
A Real-World Study of the Association between a Brief Group Psychoeducation and the Course of Bipolar Disorder

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of the Sample
3.2. Study of the Association between the Intervention and Insight and Treatment Adherence Improvement
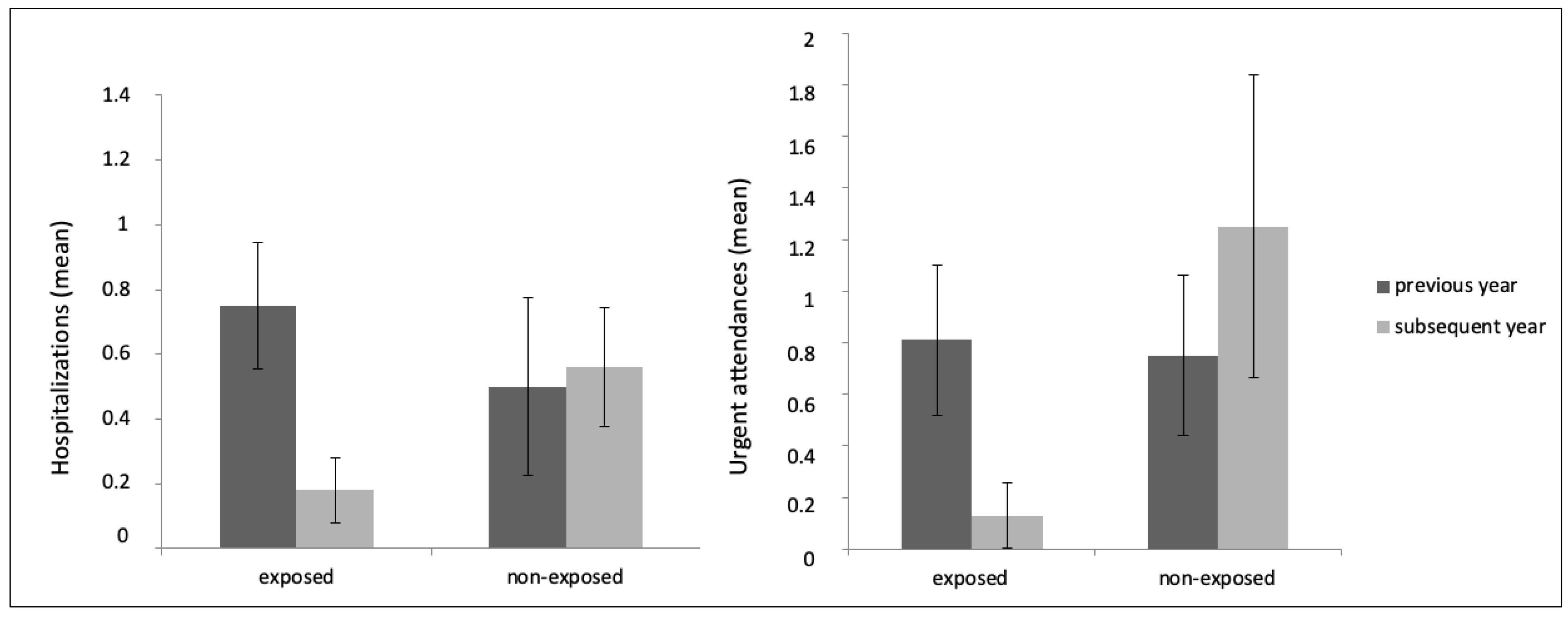
3.3. Study of the Association between the Intervention and the Number of Hospitalizations and Visits to Emergency Services
3.4. Study of the Association between the Intervention and the Rates of Hospitalizations and Visits to Emergency Services
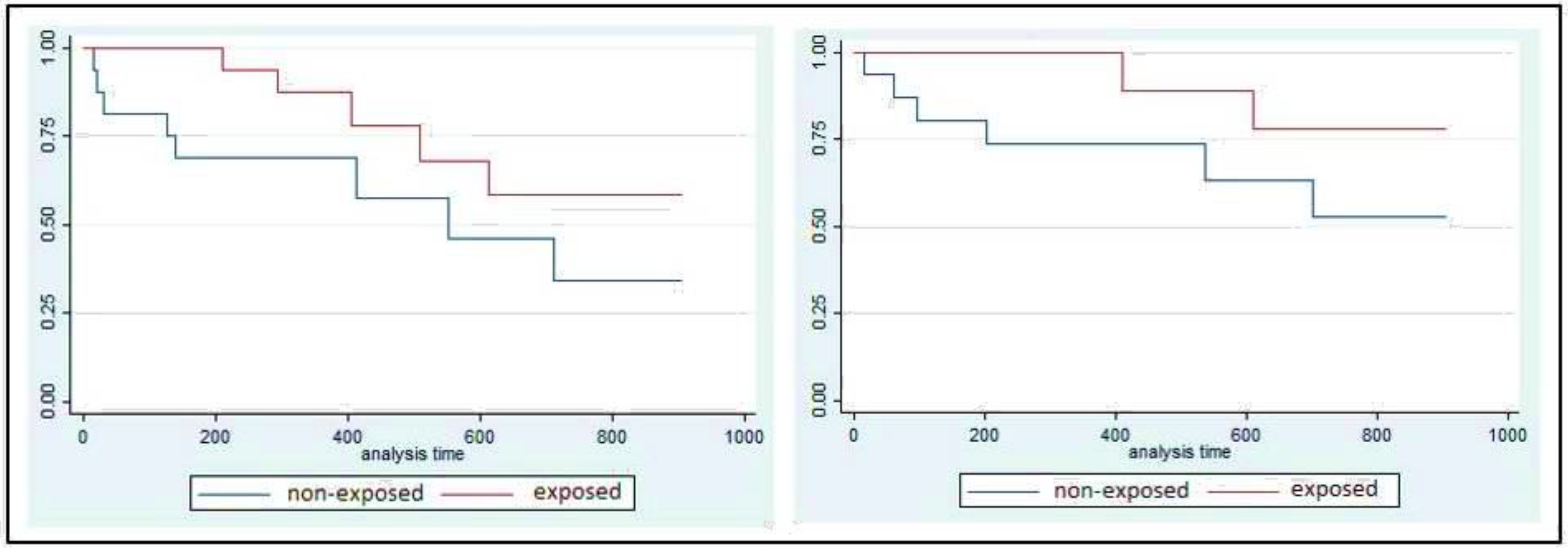
3.5. Study of the Association between the Intervention and the Lapsed Time until the First Hospitalization and the First Visit to the Emergency Services
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- IsHak, W.; Brown, K.; Aye, S.; Kahloon, M.; Mobaraki, S.; Hanna, R. Health-related quality of life in bipolar disorder. Bipolar Disord. 2012, 14, 6–18. [Google Scholar] [CrossRef] [PubMed]
- Dean, B.; Gerner, D.; Gerner, R. A systematic review evaluating health-related quality of life, work impairment, and healthcare costs and utilization in bipolar disorder. Curr. Med. Res. Opin. 2004, 20, 139–154. [Google Scholar] [CrossRef]
- Kleine-Budde, K.; Touil, E.; Moock, J.; Bramesfeld, A.; Kawohl, W.; Rössler, W. Cost of illness for bipolar disorder: A systematic review of the economic burden. Bipolar Disord. 2013, 16, 337–353. [Google Scholar] [CrossRef]
- Ferrari, A.J.; Stockings, E.; Khoo, J.P.; Erskine, H.E.; Degenhardt, L.; Vos, T.; Whiteford, H.A. The prevalence and burden of bipolar disorder: Findings from the Global Burden of Disease Study 2013. Bipolar Disord. 2016, 18, 440–450. [Google Scholar] [CrossRef]
- Grunze, H.; Vieta, E.; Goodwin, G.M.; Bowden, C.; Licht, R.W.; Möller, H.J.; Kasper, S.; WFSBP Task Force on Treatment Guidelines for Bipolar Disorders*. The World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the Biological Treatment of Bipolar Disorders: Update 2012 on the long-term treatment of bipolar disorder. World J. Biol. Psychiatry 2013, 14, 154–219. [Google Scholar] [CrossRef] [Green Version]
- Vieta, E.; Azorin, J.M.; Bauer, M.; Frangou, S.; Perugi, G.; Martinez, G.; Schreiner, A. Psychiatrists’ perceptions of potential reasons for non- and partial adherence to medication: Results of a survey in bipolar disorder from eight European countries. J. Affect Disord. 2012, 143, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Reed, C.; Novick, D.; Haro, J.; Aguado, J. Clinical and economic consequences of medication non-adherence in the treatment of patients with a manic/mixed episode of bipolar disorder: Results from the European Mania in Bipolar Longitudinal Evaluation of Medication (EMBLEM) Study. Psychiatry Res. 2011, 190, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Oud, M.; Mayo-Wilson, E.; Braidwood, R.; Schultet, P.; Jones, S.H.; Morriss, R.; Kupka, R.; Cuijpers, P.; Kendall, T. Psychological interventions for adults with bipolar disorder: Systematic review and meta-analysis. Br. J. Psychiatry 2016, 208, 213–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demissie, M.; Hanlon, C.; Birhane, R.; Ng, L.; Medhin, G.; Fekadu, A. Psychological interventions for bipolar disorder in low- and middle-income countries: Systematic review. Br. J. Psychiatry Open 2018, 4, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Joas, E.; Bäckman, K.; Karanti, A.; Sparding, T.; Colom, F.; Pålsson, E.; Landén, M. Psychoeducation for bipolar disorder and risk of recurrence and hospitalization-a within-individual analysis using registry data. Psychol. Med. 2020, 50, 1043–1049. [Google Scholar] [CrossRef]
- Bond, K.; Anderson, I. Psychoeducation for relapse prevention in bipolar disorder: A systematic review of efficacy in randomized controlled trials. Bipolar Disord. 2015, 17, 349–362. [Google Scholar] [CrossRef]
- Miklowitz, D.J.; Efthimiou, O.; Furukawa, T.A.; Scott, J.; McLaren, R.; Geddes, J.R.; Cipriani, A. Adjunctive Psychotherapy for Bipolar Disorder: A Systematic Review and Component Network Meta-analysis. JAMA Psychiatry 2021, 78, 141–150. [Google Scholar] [CrossRef]
- Buizza, C.; Candini, V.; Ferrari, C.; Ghilardi, A.; Saviotti, F.M.; Turrina, C.; Nobili, G.; Sabaudo, M.; De Girolamo, G. The Long-Term Effectiveness of Psychoeducation for Bipolar Disorders in Mental Health Services. A 4-Year Follow-Up Study. Front. Psychiatry 2019, 10, 873. [Google Scholar] [CrossRef]
- Colom, F.; Vieta, E.; Sánchez-Moreno, J.; Palomino-Otiniano, R.; Reinares, M.; Goikolea, J.M.; Benabarre, A.; Martínez-Arán, A. Group psychoeducation for stabilised bipolar disorders: 5-year outcome of a randomised clinical trial. Br. J. Psychiatry 2019, 194, 260–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, J.; Colom, F.; Popova, E.; Benabarre, A.; Cruz, N.; Valentí, M.; Goikolea, J.M.; Sánchez-Moreno, J.; Asenjo, M.A.; Vieta, E. Long-Term Mental Health Resource Utilization and Cost of Care Following Group Psychoeducation or Unstructured Group Support for Bipolar Disorders. J. Clin. Psychiatry 2009, 70, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Depp, C.A.; Ceglowski, J.; Wang, V.C.; Yaghouti, F.; Mausbach, B.T.; Thompson, W.K.; Granholm, E.L. Augmenting psychoeducation with a mobile intervention for bipolar disorder: A randomized controlled trial. J. Affect. Disord. 2015, 174, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, L.; Sharma, P.; Nair, S. Effect of psycho-education on quality of life and disability among persons with bipolar disorder: Randomized controlled trial. Indian J. Health Wellbeing 2015, 5, 461–466. [Google Scholar]
- Chen, R.; Zhu, X.; Capitão, L.; Zhang, H.; Luo, J.; Wang, X.; Xi, Y.; Song, X.; Feng, Y.; Cao, L.; et al. Psychoeducation for psychiatric inpatients following remission of a manic episode in bipolar I disorder: A randomized controlled trial. Bipolar Disord. 2019, 21, 76–85. [Google Scholar] [CrossRef]
- Faridhosseini, F.; Baniasadi, M.; Bordbar, M.; Pourgholami, M.; Ahrari, S.; Asgharipour, N. Effectiveness of Psychoeducational Group Training on Quality of Life and Recurrence of Patients with Bipolar Disorder. Iran. J. Psychiatry 2017, 12, 21–28. [Google Scholar]
- Wiener, C.; Molina, M.; Moreira, F.; Dos Passos, M.B.; Jansen, K.; Da Silva, R.A.; Souza, L.D.D.M.; Oses, J.P. Brief psychoeducation for bipolar disorder: Evaluation of trophic factors serum levels in young adults. Psychiatry Res. 2017, 257, 367–371. [Google Scholar] [CrossRef]
- Çuhadar, D.; Çam, M. Effectiveness of Psychoeducation in Reducing Internalized Stigmatization in Patients With Bipolar Disorder. Arch. Psychiatry Nurs. 2014, 28, 62–66. [Google Scholar] [CrossRef]
- Bilderbeck, A.; Atkinson, L.; McMahon, H.; Voysey, M.; Simon, J.; Price, J.; Rendell, J.; Hinds, C.; Geddes, J.R.; Holmes, E.; et al. Psychoeducation and online mood tracking for patients with bipolar disorder: A randomised controlled trial. J. Affect. Disord. 2016, 205, 245–251. [Google Scholar] [CrossRef]
- Eker, F.; Harkin, S. Effectiveness of six-week psychoeducation program on adherence of patients with bipolar affective disorder. J. Affect. Disord. 2012, 138, 409–416. [Google Scholar]
- Novick, D.; Montgomery, W.; Treuer, T.; Aguado, J.; Kraemer, S.; Haro, J.M. Relationship of insight with medication adherence and the impact on outcomes in patients with schizophrenia and bipolar disorder: Results from a 1-year European outpatient observational study. BMC Psychiatry 2015, 15, 189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colom, F.; Vieta, E. Manual de Psicoeducación Para el Trastorno Bipolar; Ars Médica: Barcelona, Spain, 2004. [Google Scholar]
- Colom, F.; Vieta, E.; Martínez-Arán, A.; Reinares, M.; Goikolea, J.M.; Benabarre, A.; Torrent, C.; Comes, M.; Corbella, B.; Parramon, G.; et al. A randomized trial on the efficacy of group psychoeducation in the prophylaxis of recurrences in bipolar patients whose disease is in remission. Arch. Gen. Psychiatry 2003, 60, 402–407. [Google Scholar] [CrossRef] [Green Version]
- Andersen, P.; Gill, R. Cox’s regression model for counting processes: A large sample study. Ann. Stat. 1982, 10, 1100–1120. [Google Scholar] [CrossRef]
- Depp, C.; Perivoliotis, D.; Holden, J.; Dorr, J.; Granholm, E. Single-Session Mobile-Augmented Intervention in Serious Mental Illness: A Three-Arm Randomized Controlled Trial. Schizophr. Bull. 2019, 45, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo-Mazzei, D.; Reinares, M.; Mateu, A.; Nikolova, V.L.; Bonnín, C.D.M.; Samalin, L.; García-Estela, A.; Pérez-Solá, V.; Young, A.H.; Strejilevich, S.; et al. OpenSIMPLe: A real-world implementation feasibility study of a smartphone-based psychoeducation programme for bipolar disorder. J. Affect. Disord. 2018, 241, 436–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amador, X.; Strauss, D.; Yale, S.; Flaum, M.; Endicott, J.; Gorman, J. Assessment of insight in psychosis. Am. J. Psychiatry 1993, 150, 873–879. [Google Scholar] [PubMed] [Green Version]
- Olaya, B.; Marsà, F.; Ochoa, S.; Balanzá-Martínez, V.; Barbeito, S.; García-Portilla, M.P.; González-Pinto, A.; Lobo, A.; López-Antón, R.; Usall, J.; et al. Development of the insight scale for affective disorders (ISAD): Modification from the scale to assess unawareness of mental disorder. J. Affect. Disord. 2012, 142, 65–71. [Google Scholar] [CrossRef]
- Sajatovic, M.; Chen, P.; Dines, P.; Shirley, E. Psychoeducational Approaches to Medication Adherence in Patients with Bipolar Disorder. Dis. Manag. Health Outcomes 2007, 15, 181–192. [Google Scholar] [CrossRef]
- Pakpour, A.H.; Modabbernia, A.; Lin, C.Y.; Saffari, M.; Ahmadzad Asl, M.; Webb, T.L. Promoting medication adherence among patients with bipolar disorder: A multicenter randomized controlled trial of a multifaceted intervention. Psychol. Med. 2017, 47, 2528–2539. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, F.; Ebrahimi, H.; Ranjbar, F.; Razavi, S.S.; Asghari, E. The Effect of Group Psychoeducation Program on Medication Adherence in Patients with Bipolar Mood Disorders: A Randomized Controlled Trial. J. Caring Sci. 2016, 5, 287–297. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Exposed Cohort | Non-Exposed Cohort | Statistical Test | p-Value | |
|---|---|---|---|---|
| Age [mean (SD)] | 37.19 (6.91) | 40.38 (9.75) | t = 1.0672 | 0.2944 |
| Sex, women [N (%)] | 9 (56.25%) | 9 (56.25%) | chi2 = 0.0000 | 1.0000 |
| Duration of illness, years [M (SD)] | 8.31 (8.87) | 10.5 (10.53) | t = 0.6355 | 0.5299 |
| Educational level [N (%)] | chi2 = 0.5818 | 0.446 | ||
| Primary studies | 0 (0%) | 0 (0%) | ||
| Secondary studies | 6 (37.50%) | 4 (25.00%) | ||
| Superior studies | 10 (62.50%) | 12 (75.00%) | ||
| Basal insight level [N (%)] | chi2 = 1.6769 | 0.504 * | ||
| Poor | 1 (6.25%) | 3 (18.75%) | ||
| Partial | 6 (37.50%) | 7 (43.75%) | ||
| Good | 9 (56.25%) | 6 (37.50%) | ||
| Basal treatment adherence level [N (%)] | chi2 = 0.5333 | 1.000 * | ||
| Poor | 2 (12.50%) | 3 (18.75%) | ||
| Partial | 2 (12.50%) | 1 (6.25%) | ||
| Good | 12 (75.00%) | 12 (75.00%) | ||
| Rapid-cycling [N (%)] | 1 (6.25%) | 1 (6.25%) | chi2 = 0.000 | 1.000 * |
| Psychotic features [N (%)] | 11 (68.75%) | 10 (62.50%) | chi2 = 0.1385 | 0.710 |
| Basal pharmacological treatment [N (%)] | ||||
| Mood stabilizers | 15 (93.75%) | 16 (100%) | chi2 = 1.0323 | 1.000 * |
| Antipsychotics | 9 (56.25%) | 9 (56.25%) | chi2 = 0.0000 | 1.000 * |
| Antidepressants | 3 (18.75%) | 3 (18.75%) | chi2 = 0.0000 | 1.000 * |
| Benzodiazepines | 2 (12.50%) | 6 (37.50%) | chi2 = 2.6667 | 0.220 * |
| Hazard Ratio | 95% Confidence Interval | |
|---|---|---|
| Raw Data | ||
| Hospitalizations | 0.44 | 0.17–1.14 |
| Urgent attendances | 0.25 | 0.05–1.16 |
| Controlling for Psychotic Features | ||
| Hospitalizations | 0.42 | 0.18–0.96 |
| Urgent attendances | 0.25 | 0.06–1.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casellas, E.; Raventós, B.; Piñeiro-Ríos, M.; Navarro-Martínez, H.; Castillón-Espezel, M.; Portella, M.J.; Martín-Blanco, A. A Real-World Study of the Association between a Brief Group Psychoeducation and the Course of Bipolar Disorder. Int. J. Environ. Res. Public Health 2021, 18, 5019. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095019
Casellas E, Raventós B, Piñeiro-Ríos M, Navarro-Martínez H, Castillón-Espezel M, Portella MJ, Martín-Blanco A. A Real-World Study of the Association between a Brief Group Psychoeducation and the Course of Bipolar Disorder. International Journal of Environmental Research and Public Health. 2021; 18(9):5019. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095019
Chicago/Turabian StyleCasellas, Elisabet, Beatriz Raventós, Marina Piñeiro-Ríos, Helena Navarro-Martínez, Maite Castillón-Espezel, Maria J. Portella, and Ana Martín-Blanco. 2021. "A Real-World Study of the Association between a Brief Group Psychoeducation and the Course of Bipolar Disorder" International Journal of Environmental Research and Public Health 18, no. 9: 5019. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095019