
Coping and Post-Traumatic Stress in Children and Adolescents after an Acute Onset Disaster: A Systematic Review


Abstract
:1. Introduction
2. Method
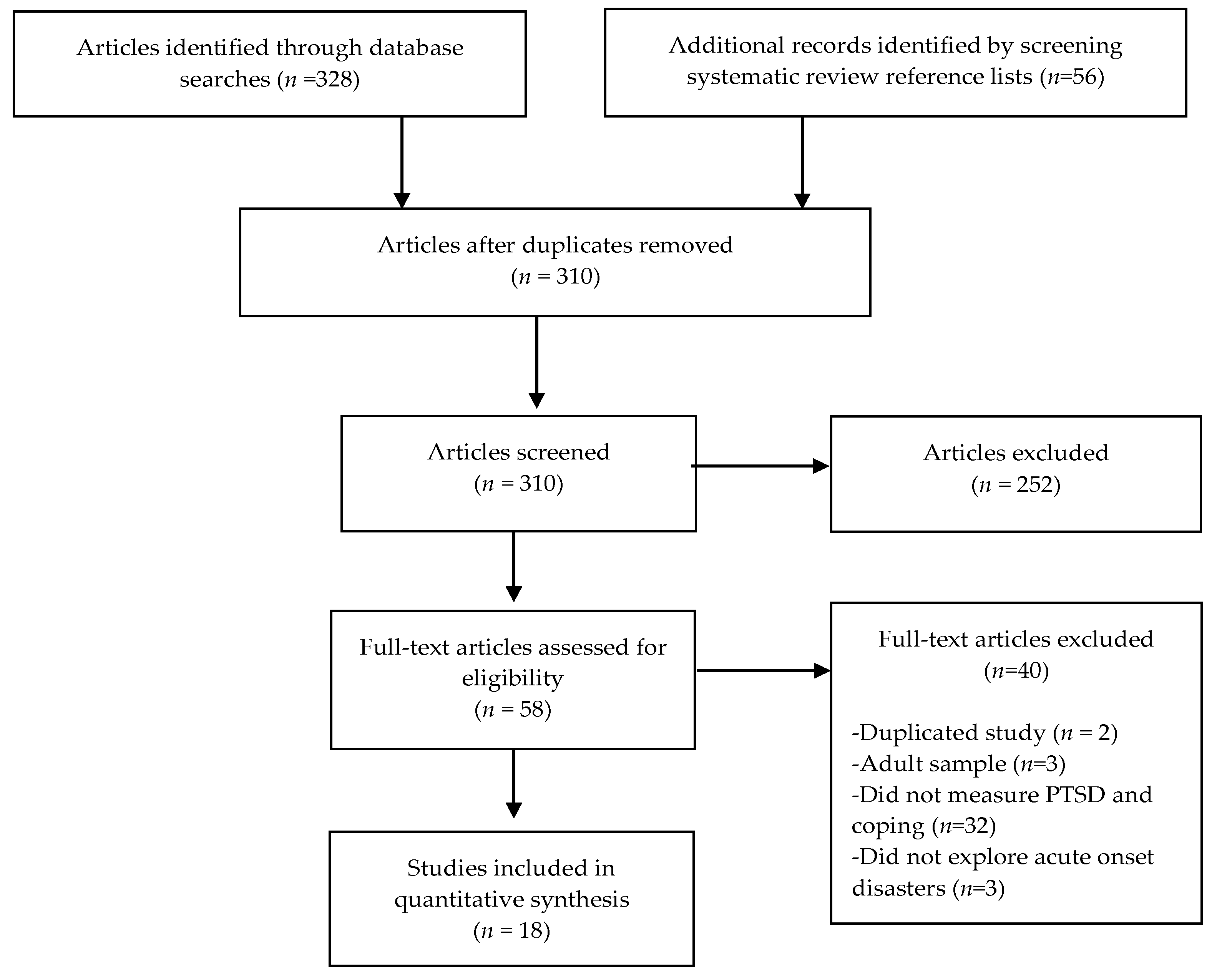
2.1. Search Strategies
2.2. Eligibility Criteria
2.3. Articles Included
2.4. Data Extraction and Quality Appraisal
3. Results
3.1. PTSD Measures
3.2. Coping Measures
3.3. Relationship between Coping Style and PTSD Symptoms
4. Discussion
4.1. Coping Measurement
4.2. Self-Report Measurement
4.3. Coping and PTSD
4.4. Limitations and Directions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garrett, A.L.; Grant, R.; Madrid, P.; Brito, A.; Abramson, D.; Redlener, I. Children and Megadisasters: Lessons Learned in the New Millennium. Adv. Pediatr. 2007, 54, 189–214. [Google Scholar] [CrossRef] [Green Version]
- Ursano, R.J.; Cerise, F.P.; DeMartino, R.; Reissman, D.B.; Shear, M.K. The Impact of Disasters and Their Aftermath on Mental Health. Prim. Care Companion J. Clin. Psychiatry 2006, 8, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.-W.; Chan, C.L.W.; Ho, R.T.H. Prevalence and trajectory of psychopathology among child and adolescent survivors of disasters: A systematic review of epidemiological studies across 1987–2011. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 1697–1720. [Google Scholar] [CrossRef] [PubMed]
- Lock, S.; Rubin, G.J.; Murray, V.; Rogers, M.B.; Amlot, R.; Williams, R. Secondary stressors and extreme events and disasters: A systematic review of primary research from 2010–2011. PLoS Curr. 2012, 4. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.R.; Danielson, C.K.; Adams, Z.W.; Ruggiero, K.J. Distress Tolerance and Social Support in Adolescence: Predicting Risk for Internalizing and Externalizing Symptoms Following a Natural Disaster. J. Psychopathol. Behav. Assess. 2016, 38, 538–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfefferbaum, B.; Jacobs, A.K.; Griffin, N.; Houston, J.B. Children’s Disaster Reactions: The Influence of Exposure and Personal Characteristics. Curr. Psychiatry Rep. 2015, 17, 56. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; Jacobs, A.K.; Van Horn, R.L.; Houston, J.B. Effects of Displacement in Children Exposed to Disasters. Curr. Psychiatry Rep. 2016, 18, 71. [Google Scholar] [CrossRef]
- Becker-Blease, K.A.; Turner, H.A.; Finkelhor, D. Disasters, Victimization, and Children’s Mental Health. Child Dev. 2010, 81, 1040–1052. [Google Scholar] [CrossRef]
- Busso, D.S.; McLaughlin, K.A.; Sheridan, M.A. Media Exposure and Sympathetic Nervous System Reactivity Predict PTSD Symptoms after the Boston Marathon Bombings. Depress. Anxiety 2014, 31, 551–558. [Google Scholar] [CrossRef] [Green Version]
- Sapienza, J.K.; Masten, A.S. Understanding and promoting resilience in children and youth. Curr. Opin. Psychiatry 2011, 24, 267–273. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; Noffsinger, M.A.; Wind, L.H.; Allen, J.R. Children’s Coping in the Context of Disasters and Terrorism. J. Loss Trauma 2014, 19, 78–97. [Google Scholar] [CrossRef]
- Kilmer, R.P.; Gil-Rivas, V. Exploring Posttraumatic Growth in Children Impacted by Hurricane Katrina: Correlates of the Phenomenon and Developmental Considerations. Child Dev. 2010, 81, 1211–1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gil-Rivas, V.; Silver, R.C.; Holman, E.A.; McIntosh, D.N.; Poulin, M. Parental response and adolescent adjustment to the 11 september 2001 terrorist attacks. J. Trauma. Stress 2007, 20, 1063–1068. [Google Scholar] [CrossRef] [Green Version]
- An, Y.; Fu, F.; Wu, X.; Lin, C.; Zhang, Y. Longitudinal Relationships Between Neuroticism, Avoidant Coping, and Posttraumatic Stress Disorder Symptoms in Adolescents Following the 2008 Wenchuan Earthquake in China. J. Loss Trauma 2013, 18, 556–571. [Google Scholar] [CrossRef]
- La Greca, A.M.; Lai, B.S.; Llabre, M.M.; Silverman, W.K.; Vernberg, E.M.; Prinstein, M.J. Children’s Postdisaster Trajectories of PTS Symptoms: Predicting Chronic Distress. Child Youth Care Forum 2013, 42, 351–369. [Google Scholar] [CrossRef] [Green Version]
- Navarro, P.N.; Landin-Romero, R.; Guardiola-Wanden-Berghe, R.; Moreno-Alcázar, A.; Valiente-Gómez, A.; Lupo, W.; García, F.; Fernández, I.; Pérez, V.; Amann, B.L. 25 years of Eye Movement Desensitization and Reprocessing (EMDR): The EMDR therapy protocol, hypotheses of its mechanism of action and a systematic review of its efficacy in the treatment of post-traumatic stress disorder. Rev. Psiquiatr. Salud Ment. (Engl. Ed.) 2018, 11, 101–114. [Google Scholar] [CrossRef]
- Papadatou, D.; Giannopoulou, I.; Bitsakou, P.; Bellali, T.; Talias, M.A.; Tselepi, K. Adolescents’ reactions after a wildfire disaster in Greece. J. Trauma. Stress 2012, 25, 57–63. [Google Scholar] [CrossRef]
- Pina, A.A.; Villalta, I.K.; Ortiz, C.D.; Gottschall, A.C.; Costa, N.M.; Weems, C.F. Social Support, Discrimination, and Coping as Predictors of Posttraumatic Stress Reactions in Youth Survivors of Hurricane Katrina. J. Clin. Child Adolesc. Psychol. 2008, 37, 564–574. [Google Scholar] [CrossRef]
- Grolnick, W.S.; Schonfeld, D.J.; Schreiber, M.; Cohen, J.; Cole, V.; Jaycox, L.; Lochman, J.; Pfefferbaum, B.; Ruggiero, K.; Wells, K.; et al. Improving adjustment and resilience in children following a disaster: Addressing research challenges. Am. Psychol. 2018, 73, 215–229. [Google Scholar] [CrossRef]
- Balaban, V. Psychological Assessment of Children in Disasters and Emergencies. Disasters 2006, 30, 178–198. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; North, C.S. Child Disaster Mental Health Services: A Review of the System of Care, Assessment Approaches, and Evidence Base for Intervention. Curr. Psychiatry Rep. 2016, 18, 5. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Ross, L.E.; Grigoriadis, S.; Mamisashvili, L.; Koren, G.; Steiner, M.; Dennis, C.; Cheung, A.; Mousmanis, P. Quality assessment of observational studies in psychiatry: An example from perinatal psychiatric research. Int. J. Methods Psychiatr. Res. 2011, 20, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Betancourt, T.S.; Borisova, I.; Williams, T.P.; Meyers-Ohki, S.E.; Rubin-Smith, J.E.; Annan, J.; Kohrt, B.A. Research Review: Psychosocial adjustment and mental health in former child soldiers—A systematic review of the literature and recommendations for future research. J. Child Psychol. Psychiatry 2013, 54, 17–36. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Burns, J.K.; Dhingra, M.; Tarver, L.; Kohrt, B.A.; Lund, C. Income inequality and depression: A systematic review and meta-analysis of the association and a scoping review of mechanisms. World Psychiatry 2018, 17, 76–89. [Google Scholar] [CrossRef]
- Keane, L.; Loades, M. Low self-esteem and internalizing disorders in young people—A systematic review. Child Adolesc. Ment. Health 2017, 22, 4–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenhard, W.; Lenhard, A. Berechnung von Effektstärken [Calculation of Effect Sizes]. Dettelbach: Psychometrica. Available online: https://www.psychometrica.de/effektstaerke.html (accessed on 15 February 2020).
- Martin, N.C.; Felton, J.W.; Cole, D.A. Predictors of Youths’ Posttraumatic Stress Symptoms Following a Natural Disaster: The 2010 Nashville, Tennessee, Flood. J. Clin. Child Adolesc. Psychol. 2014, 45, 1–13. [Google Scholar] [CrossRef]
- Fan, F.; Long, K.; Zhou, Y.; Zheng, Y.; Liu, X. Longitudinal trajectories of post-traumatic stress disorder symptoms among adolescents after the Wenchuan earthquake in China. Psychol. Med. 2015, 45, 2885–2896. [Google Scholar] [CrossRef]
- Chen, W.; Wang, L.; Zhang, X.-L.; Shi, J.-N. Understanding the Impact of Trauma Exposure on Posttraumatic Stress Symptomatology: A Structural Equation Modeling Approach. J. Loss Trauma 2012, 17, 98–110. [Google Scholar] [CrossRef]
- Du, B.; Ma, X.; Ou, X.; Jin, Y.; Ren, P.; Li, J. The prevalence of posttraumatic stress in adolescents eight years after the Wenchuan earthquake. Psychiatry Res. 2018, 262, 262–269. [Google Scholar] [CrossRef]
- Xiao, Y.; Liu, N.; Liu, K.; Jiang, X. Post-traumatic stress disorder and its risk factors in bereaved Tibetan adolescents 3 years after the 2010 Yushu earthquake, a cross-sectional study in China. Arch. Psychiatr. Nurs. 2019, 33, 149–154. [Google Scholar] [CrossRef]
- Stratta, P.; Capanna, C.; Dell’Osso, L.; Carmassi, C.; Patriarca, S.; Di Emidio, G.; Riccardi, I.; Collazzoni, A.; Rossi, A. Resilience and coping in trauma spectrum symptoms prediction: A structural equation modeling approach. Pers. Individ. Differ. 2015, 77, 55–61. [Google Scholar] [CrossRef]
- Prinstein, M.J.; La Greca, A.M.; Vernberg, E.M.; Silverman, W.K. Children’s Coping Assistance: How Parents, Teachers, and Friends Help Children Cope After a Natural Disaster. J. Clin. Child Psychol. 1996, 25, 463–475. [Google Scholar] [CrossRef]
- Russoniello, C.V.; Skalko, T.K.; O’Brien, K.; McGhee, S.A.; Bs, D.B.-A.; Ms, J.B. Childhood Posttraumatic Stress Disorder and Efforts to Cope After Hurricane Floyd. Behav. Med. 2002, 28, 61–71. [Google Scholar] [CrossRef]
- Terranova, A.M.; Boxer, P.; Morris, A.S. Factors influencing the course of posttraumatic stress following a natural disaster: Children’s reactions to Hurricane Katrina. J. Appl. Dev. Psychol. 2009, 30, 344–355. [Google Scholar] [CrossRef]
- Lewis, K.M.; Langley, A.K.; Jones, R.T. Impact of Coping Efficacy and Acculturation on Psychopathology in Adolescents Following a Wildfire. J. Child Fam. Stud. 2013, 24, 317–329. [Google Scholar] [CrossRef]
- Lack, C.W.; Sullivan, M.A. Attributions, Coping, and Exposure as Predictors of Long-term Posttraumatic Distress in Tornado-Exposed Children. J. Loss Trauma 2007, 13, 72–84. [Google Scholar] [CrossRef]
- Lengua, L.J.; Long, A.C.; Meltzoff, A.N. Pre-attack stress-load, appraisals, and coping in children’s responses to the 9/11 terrorist attacks. J. Child Psychol. Psychiatry 2006, 47, 1219–1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernando, G.A.; Berger, D.E. The role of religion in youth exposed to disasters in Sri Lanka. J. Prev. Interv. Community 2017, 45, 238–249. [Google Scholar] [CrossRef]
- Xie, F. Reliability and validity of the simplified Coping Style Questionnaire. Chin. J. Clin. Psychol. 1998, 6, 114–115. [Google Scholar]
- Causey, D.L.; Dubow, E.F. Development of a Self-Report Coping Measure for Elementary School Children. J. Clin. Child Psychol. 1992, 21, 47–59. [Google Scholar] [CrossRef]
- Bagby, R.M.; Parker, J.D. Relation of rumination and distraction with neuroticism and extraversion in a sample of patients with major depression. Cogn. Ther. Res. 2001, 25, 91–102. [Google Scholar] [CrossRef]
- Chen, S.; Zheng, Q.; Pan, J.; Zheng, S. Preliminary development of the Coping Style Scale for Middle School Students. Chin. J. Clin. Psychol. 2000, 8, 211–214. [Google Scholar]
- Ayers, T.S.; Sandler, I.N.; West, S.G.; Roosa, M.W. A Dispositional and Situational Assessment of Children’s Coping: Testing Alternative Models of Coping. J. Pers. 1996, 64, 923–958. [Google Scholar] [CrossRef]
- Ayers, T.; Sandler, I.N. The children’s coping strategies checklist and the how I coped under pressure scale. Program for Prevention Research, Arizona State University, Tempe, AZ, USA. Unpublished work. 2000. [Google Scholar]
- Xiao, J.; Xu, X. Study on the validity and reliability of ‘COPE’. Chin. Ment. Health J. 1996, 10, 164–168. [Google Scholar]
- Spirito, A.; Stark, L.J.; Williams, C. Development of a Brief Coping Checklist for Use with Pediatric Populations. J. Pediatr. Psychol. 1988, 13, 555–574. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.-T.; Chan, A.C.M. Factorial Structure of the Kidcope in Hong Kong Adolescents. J. Genet. Psychol. 2003, 164, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Vernberg, E.M.; La Greca, A.M.; Silverman, W.K.; Prinstein, M.J. Prediction of posttraumatic stress symptoms in children after Hurricane Andrew. J. Abnorm. Psychol. 1996, 105, 237. [Google Scholar] [CrossRef]
- Carver, C.S. You want to measure coping but your protocol’too long: Consider the brief cope. Int. J. Behave. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef]
- Sandler, I.N.; Tein, J.Y.; Mehta, P.; Wolchik, S.; Ayers, T. Coping efficacy and psychological problems of children of divorce. Child Dev. 2000, 71, 1099–1118. [Google Scholar] [CrossRef]
- Weyer, M.; Sandler, I.N. Stress and coping as predictors of children’s divorce-related ruminations. J. Clin. Child Psychol. 1998, 27, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Foa, E.B.; Johnson, K.M.; Feeny, N.C.; Treadwell, K.R.H. The Child PTSD Symptom Scale: A Preliminary Examination of its Psychometric Properties. J. Clin. Child Adolesc. Psychol. 2001, 30, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Frederick, C.J. Selected foci in the Spectrum of Posttraumatic Stress Disorders. Available online: https://ci.nii.ac.jp/naid/10025019445/ (accessed on 26 April 2021).
- Blanchard, E.B.; Jones-Alexander, J.; Buckley, T.C.; Forneris, C.A. Psychometric properties of the PTSD checklist (PCL). Behav. Res. Ther. 1996, 34, 669–673. [Google Scholar] [CrossRef]
- Perrin, S.; Meiser-Stedman, R.; Smith, P. The Children’s Revised Impact of Event Scale (CRIES): Validity as a Screening Instrument for PTSD. Behav. Cogn. Psychother. 2005, 33, 487–498. [Google Scholar] [CrossRef] [Green Version]
- Amaya-Jackson, L.; McCarthy, G.; Cherney, M.S.; Newman, E. Child PTSD Checklist; Duke University Medical Center: Durham, UK, 1995. [Google Scholar]
- Steinberg, A.M.; Brymer, M.J.; Decker, K.B.; Pynoos, R.S. The University of California at Los Angeles post-traumatic stress disorder reaction index. Curr. Psychiatry Rep. 2004, 6, 96–100. [Google Scholar] [CrossRef]
- Weiss, D.; Marmar, C. The Impact of Event Scale—Revised. Assessing Psychological Trauma and PTSD: A Handbook for Practitioners; Wilson, J., Keane, T., Eds.; Guildford Press: New York, NY, USA, 1997. [Google Scholar]
- Liu, X.; Ma, D.D.; Liu, L.Q.; Zhao, G.F.; Li, C.Q.; Yang, J.; Shun, L.M. Development of the post-traumatic stress disorder self-rating scale and its reliability and validity. Chin J. Behav Med. Sci. 1998, 7, 93–96. [Google Scholar]
- Dell’Osso, L.; Carmassi, C.; Rucci, P.; Conversano, C.; Shear, M.K.; Calugi, S.; Maser, J.D.; Endicott, J.; Fagiolini, A.; Cassano, G.B. A multidimensional spectrum approach to post-traumatic stress disorder: Comparison between the Structured Clinical Interview for Trauma and Loss Spectrum (SCI-TALS) and the Self-Report instrument (TALS-SR). Compr. Psychiatry 2009, 50, 485–490. [Google Scholar] [CrossRef]
- Cryder, C.H.; Kilmer, R.P.; Tedeschi, R.G.; Calhoun, L.G. An exploratory study of posttraumatic growth in children following a natural disaster. Am. J. Orthopsychiatry 2006, 76, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; Noffsinger, M.A.; Wind, L.H. Issues in the Assessment of Children’s Coping in the Context of Mass Trauma. Prehospital Disaster Med. 2012, 27, 272–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clauss-Ehlers, C.S. Sociocultural factors, resilience, and coping: Support for a culturally sensitive measure of resilience. J. Appl. Dev. Psychol. 2008, 29, 197–212. [Google Scholar] [CrossRef]
- DeLongis, A.; Holtzman, S. Coping in Context: The Role of Stress, Social Support, and Personality in Coping. J. Pers. 2005, 73, 1633–1656. [Google Scholar] [CrossRef] [PubMed]
- Dowdy, E.; Kamphaus, R.W.; Twyford, J.M.; Dever, B.V. Culturally competent behavioral and emotional screening. In Handbook of School Mental Health; Springer: Berlin/Heidelberg, Germany, 2014; pp. 311–321. [Google Scholar]
- Moore, S.A.; Widales-Benitez, O.; Carnazzo, K.W.; Kim, E.K.; Moffa, K.; Dowdy, E. Conducting Universal Complete Mental Health Screening via Student Self-Report. Contemp. Sch. Psychol. 2015, 19, 253–267. [Google Scholar] [CrossRef]
- Craig, S.L.; Austin, A.; Huang, Y.-T. Being humorous and seeking diversion: Promoting healthy coping skills among LGBTQ+ youth. J. Gay Lesbian Ment. Health 2018, 22, 20–35. [Google Scholar] [CrossRef]
- Krägeloh, C.U. A Systematic Review of Studies Using the Brief COPE: Religious Coping in Factor Analyses. Religions 2011, 2, 216–246. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, K.E. Understanding and Assessing Traumatic Responses of Guilt, Shame, and Anger among Children, Adolescents, and Young Adults. J. Child Adolesc. Trauma 2011, 4, 339–360. [Google Scholar] [CrossRef]
- Xu, J.; He, Y. Psychological health and coping strategy among survivors in the year following the 2008 Wenchuan earthquake. Psychiatry Clin. Neurosci. 2012, 66, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Moscardino, U.; Scrimin, S.; Capello, F.; Altoè, G. Brief report: Self-blame and PTSD symptoms in adolescents exposed to terrorism: Is school connectedness a mediator? J. Adolesc. 2014, 37, 47–52. [Google Scholar] [CrossRef]
- Makwana, N. Disaster and its impact on mental health: A narrative review. J. Fam. Med. Prim. Care 2019, 8, 3090–3095. [Google Scholar] [CrossRef]
- Compas, B.E.; Epping, J.E. Stress and coping in children and families. In Children and Disasters; Springer: Berlin/Heidelberg, Germany, 1993; pp. 11–28. [Google Scholar]
- Woolley, M.E.; Bowen, G.L.; Bowen, N.K. The Development and Evaluation of Procedures to Assess Child Self-Report Item Validity Educational and Psychological Measurement. Educ. Psychol. Meas. 2006, 66, 687–700. [Google Scholar] [CrossRef] [Green Version]
- Benight, C.C.; Bandura, A. Social cognitive theory of posttraumatic recovery: The role of perceived self-efficacy. Behav. Res. Ther. 2004, 42, 1129–1148. [Google Scholar] [CrossRef]
- Gallagher, M.W.; Long, L.J.; Phillips, C.A. Hope, optimism, self-efficacy, and posttraumatic stress disorder: A meta-analytic review of the protective effects of positive expectancies. J. Clin. Psychol. 2019, 76, 329–355. [Google Scholar] [CrossRef] [PubMed]
- Woodward, E.C.; Viana, A.G.; Trent, E.S.; Raines, E.M.; Zvolensky, M.J.; Storch, E.A. Emotional Nonacceptance, Distraction Coping and PTSD Symptoms in a Trauma-Exposed Adolescent Inpatient Sample. Cogn. Ther. Res. 2019, 44, 412–419. [Google Scholar] [CrossRef]
- Moulds, M.L.; Bisby, M.A.; Wild, J.; Bryant, R.A. Rumination in posttraumatic stress disorder: A systematic review. Clin. Psychol. Rev. 2020, 82, 101910. [Google Scholar] [CrossRef] [PubMed]
- Topper, M.; Emmelkamp, P.M.; Watkins, E.; Ehring, T. Prevention of anxiety disorders and depression by targeting excessive worry and rumination in adolescents and young adults: A randomized controlled trial. Behav. Res. Ther. 2017, 90, 123–136. [Google Scholar] [CrossRef]
- Watkins, E.R.; Roberts, H. Reflecting on rumination: Consequences, causes, mechanisms and treatment of rumination. Behav. Res. Ther. 2020, 127, 103573. [Google Scholar] [CrossRef] [PubMed]
- Masten, A.S.; Osofsky, J.D. Disasters and Their Impact on Child Development: Introduction to the Special Section. Child. Dev. 2010, 81, 1029–1039. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Event 1 | Time Frame | Age/ Grade | n | Race/ Ethnicity | Country | PTSD Measure | Coping Measure | Exposure Measure | Summary of PTSD and Coping Styles 2 | QS 3 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Natural Disaster | |||||||||||
| Martin, Felton & Cole [28] | F | Longitudinal 6-months pre flood 10-days post flood | 10–15 years old | 127 | 87% White 5% Latinx 3% Black 0.5% Asian American 6% Multiracial/ other | United States | The Child PTSD Symptom Scale (CPSS) | Rumination Response Scale (RRS) | Flood events questionnaire | Rumination (+) | Moderate |
| An, Fu, Wu, Lin, & Zhang [14] | EQ | Longitudinal 1-year, 1.5-years, 2-years post-EQ | 13–16 years old | 636 | 52% Quiang 26% Tibetan 18% Han 6% other | China | Child PTSD Symptom Scale (CPSS) | Coping Style Scale | N/A | Avoidant (+) | Moderate |
| Fan, Long, Zhou, Zheng, & Liu, [29] | EQ | Longitudinal 6, 12, 18, 24-months post-EQ | 7th and 10th grade | 1573 | No ethnicity information included | China | Posttraumatic Stress Disorder Self-Rating Scale (PTSD-SS), | Simplified Coping Style Questionnaire (SCSQ) | 4-item earthquake exposure measure | Negative (+) Positive (-) | Moderate |
| Chen, Wang, Zhang & Shi [30] | EQ | Cross-sectional 6-months post-EQ | 4–8th grade | 156 | No ethnicity information included | China | Children’s Revised Impact of Event Scale (CRIES-13) | Coping Strategy Scale | 7-item earthquake exposure measure | Emotion-focused (+) | Moderate |
| Du, Ma, Ou, Ye, Ren, & Li [31] | EQ | Cross-sectional 8-years post EQ | 14–20 years | 4118 | 99% Han 1% other | China | PTSD Checklist-Civilian Version (PCL-C) | Simplified Coping Style Questionnaire (SCSQ) | 4-item earthquake exposure measure | Negative (+) Positive (-) | Moderate |
| Xiao, Liu, Liu, Jiang [32] | EQ | Cross-sectional 3-years post-EQ | 11–18 years old | 867 | 100% Tibetan | China | PTSD Checklist–Civilian Version. (PCL-C) | Coping Styles Scale | 13-item earthquake exposure measure | Negative (+) | Moderate |
| Stratta et al. [33] | EQ | Cross-sectional 2-years post-EQ | 17–18 years old | 371 | Not specified | Italy | Trauma and Loss Spectrum (TALS) Self Report | Brief Cope | N/A | Self-distraction (+) Venting (+) Denial (+) Behavioral Disengagement (+) Humor (-) Emotional support (+) | Fair |
| La Greca, Lai, Llabre, Silverman, Vernberg, & Prinstein [15] | H | Longitudinal 3, 7, 10-months post hurricane | 3–5th grade | 568 | 44% White 26% Latinx 22% Black 8% other | United States | PTSD Reaction Index for Children (PTSD-RI) | Kidcope 15-items | Life Events Schedule | Blame and anger (+) | Moderate |
| Prinstein, La Greca, Vernberg, Silverman [34] | H | Cross-sectional 7-months post hurricane | 3–5th grade | 506 | 47% White 27% Latinx 23% Black 3% Asian American | United States | PTSD Reaction Index for Children (PTSD-RI) | -Children’s Coping Assistance Checklist -KidCope 15-items | N/A | Emotional processing (+) Distraction coping assistance (+) | Moderate |
| Pina, Villalta, Ortiz, Gottschall, Costa and Weems [18] | H | Longitudinal 12-months pre-hurricane 6-7 months post hurricane | 7–16 years old | 46 | 67% White 33% Black | United States | The Child PTSD Checklist | Children’s Coping Strategies Checklist | 13-item hurricane related experiences measure | Avoidant (+) | Fair |
| Kilmer, & Gil-Rivas [12] | H | Longitudinal 1- and 2-years post hurricane | 7–10 years old | 51 | 77% Black 15% White 8% other | United States | UCLA PTSD Reaction Index | -Coping Competency Beliefs -Rumination Scale for children | Hurricane-Related Exposure scale | Intrusive and deliberate rumination (+) | Moderate |
| Russoniello et al. [35] | H | Cross-sectional 6-months post hurricane | 4th grade | 150 | 63% Black 33% White 4% Latinx | United States | PTSD Reaction Index for Children (PTSD-RI) | Kidcope 15-items | 1-item Assessing home flooding | Social withdrawal (+) Self-criticism (+) Blaming others (+) Problem solving (+) | Fair |
| Terranova [36] | H | Longitudinal 1–1.5 months and 2–8 months post hurricane | 6th grade | 175 | 61% White 18% Black 17% Multiple ethnicity 4% Native American/ Latinx | United States | The Child PTSD Checklist | -Self-Report Coping Measure (SRCM) -How I Coped Under Pressure Scale (HICUPS) | 6-item hurricane exposure measure | Negative (+) | Moderate |
| Papadatou GiannopoulouBitsakou, Bellali, Talias, & Tselepi [17] | WF | Cross-sectional 6 months post wildfire | 12–17 years | 1468 | 93% Greek 6% immigrant | Greece | Children’s Revised Impact of Event Scale (CRIES) | Kidcope 11-items | Wildfire Experience Questionnaire | Escape- oriented (+) | High |
| Lewis Langley & Jones [37] | WF | Longitudinal 3- and 10-months post WF | 14–16 years old | 206 | 68% White 32% Black | United States | PTSD Reaction Index for Adolescents (PTSD-RI) | Child Coping Efficacy Scale | Fire-Related Traumatic Experiences | Coping efficacy (-) | Moderate |
| Lack & Sullivan [38] | T | Cross sectional 13-months post tornado | 3–6th grade | 102 | 90.9% White 5.5% Native American | United States | PTSD Reaction Index (PTSD-RI) | Kid Cope 15-item | Tornado exposure questionnaire | Number of coping strategies (+) | Fair |
| Manmade Disaster | |||||||||||
| Lengua, Long, & Meltzoff, [39] | TA | Longitudinal 2–9 weeks post-9/11 terrorist attack; 6-months before 9/11 terrorist attack | 9–13 years old | 143 | 66% White 19% Black 6% Multiple ethnicity 4% Latinx 3% Asian American 2% Native American | United States | Child PTSD Symptom Scale (CPSS) | Children’s Coping Strategies Checklist | 2-items assessing direct and indirect exposure to terrorist attacks | Avoidant (+) | High |
| Multiple Disasters | |||||||||||
| Fernando & Berger [40] | TS | Cross-sectional (timeframe post TS not reported) | 6–13th grade | 669 | 77% Sri Lankan 23% Tamil 48% Buddhist 28% Muslim 15% Hindu 8% Christian | Sri Lanka | Child Post-traumatic Stress Scale (CPSS) | Kidcope Religious Coping Index | War- and Tsunami-Related Stressor Scale | Avoidant (+) | Moderate |
| Coping Scale | Validated Populations | Response Style | Author | Positive, Active, Approach Coping Mechanisms (Internal Consistency) | Negative, Passive, Avoidant, Emotion-Focused (Internal Consistency) | Association between Coping and PTSD (Effect Size) |
|---|---|---|---|---|---|---|
| Simplified Coping Style Questionnaire | Chinese university students: normative population [41] | Self-report | Fan et al. [29] | Positive ɑ = 0.76 | Negative ɑ = 0.65 | Odds of PTSD at any wave (Fan et al.): -Medium vs. low negative coping: OR = 1.89 -High vs. low negative coping: OR = 1.73 -High vs. low positive coping: OR = 0.63 |
| Du et al. [31] | Active ɑ = 0.80 | Passive ɑ = 0.73 | N/A | |||
| Self-report coping measure | United States 4-6th grade students: normative population [42] | Self-report | Terranova [36] | N/A | Negative -Internalized (inwardly managing emotional stress reactions) ɑ = 0.78 -Externalized (venting negative emotions) ɑ = 0.74 | Negative coping Time 1: r = 0.47 Time 2: r = 0.29 |
| Rumination Response Scale (RRS) | United States adults with depressive disorders [43] | Self-report | Martin Felton and Cole [28] | N/A | Rumination Wave 1 ɑ = 0.81 Wave 2 ɑ = 0.91 | Rumination: Wave 2 r = 0.35 |
| Rumination Scale for Children | Psychometric testing not conducted | Self-report | Kilmer and Gil-Rivas [12] | N/A | Rumination deliberate rumination ɑ = 0.65 Intrusive rumination ɑ = 0.33 | Rumination: r = 0.28 |
| Coping Strategy Scale | Chinese middle school children and adolescents: normative population [44] | Self-report | Chen, Wang Zhang, & Shi [30] | Problem Focused (problem solving, social support, positive cognitive restructuring) ɑ = 0.85 | Emotion Focused (forbearance, escape, emotional expression, wishful thinking) ɑ = 0.80 | Intrusion Problem Focused -Problem-solving: r = 0.09 -Social support: r = 0.01 -Positive cognitive restructuring: r = 0.04 Emotion Focused -Forbearance: r = 0.32 -Escape: r = 0.23 -Emotional expression: r = 0.23 -Wishful thinking: r = 0.22 Avoidance Problem-Focused -Problem-solving: r = 0.20 -Social support: r = 0.04 -Positive cognitive restructuring: r = 0.06 Emotion-Focused -Forbearance: r = 0.16 -Escape: r = 0.04 -Emotional expression: r = 0.01 -Wishful thinking: r = 0.08 |
| Children’s Coping Strategies Checklist | United States 4-6th grade children: normative population [45] | Researcher administered interview | Lengua, Long, & Meltzof [39] | Active (assessing cognitive decision making, control, direct problem solving, positive cognitive restructuring, optimism, seeking understanding) ɑ = 0.90 | Avoidant (assessing cognitive avoidance, avoidant actions) ɑ = 0.82 | Active: r = 0.10 Avoidant: r = 0.26 |
| Pina et al. [18] | ɑ = 0.87 | ɑ = 0.68 | Active: r = 0.55 Avoidant: r = 0.58 | |||
| How I coped under pressure | United States 9–13 year-old children and adolescents: normative population [46] | Self-report | Terranova [36] | N/A | Negative (avoiding situations where stressor may occur) ɑ = 0.79 | Negative coping: r = 0.47 |
| Coping Style Scale | Chinese middle school students [47] | Self-report | Xiao, Liu, Liu, Jian [32] | Positive (problem solving, resorting) total α = 0.88 combined positive and negative | Negative (withdrawal, abreacting, imagining, tolerating) total α = 0.88 combined positive and negative | Positive coping: OR = 0.63 Negative coping: OR = 2.85 |
| An et al. [14] | N/A | Avoidant (not specified) Time 1 α = 0.77 Time 2 α = 0.83 Time 3 α = 0.85 | Avoidant Time 1: r = 0.24 Time 2: r = 0.24 Time 3: r = 0.28 | |||
| Kidcope 10-items | United States 10–18-year-old children and adolescents Setting: normative population and chronic illness [48] | Self-report | Fernando and Berger [40] | Approach (problem-solving and positive cognitive restructuring) α = not reported | Avoidant (distraction, blaming, wishful thinking, and resignation) α = not reported | Approach: r = 0.11 Avoidant: r = 0.16 |
| Kidcope 11-items | Hong Kong Adolescents normative sample [49] Greek Adolescents wildfire affected sample [17] | Self-report | Papadatou et al. [17] | Control Oriented (cognitive restructuring, problem solving, social support, emotional relaxation) ɑ = 0.64 | Escape Oriented (distraction, social withdrawal, self-criticism, blaming others, resignation, emotional outbursts) ɑ = 0.64 | Control-oriented: Incident risk ratio (IRR) = 1.09 Escape-oriented: IRR = 1.14 |
| Kidcope 15-items | United States 3rd–5th grade hurricane affected children [50] | Self-report | La Greca et al. [15] | N/A | Blame and Anger (blame self, blame others, yell, scream, get mad) ɑ = not reported | Odds of blame and anger coping with membership in: -Recovering trajectory of PTSD vs. resilient trajectory: OR = 5.77 -Chronic trajectory of PTSD vs. resilient trajectory: OR = 7.79 -Chronic PTSD trajectory vs. recovering trajectory: OR = 1.35 |
| Prinstein et al. [34] | Positive (problem solving, distraction, cognitive restructuring, social support, adaptive emotional regulation) ɑ = 0.77 Distraction ɑ = not reported | Resignation ɑ = not reported | N/A | |||
| Russionello et al. [35] | Not designated-used individual items ɑ = 0.09–0.41 | Distraction r = 0.02 Social Withdrawal r = 0.25 Cognitive Restructuring r = 0.07 Self-criticism r = 0.26 Blaming others r = 0.20 Problem solving r = 0.24 Emotional Regulation r = 0.40 Wishful Thinking r = −0.01 Social Support r = 0.04 Resignation r = 0.12 | ||||
| Lack & Sullivan [38] | Combined all coping items into one composite measure ɑ = not reported | Total score r = 0.44 | ||||
| Children’s Coping Assistance Checklist | United States 3-5th grade after hurricane Andrew [34] | Self-report | Prinstein et al, [34] | Roles and Routines α = 0.78 | Emotional processing ɑ = 0.74 Distraction α = 0.84 | Emotional processing: d = 0.49 Roles and routines: d = −0.40 Distraction: d = 0.78 |
| Brief Cope | United States adults after hurricane Andrew [51] | Self-Report | Stratta et al. [33] | Positive (planning, positive reframing, active, acceptance) α = N/A | Emotional (venting, self-blame, instrumental, support, emotional support) α = N/A Disengagement (humor, substance abuse, behavioral disengagement, denial, religion) α = N/A | Re-experiencing Emotional: Venting r = 0.30; Instrumental support r = 0.15; Use of emotional support = 0.22 Disengagement: Denial r = 0.31; Religion r = 0.07; Behavioral disengagement = r = 0.14 Positive: Humor = −0.09 Not categorized: Self-distraction r = 0.21 Avoidance Emotional: Venting r = 0.29 Disengagement: Denial r = 0.26; Use of emotional support r = 0.12 Not categorized Self-distraction r = 0.17 Arousal Emotional: Use of emotional support r = 0.12 Disengagement: Venting r = 0.31; Denial r = 0.26 Not categorized: Self-distraction r = 0.23 |
| Child Coping Efficacy | United States 9-12 year-old children who experienced divorce [52] | Self-report | Lewis, Langley and Jones [37] | Coping Efficacy Black adolescents: ɑ = 0.86 White adolescents: ɑ = 0.85 | N/A | Coping efficacy Black adolescents: r = −0.42 White adolescents: r = −0.47 |
| Coping Competency Beliefs | United States 9–12-year-old children who experienced divorce [53] | Self-report | Kilmer & Gil-Rivas [12] | Coping Competency ɑ = 0.63 | N/A | Coping competency Time 1: r = 0.11 Time 2: r = −0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Powell, T.; Wegmann, K.M.; Backode, E. Coping and Post-Traumatic Stress in Children and Adolescents after an Acute Onset Disaster: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4865. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094865
Powell T, Wegmann KM, Backode E. Coping and Post-Traumatic Stress in Children and Adolescents after an Acute Onset Disaster: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(9):4865. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094865
Chicago/Turabian StylePowell, Tara, Kate M. Wegmann, and Emily Backode. 2021. "Coping and Post-Traumatic Stress in Children and Adolescents after an Acute Onset Disaster: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 9: 4865. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094865