
Frequency of Injury and Illness in the Final 4 Weeks before a Trail Running Competition

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Data Sources and Variables
2.4. Statistical Methods
3. Results
3.1. Aim 1: Frequency of Injury and Illness
3.2. Aim 2: Comparison of Injured and Ill Athletes by Sex, Age, BMI and Competition Distance
3.3. Aim 3: Description of the Mechanism of Injury, Anatomical Region (Injury) or Organ System (Illness), Consequences of Injury on Training (i.e., Volume, Intensity and Performance) and Self-Perception of the Severity of Injury for Competition
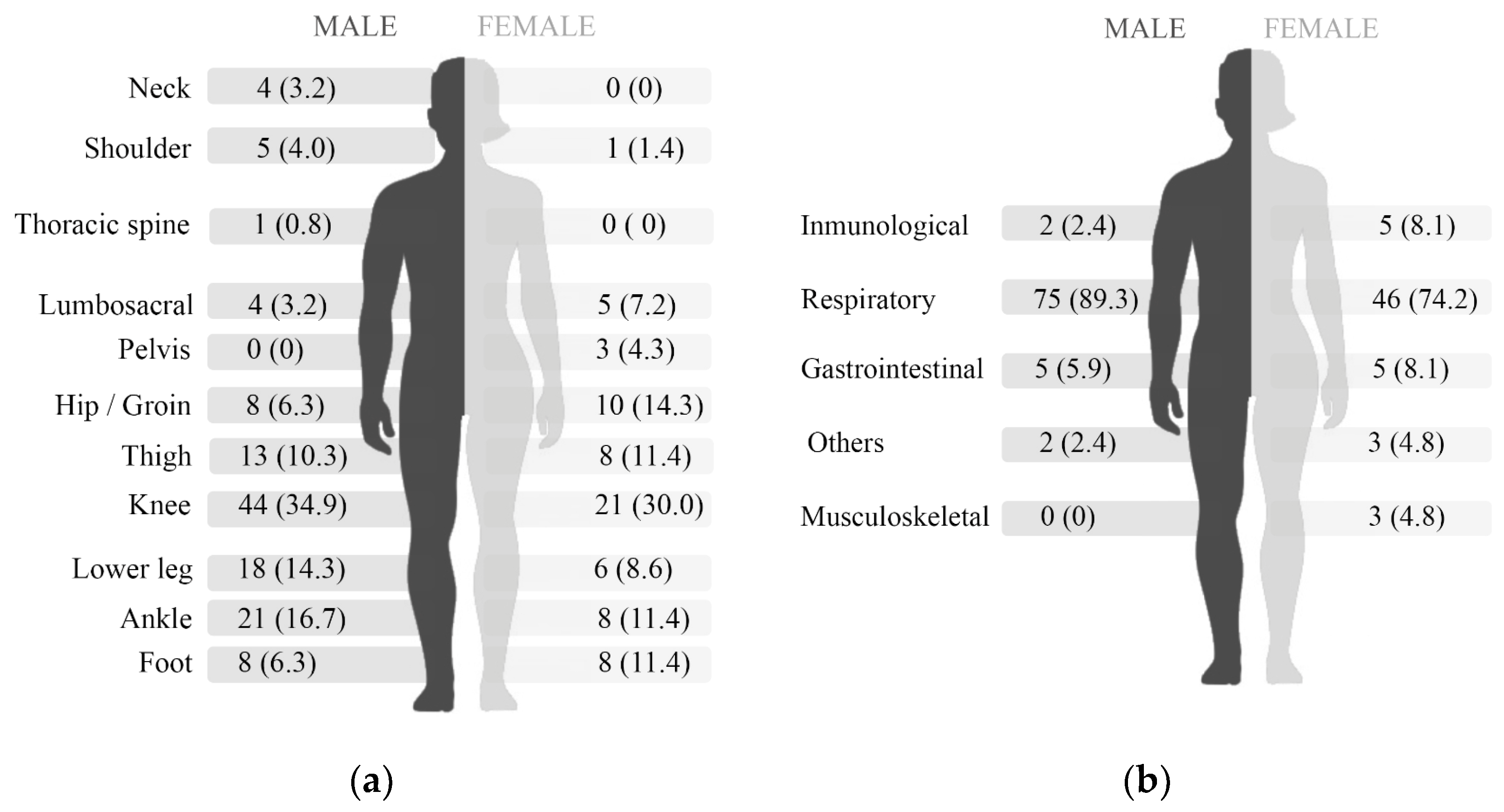
3.4. Aim 4: Comparison of the Anatomical Region (Injury) and the Organ System (Illness) Affected among Athletes by Sex
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hespanhol, L.C., Jr.; Pillay, J.D.; van Mechelen, W.; Verhagen, E. Meta-Analyses of the Effects of Habitual Running on Indices of Health in Physically Inactive Adults. Sports Med. 2015, 45, 1455–1468. [Google Scholar] [CrossRef] [Green Version]
- Cejka, N.; Rust, C.A.; Lepers, R.; Onywera, V.; Rosemann, T.; Knechtle, B. Participation and performance trends in 100-km ultra-marathons worldwide. J. Sports Sci. 2014, 32, 354–366. [Google Scholar] [CrossRef] [Green Version]
- Association, I.T. Definition Trail. Available online: https://itra.run/content/definition-trail (accessed on 17 May 2021).
- van Gent, R.N.; Siem, D.; van Middelkoop, M.; van Os, A.G.; Bierma-Zeinstra, S.M.; Koes, B.W. Incidence and determinants of lower extremity running injuries in long distance runners: A systematic review. Br. J. Sports Med. 2007, 41, 469–480. [Google Scholar] [CrossRef] [Green Version]
- Kluitenberg, B.; van Middelkoop, M.; Diercks, R.; van der Worp, H. What are the Differences in Injury Proportions between Different Populations of Runners? A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1143–1161. [Google Scholar] [CrossRef] [Green Version]
- Viljoen, C.T.; van Rensburg, D.C.J.; Verhagen, E.; van Mechelen, W.; Tomás, R.; Schoeman, M.; Scheepers, S.; Korkie, E. Epidemiology of Injury and Illness Among Trail Runners: A Systematic Review. Sports Med. 2021, 51, 917–943. [Google Scholar] [CrossRef]
- Hulme, A.; Nielsen, R.O.; Timpka, T.; Verhagen, E.; Finch, C. Risk and Protective Factors for Middle- and Long-Distance Running-Related Injury. Sports Med. 2017, 47, 869–886. [Google Scholar] [CrossRef]
- Viljoen, C.T.; van Rensburg, D.C.C.J.; van Rensburg, A.J.; Booysen, E.; Chauke, S.; Coetzee, P.; Hurlimann, A.; Jooste, M.; Nibe, Y.; Schulenburg, C.; et al. One in four trail running race entrants sustained an injury in the 12 months training preceding the 2019 SkyRun race. Phys. Ther. Sport 2020, 47, 120–126. [Google Scholar] [CrossRef]
- Gleeson, M.; Pyne, D.B. Respiratory inflammation and infections in high-performance athletes. Immunol. Cell Biol. 2016, 94, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Schwellnus, M.; Soligard, T.; Alonso, J.M.; Bahr, R.; Clarsen, B.; Dijkstra, H.P.; Gabbett, T.J.; Gleeson, M.; Hägglund, M.; Hutchinson, M.R.; et al. How much is too much? (Part 2) International Olympic Committee consensus statement on load in sport and risk of illness. Br. J. Sports Med. 2016, 50, 1043–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hespanhol, L.C., Jr.; van Mechelen, W.; Verhagen, E. Health and Economic Burden of Running-Related Injuries in Dutch Trailrunners: A Prospective Cohort Study. Sports Med. 2017, 47, 367–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saragiotto, B.T.; Yamato, T.P.; Lopes, A.D. What do recreational runners think about risk factors for running injuries? A descriptive study of their beliefs and opinions. J. Orthop. Sports Phys. Ther. 2014, 44, 733–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheer, B.V.; Murray, A. Al Andalus Ultra Trail: An observation of medical interventions during a 219-km, 5-day ultramarathon stage race. Clin. J. Sport Med. 2011, 21, 444–446. [Google Scholar] [CrossRef] [PubMed]
- Bertelsen, M.L.; Hulme, A.; Petersen, J.; Brund, R.K.; Sørensen, H.; Finch, C.F.; Parner, E.T.; Nielsen, R.O. A framework for the etiology of running-related injuries. Scand. J. Med. Sci. Sports 2017, 27, 1170–1180. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.M.; Jacobsson, J.; Timpka, T.; Ronsen, O.; Kajenienne, A.; Dahlstrom, O.; Spreco, A.; Edouard, P. Preparticipation injury complaint is a risk factor for injury: A prospective study of the Moscow 2013 IAAF Championships. Br. J. Sports Med. 2015, 49, 1118–1124. [Google Scholar] [CrossRef] [Green Version]
- Hoover, D.L.; VanWye, W.R.; Judge, L.W. Periodization and physical therapy: Bridging the gap between training and rehabilitation. Phys. Ther. Sport 2016, 18, 1–20. [Google Scholar] [CrossRef]
- Nielsen, R.O.; Parner, E.T.; Nohr, E.A.; Sorensen, H.; Lind, M.; Rasmussen, S. Excessive progression in weekly running distance and risk of running-related injuries: An association which varies according to type of injury. J. Orthop. Sports Phys. Ther. 2014, 44, 739–747. [Google Scholar] [CrossRef]
- Edouard, P.; Jacobsson, J.; Timpka, T.; Alonso, J.M.; Kowalski, J.; Nilsson, S.; Karlsson, D.; Depiesse, F.; Branco, P. Extending in-competition Athletics injury and illness surveillance with pre-participation risk factor screening: A pilot study. Phys. Ther. Sport 2015, 16, 98–106. [Google Scholar] [CrossRef]
- Mountjoy, M.; Junge, A.; Benjamen, S.; Boyd, K.; Diop, M.; Gerrard, D.; van den Hoogenband, C.R.; Marks, S.; Martinez-Ruiz, E.; Miller, J.; et al. Competing with injuries: Injuries prior to and during the 15th FINA World Championships 2013 (aquatics). Br. J. Sports Med. 2015, 49, 37–43. [Google Scholar] [CrossRef] [Green Version]
- van Mechelen, W.; Hlobil, H.; Kemper, H.C. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med. 1992, 14, 82–99. [Google Scholar] [CrossRef]
- Franke, T.P.C.; Backx, F.J.G.; Huisstede, B.M.A. Running Themselves into the Ground? Incidence, Prevalence, and Impact of Injury and Illness in Runners Preparing for a Half or Full Marathon. J. Orthop. Sports Phys. Ther. 2019, 49, 518–528. [Google Scholar] [CrossRef] [PubMed]
- Malliaropoulos, N.; Mertyri, D.; Tsaklis, P. Prevalence of Injury in Ultra Trail Running. Hum. Mov. 2015, 16, 52–59. [Google Scholar] [CrossRef]
- Roi, G.S.; Monticone, M.; Salvoni, M.; Sassi, R.; Alberti, G. Self-Reported Knee Symptoms Assessed by KOOS Questionnaire in Downhill Runners (Skyrunners). PLoS ONE 2015, 10, e0126382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsang, S.; Royse, C.F.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J. Anaesth. 2017, 11 (Suppl. 1), S80–S89. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.M.; Junge, A.; Renstrom, P.; Engebretsen, L.; Mountjoy, M.; Dvorak, J. Sports injuries surveillance during the 2007 IAAF World Athletics Championships. Clin. J. Sport Med. 2009, 19, 26–32. [Google Scholar] [CrossRef]
- Van Tonder, A.; Schwellnus, M.; Swanevelder, S.; Jordaan, E.; Derman, W.; van Rensburg, D.C.J. A prospective cohort study of 7031 distance runners shows that 1 in 13 report systemic symptoms of an acute illness in the 8–12 day period before a race, increasing their risk of not finishing the race 1.9 times for those runners who started the race: SAFER study IV. Br. J. Sports Med. 2016, 50, 939–945. [Google Scholar]
- Hollander, K.; Rahlf, A.L.; Wilke, J.; Edler, C.; Steib, S.; Junge, A.; Zech, A. Sex-Specific Differences in Running Injuries: A Systematic Review with Meta-Analysis and Meta-Regression. Sports Med. 2021, 51, 1011–1039. [Google Scholar] [CrossRef] [PubMed]
- van der Worp, M.P.; ten Haaf, D.S.; van Cingel, R.; de Wijer, A.; Nijhuis-van der Sanden, M.W.; Staal, J.B. Injuries in runners; a systematic review on risk factors and sex differences. PLoS ONE 2015, 10, e0114937. [Google Scholar] [CrossRef]
- van Poppel, D.; van der Worp, M.; Slabbekoorn, A.; van den Heuvel, S.S.P.; van Middelkoop, M.; Koes, B.W.; Verhagen, A.P.; Scholten-Peeters, G.G.M. Risk factors for overuse injuries in short- and long-distance running: A systematic review. J. Sport Health Sci. 2021, 10, 14–28. [Google Scholar] [CrossRef]
- Palmer-Green, D.; Fuller, C.; Jaques, R.; Hunter, G. The Injury/Illness Performance Project (IIPP): A Novel Epidemiological Approach for Recording the Consequences of Sports Injuries and Illnesses. J. Sports Med. 2013, 2013, 523974. [Google Scholar] [CrossRef]
- Fourchet, F.; Millet, G.P.; Tomazin, K.; Guex, K.; Nosaka, K.; Edouard, P.; Degache, F.; Millet, G.Y. Effects of a 5-h hilly running on ankle plantar and dorsal flexor force and fatigability. Eur. J. Appl. Physiol. 2012, 112, 2645–2652. [Google Scholar] [CrossRef]
- Soligard, T.; Schwellnus, M.; Alonso, J.M.; Bahr, R.; Clarsen, B.; Dijkstra, H.P.; Gabbett, T.; Gleeson, M.; Hagglund, M.; Hutchinson, M.R.; et al. How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br. J. Sports Med. 2016, 50, 1030–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mujika, I.; Padilla, S. Detraining: Loss of training-induced physiological and performance adaptations. Part I: Short term insufficient training stimulus. Sports Med. 2000, 30, 79–87. [Google Scholar] [CrossRef]
- Covassin, T.; Beidler, E.; Ostrowski, J.; Wallace, J. Psychosocial aspects of rehabilitation in sports. Clin. Sports Med. 2015, 34, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.S.; Barton, C.J.; Gallie, R.; O’Halloran, P.; Morrissey, D. Runners with patellofemoral pain have altered biomechanics which targeted interventions can modify: A systematic review and meta-analysis. Gait Posture 2016, 45, 69–82. [Google Scholar] [CrossRef]
- Chumanov, E.S.; Wall-Scheffler, C.; Heiderscheit, B.C. Gender differences in walking and running on level and inclined surfaces. Clin. Biomech. 2008, 23, 1260–1268. [Google Scholar] [CrossRef] [PubMed]
- He, C.S.; Bishop, N.C.; Handzlik, M.K.; Muhamad, A.S.; Gleeson, M. Sex differences in upper respiratory symptoms prevalence and oral-respiratory mucosal immunity in endurance athletes. Exerc. Immunol. Rev. 2014, 20, 8–22. [Google Scholar] [PubMed]
- Schuh-Renner, A.; Canham-Chervak, M.; Grier, T.L.; Jones, B.H. Accuracy of self-reported injuries compared to medical record data. Musculoskelet. Sci. Pract. 2019, 39, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Perrotin, N.; Gardan, N.; Lesprillier, A.; Le Goff, C.; Seigneur, J.-M.; Abdi, E.; Sanudo, B.; Taiar, R. Biomechanics of Trail Running Performance: Quantification of Spatio-Temporal Parameters by Using Low Cost Sensors in Ecological Conditions. Appl. Sci. 2021, 11, 2093. [Google Scholar] [CrossRef]


{kind=link}
| Total n = 654 | Injured Athletes n = 205 | Non-Injured Athletes n = 449 | p-Value | Ill Athletes n = 146 | Non-Ill Athletes n = 508 | p-Value | |
|---|---|---|---|---|---|---|---|
| Sex ‡ | |||||||
| Female | 241 (36.9) | 74 (30.7) | 167 (69.3) | 0.787 | 59 (40.4) | 182 (35.8) | 0.312 |
| Males | 413 (63.1) | 131 (31.7) | 282 (68.3) | 87 (59.6) | 326 (64.2) | ||
| Age (years) † | 36.2 [30.6–43.0] | 36.7 [30.4–43.9] | 35.9 [30.8–42.3] | 0.595 | 36.4 [30.5–41.2] | 36.1 [30.7–43.3] | 0.632 |
| Height (cm) †,§ | 170.0 [163.0–175.0] | 170.0 [163.0–175.0] | 170.0 [163.0–175.3] | 169.5 [162.3–176.0] | 170.0 [164.0–175.0] | ||
| Weight (kg) †,§§ | 70.0 [60.0–78.0] | 70.0 [60.0–77.8] | 70.0 [60.0–79.0] | 70.0 [60.0–80.0] | 70.0 [60.0–78.0] | ||
| BMI †,§§§ | 24.0 [22.2–26.0] | 24.1 [22.3–25.8] | 23.9 [22.2–26.1] | 0.996 | 24.2 [22.6–26.1] | 23.9 [22.2–25.9] | 0.343 |
| Distance ‡ | |||||||
| 11 k | 194 (29.7) | 64 (33.0) | 130 (67.0) | 0.411 | 49 (33.6) | 145 (28.5) | 0.817 |
| 18 k | 136 (20.8) | 36 (26.5) | 100 (73.5) | 27 (18.5) | 109 (21.5) | ||
| 24 k | 144 (22.0) | 44 (30.6) | 100 (69.4) | 29 (19.9) | 115 (22.6) | ||
| 45 k | 101 (15.4) | 36 (35.6) | 65 (64.4) | 24 (16.4) | 77 (15.2) | ||
| 63 k | 47 (7.2) | 18 (38.3) | 29 (61.7) | 11 (7.5) | 36 (7.1) | ||
| Crossing (23 + 22 k) | 32 (4.9) | 7 (21.9) | 25 (78.1) | 6 (4.1) | 26 (5.1) |
| Consequences on Training | Total |
|---|---|
| Volume | n = 201 § |
| Not affected | 45 (22.4) |
| Mildly affected | 45 (22.4) |
| Moderately affected | 67 (33.3) |
| Significantly affected | 25 (12.4) |
| Not able to train | 19 (9.5) |
| Intensity | n = 198 §§ |
| Not affected | 39 (19.7) |
| Mildly affected | 50 (25.3) |
| Moderately affected | 64 (32.3) |
| Significantly affected | 30 (15.2) |
| Not able to train | 15 (7.6) |
| Performance | n = 199 §§§ |
| Not affected | 29 (14.6) |
| Mildly affected | 63 (31.7) |
| Moderately affected | 71 (35.7) |
| Significantly affected | 27 (13.6) |
| Not able to train | 9 (4.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gajardo-Burgos, R.; Monrroy-Uarac, M.; Barría-Pailaquilén, R.M.; Norambuena-Noches, Y.; van Rensburg, D.C.J.; Bascour-Sandoval, C.; Besomi, M. Frequency of Injury and Illness in the Final 4 Weeks before a Trail Running Competition. Int. J. Environ. Res. Public Health 2021, 18, 5431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105431
Gajardo-Burgos R, Monrroy-Uarac M, Barría-Pailaquilén RM, Norambuena-Noches Y, van Rensburg DCJ, Bascour-Sandoval C, Besomi M. Frequency of Injury and Illness in the Final 4 Weeks before a Trail Running Competition. International Journal of Environmental Research and Public Health. 2021; 18(10):5431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105431
Chicago/Turabian StyleGajardo-Burgos, Rubén, Manuel Monrroy-Uarac, René Mauricio Barría-Pailaquilén, Yessenia Norambuena-Noches, Dina Christa Janse van Rensburg, Claudio Bascour-Sandoval, and Manuela Besomi. 2021. "Frequency of Injury and Illness in the Final 4 Weeks before a Trail Running Competition" International Journal of Environmental Research and Public Health 18, no. 10: 5431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105431