
Comparison of Generalized Anxiety and Sleep Disturbance among Frontline and Second-Line Healthcare Workers during the COVID-19 Pandemic


Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Design and Settings
2.2. Selection of Healthcare Workers and Data Collection
2.3. Inclusion and Exclusion Criteria
2.4. Questionnaire
2.5. General Anxiety Disorder-7 (GAD-7) and Pittsburgh Sleep Quality Index (PSQI) Scales
2.6. Statistical Analysis
2.7. Ethics Statement
3. Results
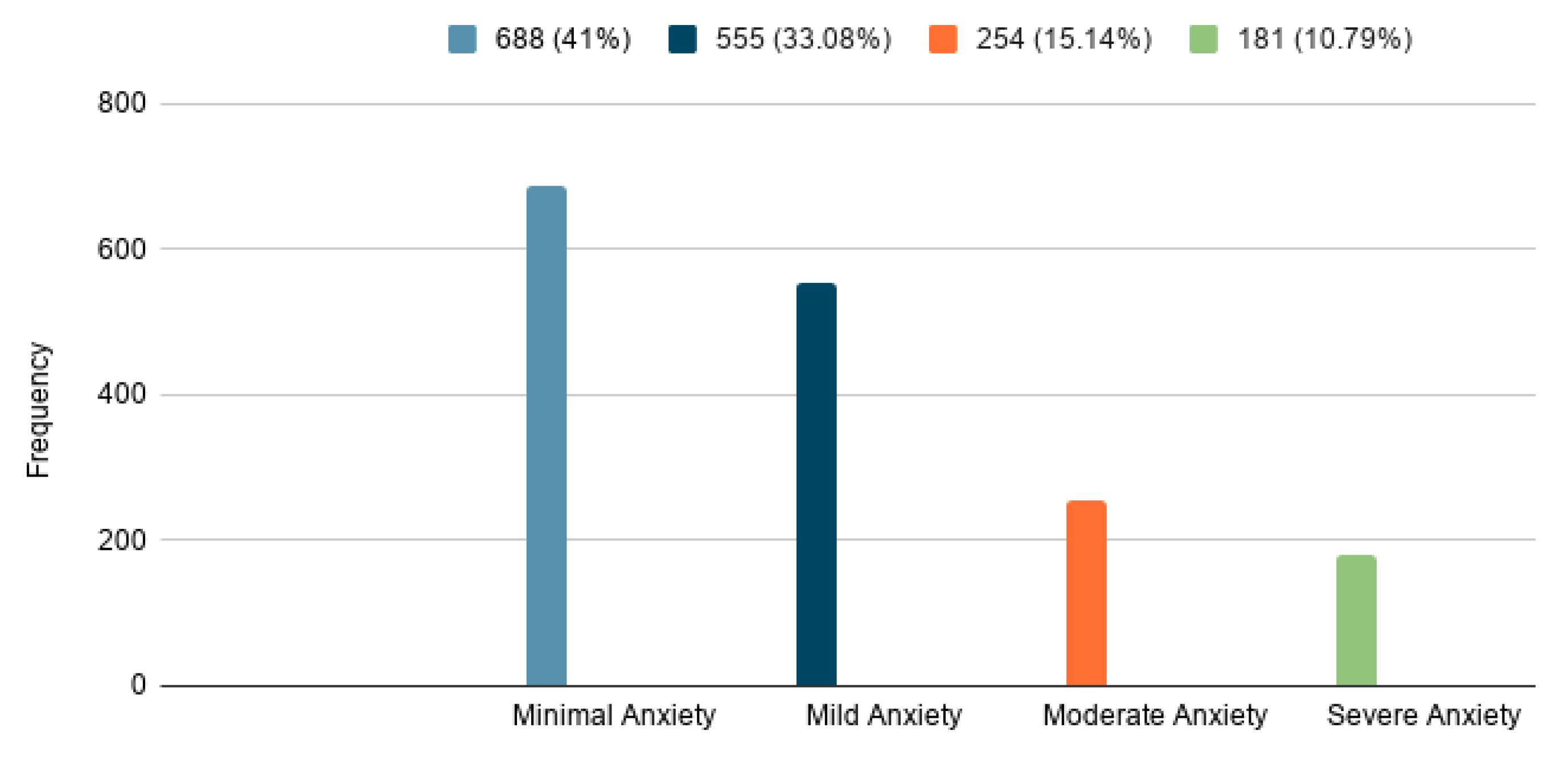
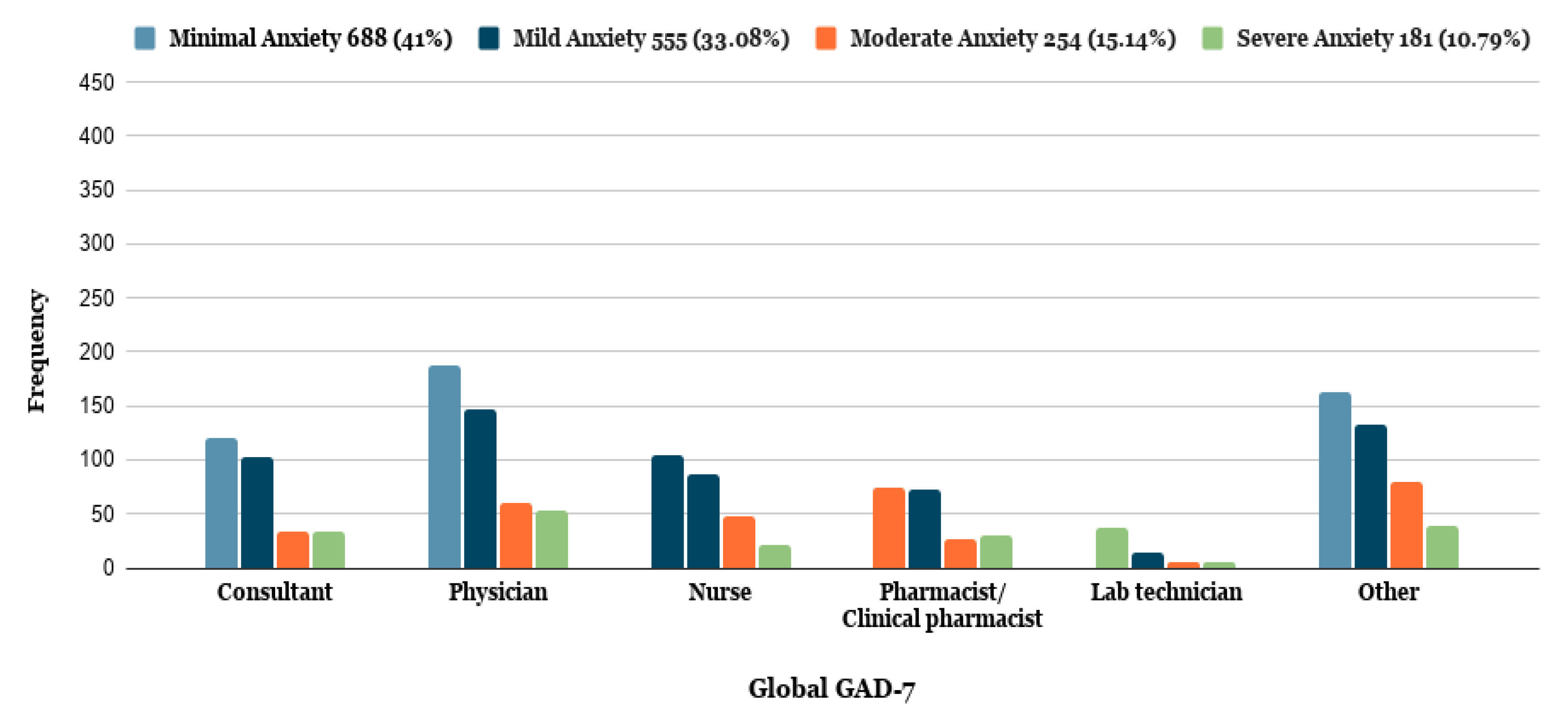
3.1. Generalized Anxiety Disorder-7 (GAD-7)
3.2. Anxiety Levels between Frontline and Second-Line Healthcare Workers
3.3. Anxiety Levels and COVID-19 Involvement
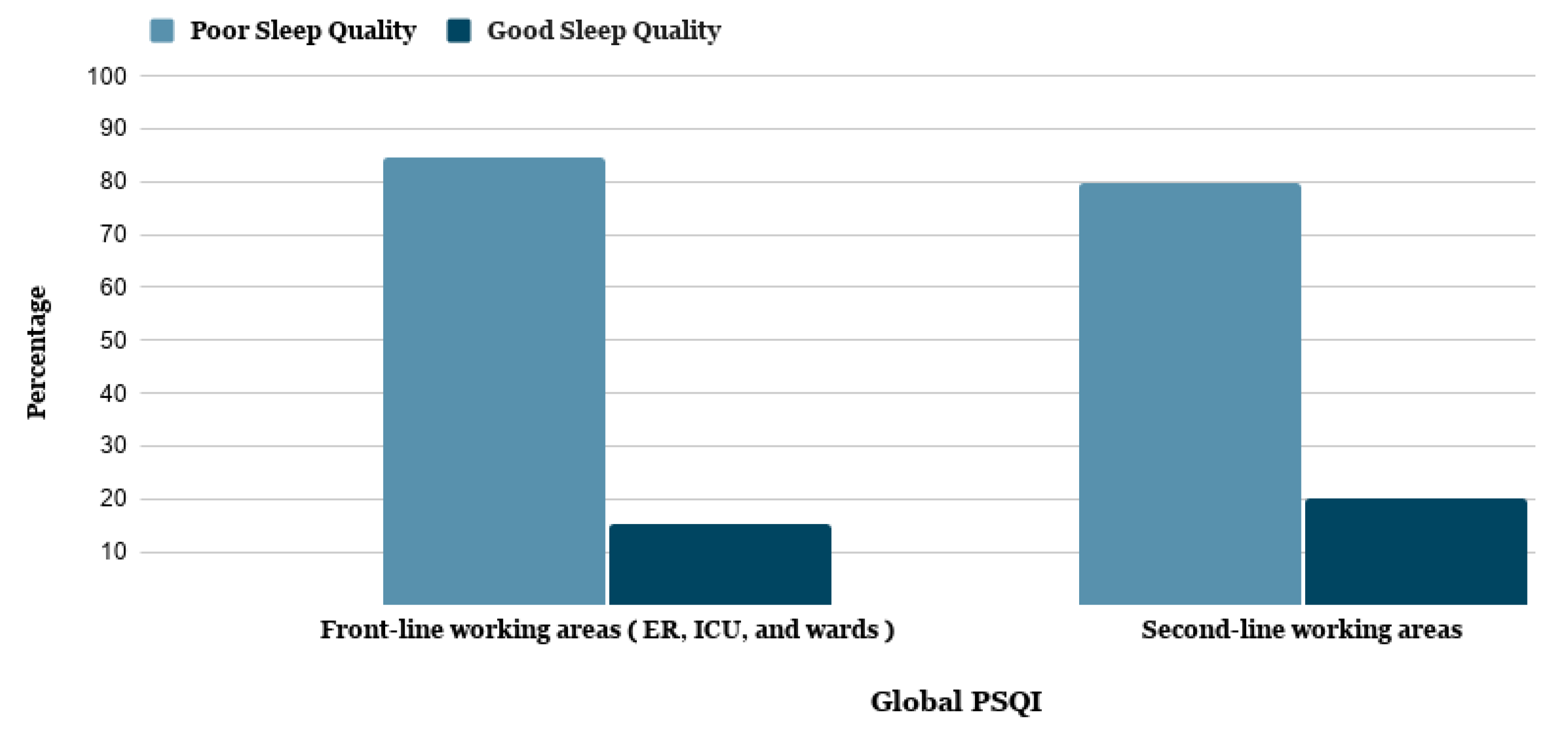
3.4. Pittsburgh Sleep Quality Index (PSQI)
3.5. Sleep Quality and COVID-19 Involvement
4. Discussion
5. Study Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meo, S.A.; Bukhari, I.A.; Akram, J.; Meo, A.S.; Klonoff, D.C. COVID-19 vaccines: Comparison of biological, pharmacological characteristics and adverse effects of Pfizer/BioNTech and Moderna Vaccines. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1663–1669. [Google Scholar] [CrossRef] [PubMed]
- Meo, S.A.; Zaidi, S.Z.A.; Shang, T.; Zhang, J.Y.; Al-Khlaiwi, T.; Bukhari, I.A.; Akram, J.; Klonoff, D.C. Biological, molecular and pharmacological characteristics of chloroquine, hydroxychloroquine, convalescent plasma, and remdesivir for COVID-19 pandemic: A comparative analysis. J. King Saud Univ. Sci. 2020, 32, 3159–3166. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 30 April 2021).
- Ge, Y.; Sun, S.; Shen, Y. Estimation of case-fatality rate in COVID-19 patients with hypertension and diabetes mellitus in the New York state: A preliminary report. Epidemiol. Infect. 2021, 149, e14. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Nayan, N.; Nair, R.; Kumar, K.; Joshi, A.; Sharma, S.; Singh, J.; Kapoor, R. Diabetes Mellitus and Hypertension Increase Risk of Death in Novel Corona Virus Patients Irrespective of Age: A Prospective Observational Study of Co-morbidities and COVID-19 from India. SN Compr. Clin. Med. 2021, 3, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Lima-Martínez, M.M.; Carrera, B.C.; Madera-Silva, M.D.; Marín, W.; Contreras, M. COVID-19 and diabetes: A bidirectional relationship. Clin. Investig. Arterioscler. 2020. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Meo, S.A.; Abukhalaf, A.A.; Alomar, A.A.; Sumaya, O.Y.; Sami, W.; Shafi, K.M.; Meo, A.S.; Usmani, A.M.; Akram, J. Effect of heat and humidity on the incidence and mortality due to COVID-19 pandemic in European countries. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 9216–9225. [Google Scholar] [CrossRef] [PubMed]
- Meo, S.A.; Abukhalaf, A.A.; Alomar, A.A.; Al-Beeshi, I.Z.; Alhowikan, A.; Shafi, K.M.; Meo, A.S.; Usmani, A.M.; Akram, J. Climate and COVID-19 pandemic: Effect of heat and humidity on the incidence and mortality in world’s top ten hottest and top ten coldest countries. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 8232–8238. [Google Scholar] [CrossRef] [PubMed]
- Meo, S.A.; Abukhalaf, A.A.; Alomar, A.A.; Alessa, O.M.; Sami, W.; Klonoff, D.C. Effect of environmental pollutants PM-2.5, carbon monoxide, and ozone on the incidence and mortality of SARS-COV-2 infection in ten wildfire affected counties in California. Sci. Total. Environ. 2021, 757, 143948. [Google Scholar] [CrossRef]
- Meo, S.A.; Abukhalaf, A.A.; Sami, W.; Hoang, T.D. Effect of environmental pollution PM2.5, carbon monoxide, and ozone on the incidence and mortality due to SARS-CoV-2 infection in London, United Kingdom. J. King Saud Univ. Sci. 2021, 33, 101373. [Google Scholar] [CrossRef]
- Li, W.; Yang, Y.; Liu, Z.H. Progression of Mental Health Services during the COVID-19 Outbreak in China. Int. J. Biol. Sci. 2020, 16, 1732–1738. [Google Scholar] [CrossRef] [Green Version]
- Meo, S.A.; Abukhalaf, A.A.; Alomar, A.A.; Sattar, K.; Klonoff, D.C. COVID-19 Pandemic: Impact of Quarantine on Medical Students’ Mental Wellbeing and Learning Behaviors. Pak. J. Med. Sci. 2020, 36, S43–S48. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.B.; Butcher, F. Doctors during the COVID-19 pandemic: What are their duties and what is owed to them? J. Med. Ethics 2021, 47, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.T.; Zhao, Y.J.; Liu, Z.H.; Li, X.H.; Zhao, N.; Cheung, T.; Ng, C.H. The COVID-19 outbreak and psychiatric hospitals in China: Managing challenges through mental health service reform. Int. J. Biol. Sci. 2020, 16, 1741–1744. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.H.; Zhao, Y.J.; Wang, C.; Zhang, Q.; Yu, H.Y.; Cheung, T.; Hall, B.J.; An, F.R.; Xiang, Y.T. Depression and its relationship with quality of life in frontline psychiatric clinicians during the COVID-19 pandemic in China: A national survey. Int. J. Biol. Sci. 2021, 17, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Mohd Noor, N.; Che Yusof, R.; Yacob, M.A. Anxiety in Frontline and Non-Frontline Healthcare Providers in Kelantan, Malaysia. Int. J. Environ. Res. Public Health 2021, 18, 861. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1099. [Google Scholar] [CrossRef] [Green Version]
- IBM Support. Using (SPSS) Software Version 26.0 for Mac. Available online: https://www.ibm.com/support/pages/downloading-ibm-spss-statistics-26 (accessed on 12 July 2020).
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Alsulimani, L.K.; Farhat, A.M.; Borah, R.A.; AlKhalifah, J.A.; Alyaseen, S.M.; Alghamdi, S.M.; Bajnaid, M.J. Health care worker burnout during the COVID-19 pandemic: A cross-sectional survey study in Saudi Arabia. Saudi Med. J. 2021, 42, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Khazaie, H.; Hosseinian-Far, A.; Khaledi-Paveh, B.; Kazeminia, M.; Mohammadi, M.; Shohaimi, S.; Daneshkhah, A.; Eskandari, S. The prevalence of stress, anxiety, and depression within frontline healthcare workers caring for COVID-19 patients: A systematic review and meta-regression. Hum. Resour. Health 2020, 18, 100. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Liang, Y.; Chen, M.; Zheng, X.; Liu, J. Screening for Chinese medical staff mental health by S.D.S. and S.A.S. during the outbreak of COVID-19. J. Psychosom. Res. 2020, 133, 110102. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Tu, B.; Ma, J.; Chen, L.; Fu, L.; Jiang, Y.; Zhuang, Q. Psychological Impact and Coping Strategies of Frontline Medical Staff in Hunan Between January and March 2020 During the Outbreak of Coronavirus Disease 2019 (COVID-19) in Hubei, China. Med. Sci. Monit. 2020, 26, e924171. [Google Scholar]
- Al-Maqbali, M.; Al-Sinani, M.; Al-Lenjawi, B. Prevalence of stress, depression, anxiety, and sleep disturbance among nurses during COVID-19 pandemic. A systematic review and meta-analysis. J. Psychosom. Res. 2021, 141, 110343. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Beliavsky, A.; Katz, K.; Powis, J.E.; Ng, W.; Williamsm, V. What can early Canadian experience screening for COVID-19 teach us about how to prepare for a pandemic? Can. Med. Assoc. J. 2020, 192, E314–E318. [Google Scholar] [CrossRef] [Green Version]
- Koh, D. Occupational risks for COVID-19 infection. Occup. Med. 2020, 70, 3–5. [Google Scholar] [CrossRef] [Green Version]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during the COVID-19 outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental Health Outcomes Among Frontline and Second-Line Health Care Workers During the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef]
- Alamri, H.S.; Algarni, A.; Shehata, S.F.; Al Bshabshe, A.; Alshehri, N.N.; ALAsiri, A.M.; Hussain, A.H.; Alalmay, A.Y.; Alshehri, E.A.; Alqarni, Y.; et al. Prevalence of Depression, Anxiety, and Stress among the General Population in Saudi Arabia during the Covid-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9183. [Google Scholar] [CrossRef]
- Alharbi, A.S.; Alshahrani, S.M.; Alsaadi, M.M.; Al-Jahdali, H.H.; Wali, S.O.; BaHammam, A.S. Sleep quality and insomnia during the COVID-19 lockdown among the Saudi public. Saudi Med. J. 2021, 42, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N.; Tripepi, G.; Di Prinzio, R.R. Symptoms in Health Care Workers during the COVID-19 Epidemic. A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 5218. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N.; Soave, P.M.; Ricciardi, W.; Antonelli, M. Occupational Stress and Mental Health among Anesthetists during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8245. [Google Scholar] [CrossRef]
- Magnavita, N.; Soave, P.M.; Antonelli, M. Prolonged stress causes depression in frontline workers facing the COVID-19 pandemic. A repeated cross-sectional study. Int. J. Environ. Res. Public Health 2021, 2021050129. [Google Scholar] [CrossRef]
- Santarone, K.; McKenney, M.; Elkbulim, A. Preserving mental health and resilience in frontline healthcare workers during COVID-19. Am. J. Emerg. Med. 2020, 38, 1530–1531. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Number (N) and Percentage (%) |
|---|---|
| Age (years) | |
| 20 to 30 | 805 (48.0) |
| 31 to 40 | 475 (28.3) |
| 41 to 50 | 238 (14.2) |
| 51 to 60 | 117 (7.0) |
| 61 or above | 43 (2.6) |
| Gender | |
| Male | 819 (48.8) |
| Female | 859 (51.2) |
| Profession | |
| Frontline healthcare workers | 1200 (71.5) |
| Consultants | 289 (17.2) |
| Physicians | 447 (26.6) |
| Nurses | 259 (15.4) |
| Clinical pharmacists | 205 (12.2) |
| Second-line healthcare workers | 478 (28.5) |
| Lab technicians | 64 (3.8) |
| Others | 414 (24.7) |
| Area of workplace | |
| Emergency department | 219 (13.1) |
| Ward | 413 (24.6) |
| Intensive care unit (ICU) | 127 (7.6) |
| Labs | 87 (5.2) |
| Other | 832 (49.6) |
| HCWs’ involvement with COVID-19 patients | |
| No involvement | 534 (31.8) |
| Diagnosis | 229 (13.6) |
| Treatment | 303 (18.1) |
| Nursing care | 151 (9.0) |
| Other | 461 (27.5) |
| Survey Statement | Minimal Anxiety N (%) | Mild Anxiety N (%) | Moderate Anxiety N (%) | Severe Anxiety N (%) | Total N (%) | Chi (df) | p-Value |
|---|---|---|---|---|---|---|---|
| Age (years) | |||||||
| 20 to 30 | 301 (37.4) | 266 (33.0) | 142 (17.6) | 96 (11.9) | 805 (100.0) | 30.007 (12) | 0.003 |
| 31 to 40 | 199 (41.9) | 161 (33.9) | 62 (13.0) | 53 (11.1) | 475 (100.0) | ||
| 41 to 50 | 97 (40.8) | 87 (36.5) | 31 (13.0) | 23 (9.6) | 238 (100.0) | ||
| 51 to 60 | 65 (55.5) | 28 (23.9) | 16 (13.6) | 8 (6.8) | 117 (100.0) | ||
| 61 above | 26 (60.5) | 13 (30.2) | 3 (6.9) | 1 (2.3) | 43 (100.0) | ||
| Gender | |||||||
| Male | 390 (47.6) | 267 (32.6) | 99 (12.0) | 63 (7.7) | 819 (100.0) | 41.226 (3) | 0.000 |
| Female | 298 (34.7) | 288 (33.5) | 155 (18.0) | 118 (13.7) | 859 (100.0) | ||
| Professional title | |||||||
| Consultant | 121 (41.8) | 102 (35.3) | 33 (11.4) | 33 (11.4) | 289 (100.0) | 27.460 (15) | 0.025 |
| Physician | 187 (41.8) | 146 (32.6) | 61 (13.6) | 53 (11.8) | 447 (100.0) | ||
| Nurses | 104 (40.1) | 87 (33.6) | 47 (18.1) | 21 (8.1) | 259 (100.0) | ||
| Clinical pharmacist | 75 (36.6) | 73 (35.6) | 27 (13.1) | 30 (14.6) | 205 (100.0) | ||
| Lab technician | 38 (59.4) | 15 (23.4) | 6 (9.3) | 5 (7.8) | 64 (100.0) | ||
| Others | 163 (39.3) | 132 (31.9) | 80 (19.3) | 39 (9.4) | 414 (100.0) | ||
| HCWs’ involvement with COVID-19 patients | |||||||
| No involvement | 239 (44.8) | 173 (32.4) | 79 (14.8) | 43 (8.1) | 534 (100.0) | 34.536 (12) | 0.001 |
| Diagnosis | 94 (41.0) | 73 (31.9) | 30 (13.1) | 32 (14.0) | 229 (100.0) | ||
| Treatment | 99 (32.7) | 97 (32.0) | 55 (18.2) | 52 (17.2) | 303 (100.0) | ||
| Nursing care | 63 (41.7) | 47 (31.1) | 30 (19.9) | 11 (7.3) | 151 (100.0) | ||
| SOther | 193 (41.9) | 165 (35.8) | 60 (13.0) | 43 (9.3) | 461 (100.0) | ||
| Survey Statement | Good Sleep Quality <5 N (%) | Poor Sleep Quality ≥5 N (%) | Total N (%) | Chi (Degree of Freedom-df) | p-Value |
|---|---|---|---|---|---|
| Healthcare facility | |||||
| Primary healthcare center | 76 (21.9) | 270 (78.0) | 346 (100.0) | 0.026 | |
| Secondary or tertiary hospital | 88 (16.9) | 432 (83.0) | 520 (100.0) | ||
| Specialized hospital | 61 (14.8) | 349 (85.1) | 410 (100.0) | ||
| Polyclinic | 9 (11.2) | 71 (88.75) | 80 (100.0) | 12.775 (5) | |
| Laboratories | 8 (15.3) | 44 (84.6) | 52 (100.0) | ||
| Others | 60 (22.2) | 210 (77.7) | 270 (100.0) | ||
| Work area | |||||
| Emergency department | 49 (22.3) | 170 (77.6) | 219 (100.0) | 0.002 | |
| Ward | 51 (12.3) | 362 (87.6) | 413 (100.0) | ||
| Intensive care unit (ICU) | 17 (13.4) | 110 (86.6) | 127 (100.0) | 16.979 (4) | |
| Labs | 15 (17.2) | 72 (82.7) | 87 (100.0) | ||
| Other | 170 (20.4) | 662 (79.5) | 832 (100.0) | ||
| HCWs’ involvement with COVID-19 | |||||
| No involvement | 117 (21.9) | 417 (78.0) | 534 (100.0) | 0.00 | |
| Diagnosis | 32 (13.9) | 197 (86.0) | 229 (100.0) | ||
| Treatment | 32 (10.5) | 271 (89.4) | 303 (100.0) | 21.733 (4) | |
| Nursing care | 34 (22.5) | 117 (77.4) | 151 (100.0) | ||
| Others | 87 (18.8) | 374 (81.1) | 461 (100.0) | ||
| Profession | |||||
| Consultant | 65 (22.5) | 224 (77.5) | 289 (100.0) | 7.658 (5) | 0.176 |
| Physician | 74 (16.6) | 373 (83.4) | 447 (100.0) | ||
| Nurse | 53 (20.5) | 206 (79.5) | 259 (100.0) | ||
| Clinical pharmacist | 33 (16.1) | 172 (83.9) | 205 (100.0) | ||
| Lab technician | 12 (18.8) | 52 (81.2) | 64 (100.0) | ||
| Other | 65 (15.7) | 349 (84.3) | 414 (100.0) | ||
| Global PSQI Score Mean ± SD (8.944 ± 3.79) | 302 (18.0) | 1376 (82.0) | 1678 (100.0) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meo, S.A.; Alkhalifah, J.M.; Alshammari, N.F.; Alnufaie, W.S. Comparison of Generalized Anxiety and Sleep Disturbance among Frontline and Second-Line Healthcare Workers during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 5727. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115727
Meo SA, Alkhalifah JM, Alshammari NF, Alnufaie WS. Comparison of Generalized Anxiety and Sleep Disturbance among Frontline and Second-Line Healthcare Workers during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(11):5727. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115727
Chicago/Turabian StyleMeo, Sultan Ayoub, Joud Mohammed Alkhalifah, Nouf Faisal Alshammari, and Wejdan Saud Alnufaie. 2021. "Comparison of Generalized Anxiety and Sleep Disturbance among Frontline and Second-Line Healthcare Workers during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 11: 5727. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115727