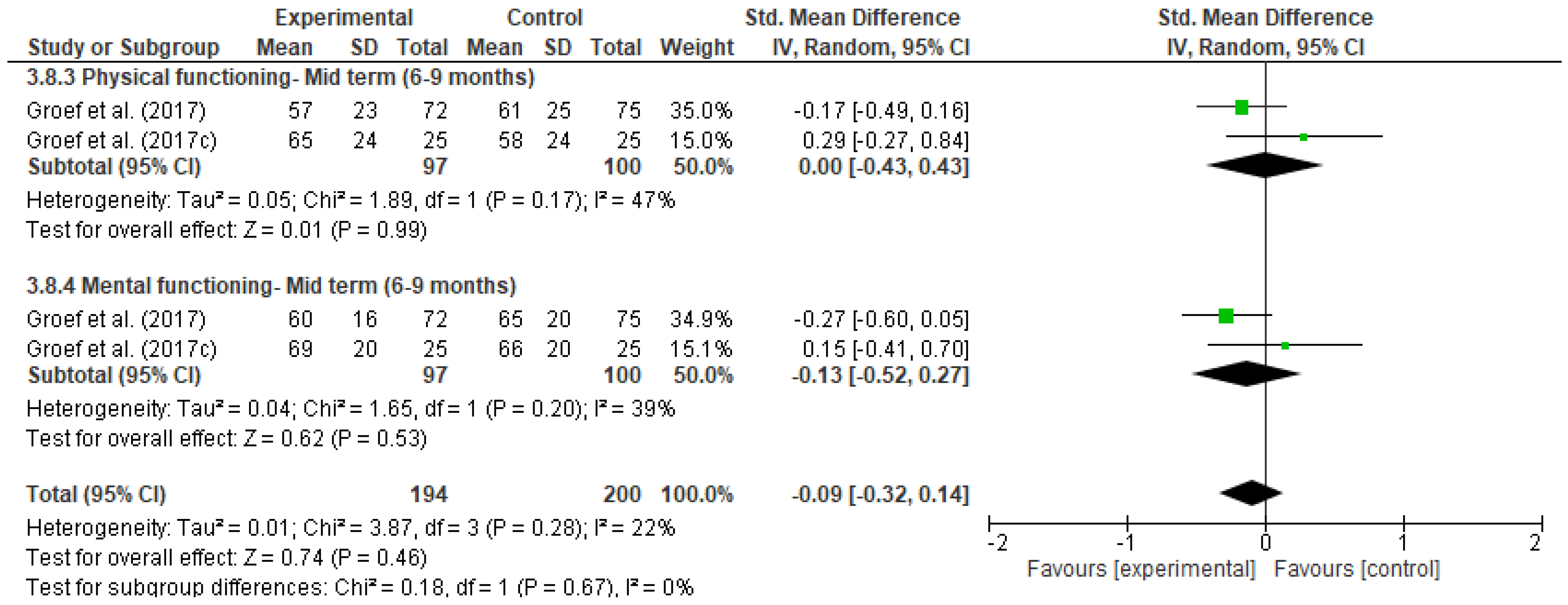
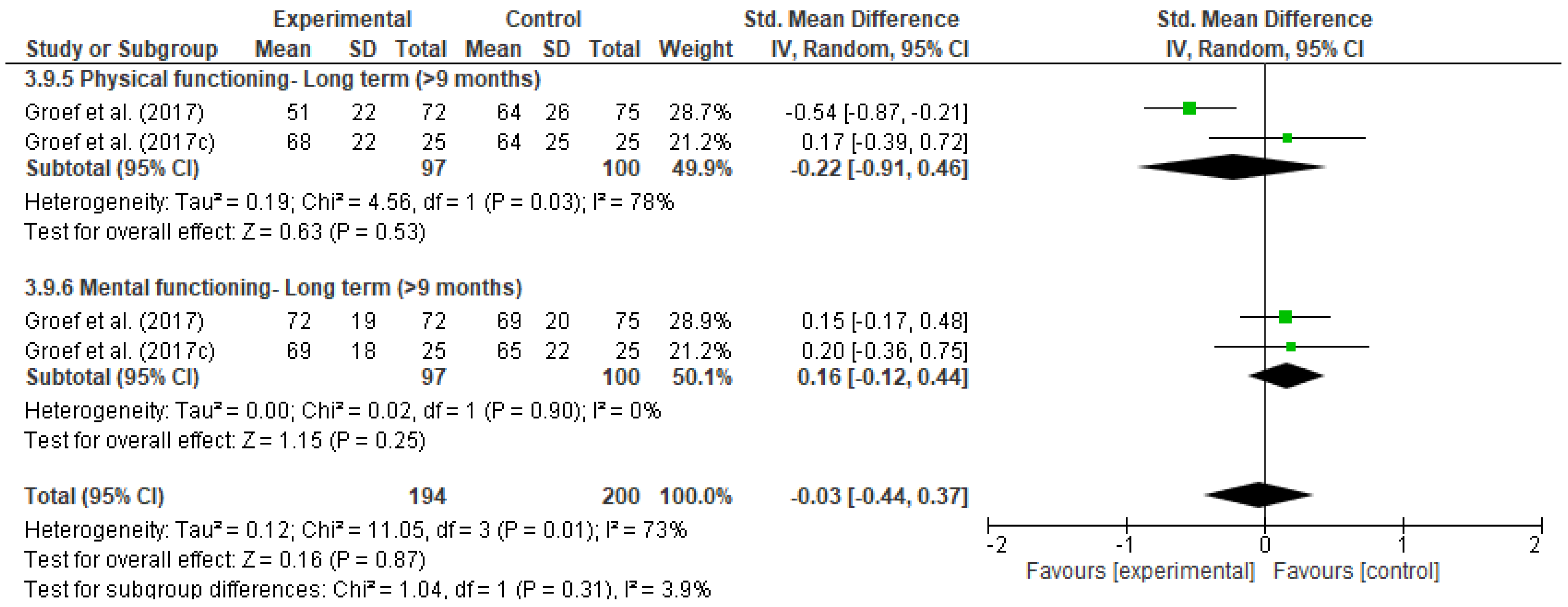
- Quality of life
4. Discussion
4.1. Summary of Evidence
4.2. Agreements or Disagreements with Other Studies or Reviews
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aapro, M.; Piccart, M. Breast cancer. Crit. Rev. Oncol. Hematol. 1998, 27, 135–137. [Google Scholar] [CrossRef]
- Bray, F.; Ren, J.; Masuyer, E.; Ferlay, J. Global estimates of cancer prevalence for 27 sites in the adult population in 2008. Int. J. Cancer 2013, 132, 1133–1145. [Google Scholar] [CrossRef]
- Naghavi, M.; Abajobir, A.; Abbafati, C.; Abbas, K.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Afshin, A.; Agrawal, A.; et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar]
- Fitzmaurice, C.; Akinyemiju, T.; Al Lami, F.; Alam, T.; Alizadeh-Navaei, R.; Allen, C.; Alsharif, U.; Alvis-Guzman, N.; Amini, E.; Anderson, B.O.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2016. JAMA Oncol. 2018, 4, 1553. [Google Scholar]
- Rojas, K.; Stuckey, A. Breast Cancer Epidemiology and Risk Factors. Clin. Obstet. Gynecol. 2016, 59, 651–672. [Google Scholar] [CrossRef]
- Tabar, L.; Dean, P.B.; Chen, T.H.; Yen, A.M.-F.; Chen, S.L.S.; Fann, J.C.Y.; Chiu, S.Y.-H.; Ku, M.M.-S.; Wu, W.Y.; Hsu, C.-Y.; et al. The incidence of fatal breast cancer measures the increased effectiveness of therapy in women participating in mammography screening. Cancer 2019, 125, 515–523. [Google Scholar] [CrossRef]
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Bishop, K.; Altekruse, S.F.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; et al. SEER Cancer Statistics Review, 1975–2013; National Cancer Institute: Bethesda, MD, USA, 2016; Based on November 2015 SEER Data Submission, Posted to the SEER Web Site, April 2016. Available online: https://seer.cancer.gov/archive/csr/1975_2013/ (accessed on 1 December 2020).
- Warpenburg, M.J. Deep Friction Massage in Treatment of Radiation-induced Fibrosis: Rehabilitative Care for Breast Cancer Survivors. Integr. Med. 2014, 13, 32–36. [Google Scholar]
- Runowicz, C.D.; Leach, C.R.; Henry, N.L.; Henry, K.S.; Mackey, H.T.; Cowens-Alvarado, R.L.; Cannady, R.S.; Pratt-Chapman, M.L.; Edge, S.B.; Jacobs, L.A.; et al. American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline. CA Cancer J. Clin. 2016, 66, 43–73. [Google Scholar] [CrossRef]
- Lazovich, D.; Solomon, C.C.; Thomas, D.B.; Moe, R.E.; White, E. Breast conservation therapy in the United States following the 1990 National Institutes of Health Consensus Development Conference on the treatment of patients with early stage invasive breast carcinoma. Cancer 1999, 86, 628–637. [Google Scholar] [CrossRef]
- Douay, N.; Akerman, G.; Clément, D.; Malartic, C.; Morel, O.; Barranger, E. Seroma after axillary lymph node dissection in breast cancer. Gynecol. Obstet. Fertil. 2008, 36, 130–135. [Google Scholar] [CrossRef]
- Francis, W.; Abghari, P.; Du, W.; Rymal, C.; Suna, M.; Kosir, M. Improving surgical outcomes: Standardizing the reporting of incidence and severity of acute lymphedema after sentinel lymph node biopsy and axillary lymph node dissection. Am. J. Surg. 2006, 192, 636–639. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, Y.; Ohno, Y.; Kasahara, S.; Murata, K.; Sugiyama, H.; Oshima, A.; Tsukuma, H.; Ajiki, W.; Hasegawa, T. Statistical estimation of the number of breast cancer patients with disabilities resulting from surgery. Breast Cancer 2005, 12, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Madsen, A.; Haugaard, K.; Soerensen, J.; Bokmand, S.; Friis, E.; Holtveg, H.; Garne, J.; Horby, J.; Christiansen, P. Arm morbidity following sentinel lymph node biopsy or axillary lymph node dissection: A study from the danish breast cancer cooperative. Breast 2007, 10, 291–401. [Google Scholar]
- Nesvold, I.; Dahl, A.; Løkkevik, E.; Marit Mengshoel, A.; Fosså, S. Arm and shoulder morbidity in breast cancer patients after breast-conserving therapy versus mastectomy. Acta Oncol. 2008, 47, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.J.; Mendenhall, N.P.; Kamath, S.S.; Lind, S.S.; Haigh, L.S.; Copeland, E.M. Persistent symptomatology after breast conservation therapy: Prevalence and impact on quality of life. Int. J. Radiat. Oncol. Biol. Phys. 1998, 42, 2058. [Google Scholar] [CrossRef]
- Bentzen, S.M.; Thames, H.D.; Overgaard, M. Latent-time estimation for late cutaneous and subcutaneous radiation reactions in a single-follow-up clinical study. Radiother. Oncol. 1989, 15, 267–274. [Google Scholar] [CrossRef]
- Dupilka, A.; Gramling, K. Radiation Side Effects and Syndromes. Available online: http://www.physio-pedia.com/Radiation_Side_Effects_and_Syndromes (accessed on 21 April 2014).
- Stubblefield, M.D. Radiation fibrosis syndrome: Neuromuscular and musculoskeletal complications in cancer survivors. PM&R 2011, 3, 1041–1054. [Google Scholar]
- McDuff, S.G.R.; Mina, A.I.; Brunelle, C.L.; Salama, L.; Warren, L.E.; Abouegylah, M.; Swaroop, M.; Skolny, M.N.; Asdourian, M.; Gillespie, T.; et al. Timing of Lymphedema After Treatment for Breast Cancer: When Are Patients Most At Risk? Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 62–70. [Google Scholar] [CrossRef]
- Warren, L.E.G.; Miller, C.L.; Horick, N.; Skolny, M.N.; Jammallo, L.S.; Sadek, B.T.; Shenouda, M.N.; O’Toole, J.A.; MacDonald, S.M.; Specht, M.C. The impact of radiation therapy on the risk of lymphedema after treatment for breast cancer: A prospective cohort study. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 565–571. [Google Scholar] [CrossRef] [Green Version]
- Norman, S.A.; Localio, A.R.; Potashnik, S.L.; Torpey, H.A.S.; Kallan, M.J.; Weber, A.L.; Miller, L.T.; DeMichele, A.; Solin, L.J. Lymphedema in breast cancer survivors: Incidence, degree, time course, treatment, and symptoms. J. Clin. Oncol. 2009, 27, 390–397. [Google Scholar] [CrossRef]
- DiSipio, T.; Rye, S.; Newman, B.; Hayes, S. Incidence of unilateral arm lymphoedema after breast cancer: A systematic review and meta-analysis. Lancet Oncol. 2013, 14, 500–515. [Google Scholar] [CrossRef]
- Togawa, K.; Ma, H.; Sullivan-Halley, J.; Neuhouser, M.L.; Imayama, I.; Baumgartner, K.B.; Smith, A.W.; Alfano, C.M.; McTiernan, A.; Ballard-Barbash, R.; et al. Risk factors for self-reported arm lymphedema among female breast cancer survivors: A prospective cohort study. Breast Cancer Res. 2014, 16, 414. [Google Scholar] [CrossRef] [Green Version]
- Rupp, J.; Hadamitzky, C.; Henkenberens, C.; Christiansen, H.; Steinmann, D.; Bruns, F. Frequency and risk factors for arm lymphedema after multimodal breast-conserving treatment of nodal positive breast Cancer—A long-term observation. Radiat. Oncol. 2019, 14, 39. [Google Scholar] [CrossRef] [Green Version]
- Ridner, S.H. Quality of life and symptom cluster associated with breast cancer treatment-related lymphedema. Support. Care Cancer 2005, 13, 904–911. [Google Scholar] [CrossRef] [PubMed]
- Edmond, S.N.; Shelby, R.A.; Keefe, F.J.; Fisher, H.M.; Schmidt, J.; Soo, M.S.; Skinner, C.S.; Ahrendt, G.M.; Manculich, J.; Sumkin, J.H.; et al. Persistent Breast Pain Among Women with Histories of Breast-Conserving Surgery for Breast Cancer Compared with Women without Histories of Breast Surgery or Cancer. Clin. J. Pain 2017, 33, 51–56. [Google Scholar] [CrossRef] [Green Version]
- Bruce, J.; Thornton, A.; Powell, R.; Johnston, M.; Wells, M.; Heys, S.; Thompson, A.M.; Smith, W.C.; Chambers, W.A.; Scott, N.W.; et al. Psychological, surgical, and sociodemographic predictors of pain outcomes after breast cancer surgery: A population-based cohort study. Pain 2014, 155, 232–243. [Google Scholar] [CrossRef] [PubMed]
- Blumen, H.; Fitch, K.; Polkus, V. Comparison of Treatment Costs for Breast Cancer, by Tumor Stage and Type of Service. Am. Health Drug Benefits 2016, 9, 23–32. [Google Scholar] [PubMed]
- De Groef, A.; Van Kampen, M.; Dieltjens, E.; Christiaens, M.; Neven, P.; Geraerts, I.; Devoogdt, N. Effectiveness of Postoperative Physical Therapy for Upper-Limb Impairments After Breast Cancer Treatment: A Systematic Review. Arch. Phys. Med. Rehabil. 2015, 96, 1140–1153. [Google Scholar] [CrossRef] [PubMed]
- Borstad, J.; Ludewig, P. The Effect of Long Versus Short Pectoralis Minor Resting Length on Scapular Kinematics in Healthy Individuals. J. Orthop. Sports Phys. Ther. 2005, 35, 227–238. [Google Scholar] [CrossRef] [Green Version]
- McNeely, M.; Campbell, K.; Ospina, M.; Rowe, B.; Dabbs, K.; Klassen, T.; Mackey, J.; Courneya, K. Exercise interventions for upper-limb dysfunction due to breast cancer treatment. Cochrane Database Syst. Rev. 2010, 6, CD005211. [Google Scholar] [CrossRef]
- Pilat, A. Myofascial induction approaches. In Fascia: The Tensional Network of the Human Body. The Science and Clinical Applications in Manual and Movement Therapy; Churchill Livingstone: London, UK, 2011; p. 455. [Google Scholar]
- Rodríguez-Huguet, M.; Gil-Salú, J.L.; Rodríguez-Huguet, P.; Cabrera-Afonso, J.R.; Lomas-Vega, R. Effects of Myofascial Release on Pressure Pain Thresholds in Patients with Neck Pain: A Single-Blind Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2018, 97, 16–22. [Google Scholar] [CrossRef]
- Chamorro Comesaña, A.; del Suárez Vicente, M.P.; Docampo Ferreira, T.; del Pérez-La Fuente Varela, M.M.; Porto Quintáns, M.M.; Pilat, A. Effect of myofascial induction therapy on post-c-section scars, more than one and a half years old. Pilot study. J. Bodyw. Mov. Ther. 2017, 21, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Ozsoy, G.; Ilcin, N.; Ozsoy, I.; Gurpinar, B.; Buyukturan, O.; Buyukturan, B.; Kararti, C.; Sas, S. The Effects Of Myofascial Release Technique Combined with Core Stabilization Exercise in Elderly with Non-Specific Low Back Pain: A Randomized Controlled, Single-Blind Study. Clin. Interv. Aging 2019, 14, 1729–1740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceca, D.; Elvira, L.; Guzmán, J.F.; Pablos, A. Benefits of a self-myofascial release program on health-related quality of life in people with fibromyalgia: A randomized controlled trial. J. Sports Med. Phys. Fit. 2017, 57, 993–1002. [Google Scholar]
- Urrútia, G.; Bonfill, X. Declaración Prisma: Una propuesta para mejorar la publicación de revisiones sistemáticas y metaanálisis. Med. Clin. 2010, 135, 507–511. [Google Scholar] [CrossRef]
- Da Costa Santos, C.M.; de Mattos Pimenta, C.A.; Nobre, M.R. The PICO strategy for the research question construction and evidence search. Rev. Lat. Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Lao, C.; Cantarero-Villanueva, I.; Díaz-Rodríguez, L.; Fernández-de-las-Peñas, C.; Sánchez-Salado, C.; Arroyo-Morales, M. The Influence of Patient Attitude Toward Massage on Pressure Pain Sensitivity and Immune System after Application of Myofascial Release in Breast Cancer Survivors: A Randomized, Controlled Crossover Study. J. Manip. Physiol. Ther. 2012, 35, 94–100. [Google Scholar] [CrossRef]
- Fernández-Lao, C.; Cantarero-Villanueva, I.; Díaz-Rodríguez, L.; Cuesta-Vargas, A.; Fernández-Delas-Peñas, C.; Arroyo-Morales, M. Attitudes towards massage modify effects of manual therapy in breast cancer survivors: A randomised clinical trial with crossover design. Eur. J. Cancer Care 2011, 21, 233–241. [Google Scholar] [CrossRef] [PubMed]
- De Groef, A.; Van Kampen, M.; Vervloesem, N.; De Geyter, S.; Christiaens, M.; Neven, P.; Vos, L.; de Vrieze, T.; Geraerts, I.; Devoogdt, N. Myofascial techniques have no additional beneficial effects to a standard physical therapy programme for upper limb pain after breast cancer surgery: A randomized controlled trial. Clin. Rehabil. 2017, 31, 1625–1635. [Google Scholar] [CrossRef]
- Castro-Martín, E.; Ortiz-Comino, L.; Gallart-Aragón, T.; Esteban-Moreno, B.; Arroyo-Morales, M.; Galiano-Castillo, N. Myofascial Induction Effects on Neck-Shoulder Pain in Breast Cancer Survivors: Randomized, Single-Blind, Placebo-Controlled Crossover Design. Arch. Phys. Med. Rehabil. 2017, 98, 832–840. [Google Scholar] [CrossRef]
- Serra-Añó, P.; Inglés, M.; Bou-Catalá, C.; Iraola-Lliso, A.; Espí-López, G. Effectiveness of myofascial release after breast cancer surgery in women undergoing conservative surgery and radiotherapy: A randomized controlled trial. Support. Care Cancer 2018, 27, 2633–2641. [Google Scholar] [CrossRef]
- De Groef, A.; Van Kampen, M.; Verlvoesem, N.; Dieltjens, E.; Vos, L.; De Vrieze, T.; Christiaens, M.-R.; Neven, P.; Geraerts, I.; Devoogdt, N. Effect of myofascial techniques for treatment of upper limb dysfunctions in breast cancer survivors: Randomized controlled trial. Support. Care Cancer 2017, 25, 2119–2127. [Google Scholar] [CrossRef]
- De Groef, A.; Van Kampen, M.; Vervloesem, N.; Dieltjens, E.; Christiaens, M.; Neven, P.; Vos, L.; de Vrieze, T.; Geraerts, I.; Devoogdt, N. Effect of myofascial techniques for treatment of persistent arm pain after breast cancer treatment: Randomized controlled trial. Clin. Rehabil. 2017, 32, 451–461. [Google Scholar] [CrossRef]
- Massingill, J.; Jorgensen, C.; Dolata, J.; Sehgal, A. Myofascial Massage for Chronic Pain and Decreased Upper Extremity Mobility After Breast Cancer Surgery. Int. J. Ther. Massag. Bodyw. Res. Educ. Pract. 2018, 11, 4–9. [Google Scholar]
- Webb, T.R.; Rajendran, D. Myofascial techniques: What are their effects on joint range of motion and pain? A systematic review and meta-analysis of randomised controlled trials. J. Bodyw. Mov. Ther. 2016, 20, 682–699. [Google Scholar] [CrossRef] [PubMed]
- Burk, C.; Perry, J.; Lis, S.; Dischiavi, S.; Bleakley, C. Can Myofascial Interventions have a remote effect on ROM? A systematic Review and Meta-analysis. J. Sport Rehabil. 2020, 29, 650–656. [Google Scholar] [PubMed]
- Pinheiro Da Silva, F.; Moreira, G.M.; Zomkowski, K.; Amaral de Noronha, M.; Flores Sperandio, F. Manual therapy as treatment for chronic musculoskeletal pain in female breast cancer survivors: A systematic review and meta-analysis. J. Manip. Physiol. Ther. 2019, 42, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Deng, G. Integrative Medicine Therapies for Pain Management in Cancer Patients. Cancer J. 2019, 25, 343–348. [Google Scholar] [CrossRef]
- Pilat, A. Myofascial Therapies: Myofascial Induction; McGraw-Hill Interamericana: Madrid, Spain, 2003. [Google Scholar]
- Bjerkeset, E.; Rhrl, K.; Schou-Bredal, I. Symptom cluster of pain, fatigue, and psychological distress in breast cancer survivors: Prevalence and characteristics. Breast Cancer Res. Treat. 2020, 180, 63–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year | Sample and Average Age | Diagnosis | Type of Surgical Intervention | Type of Intervention | Sessions and Length of Time | Outcome Measures | Follow-Up | Results |
|---|---|---|---|---|---|---|---|---|
| Fernández-Lao et al. (2012) [40] * | N = 20 EG = 10 CG = 10 49 ± 8 | Breast cancer (I–IIIA), with moderate/high fatigue (>6 points). | 70% of the women had received a lumpectomy and 30% a mastectomy. Adjuvant radiation therapy or chemotherapy. | EG: A protocol of myofascial induction focused on the neck–shoulder area using the Barnes approach. CG: Educational session on healthy lifestyles. | 2 sessions 40′/session 3 weeks | PPT: algometer (kg/cm2) ATOM (0–45) Function of the sympathetic and immune system: saliva samples | 3 weeks | Increased salivary flow (p = 0.010) after intervention with myofascial therapy. In addition, positive attitude had a significant increase in IgA (p < 0.05) in the experimental group. There were no effects for PPT on the cervical spine or temporalis muscle. |
| Fernández-Lao et al. (2011) [41] * | N = 20 EG = 10 CG = 10 49 ± 8 | Breast cancer (stage I–IIIA) and with moderate/high fatigue (>6 points). | 70% of the women had received a lumpectomy and 30% a mastectomy. Adjuvant radiation therapy or chemotherapy. | EG: A protocol of myofascial induction focused on the neck–shoulder area using the Barnes approach. CG: Advice for improving quality of life after breast cancer. | 2 sessions 40′/session 2 weeks | HR variability: Holter ATOM (0–45) POMS | 2 weeks | Increased HR after myofascial induction (p < 0.05) Improvement in perceived fatigue and general mood by POMS after myofascial induction (p < 0.05. Improved anxiety, depression and anger in patients with a better attitude towards massage after myofascial therapy (p < 0.05). |
| Groef et al. (2017) [42] | N = 147 EG = 72 CG = 75 EG: 53.9 ± 11.5 CG: 54.7 ± 11.9 | Patients with unilateral axillary clearance for primary breast cancer after surgery. | Between 60–70% received a mastectomy and between 30–40% breast conservation. Adjuvant radiation therapy or chemotherapy. | EG: Standard physical therapy program and myofascial induction (in active trigger points of the affected limb and in adhesions of the pectoral, axillary and cervical region, diaphragm and scar). CG: Standard physical therapy intervention and placebo intervention (static hand placement on the upper body and arm). | 8 sessions 30′/session 8 weeks | VAS (0–100) DASH (0–100) SF-36 (0–100) PPT: algometer (kg/cm2) McGill Pain Questionnaire | 8 weeks 9 and 12 months | The PPT in the upper trapezius (p = 0.012) was significantly higher at 4 months in the intervention group, and at 4 and 9 months in supraspinatus (p = 0.021) and (p = 0.040), respectively. |
| Castro-Martín et al. (2016) [43] | N = 21 EG = 11 CG = 10 25–65 | Breast cancer in stage I–IIIA. | The types of surgery were: lumpectomy, quadrantectomy, unilateral mastectomy, mastectomy and lymphadenectomy. All patients had received radiotherapy and chemotherapy. | EG: Myofascial induction in the upper limb area, following the Pilat approach. CG: Simulated pulsed short wave (disconnected) | 2 sessions 30′/session 4 weeks | VAS (0–100) Shoulder mobility: Goniometer POMS ATOM Scale (0–45) | 4 weeks | The VAS improved after myofascial induction in the affected arm (p = 0.031), as well as flexion, abduction and external and internal rotations of the affected arm (p < 0.05), and cervical rotation and inclination towards the affected side (p < 0.05). After myofascial induction there were also improvements in mood, anxiety, depression, anger, vigor, fatigue and confusion (p < 0.05). There were no significant changes on the ATOMS scale. |
| Serra-añó et al. (2018) [44] | N = 24 EG = 13 CG = 11 EG: 53.15 ± 10.91 CG: 54.36 ± 6.86 | Breast cancer with conservative treatment/surgery at least 4 months before, without lymphedema or in stage I. | Conservative/partial surgery with or without stage I lymphedema. | EG: Myofascial induction through four maneuvers. CG: Placebo manual lymphatic drainage | 4 sessions 50′/session 4 weeks | VAS (0–100) Shoulder mobility range. DASH (0–100) PHQ-9 (0–100) FACT-B + 4 | 4 weeks 1 month | Only the participants who received myofascial induction had improved pain intensity, range of motion in flexion, extension, abduction and external rotation of the shoulder (p < 0.05), and physical well-being and the general scale of quality of life (p < 0.05). |
| Groef et al. (2017) [45] | N = 50 EG = 23 CG = 25 EG: 55.3 ± 7.5 CG: 53.1 ± 7.5 | Unilateral breast cancer with pain (VAS > 4 points) and myofascial dysfunctions in the upper limb area. | Between 60–70% received a mastectomy and between 30–40% breast conservation. | EG: Standard physical therapy program and myofascial induction CG: Standard physical therapy intervention and placebo intervention | 20 sessions 60′/session 12 weeks | Shoulder mobility range. Presence of lymphedema Force Dynamics and scapular position: dynamometry. Acromion-table index. Inclinometer. DASH (0–100) SF-36 | 3 months 12 months | After the intervention, the pain intensity significantly decreased for participants in the experimental group (p < 0.046). In the SF-36, mental function improved after myofascial induction (p < 0.05). |
| Groef et al. (2017) [46] | N = 50 EG = 23 CG = 25 EG: 55.36 ± 7.5 CG: 53.1 ± 7.5 | Unilateral breast cancer with pain (VAS > 4 points) and myofascial dysfunctions in the upper limb area. | Between 60–70% received a mastectomy and between 30–40% breast conservation. | EG: Standard physical therapy program and myofascial induction CG: Standard physical therapy intervention and placebo intervention | 20 sessions 60′/session 12 weeks | VAS (0–100) McGill PPT: algometer (kg/cm2) Shoulder functionality: DASH (0–100) SF-36 (0–100) | 3 months 6 and 12 months | Increase in the external scale of the scapula in the experimental group (p < 0.05) and improvement in physical function related to quality of life (p = 0.018). |
| Massingill et al. (2018) [47] | N = 21 EG = 11 CG = 10 EG/CG: 21 − 55 + | Breast cancer patients who have persistent pain and mobility limitations after breast cancer surgery. | The types of breast cancer surgery included biopsy, lumpectomy, mastectomy or certain types of reconstruction. | EG: Myofascial massage CG: Relaxing massage | Two 30-min sessions a week for 8 weeks | Pain (0–30, with 0 being nothing and 30 being the maximum) Mobility (0–40) Quality of life (0–100) | 8 weeks. | The EG experienced more favorable changes in pain than the CG (−10.7 vs. +0.4, p < 0.001), mobility (−14.5 vs. −0.8, p < 0.001) and overall health (+29.5 vs. −2.5, p = 0.002) after 8 weeks |
| Author/Year | N Therapeutic Group | Type | Time Per Session | Number of Sessions | Length of Intervention | Observations |
|---|---|---|---|---|---|---|
| Fernández-Lao et al. (2012) [40] * | 10 | Myofascial release: the patients received a myofascial release protocol which focused on the neck and shoulder area following the Barnes approach. The protocol included longitudinal strokes, J-strokes, sustained suboccipital pressure, frontal bone decompression and the ear traction technique. | 40 min (length adapted to the tissue response of the patient) | 2 sessions separated by a 3-week interval | 5 weeks | N/A |
| Fernández-Lao et al. (2011) [41] * | 10 | Myofascial release: protocol which focused on the neck and shoulder area using the Barnes approach. The protocol included longitudinal strokes, J-strokes, sustained suboccipital pressure, frontal bone decompression and the ear traction technique. | 40 min (length adapted to the tissue response of the patient) | 2 sessions separated by 2 weeks | 4 weeks | 80% of the patients underwent surgery at least 12 months before the intervention. |
| Groef et al. (2017) [42] | 72 | Standard physical therapy program (shoulder mobilizations, pectoral stretching and relaxation, scar massage, shoulder exercise schemes) + Myofascial therapy consisting of manual myofascial release techniques on (1) active myofascial trigger points in the upper limb area and (2) myofascial adhesions in the pectoral, axillary and cervical regions, diaphragm and scars. | Physical therapy program: 30 min Myofascial release: 30 min | 2 sessions a week | 8 weeks | The patients were asked to perform exercises twice a day at home. Myofascial interventions were performed from 2 to 4 months after surgery. |
| Castro-Martín et al. (2016) [43] | 21 | The patients received a fascial relaxation intervention which focused on the upper limb area, using the Pilat approach. | 30 min (length adapted to the tissue response of the patient) | 2 sessions separated by a 4-week interval | 4 weeks | 60% of patients received myofascial intervention in less than 12 months after surgery. |
| Serra-Añó et al. (2018) [44] | 13 | The applied treatment was based on the Pilat technique. Four maneuvers were selected for the perinodal and upper thoracic region. They were applied in the following order: sterno-pectoral, global pectoral, pectoral and subscapular. | 50 min | 1 session a week | 4 weeks | The intervention was carried out at least 4 months after surgery. |
| Groef et al. (2017) [45,46] | 25 (2) | Standard physical therapy program (shoulder mobilizations, pectoral stretching and relaxation, scar massage, shoulder exercise schemes) + Myofascial release in (1) active trigger points of the upper limbs and in (2) myofascial adhesions of the pectoralis, axillary and cervical regions, diaphragm and scars. | Physical therapy program: 30 min Myofascial release: 30 min | 2 sessions a week (week 1–8) 1 session a week (week 9–12) | 12 weeks | The intervention was at least 3 months after radiation therapy and 3 years after surgery. |
| Massingill et al. (2018) [47] | 10 | The participants of the intervention received myofascial massage specifically for the chest, thorax and shoulder on the affected side. The massages of the intervention included the following techniques: skin gliding (variable length of time), J-stroke (2–3 min), vertical strokes (2–3 min), strumming (2–3 min), fascial stretching (3–5 min), circular friction (1 to 2 min), deep fascial release (3–5 min), arm pull (60 s on each arm), lateral latissimus dorsi stretch (3 to 5 min) and twisting (3 min). | 30 min | 2 sessions a week | 8 weeks | The intervention began between 3 and 18 months after surgery. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lara-Palomo, I.C.; Castro-Sánchez, A.M.; Córdoba-Peláez, M.M.; Albornoz-Cabello, M.; Ortiz-Comino, L. Effect of Myofascial Therapy on Pain and Functionality of the Upper Extremities in Breast Cancer Survivors: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4420. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094420
Lara-Palomo IC, Castro-Sánchez AM, Córdoba-Peláez MM, Albornoz-Cabello M, Ortiz-Comino L. Effect of Myofascial Therapy on Pain and Functionality of the Upper Extremities in Breast Cancer Survivors: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(9):4420. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094420
Chicago/Turabian StyleLara-Palomo, Inmaculada Carmen, Adelaida María Castro-Sánchez, Marta María Córdoba-Peláez, Manuel Albornoz-Cabello, and Lucía Ortiz-Comino. 2021. "Effect of Myofascial Therapy on Pain and Functionality of the Upper Extremities in Breast Cancer Survivors: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 9: 4420. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094420