
Bioelectrical Impedance Vector Analysis: A Valuable Tool to Monitor Daily Body Hydration Dynamics at Altitude

 , , and
, , and 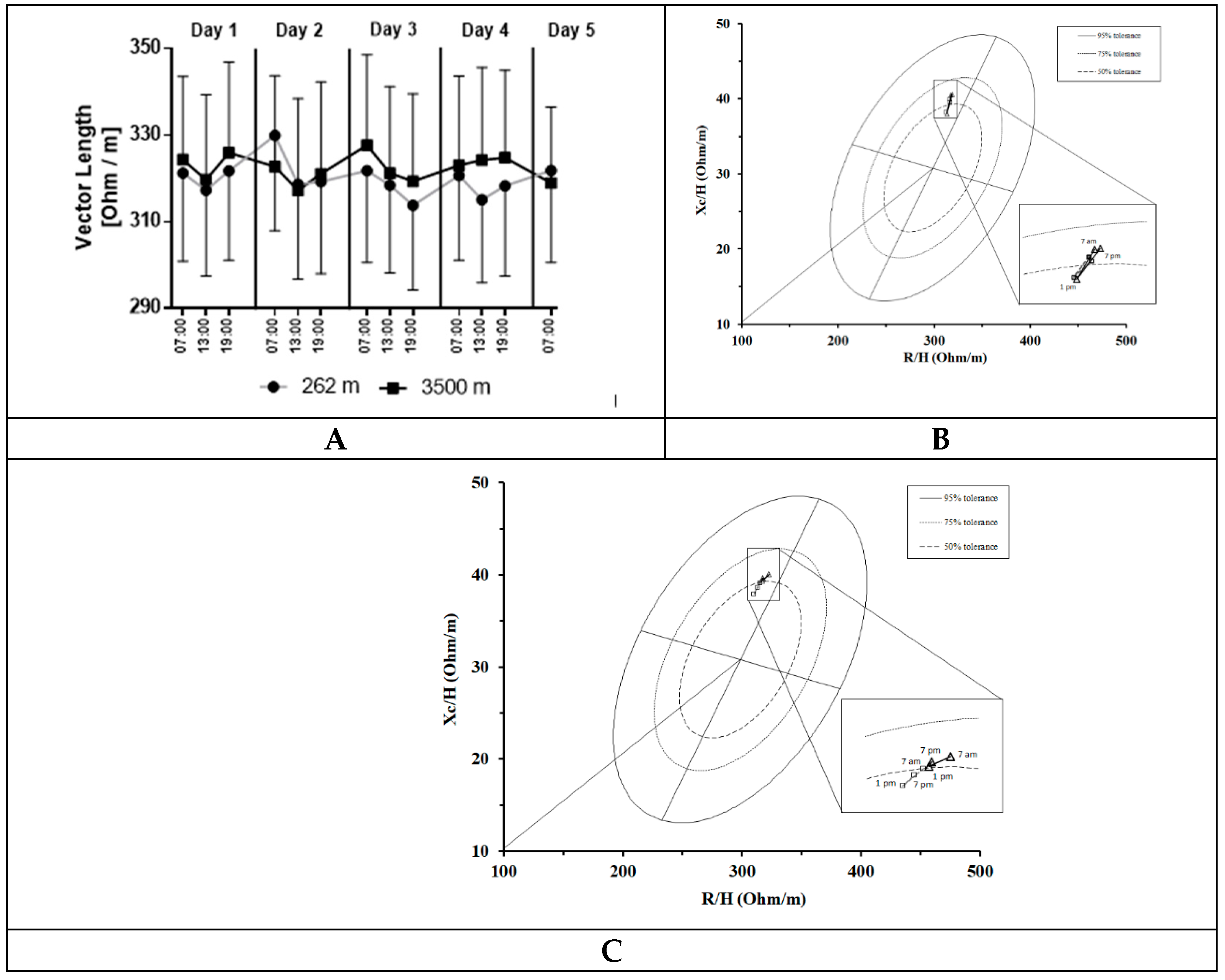{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. BIVA Measurements
2.3. Body Weight Measurements
2.4. Deuterium-Based Total Body Water Measurements
2.5. Statistical Analysis
3. Results
3.1. Circadian Body Fluid Fluctuations at NX and HH
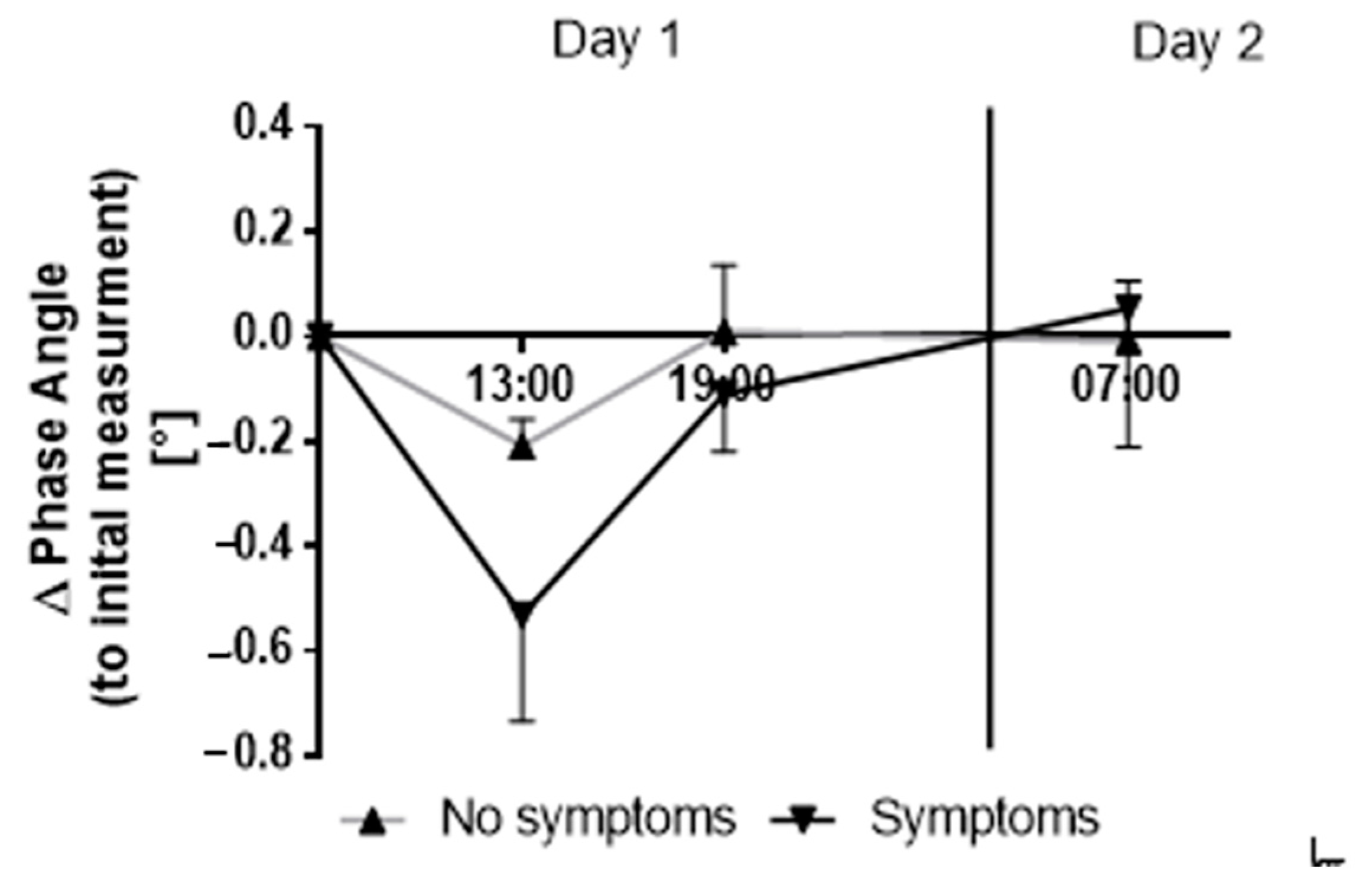
3.2. AMS-Related Clinical Symptoms and BIVA Parameters
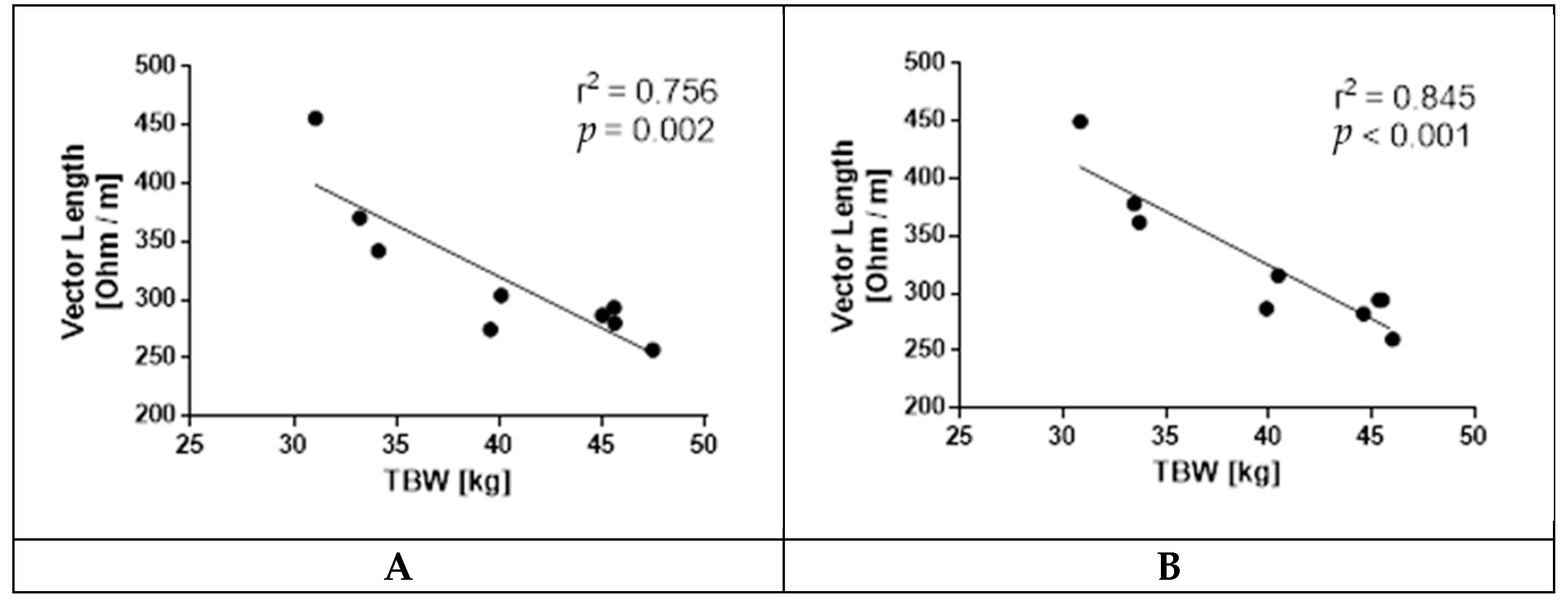
3.3. Vector Length and Deuterium Dilution Total Body Water
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lukaski, H.C.; Moore, M. Bioelectrical Impedance Assessment of Wound Healing. J. Diabetes Sci. Technol. 2012, 6, 209–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piccoli, A.; Rossi, B.; Pillon, L.; Bucciante, G. A new method for monitoring body fluid variation by bioimpedance analysis: The RXc graph. Kidney Int. 1994, 46, 534–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukaski, H.C.; Diaz, N.V.; Talluri, A.; Nescolarde, L. Classification of Hydration in Clinical Conditions: Indirect and Direct Approaches Using Bioimpedance. Nutrients 2019, 11, 809. [Google Scholar] [CrossRef] [Green Version]
- Barbosa-Silva, M.C.G.; Barros, A.J.D. Bioelectrical impedance analysis in clinical practice: A new perspective on its use beyond body composition equations. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 311–317. [Google Scholar] [CrossRef]
- Marini, E.; Campa, F.; Buffa, R.; Stagi, S.; Matias, C.N.; Toselli, S.; Sardinha, L.; Silva, A.M. Phase angle and bioelectrical impedance vector analysis in the evaluation of body composition in athletes. Clin. Nutr. 2020, 39, 447–454. [Google Scholar] [CrossRef]
- Francisco, R.; Matias, C.N.; Santos, D.A.; Campa, F.; Minderico, C.S.; Rocha, P.; Heymsfield, S.B.; Lukaski, H.; Sardinha, L.B.; Silva, A.M. The Predictive Role of Raw Bioelectrical Impedance Parameters in Water Compartments and Fluid Distribution Assessed by Dilution Techniques in Athletes. Int. J. Environ. Res. Public Health 2020, 17, 759. [Google Scholar] [CrossRef] [Green Version]
- Campa, F.; Gatterer, H.; Lukaski, H.; Toselli, S. Stabilizing Bioimpedance-Vector-Analysis Measures With a 10-Minute Cold Shower After Running Exercise to Enable Assessment of Body Hydration. Int. J. Sports Physiol. Perform. 2019, 14, 1006–1009. [Google Scholar] [CrossRef]
- Gatterer, H.; Schenk, K.; Laninschegg, L.; Schlemmer, P.; Lukaski, H.; Burtscher, M. Bioimpedance Identifies Body Fluid Loss after Exercise in the Heat: A Pilot Study with Body Cooling. PLoS ONE 2014, 9, e109729. [Google Scholar] [CrossRef] [PubMed]
- Gatterer, H.; Wille, M.; Faulhaber, M.; Lukaski, H.; Melmer, A.; Ebenbichler, C.; Burtscher, M. Association between Body Water Status and Acute Mountain Sickness. PLoS ONE 2013, 8, e73185. [Google Scholar] [CrossRef] [Green Version]
- Campa, F.; Matias, C.N.; Marini, E.; Heymsfield, S.B.; Toselli, S.; Sardinha, L.; Silva, A.M. Identifying Athlete Body Fluid Changes During a Competitive Season with Bioelectrical Impedance Vector Analysis. Int. J. Sports Physiol. Perform. 2019, 15, 361–367. [Google Scholar] [CrossRef]
- Piccoli, A. Bioelectric Impedance Measurement for Fluid Status Assessment. Contrib. Nephrol. 2010, 164, 143–152. [Google Scholar] [CrossRef] [Green Version]
- Battaglia, Y.; Ullo, I.; Massarenti, S.; Esposito, P.; Prencipe, M.; Ciancio, G.; Provenzano, M.; Fiorini, F.; Andreucci, M.; Storari, A.; et al. Ultrasonography of Quadriceps Femoris Muscle and Subcutaneous Fat Tissue and Body Composition by BIVA in Chronic Dialysis Patients. Nutrients 2020, 12, 1388. [Google Scholar] [CrossRef] [PubMed]
- Buffa, R.; Saragat, B.; Cabras, S.; Rinaldi, A.C.; Marini, E. Accuracy of Specific BIVA for the Assessment of Body Composition in the United States Population. PLoS ONE 2013, 8, e58533. [Google Scholar] [CrossRef] [PubMed]
- Razzera, E.L.; Marcadenti, A.; Rovedder, S.W.; Alves, F.D.; Fink, J.D.S.; Silva, F.M. Parameters of Bioelectrical Impedance Are Good Predictors of Nutrition Risk, Length of Stay, and Mortality in Critically Ill Patients: A Prospective Cohort Study. J. Parenter. Enter. Nutr. 2020, 44, 849–854. [Google Scholar] [CrossRef]
- Del Giorno, R.; Quarenghi, M.; Stefanelli, K.; Rigamonti, A.; Stanglini, C.; De Vecchi, V.; Gabutti, L. Phase angle is associated with length of hospital stay, readmissions, mortality, and falls in patients hospitalized in internal-medicine wards: A retrospective cohort study. Nutrition 2021, 85, 111068. [Google Scholar] [CrossRef]
- Matias, C.N.; Cavaco-Silva, J.; Reis, M.; Campa, F.; Toselli, S.; Sardinha, L.; Silva, A.M. Phase Angle as a Marker of Muscular Strength in Breast Cancer Survivors. Int. J. Environ. Res. Public Health 2020, 17, 4452. [Google Scholar] [CrossRef]
- Pollastri, L.; Lanfranconi, F.; Tredici, G.; Schenk, K.; Burtscher, M.; Gatterer, H. Body fluid status and physical demand during the Giro d’Italia. Res. Sports Med. 2016, 24, 30–38. [Google Scholar] [CrossRef]
- Bongiovanni, T.; Mascherini, G.; Genovesi, F.; Pasta, G.; Iaia, F.M.; Trecroci, A.; Ventimiglia, M.; Alberti, G.; Campa, F. Bioimpedance Vector References Need to Be Period-Specific for Assessing Body Composition and Cellular Health in Elite Soccer Players: A Brief Report. J. Funct. Morphol. Kinesiol. 2020, 5, 73. [Google Scholar] [CrossRef]
- Martins, P.; Teixeira, A.; Guglielmo, L.; Francisco, J.; Silva, D.; Nakamura, F.; Lima, L. Phase Angle Is Related to 10 m and 30 m Sprint Time and Repeated-Sprint Ability in Young Male Soccer Players. Int. J. Environ. Res. Public Health 2021, 18, 4405. [Google Scholar] [CrossRef]
- Campa, F.; Silva, A.M.; Matias, C.N.; Monteiro, C.P.; Paoli, A.; Nunes, J.P.; Talluri, J.; Lukaski, H.; Toselli, S. Body Water Content and Morphological Characteristics Modify Bioimpedance Vector Patterns in Volleyball, Soccer, and Rugby Players. Int. J. Environ. Res. Public Health 2020, 17, 6604. [Google Scholar] [CrossRef] [PubMed]
- Reis, J.F.; Matias, C.N.; Campa, F.; Morgado, J.P.; Franco, P.; Quaresma, P.; Almeida, N.; Curto, D.; Toselli, S.; Monteiro, C.P. Bioimpedance Vector Patterns Changes in Response to Swimming Training: An Ecological Approach. Int. J. Environ. Res. Public Health 2020, 17, 4851. [Google Scholar] [CrossRef] [PubMed]
- Stagi, S.; Doneddu, A.; Mulliri, G.; Ghiani, G.; Succa, V.; Crisafulli, A.; Marini, E. Lower Percentage of Fat Mass among Tai Chi Chuan Practitioners. Int. J. Environ. Res. Public Health 2020, 17, 1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toselli, S.; Marini, E.; Latessa, P.M.; Benedetti, L.; Campa, F. Maturity Related Differences in Body Composition Assessed by Classic and Specific Bioimpedance Vector Analysis among Male Elite Youth Soccer Players. Int. J. Environ. Res. Public Health 2020, 17, 729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campa, F.; Matias, C.; Gatterer, H.; Toselli, S.; Koury, J.C.; Andreoli, A.; Melchiorri, G.; Sardinha, L.B.; Silva, A.M. Classic Bioelectrical Impedance Vector Reference Values for Assessing Body Composition in Male and Female Athletes. Int. J. Environ. Res. Public Health 2019, 16, 5066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campa, F.; Silva, A.M.; Iannuzzi, V.; Mascherini, G.; Benedetti, L.; Toselli, S. The Role of Somatic Maturation on Bioimpedance Patterns and Body Composition in Male Elite Youth Soccer Players. Int. J. Environ. Res. Public Health 2019, 16, 4711. [Google Scholar] [CrossRef] [Green Version]
- Toselli, S.; Badicu, G.; Bragonzoni, L.; Spiga, F.; Mazzuca, P.; Campa, F. Comparison of the Effect of Different Resistance Training Frequencies on Phase Angle and Handgrip Strength in Obese Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 1163. [Google Scholar] [CrossRef] [Green Version]
- Campa, F.; Toselli, S.; Mazzilli, M.; Gobbo, L.; Coratella, G. Assessment of Body Composition in Athletes: A Narrative Review of Available Methods with Special Reference to Quantitative and Qualitative Bioimpedance Analysis. Nutrients 2021, 13, 1620. [Google Scholar] [CrossRef]
- Vermeulen, K.M.; Lopes, M.M.G.D.; Alves, C.X.; Brito, N.J.N.; Almeida, M.D.G.; Leite-Lais, L.; Vale, S.H.L.; Brandão-Neto, J. Bioelectrical Impedance Vector Analysis and Phase Angle on Different Oral Zinc Supplementation in Eutrophic Children: Randomized Triple-Blind Study. Nutrients 2019, 11, 1215. [Google Scholar] [CrossRef] [Green Version]
- Piccoli, A.; Piazza, P.; Noventa, D.; Pillon, L.; Zaccaria, M. A new method for monitoring hydration at high altitude by bioimpedance analysis. Med. Sci. Sports Exerc. 1996, 28, 1517–1522. [Google Scholar] [CrossRef]
- Strapazzon, G.; Pun, M.; Cappello, T.D.; Procter, E.; Lochner, P.; Brugger, H.; Piccoli, A. Total Body Water Dynamics Estimated with Bioelectrical Impedance Vector Analysis and B-Type Natriuretic Peptide After Exposure to Hypobaric Hypoxia: A Field Study. High Alt. Med. Biol. 2017, 18, 384–391. [Google Scholar] [CrossRef]
- West, J.B. The physiologic basis of high-altitude diseases. Ann. Intern. Med. 2004, 141, 789–800. [Google Scholar] [CrossRef] [PubMed]
- Schlittler, M.; Gatterer, H.; Turner, R.; Regli, I.B.; Woyke, S.; Strapazzon, G.; Rasmussen, P.; Kob, M.; Mueller, T.; Goetze, J.P.; et al. Regulation of plasma volume in male lowlanders during four days of exposure to hypobaric hypoxia equivalent to 3,500 m altitude. J. Physiol. 2021, 599, 1083–1096. [Google Scholar] [CrossRef] [PubMed]
- Bosco, G.; Ionadi, A.; Panico, S.; Faralli, F.; Gagliardi, R.; Data, P.; Mortola, J.P. Effects of Hypoxia on the Circadian Patterns in Men. High Alt. Med. Biol. 2003, 4, 305–318. [Google Scholar] [CrossRef] [PubMed]
- Buemi, M.; Campo, S.; Sturiale, A.; Aloisi, C.; Romeo, A.; Nostro, L.; Crascì, E.; Ruello, A.; Manfredini, R.; Floccari, F.; et al. Circadian Rhythm of Hydration in Healthy Subjects and Uremic Patients Studied by Bioelectrical Impedance Analysis. Nephron Physiol. 2007, 106, p39–p44. [Google Scholar] [CrossRef]
- Cugini, P.; Salandri, A.; Petrangeli, C.M.; Capodaglio, P.F.; Giovannini, C. Circadian Rhythms in Human Body Composition. Chrono- Int. 1996, 13, 359–371. [Google Scholar] [CrossRef]
- Castellani, J.W.; Muza, S.R.; Cheuvront, S.N.; Sils, I.V.; Fulco, C.S.; Kenefick, R.W.; Beidleman, B.A.; Sawka, M.N. Effect of hypohydration and altitude exposure on aerobic exercise performance and acute mountain sickness. J. Appl. Physiol. 2010, 109, 1792–1800. [Google Scholar] [CrossRef] [Green Version]
- Basnyat, B.; LeMaster, J.; Litch, J.A. Everest or bust: A cross sectional, epidemiological study of acute mountain sickness at 4243 meters in the Himalayas. Aviat. Space. Environ. Med. 1999, 70, 867–873. [Google Scholar]
- Nerín, M.A.; Palop, J.; Montaño, J.A.; Morandeira, J.R.; Vázquez, M. Acute Mountain Sickness: Influence of Fluid Intake. Wilderness Environ. Med. 2006, 17, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Norris, J.N.; Viirre, E.; Aralis, H.; Sracic, M.K.; Thomas, D.; Gertsch, J.H. High Altitude Headache and Acute Mountain Sickness at Moderate Elevations in a Military Population During Battalion-Level Training Exercises. Mil. Med. 2012, 177, 917–923. [Google Scholar] [CrossRef] [Green Version]
- Richardson, A.; Watt, P.; Maxwell, N. The effect of hypohydration severity on the physiological, psychological and renal hormonal responses to hypoxic exercise. Graefe’s Arch. Clin. Exp. Ophthalmol. 2009, 106, 123–130. [Google Scholar] [CrossRef]
- Loeppky, J.A.; Icenogle, M.V.; Maes, D.; Riboni, K.; Hinghofer-Szalkay, H.; Roach, R.C. Early fluid retention and severe acute mountain sickness. J. Appl. Physiol. 2005, 98, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Westerterp, K.R.; Robach, P.; Wouters, L.; Richalet, J.P. Water balance and acute mountain sickness before and after arrival at high altitude of 4,350 m. J. Appl. Physiol. 1996, 80, 1968–1972. [Google Scholar] [CrossRef] [PubMed]
- Hackett, P.H.; Rennie, D. Rales, peripheral edema, retinal hemorrhage and acute mountain sickness. Am. J. Med. 1979, 67, 214–218. [Google Scholar] [CrossRef]
- Hackett, P.H.; Rennie, D.; Grover, R.F.; Reeves, J.T. Acute mountain sickness and the edemas of high altitude: A common pathogenesis? Respir. Physiol. 1981, 46, 383–390. [Google Scholar] [CrossRef]
- Biollaz, J.; Buclin, T.; Hildebrandt, W.; Décosterd, L.A.; Nussberger, J.; Swenson, E.R.; Bärtsch, P. No renal dysfunction or salt and water retention in acute mountain sickness at 4,559 m among young resting males after passive ascent. J. Appl. Physiol. 2021, 130, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Roach, R.C.; Hackett, P.H.; Oelz, O.; Bärtsch, P.; Luks, A.M.; MacInnis, M.J.; Baillie, J.K.; Achatz, E.; Albert, E.; Andrews, J.S.; et al. The 2018 Lake Louise Acute Mountain Sickness Score. High Alt. Med. Biol. 2018, 19, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Gatterer, H.; Schenk, K.; Burtscher, M.; Lukaski, H. Assessment of Human Body Composition Methods and Limitations. In Body Composition; CRC Press: Boca Raton, FL, USA, 2017; pp. 13–26. [Google Scholar]
- Cornejo-Pareja, I.; Vegas-Aguilar, I.M.; García-Almeida, J.M.; Bellido-Guerrero, D.; Talluri, A.; Lukaski, H.; Tinahones, F.J. Phase angle and standardized phase angle from bioelectrical impedance measurements as a prognostic factor for mortality at 90 days in patients with COVID-19: A longitudinal cohort study. Clin. Nutr. 2021, in press. [Google Scholar] [CrossRef]
- Schoeller, D.A.; Van Santen, E.; Peterson, D.W.; Dietz, W.; Jaspan, J.; Klein, P.D. Total body water measurement in humans with 18O and 2H labeled water. Am. J. Clin. Nutr. 1980, 33, 2686–2693. [Google Scholar] [CrossRef]
- Piccoli, A.; Nigrelli, S.; Caberlotto, A.; Bottazzo, S.; Rossi, B.; Pillon, L.; Maggiore, Q. Bivariate normal values of the bioe-lectrical impedance vector in adult and elderly populations. Am. J. Clin. Nutr. 1995, 61, 269–270. [Google Scholar] [CrossRef]
- Evans, W.; McClagish, H.; Trudgett, C. Factors affecting the In vivo precision of bioelectrical impedance analysis. Appl. Radiat. Isot. 1998, 49, 485–487. [Google Scholar] [CrossRef]
- Slinde, F.; Bark, A.; Jansson, J.; Rossander-Hulthén, L. Bioelectrical impedance variation in healthy subjects during 12 h in the supine position. Clin. Nutr. 2003, 22, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Dünnwald, T.; Gatterer, H.; Faulhaber, M.; Arvandi, M.; Schobersberger, W. Body Composition and Body Weight Changes at Different Altitude Levels: A Systematic Review and Meta-Analysis. Front. Physiol. 2019, 10, 430. [Google Scholar] [CrossRef] [PubMed]
- Ermolao, A.; Bergamin, M.; Rossi, A.C.; Carbonare, L.D.; Zaccaria, M. Cardiopulmonary Response and Body Composition Changes after Prolonged High Altitude Exposure in Women. High Alt. Med. Biol. 2011, 12, 357–369. [Google Scholar] [CrossRef]
- Sawka, M.N.; Burke, L.M.; Eichner, E.R.; Maughan, R.J.; Montain, S.J.; Stachenfeld, N.S. American College of Sports Medicine position stand. Exercise and fluid replacement. Med. Sci. Sports Exerc. 2007, 39, 377–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, M.M.; Sareban, M.; Bärtsch, P. Acute mountain sickness: Do different time courses point to different pathophysiological mechanisms? J. Appl. Physiol. 2020, 128, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.; Watt, P.; Maxwell, N. Hydration and the Physiological Responses to Acute Normobaric Hypoxia. Wilderness Environ. Med. 2009, 20, 212–220. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Regli, I.B.; Turner, R.; Woyke, S.; Rauch, S.; Brugger, H.; Gatterer, H. Bioelectrical Impedance Vector Analysis: A Valuable Tool to Monitor Daily Body Hydration Dynamics at Altitude. Int. J. Environ. Res. Public Health 2021, 18, 5455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105455
Regli IB, Turner R, Woyke S, Rauch S, Brugger H, Gatterer H. Bioelectrical Impedance Vector Analysis: A Valuable Tool to Monitor Daily Body Hydration Dynamics at Altitude. International Journal of Environmental Research and Public Health. 2021; 18(10):5455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105455
Chicago/Turabian StyleRegli, Ivo B., Rachel Turner, Simon Woyke, Simon Rauch, Hermann Brugger, and Hannes Gatterer. 2021. "Bioelectrical Impedance Vector Analysis: A Valuable Tool to Monitor Daily Body Hydration Dynamics at Altitude" International Journal of Environmental Research and Public Health 18, no. 10: 5455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105455