
Neighborhood Socioeconomic Resources and Crime-Related Psychosocial Hazards, Stroke Risk, and Cognition in Older Adults

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
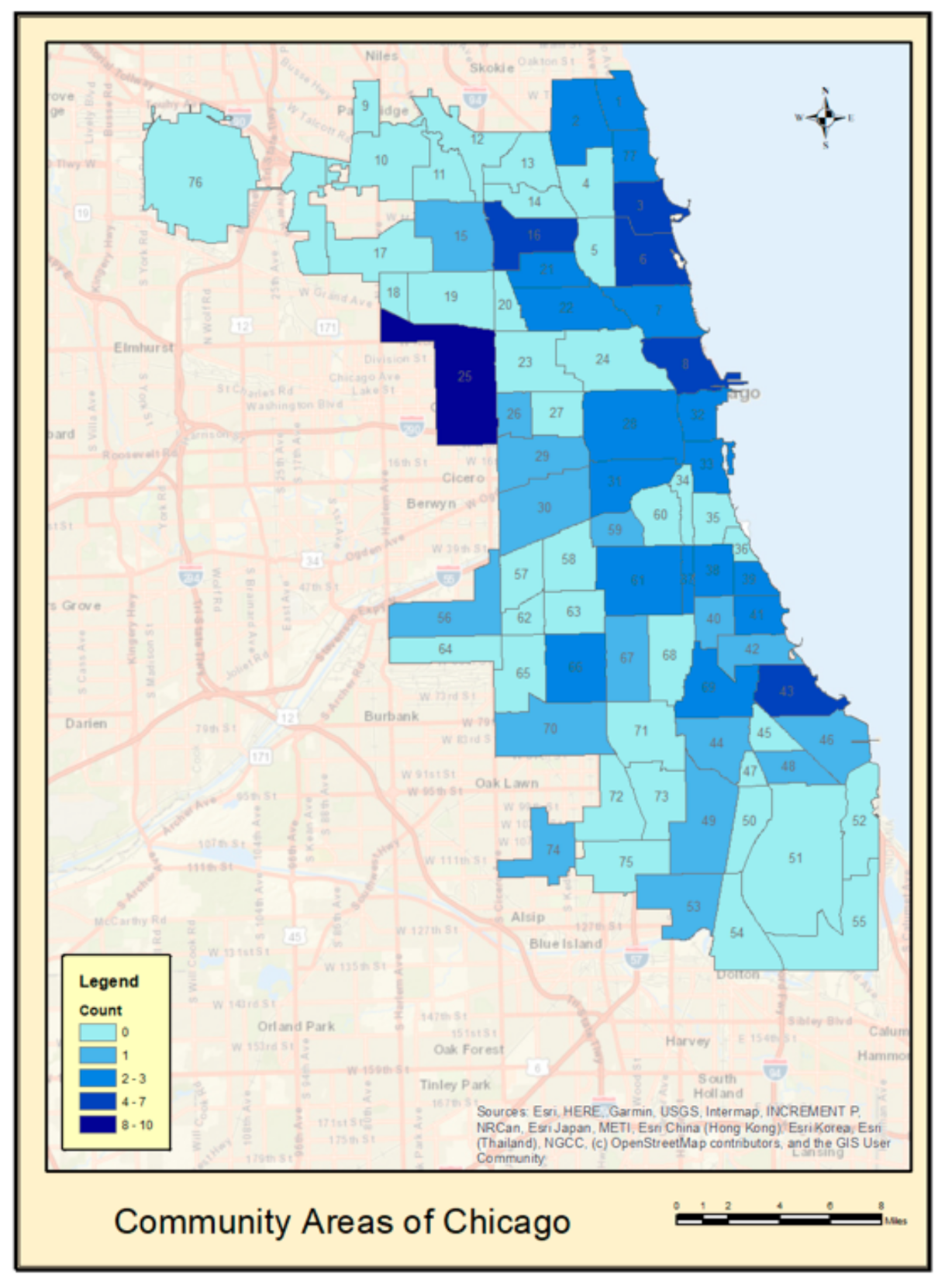
2.2. Neighborhood-Level Socioeconomic Environment
2.3. Cardiovascular Disease Risk
2.4. Cognition
2.5. Statistical Analyses
3. Results
3.1. Participants
3.2. Correlations of Key Variables of Interest
3.3. Structural Equation Modeling
3.3.1. Learning, Memory, and Recognition (LMR)
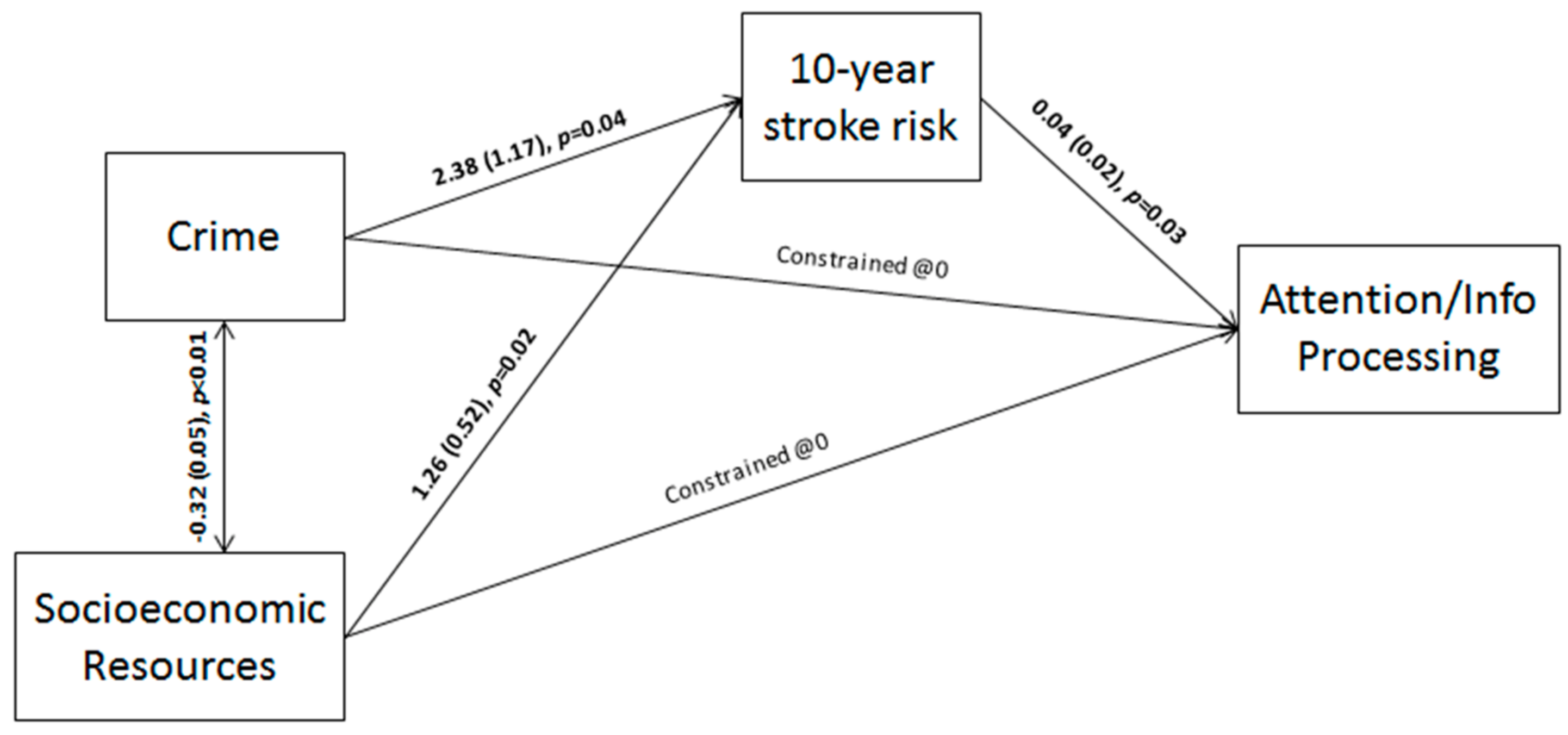
3.3.2. Attention/Information Processing (AIP)
3.3.3. Executive Functioning (EF)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bonaccorsi, G.; Manzi, F.; del Riccio, M.; Setola, N.; Naldi, E.; Milani, C.; Giorgetti, D.; Dellisanti, C.; Lorini, C. Impact of the Built Environment and the Neighborhood in Promoting the Physical Activity and the Healthy Aging in Older People: An Umbrella Review. Int. J. Environ. Res. Public Health 2020, 17, 6127. [Google Scholar] [CrossRef] [PubMed]
- Besser, L.M.; McDonald, N.C.; Song, Y.; Kukull, W.A.; Rodriguez, D.A. Neighborhood Environment and Cognition in Older Adults: A Systematic Review. Am. J. Prev. Med. 2017, 53, 241–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruger, D.J.; Reischl, T.M.; Gee, G.C. Neighborhood social conditions mediate the association between physical deterioration and mental health. Am. J. Community Psychol. 2007, 40, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Diez Roux, A.V.; Mair, C. Neighborhoods and health. Ann. N. Y. Acad. Sci. 2010, 1186, 125–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diez Roux, A.V.; Mujahid, M.S.; Hirsch, J.A.; Moore, K.; Moore, L.V. The Impact of Neighborhoods on CV Risk. Glob Heart 2016, 11, 353–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diez Roux, A.V.; Merkin, S.S.; Arnett, D.; Chambless, L.; Massing, M.; Nieto, F.J.; Sorlie, P.; Szklo, M.; Tyroler, H.A.; Watson, R.L. Neighborhood of residence and incidence of coronary heart disease. N. Engl. J. Med. 2001, 345, 99–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schultz, W.M.; Kelli, H.M.; Lisko, J.C.; Varghese, T.; Shen, J.; Sandesara, P.; Quyyumi, A.A.; Taylor, H.A.; Gulati, M.; Harold, J.G.; et al. Socioeconomic Status and Cardiovascular Outcomes: Challenges and Interventions. Circulation 2018, 137, 2166–2178. [Google Scholar] [CrossRef]
- Lee, H.; Waite, L.J. Cognition in Context: The Role of Objective and Subjective Measures of Neighborhood and Household in Cognitive Functioning in Later Life. Gerontologist 2018, 58, 159–169. [Google Scholar] [CrossRef] [Green Version]
- Duron, E.; Hanon, O. Vascular risk factors, cognitive decline, and dementia. Vasc Health Risk Manag. 2008, 4, 363–381. [Google Scholar]
- Gorelick, P.B. Prevention of cognitive impairment: Scientific guidance and windows of opportunity. J. Neurochem. 2018, 144, 609–616. [Google Scholar] [CrossRef] [Green Version]
- Sundquist, K.; Malmstrom, M.; Johansson, S.E. Neighbourhood deprivation and incidence of coronary heart disease: A multilevel study of 2.6 million women and men in Sweden. J. Epidemiol. Community Health 2004, 58, 71–77. [Google Scholar] [CrossRef]
- Diez Roux, A.V. Residential environments and cardiovascular risk. J. Urban Health 2003, 80, 569–589. [Google Scholar] [CrossRef] [Green Version]
- Clark, C.R.; Ommerborn, M.J.; Hickson, D.A.; Grooms, K.N.; Sims, M.; Taylor, H.A.; Albert, M.A. Neighborhood disadvantage, neighborhood safety and cardiometabolic risk factors in African Americans: Biosocial associations in the Jackson Heart study. PLoS ONE 2013, 8, e63254. [Google Scholar]
- Boots, E.A.; Zhan, L.; Dion, C.; Karstens, A.J.; Peven, J.C.; Ajilore, O.; Lamar, M. Cardiovascular disease risk factors, tract-based structural connectomics, and cognition in older adults. Neuroimage 2019, 196, 152–160. [Google Scholar] [CrossRef]
- Bronas, U.G.; Steffen, A.; Dion, C.; Boots, E.A.; Arfanakis, K.; Marquez, D.X.; Lamar, M. Sedentary Time and White Matter Hyperintensity Volume in Older Adults. Med. Sci. Sports Exerc. 2019, 51, 1613–1618. [Google Scholar] [CrossRef]
- Peven, J.C.; Chen, Y.; Guo, L.; Zhan, L.; Boots, E.A.; Dion, C.; Libon, D.J.; Heilman, K.M.; Lamar, M. The oblique effect: The relationship between profiles of visuospatial preference, cognition, and brain connectomics in older adults. Neuropsychologia 2019, 135, 107236. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B.W. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition with Psychotic Screen (SCID-I/P, W/PSY SCREEN); Biometrics Research; New York State Psychiatric Institute: New York, NY, USA, 2002. [Google Scholar]
- Hamilton, M. A Rating Scale for Depression. J. Neurol. Neurosurg Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Messer, L.C.; Laraia, B.A.; Kaufman, J.S.; Eyster, J.; Holzman, C.; Culhane, J.; Elo, I.; Burke, J.G.; O’Campo, P. The development of a standardized neighborhood deprivation index. J. Urban Health 2006, 83, 1041–1062. [Google Scholar] [CrossRef] [Green Version]
- Dufouil, C.; Beiser, A.; McLure, L.A.; Wolf, P.A.; Tzourio, C.; Howard, V.J.; Westwood, A.J.; Himali, J.J.; Sullivan, L.; Aparicio, H.J.; et al. Revised Framingham Stroke Risk Profile to Reflect Temporal Trends. Circulation 2017, 135, 1145–1159. [Google Scholar] [CrossRef]
- Lamar, M.; Rubin, L.H.; Ajilore, O.; Charlton, R.; Zhang, A.; Yang, S.; Cohen, J.; Kumar, A. What Metabolic Syndrome Contributes to Brain Outcomes in African American & Caucasian Cohorts. Curr. Alzheimer Res. 2015, 12, 640–647. [Google Scholar]
- Delis, D.C.; Kramer, J.H.; Kaplan, E.; Ober, B.A. California Verbal Learning Test; Harcourt Assessment, Inc.: San Antonio, TX, USA, 2000. [Google Scholar]
- Kenny, D.A. Measuring Model Fit; 2015. Available online: http://davidakenny.net/cm/fit.htm (accessed on 1 May 2021).
- MacCallum, R.C.; Browne, M.W.; Sugawara, H.M. Power analysis and determination of sample size for covariance structure modeling. Psychol. Med. 1996, 1, 130–149. [Google Scholar] [CrossRef]
- Moss, S. Fit Indices for Strutural Equation Modeling; 2016. Available online: https://www.sicotests.com/psyarticle.asp?id=277 (accessed on 1 May 2021).
- Clarke, P.J.; Ailshire, J.A.; House, J.S.; Morenoff, J.D.; King, K.; Melendez, R.; Langa, K.M. Cognitive function in the community setting: The neighbourhood as a source of ‘cognitive reserve’? J. Epidemiol. Community Health 2012, 66, 730–736. [Google Scholar] [CrossRef] [Green Version]
- Needham, B.L.; Carroll, J.E.; Diez Roux, A.V.; Fitzpatrick, A.L.; Moore, K.; Seeman, T.E. Neighborhood characteristics and leukocyte telomere length: The Multi-Ethnic Study of Atherosclerosis. Health Place 2014, 28, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Hajat, A.; Moore, K.; Do, D.P.; Stein Merkin, S.; Punjabi, N.M.; Sanchez, B.N.; Seeman, T.; Diez-Roux, A.V. Examining the cross-sectional and longitudinal association between diurnal cortisol and neighborhood characteristics: Evidence from the multi-ethnic study of atherosclerosis. Health Place 2015, 34, 199–206. [Google Scholar] [CrossRef] [Green Version]
- Waldstein, S.R.; Dore, G.A.; Davatzikos, C.; Katzel, L.I.; Gullapalli, R.; Seliger, S.L.; Kouo, T.; Rosenberger, W.F.; Erus, G.; Evans, M.K.; et al. Differential Associations of Socioeconomic Status With Global Brain Volumes and White Matter Lesions in African American and White Adults: The HANDLS SCAN Study. Psychosom. Med. 2017, 79, 327–335. [Google Scholar]
- Brenner, A.B.; Diez Roux, A.V.; Barrientos-Gutierrez, T.; Borrell, L.N. Associations of Alcohol Availability and Neighborhood Socioeconomic Characteristics With Drinking: Cross-Sectional Results From the Multi-Ethnic Study of Atherosclerosis (MESA). Subst Use Misuse 2015, 50, 1606–1617. [Google Scholar] [CrossRef] [Green Version]
- Brenner, A.B.; Borrell, L.N.; Barrientos-Gutierrez, T.; Diez Roux, A.V. Longitudinal associations of neighborhood socioeconomic characteristics and alcohol availability on drinking: Results from the Multi-Ethnic Study of Atherosclerosis (MESA). Soc. Sci. Med. 2015, 145, 17–25. [Google Scholar] [CrossRef] [Green Version]
- Clarke, P.J.; Weuve, J.; Barnes, L.; Evans, D.A.; Mendes de Leon, C.F. Cognitive decline and the neighborhood environment. Ann. Epidemiol. 2015, 25, 849–854. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Unrotated Factor Loadings | |
|---|---|
| % below poverty level | 0.87 |
| Median household income | −0.88 |
| % with less than 12 years of education | 0.79 |
| % with 16+ years of education | −0.87 |
| % unemployment | 0.81 |
| Total Variance Explained | 71.83% |
| Unrotated Factor Loadings | |
|---|---|
| Assault | 0.99 |
| Battery | 0.95 |
| Robbery | 0.84 |
| Sexual Assault | 0.93 |
| Homicide | 0.90 |
| Total Variance Explained | 85.23% |
| Age, M (SD) | 67.91 (6.66) |
| Female, Sex n (%) | 53 (50) |
| Race/Ethnicity, n (%) | |
| Non-Latino Black | 50 (47.1) |
| Non-Latino White | 48 (45.2) |
| Latino | 8 (7.5) |
| Education, M (SD) | 15.98 (2.86) |
| MMSE, M (SD) | 28.66 (1.38) |
| FSRP-10, M (SD) | 6.20 (4.86) |
| 1. | 2. | 3. | 4. | 5. | |
|---|---|---|---|---|---|
| 1. Socioeconomic composite | -- | ||||
| 2. Crime-related composite | −0.65, | -- | |||
| p < 0.001 | |||||
| 3. FSRP-10 | 0.08, | 0.02, | -- | ||
| p = 0.38 | p = 0.82 | ||||
| 4. Cognition—LMR domain | 0.09, | 0.09, | −0.02, | -- | |
| p = 0.35 | p = 0.34 | p = 0.80 | |||
| 5. Cognition—AIP domain | −0.05, | −0.13, | 0.22, | −0.33, | -- |
| p = 0.58 | p = 0.16 | p = 0.02 | p < 0.001 | ||
| 6. Cognition—EF domain | 0.09, | 0.01, | −0.15, | 0.43, | −0.40, |
| p = 0.37 | p = 0.88 | p = 0.13 | p < 0.001 | p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz, L.D.; Brown, M.; Li, Y.; Boots, E.A.; Barnes, L.L.; Jason, L.; Zenk, S.; Clarke, P.; Lamar, M. Neighborhood Socioeconomic Resources and Crime-Related Psychosocial Hazards, Stroke Risk, and Cognition in Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 5122. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105122
Ruiz LD, Brown M, Li Y, Boots EA, Barnes LL, Jason L, Zenk S, Clarke P, Lamar M. Neighborhood Socioeconomic Resources and Crime-Related Psychosocial Hazards, Stroke Risk, and Cognition in Older Adults. International Journal of Environmental Research and Public Health. 2021; 18(10):5122. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105122
Chicago/Turabian StyleRuiz, Linda D., Molly Brown, Yan Li, Elizabeth A. Boots, Lisa L. Barnes, Leonard Jason, Shannon Zenk, Philippa Clarke, and Melissa Lamar. 2021. "Neighborhood Socioeconomic Resources and Crime-Related Psychosocial Hazards, Stroke Risk, and Cognition in Older Adults" International Journal of Environmental Research and Public Health 18, no. 10: 5122. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105122