
Impacts of Dual-Income Household Rate on Suicide Mortalities in Japan


Abstract
:1. Introduction
2. Materials and Methods
2.1. Dependent Variables
2.2. Independent Variable and Covariates
2.3. Statistical Analysis
3. Results
3.1. Effects of Houeshold and Social Factors on SDR between 2009 and 2017
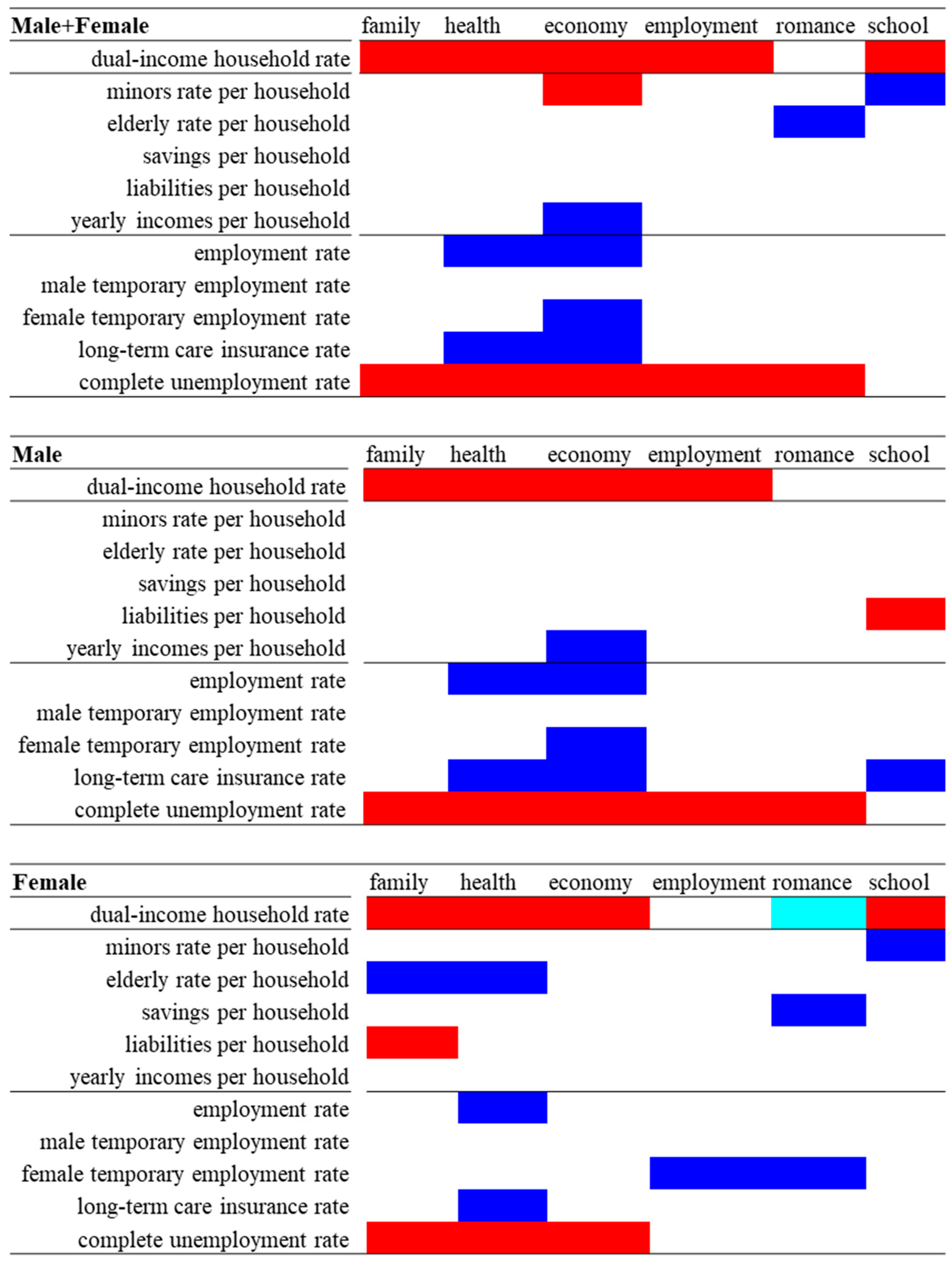
3.2. Effects of Houeshold and Social and Employment Factors on Suicide Mortalities Caused by Six Major Motives between 2009 and 2017
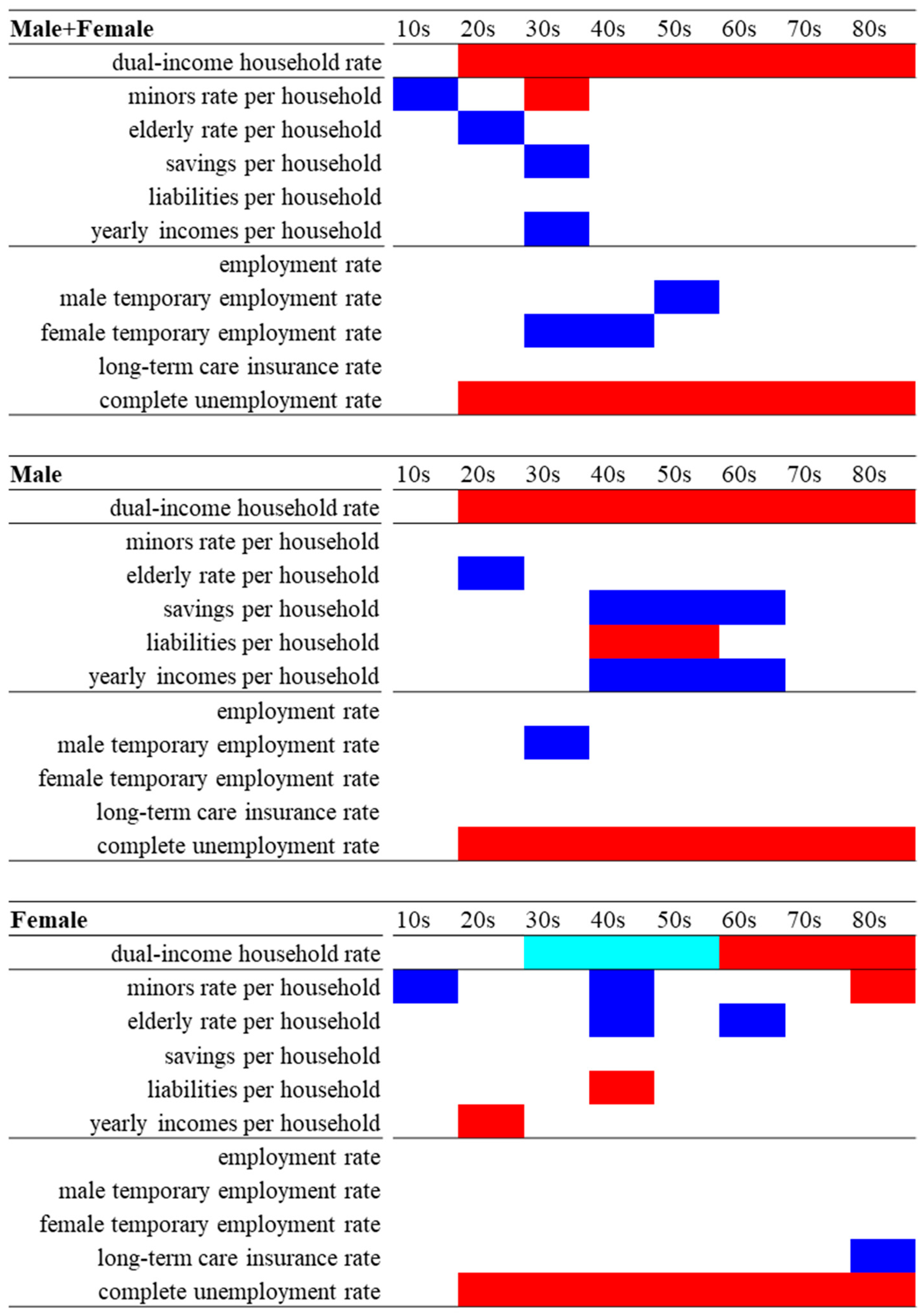
3.3. Effects of Household Structure and Social and Employment Factors on Age-Dependent Suicide Mortalities between 2009 and 2017
3.4. Effects of Household Factors on Suicide Mortalities of School-Age Populations between 2009 and 2017
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kato, R.; Okada, M. Can financial support reduce suicide mortality rates? Int. J. Environ. Res. Public Health 2019, 16, 4797. [Google Scholar] [CrossRef] [Green Version]
- Okada, M.; Hasegawa, T.; Kato, R.; Shiroyama, T. Analysing regional unemployment rates, gdp per capita and financial support for regional suicide prevention programme on suicide mortality in japan using governmental statistical data. BMJ Open 2020, 10, e037537. [Google Scholar] [CrossRef]
- Nakano, T.; Hasegawa, T.; Okada, M. Analysing the impacts of financial support for regional suicide prevention programmes on suicide mortality caused by major suicide motives in japan using statistical government data. Int. J. Environ. Res. Public Health 2021, 18, 3414. [Google Scholar] [CrossRef] [PubMed]
- Mattei, G.; Pistoresi, B.; De Vogli, R. Impact of the economic crises on suicide in italy: The moderating role of active labor market programs. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 201–208. [Google Scholar] [CrossRef]
- Mattei, G.; Pistoresi, B. Unemployment and suicide in italy: Evidence of a long-run association mitigated by public unemployment spending. Eur. J. Health Econ. HEPAC Health Econ. Prev. Care 2019, 20, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Cylus, J.; Glymour, M.M.; Avendano, M. Do generous unemployment benefit programs reduce suicide rates? A state fixed-effect analysis covering 1968–2008. Am. J. Epidemiol. 2014, 180, 45–52. [Google Scholar] [CrossRef]
- Rambotti, S. Is there a relationship between welfare-state policies and suicide rates? Evidence from the u.S. States, 2000–2015. Soc. Sci. Med. 2020, 246, 112778. [Google Scholar] [CrossRef] [Green Version]
- Mejias-Martin, Y.; Luna Del Castillo, J.D.; Rodriguez-Mejias, C.; Marti-Garcia, C.; Valencia-Quintero, J.P.; Garcia-Caro, M.P. Factors associated with suicide attempts and suicides in the general population of Andalusia (Spain). Int. J. Environ. Res. Public Health 2019, 16, 4496. [Google Scholar] [CrossRef] [Green Version]
- Schrijvers, D.L.; Bollen, J.; Sabbe, B.G. The gender paradox in suicidal behavior and its impact on the suicidal process. J. Affect. Disord. 2012, 138, 19–26. [Google Scholar] [CrossRef]
- Kumar, C.S.; Mohan, R.; Ranjith, G.; Chandrasekaran, R. Characteristics of high intent suicide attempters admitted to a general hospital. J. Affect. Disord. 2006, 91, 77–81. [Google Scholar] [CrossRef]
- Canetto, S.S.; Sakinofsky, I. The gender paradox in suicide. Suicide Life Threat. Behav. 1998, 28, 1–23. [Google Scholar] [PubMed]
- Van Orden, K.A.; Witte, T.K.; Cukrowicz, K.C.; Braithwaite, S.R.; Selby, E.A.; Joiner, T.E., Jr. The interpersonal theory of suicide. Psychol. Rev. 2010, 117, 575–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiratori, Y.; Tachikawa, H.; Nemoto, K.; Endo, G.; Aiba, M.; Matsui, Y.; Asada, T. Network analysis for motives in suicide cases: A cross-sectional study. Psychiatry Clin. Neurosci. 2014, 68, 299–307. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. White Paper on the Labour Economy. Available online: https://www.mhlw.go.jp/english/wp/l-economy/index.html (accessed on 1 May 2021).
- Thompson, C.A.; Beauvais, L.L.; Lyness, K.S. When work–family benefits are not enough: The influence of work–family culture on benefit utilization, organizational attachment, and work–family conflict. J. Vocat. Behav. 1999, 54, 392–415. [Google Scholar] [CrossRef]
- Cabinet Office. The Fifth Basic Plan for Gender Equality. Available online: https://www.gender.go.jp/english_contents/about_danjo/whitepaper/pdf/5th_bpg.pdf (accessed on 1 May 2021).
- Lo Presti, A.; Molino, M.; Emanuel, F.; Landolfi, A.; Ghislieri, C. Work-family organizational support as a predictor of work-family conflict, enrichment, and balance: Crossover and spillover effects in dual-income couples. Eur. J. Psychol. 2020, 16, 62–81. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health, Labour and Welfare. Basic Data on Suicide in the Region. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000140901.html (accessed on 18 November 2020).
- Statistics Bureau of the Ministry of Internal Affairs and Communications. Surveys of Population, Population Change and the Number of Households Based on the Basic Resident Registration. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&toukei=00200241&tstat=000001039591 (accessed on 1 May 2021).
- Kawaguchi, H.; Koike, S. Association between the density of physicians and suicide rates in japan: Nationwide ecological study using a spatial bayesian model. PLoS ONE 2016, 11, e0148288. [Google Scholar] [CrossRef]
- Ahmad, O.B.; Boschi-Pinto, C.; Lopez, A.D.; Murray, C.J.; Lozano, R.; Inoue, M. Age Standardization of Rates: A New Who Standard; World Health Organization: Geneva, Switzerland, 2001; Volume 9. [Google Scholar]
- Statistics Bureau of the Ministry of Internal Affairs and Communications. Family Income and Expenditure Survey. Available online: https://www.e-stat.go.jp/en/stat-search/files?page=1&layout=normal&toukei=00200561 (accessed on 1 May 2021).
- Statistics Bureau of the Ministry of Internal Affairs and Communications. Labour Force Survey. Available online: https://www.e-stat.go.jp/stat-search?page=1&query=%E5%8A%B4%E5%83%8D%E5%8A%9B%E8%AA%BF%E6%9F%BB&metadata=1&data=1 (accessed on 1 May 2021).
- Statistics Bureau of the Ministry of Internal Affairs and Communications. System of Social and Demographic Statistics. Available online: https://www.e-stat.go.jp/stat-search?page=1&query=%E7%9C%8C%E6%B0%91%E7%B5%8C%E6%B8%88%E8%A8%88%E7%AE%97 (accessed on 1 May 2021).
- Statistics Bureau of the Ministry of Internal Affairs and Communications. Employment Status Survey. Available online: https://www.e-stat.go.jp/en/stat-search/files?page=1&toukei=00200532&tstat=000001116777 (accessed on 1 May 2021).
- Statistics Bureau of the Ministry of Internal Affairs and Communications. Population Census. Available online: https://www.e-stat.go.jp/en/stat-search/files?page=1&layout=normal&toukei=00200521&survey=%E5%9B%BD%E5%8B%A2%E8%AA%BF%E6%9F%BB&result_page=1 (accessed on 1 May 2021).
- Hunt, K.; Sweeting, H.; Keoghan, M.; Platt, S. Sex, gender role orientation, gender role attitudes and suicidal thoughts in three generations. A general population study. Soc. Psychiatry Psychiatr. Epidemiol. 2006, 41, 641–647. [Google Scholar] [CrossRef]
- Fassberg, M.M.; van Orden, K.A.; Duberstein, P.; Erlangsen, A.; Lapierre, S.; Bodner, E.; Canetto, S.S.; De Leo, D.; Szanto, K.; Waern, M. A systematic review of social factors and suicidal behavior in older adulthood. Int. J. Environ. Res. Public Health 2012, 9, 722–745. [Google Scholar] [CrossRef] [Green Version]
- Cano-Montalbán, I.; Quevedo-Blasco, R. Sociodemographic variables most associated with suicidal behaviour and suicide methods in europe and america. A systematic review. Eur. J. Psychol. Appl. Leg. Context 2018, 10, 15–25. [Google Scholar] [CrossRef] [Green Version]
- von Brachel, R.; Teismann, T.; Feider, L.; Margraf, J. Suicide ideation as a predictor of treatment outcomes in cognitive-behavioral therapy for unipolar mood disorders. Int. J. Clin. Health Psychol. 2019, 19, 80–84. [Google Scholar] [CrossRef]
- Teismann, T.; Brailovskaia, J.; Margraf, J. Positive mental health, positive affect and suicide ideation. Int. J. Clin. Health Psychol. 2019, 19, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, S.L.; Uddin, R.; Brady, M.; Batchelor, S.; Ross, V.; Spence, S.H.; Watling, D.; Kolves, K. Systematic review: The state of research into youth helplines. J. Am. Acad. Child. Adolesc. Psychiatry 2020. [Google Scholar] [CrossRef] [PubMed]
- Ingram, S.; Ringle, J.L.; Hallstrom, K.; Schill, D.E.; Gohr, V.M.; Thompson, R.W. Coping with crisis across the lifespan: The role of a telephone hotline. J. Child. Fam. Stud. 2008, 17, 663–674. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. 2020 White Paper on Suicide Prevention. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/jisatsuhakusyo2020.html (accessed on 14 November 2020).
- Kil, H.; Aitken, M.; Henry, S.; Hoxha, O.; Rodak, T.; Bennett, K.; Andrade, B.F. Transdiagnostic associations among parental causal locus attributions, child behavior and psychosocial treatment outcomes: A systematic review. Clin. Child. Fam. Psychol. Rev. 2021, 24, 267–293. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Survey Study on the Actual Conditions of Young Carers. Available online: https://elaws.e-gov.go.jp/search/elawsSearch/elaws_search/lsg0500/detail?lawId=501AC1000000032_20190912_000000000000000&openerCode=1 (accessed on 1 May 2021).
- Statistics Bureau of the Ministry of Internal Affairs and Communications. Comprehensive Survey of LIVING conditions. Available online: https://www.e-stat.go.jp/en/statistics/00450061 (accessed on 1 May 2021).
- Greenhaus, J.H.; Beutell, N.J. Sources of conflict between work and family roles. Acad. Manag. Rev. 1985, 10, 76–88. [Google Scholar] [CrossRef]
- Greenhaus, J.H.; Powell, G.N. When work and family are allies: A theory of work-family enrichment. Acad. Manag. Rev. 2006, 31, 72–92. [Google Scholar] [CrossRef]
- Disch, J.; Barnsteiner, J. Qsen in an amazon world. Am. J. Nurs. 2021, 121, 40–46. [Google Scholar] [CrossRef]
- ter Hoeven, C.L.; van Zoonen, W. Flexible work designs and employee well-being: Examining the effects of resources and demands. New Technol. Work Employ. 2015, 30, 237–255. [Google Scholar] [CrossRef] [Green Version]
- Carlson, D.S.; Grzywacz, J.G.; Zivnuska, S. Is work-family balance more than conflict and enrichment? Hum. Relat. 2009, 62, 1459. [Google Scholar] [CrossRef] [Green Version]
- Grzywacz, J.G.; Carlson, D.S. Conceptualizing work—Family balance: Implications for practice and research. Adv. Dev. Hum. Resour. 2007, 9, 455–471. [Google Scholar] [CrossRef]
- Husky, M.M.; Guignard, R.; Beck, F.; Michel, G. Risk behaviors, suicidal ideation and suicide attempts in a nationally representative french sample. J. Affect. Disord. 2013, 151, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Faria, Y.d.O.; Gandolfi, L.; Moura, L.B.A. Prevalência de comportamentos de risco em adulto jovem e universitário. Acta Paul. De Enferm. 2014, 27, 591–595. [Google Scholar] [CrossRef] [Green Version]
- Fung, Y.-L.; Chan, Z.C.Y. A systematic review of suicidal behaviour in old age: A gender perspective. J. Clin. Nurs. 2011, 20, 2109–2124. [Google Scholar] [CrossRef] [PubMed]
- Uggla, C.; Mace, R. Someone to live for: Effects of partner and dependent children on preventable death in a population wide sample from northern ireland. Evol. Hum. Behav. 2015, 36, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S. Reproductive technologies as population control: How pronatalist policies harm reproductive health in South Korea. Sex. Reprod Health Matters 2019, 27, 1610278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2017 Population and Fertility Collaborators. Population and fertility by age and sex for 195 countries and territories, 1950–2017: A systematic analysis for the global burden of disease study 2017. Lancet 2018, 392, 1995–2051. [Google Scholar]
- Su, Z.; Hu, Z.; Peng, X. The impact of changes in China’s family patterns on family pension functions. Int. J. Health Plann Manag. 2017, 32, 351–362. [Google Scholar] [CrossRef]
- Forum, W.E. Global Gender Gap Report 2021. Available online: https://www.weforum.org/reports/global-gender-gap-report-2021 (accessed on 1 May 2021).
- World Health Organization. Suicide Rates (per 100,000 Population). Global Health Observatory. Available online: https://www.who.int/gho/mental_health/suicide_rates/en/ (accessed on 1 December 2019).




{kind=link}
{kind=link}
{kind=link}
| Factors | Male + Female | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | SE | p value | β | SE | p value | β | SE | p value | |
| Model_1 | |||||||||
| dual-income household rate | 0.158 | 0.069 | 0.017 ** | 0.169 | 0.110 | 0.009 ** | 0.094 | 0.055 | 0.274 |
| Model_2 | |||||||||
| dual-income household rate | 0.405 | 0.076 | 0.000 ** | 0.399 | 0.108 | 0.000 ** | 0.363 | 0.058 | 0.000 ** |
| minors rate per household | 0.044 | 0.034 | 0.126 | 0.035 | 0.058 | 0.236 | 0.051 | 0.025 | 0.213 |
| elderly rate per household | −0.057 | 0.056 | 0.070 | −0.038 | 0.091 | 0.238 | −0.091 | 0.044 | 0.020 * |
| savings per household | −0.042 | 0.000 | 0.176 | −0.073 | 0.001 | 0.034 * | 0.033 | 0.000 | 0.286 |
| liabilities per household | 0.033 | 0.002 | 0.373 | 0.052 | 0.004 | 0.171 | 0.025 | 0.000 | 0.527 |
| yearly incomes per household | −0.051 | 0.001 | 0.049 * | −0.082 | 0.001 | 0.006 ** | −0.004 | 0.002 | 0.912 |
| employment rate | −0.087 | 0.118 | 0.231 | −0.106 | 0.191 | 0.202 | −0.015 | 0.080 | 0.491 |
| male temporary employment rate | −0.033 | 0.331 | 0.520 | −0.045 | 0.581 | 0.477 | −0.017 | 0.227 | 0.768 |
| female temporary employment rate | −0.104 | 0.163 | 0.055 | −0.101 | 0.286 | 0.107 | −0.096 | 0.094 | 0.066 |
| long-term care insurance rate | −0.155 | 0.015 | 0.034 * | −0.122 | 0.022 | 0.071 | −0.062 | 0.010 | 0.383 |
| complete unemployment rate | 0.719 | 0.199 | 0.000 ** | 0.665 | 0.286 | 0.000 ** | 0.704 | 0.156 | 0.000 ** |
| 10s | |||||||||
| Factors | Male + Female | Male | Female | ||||||
| Model_3 | β | SE | p value | β | SE | p value | β | SE | p value |
| dual-income household rate | 0.055 | 0.020 | 0.321 | 0.103 | 0.028 | 0.117 | −0.056 | 0.019 | 0.720 |
| minors rate per household | −0.185 | 0.022 | 0.008 * | −0.147 | 0.040 | 0.063 | −0.136 | 0.017 | 0.007 * |
| elderly rate per household | −0.120 | 0.035 | 0.160 | −0.151 | 0.057 | 0.061 | 0.004 | 0.035 | 0.839 |
| savings per household | −0.036 | 0.000 | 0.672 | 0.011 | 0.000 | 0.882 | −0.078 | 0.000 | 0.287 |
| liabilities per household | −0.027 | 0.000 | 0.713 | −0.016 | 0.001 | 0.816 | −0.026 | 0.000 | 0.674 |
| yearly incomes per household | 0.072 | 0.001 | 0.453 | 0.065 | 0.002 | 0.423 | 0.080 | 0.001 | 0.369 |
| School-related motive | |||||||||
| Factors | Male + Female | Male | Female | ||||||
| Model_3 | β | SE | p value | β | SE | p value | β | SE | p value |
| dual-income household rate | 0.175 | 0.004 | 0.039 * | 0.120 | 0.005 | 0.164 | 0.135 | 0.002 | 0.012 * |
| minors rate per household | −0.117 | 0.003 | 0.034 * | 0.024 | 0.006 | 0.724 | −0.108 | 0.002 | 0.023 * |
| elderly rate per household | −0.111 | 0.005 | 0.092 | 0.032 | 0.007 | 0.495 | −0.093 | 0.006 | 0.229 |
| savings per household | 0.112 | 0.000 | 0.131 | 0.196 | 0.000 | 0.057 | −0.049 | 0.000 | 0.298 |
| liabilities per household | 0.044 | 0.000 | 0.416 | 0.087 | 0.000 | 0.129 | 0.152 | 0.000 | 0.071 |
| yearly incomes per household | 0.073 | 0.000 | 0.334 | −0.071 | 0.000 | 0.461 | −0.034 | 0.000 | 0.659 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamoto, M.; Nakagawa, T.; Murata, M.; Okada, M. Impacts of Dual-Income Household Rate on Suicide Mortalities in Japan. Int. J. Environ. Res. Public Health 2021, 18, 5670. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115670
Nakamoto M, Nakagawa T, Murata M, Okada M. Impacts of Dual-Income Household Rate on Suicide Mortalities in Japan. International Journal of Environmental Research and Public Health. 2021; 18(11):5670. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115670
Chicago/Turabian StyleNakamoto, Misaki, Takatoshi Nakagawa, Masahiko Murata, and Motohiro Okada. 2021. "Impacts of Dual-Income Household Rate on Suicide Mortalities in Japan" International Journal of Environmental Research and Public Health 18, no. 11: 5670. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115670