
Addressing Smoking Cessation among Women in Substance Use Treatment: A Qualitative Approach to Guiding Tailored Interventions

 ,
, 
Abstract
:1. Introduction
1.1. Taking Texas Tobacco-Free
1.2. Theoretical Framework and Study Aim
2. Materials and Methods
2.1. Ethical Approval
2.2. Design
2.3. Data Collection
2.4. Participating Centers
2.5. Participating Clients and Clinicians
2.6. Data Analysis
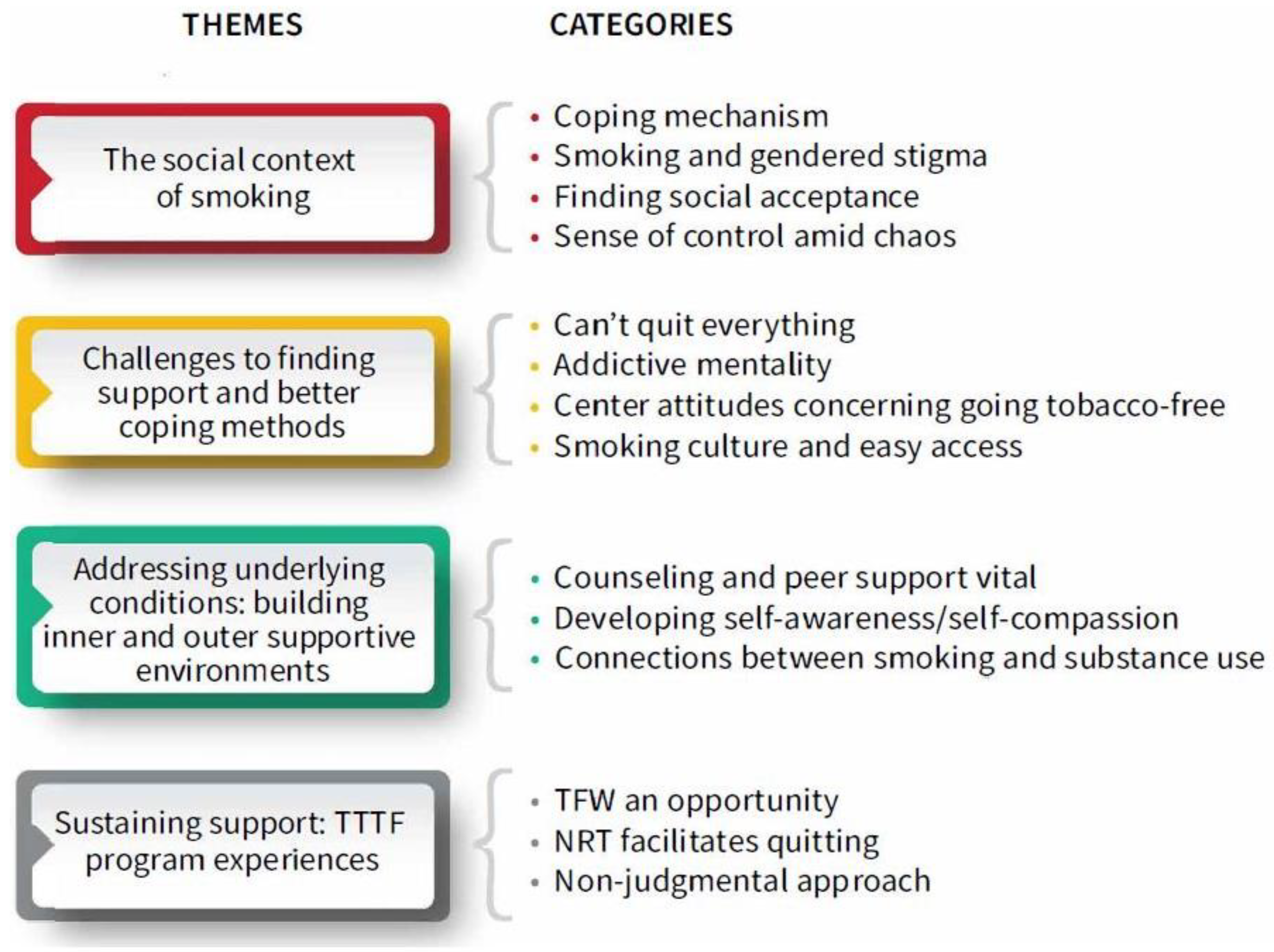
3. Results
3.1. The Social Context of Smoking
3.1.1. “Calms Me Down”/Coping Mechanism
I’d smoke a cigarette to calm myself down and I feel it was a pacifying thing… when you’re struggling with stuff that you’ve experienced… a lot of people that smoke have underlying issues. You don’t just drink or smoke for no reason, you’re trying to get away from something that’s hurting you, you’re trying to escape something that’s painful… so it’s deeper.(Rose, Women’s Center 1)
I noticed I could quit cigarettes really easily, but it was never a matter of whether I could quit, but more like I felt I needed it when I was stressed out. Like it’s not an addiction so much as I need to get rid of the stress and the anxiety… I started with a lot of self-loathing and I purposely hurt myself in different ways even subconsciously, like with smoking.(Rose, Women’s Center 1)
3.1.2. Smoking and Gendered Stigma
When my kids are getting on my nerves—I have 3 children all under the age of 5, okay—it’s probably a good thing that I can take those 5 min to smoke a cigarette and just—‘Whew’—catch a break, you know?(Mary, Women’s Center 2)
You’re still smoking while you’re pregnant? [incredulous] I quit when I was pregnant…You need to quit because it’s bad for your baby. [Others present agree](Pat, SUTC1)
I feel like one of the most negative things for me is the way my kids react to it. It eats at me because my kids will say, ‘Mom you’re smoking.’ My 3-year-old will be like, ‘Mom put that cigarette down that’s bad for you’… I want to quit, I need to quit, but it’s so hard.(Grace, Women’s Center 2)
3.1.3. Developing Social Acceptance
Yes, I want to quit. There is a side of me that’s just like grotesqued about it, you know? And there’s another side of me that still really wants it.(Alma, SUTC1)
Smoking is how I made friends here, we hung out because we all smoked. Now that I don’t smoke, it makes it really hard to be out there because they’re all still smoking and I’m just standing there wanting one. That’s one of the hardest things is that even when you do quit, it’s still everywhere and it’s with the people you hang out with and when you take your kids outside, it’s outside.(Tasha, Women’s Center 1)
3.1.4. Sense of Control Amid Chaos
I feel like sometimes I need an external source of control, I can’t control how I feel about myself or what’s going on in my mind, or my anxiety, or the things around me… smoking cigarettes gives me a sense of control… When you struggle with mental illness and depression and anxiety and the stuff that you’ve experienced, when you smoke... I’m doing something to my body that I can control… I can’t control what is going on inside, but I can control what I do to my body. And that kind of makes the craziness in my head isolated to one location.(Rose, Women’s Center 1)
3.2. Challenges to Finding Better Coping Methods
3.2.1. “Can’t Quit Everything”
A lot of people are coming from really extreme backgrounds, like drug use basically. They’re still recovering, but cigarettes are helping them… because that is something that is helping them get through their recovery.(Tracy, Women’s Center 2)
We have to be mindful that the majority of individuals that are employed here are recovering addicts. And that cigarettes helped them through quitting their drug of choice. So now getting rid of everything, is going to bring up emotions and they could relapse.(Sue, Counselor, SUTC1)
3.2.2. Addictive Mentality
I’m not going to sit here and B.S. [smoking] is bad for you. It’s deadly. And the thing is some of us, we get touchy and feely about not being able to smoke cigarettes because we’re addictive. Because we like it and get defensive as cigarette smokers, because we want what we want. But that’s when addiction plays its part, is the selfishness. We will put anything in front of us to defend it, no matter how bad it is for us. It’s a good idea we’re not allowed to smoke here, so that we can find better coping methods.(Alma, SUTC1)
3.2.3. Center Support/Attitudes Concerning Going Tobacco-Free
We’re about the whole woman and her family and how everyone is affected by cigarette smoke… now clients are able to utilize new coping skills instead of running out and having a cigarette. For a smoker that’s your main coping skill because you’re still in that addictive behavior. So, from my point of view, it’s [implementing TFW program] the best thing that we’ve ever done.(Martha, Counselor, SUTC3)
I haven’t seen very much of [smoking counseling] happening, all clients’ time is taken up dealing with more pressing matters, more dangerous behaviors to address, more processing trauma they never had a safe space to talk about. I think counselors are more focused on the bigger problems in their life, which parallels how the clients are thinking about it as well. It’s just smoking.(Peg, Counselor, SUTC1)
Sally: Sometimes you can see them [counselors] standing over there smoking… half of them are still smoking.
IML: So how do y’all feel about that?
Cindy: Makes me feel bummed, cause I can’t smoke a cigarette. They shouldn’t be able to either. It’s just like y’all are setting the example for us. We in here recovering and some of y’all have already went through y’all recoveries. So y’all should be showing a prime example of what recovery looks like.(SUTC1)
My thinking was when I was in treatment, a few years ago, there was no attempt where I was, to address that [smoking] addiction… It doesn’t seem to be an issue for the treatment team to address it here. If the treatment team isn’t addressing it, then you don’t think it’s a big deal.(Marla, Recovery coach, SUTC1)
3.2.4. Smoking Culture and Easy Access
There was a lot of resistance, mainly from other counselors, to actually implementing tobacco treatment into their regular treatment plan. I think the main buy-in was getting staff to accept the idea that nicotine is a drug. Because for such a long-time smoking was accepted in the recovery community; in all the NA and AA groups everybody smoked from the time they started in the 1930s. So, that was the biggest problem that we had; was really getting buy-in from the staff.(Martha, Counselor, SUTC3)
I had stopped smoking for two years and got back with my children’s’ father, who smoked, and from the stress and anxiety that he brought to my life that’s why I started back smoking. At that time, I didn’t know how to cope with my emotions and everything… so, I’m worried because it’s so much easier when it’s legal and it’s everywhere. There are no consequences like with my kids, or jail. I just feel like it’s going to be my biggest issue, I’m not worried about the drugs, but more cigarettes.(Juana, SUTC2)
3.3. Addressing Underlying Conditions: Building Inner and Outer Supportive Environments
3.3.1. Smoking Counseling and Peer Support Vital
At first, when I was unable to rationalize and I was angry, I had a lot of self-hate. Along with coping mechanisms and how bad it is for your health, and other things I’ve learned, is part of the reason I’m able to not smoke. I’m not as depressed, I’m not as angry, I go and do other things, like exercise, that help me feel better inside... and the NRT has helped a lot. I don’t think about it as much because I can actually deal with my problems and not mask them with a cigarette.(Kayla, SUTC2)
I was never big on asking for help. I was very ‘do it myself.’ But the more sober I get, the more recovery in therapy I get, the more I’m realizing asking for help with something that’s beneficial, it’s not something to be ashamed of. Doing something together is helpful for everybody. Team effort is better because we all want to better ourselves.(Chloe, Women’s Center 1)
It’d be helpful to be in a group simply because of the education provided and the opportunity to talk about the times when they get to a place where they can be aware of when they want that cigarette of what’s going on with them. When I quit, I found myself using a lot of the tools that I’d learned while I was in treatment and it worked for me to quit the cigarettes… what also helped me was the opportunity to talk to people, to have that person I could call and say—Hey, this is where I’m at, this is what I’m going through.(Marla, Recovery coach, SUTC1)
We do a recovery plan within a week of them coming in; their short-term, long-term goals, and smoking is part of that, and it’s amended as they progress in the program. I see a change from day 1 to 90, they acquire more coping skills.(Meg, counselor, SUTC2)
3.3.2. Self-Awareness/Self-Compassion
So, when you’re high stress, you go to your default setting which isn’t good considering where you come from… for 21 years of my life, it was not good, but I’ve been noticing the more I work on loving and taking care of myself and validating my wounds, I lose those habits without trying. But when I’ve tried to purposefully let go of habits, I relapse and then I relapse, and then I hate myself more, which is a core root problem.(Holly, Women’s Center 1)
I’m a recovering alcoholic but I’ll still get these ‘fiends’ for something and cigarettes is what I had. But those ‘fiends’ for something that’ll ‘Ah,’ just relax me, I found even after I smoked that feeling was just stronger, it’s not giving that relaxing feeling I want. I feel if I just remove the dang cigarette that feeling is not as strong… I’m finding that when I quit [smoking] altogether, just like the alcohol, that ‘fiend’ isn’t there anymore.(Zoe, Women’s Center 2)
It was my choice this time that made the big difference. All the times before I was too broke, couldn’t afford it, or the doctor said I needed to quit. This time, I wanted it and it’s been much easier. It’s still not easy, but it’s easier than the other times.(Carla, Women’s Center 2)
3.3.3. Connections between Smoking and Substance Use
I started smoking when I started shooting dope and got into my addiction. Because the nicotine from the cigarette kept the high going, and it kept me from stressing.(LaToya, SUTC1)
I think it’s really valuable to quit, that’s one of the last parts of the addiction, still holding on to that last addiction, it triggers my DOC [drug of choice] every time I smoke a cigarette, they go hand-in-hand. I feel like finally releasing that from my life, I’ll be free of it.(Kay, Women’s Center 2)
3.4. Sustaining Support: TTTF Program Experiences
3.4.1. TFW Program an Opportunity
The thing that’s motivated me to stop smoking is, number one: I’m not allowed to smoke.(Laura, SUTC3)
I have been through treatment way too many times and I never gave up cigarettes and I always end up smoking crack… I’m going try something different this time I’m giving up the cigarettes too. I’m glad for it [TTTF] because it’s easier for me to stop smoking in an environment like this. I know I wouldn’t have stopped smoking if I hadn’t been here. Cause I’d still be smoking crack, I’d still be drinking, smoking weed, and cigarettes.(LaToya, SUTC1)
I am glad I’m here because they don’t permit smoking on the premises, otherwise I don’t think I’d be able to stop. I feel a lot better about my health and that I stopped smoking.(Donna, SUTC2)
A lot of clients are heavy smokers, without this program I don’t think they’d stay, people leave because they can’t smoke, that’s their excuse. The NRT’s really helped women with their anxiety, stress, whatever they feel the cigarettes were helping them with, giving them treatment. Cigarettes is key to relapse in drug abuse, this program helps them with their triggers and offers them everything we can to successfully recover. This program is one of the biggest helpers in determining how successful they’re going to be when they leave.(Anita, Counselor, SUTC2)
I appreciate the program, it’s wonderful for someone that’s ready to quit. [Counselors] are accommodating people that are ready to quit, but it’s a waste of time for those not ready to quit. But I believe it’s very worthwhile. They’re doing the best they can now.(Karen, SUTC3)
3.4.2. NRT Facilitates Quitting
I am thankful, very thankful, for y’all’s help. I am ecstatic. I’ll be stressed out and take that gum and I’m settled down. It’s a miracle that I have been able to do it [quit smoking].(Lucy, SUTC2)
This is the first time I’ve tried NRT to quit smoking. Every other time I’ve tried cold turkey and it hasn’t ever stuck. My hopes are high that, along with the education I’m getting about addiction, might help me abstain from smoking more successfully than in the past. Even though it wasn’t my choice initially, I don’t want to continue smoking. So, I’m optimistic about being able to do it this time.(Joy, SUTC3)
[NRT] is really the only thing that’s helped. I think it’s the patch with the lozenge because it’s an oral fixation, smoking is something in your mouth all the time.(Laura, SUTC3)
3.4.3. Non-Judgmental Approach and Support
Every time I relapsed, and felt ashamed and bad, I’d tell myself ‘It’s okay, try again.’ I just kept getting up and getting up and failing and, eventually, I did stop. The big thing that helped me was having that mentality... and if there was openness about that [with counselors] without the condemnation of ‘Don’t do it,’ is a great thing... guilt and shame have kept me stuck in those cycles of going to your coping mechanisms [cigarettes, drugs]. If you quit smoking, you’re probably going to create another negative coping mechanism because it’s not the cigarette itself. You really have to deal with the guilt and shame, that is the hardest part… so focus on self-love and healing the individual and those bad side effects will slowly disappear on their own because they won’t need that negative coping mechanism anymore.(Holly, Women’s Center 1)
An effect of having a non-smoking facility I wish could be changed somehow… avoiding creating that feeling that I’m going to be judged by my counselor if I say I’m not ready to quit. Because, from my experience replacing unhealthy coping with healthy coping, an essential part of that process was detaching the judgment that unhealthy coping is bad or shameful… you give them support until they’re ready to replace it with healthy coping.(Peg, Counselor, SUTC1)
That’s one thing I’m concerned about, I don’t want that tool [the TFW policy] to be used to judge or police them... I can see that being pretty counterproductive.(Ivy, Counselor, SUTC1)
3.5. Specific Program Recommendations
4. Discussion
4.1. Responding to the Social Context of Smoking and Quitting
4.2. TTTF Program Experiences
4.3. TTTF Program Recommendations
4.4. Study Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Redfield, R.R.; Hahn, S.M.; Sharpless, N.E. Redoubling Efforts to Help Americans Quit Smoking—Federal Initiatives to Tackle the Country’s Longest-Running Epidemic. N. Engl. J. Med. 2020, 383, 1606–1609. [Google Scholar] [CrossRef]
- Businelle, M.S.; Kendzor, D.E.; Reitzel, L.R.; Costello, T.J.; Cofta-Woerpel, L.; Li, Y.; Mazas, C.A.; Vidrine, J.I.; Cinciripini, P.M.; Greisinger, A.J.; et al. Mechanisms linking socioeconomic status to smoking cessation: A structural equation modeling approach. Health Psychol. 2010, 29, 262–273. [Google Scholar] [CrossRef] [Green Version]
- Voigt, K. Smoking and Social Justice. Public Health Ethics 2010, 3, 91–106. [Google Scholar] [CrossRef]
- Farmer, M.M.; Rose, D.E.; Riopelle, D.; Lanto, A.B.; Yano, E.M. Gender Differences in Smoking and Smoking Cessation Treatment: An Examination of the Organizational Features Related to Care. Women’s Health Issues 2011, 21, S182–S189. [Google Scholar] [CrossRef] [PubMed]
- Fallin-Bennett, A.; Barnett, J.; Ducas, L.; Wiggins, A.T.; McCubbin, A.; Ashford, K. Pilot Tobacco Treatment Intervention for Women in Residential Treatment for Substance Use Disorder. J. Obstet. Gynecol. Neonatal Nurs. 2018, 47, 749–759. [Google Scholar] [CrossRef]
- Fallin-Bennett, A.; Parker, K.A.; Miller, M.A.; Ashford, K.; Hahn, E.J. Smoking and Tobacco-Free Policies in Women’s Residential Substance Use Disorder Treatment Facilities: A Community-Engaged Approach. Nicotine Tob. Res. 2017, 20, 1386–1392. [Google Scholar] [CrossRef]
- Amos, A.; Greaves, L.; Nichter, M.; Bloch, M. Women and tobacco: A call for including gender in tobacco control research, policy and practice. Tob. Control 2012, 21, 236–243. [Google Scholar] [CrossRef]
- Lawless, M.H.; Harrison, K.A.; Grandits, G.A.; Eberly, L.E.; Allen, S.S. Perceived stress and smoking-related behaviors and symptomatology in male and female smokers. Addict. Behav. 2015, 51, 80–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuchman, E. Women and Addiction: The Importance of Gender Issues in Substance Abuse Research. J. Addict. Dis. 2010, 29, 127–138. [Google Scholar] [CrossRef]
- Women and Smoking: Surgeon General’s Report on Smoking and Health; Centers for Disease Control and Prevention: Atlanta, GA, USA. Available online: https://www.cdc.gov/tobacco/data_statistics/sgr/50th-anniversary/pdfs/fs_women_smoking_508.pdf (accessed on 16 October 2020).
- Women and Tobacco: The Facts about Women and Tobacco. Available online: https://truthinitiative.org/sites/default/files/media/files/2019/03/Truth_Women%20and%20Tobacco_FactSheet_final.pdf (accessed on 24 October 2020).
- Allen, A.M.; Oncken, C.; Hatsukami, D.K. Women and Smoking: The Effect of Gender on the Epidemiology, Health Effects, and Cessation of Smoking. Curr. Addict. Rep. 2014, 1, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Hemsing, N.; Greaves, L.; Poole, N. Tobacco Cessation Interventions for Underserved Women. J. Soc. Work. Pract. Addict. 2015, 15, 267–287. [Google Scholar] [CrossRef] [Green Version]
- Husky, M.M.; Paliwal, P.; Mazure, C.M.; McKee, S.A. Gender Differences in Association with Substance Use Diagnoses and Smoking. J. Addict. Med. 2007, 1, 161–164. [Google Scholar] [CrossRef]
- Guydish, J.; Passalacqua, E.; Tajima, B.; Chan, M.; Chun, J.; Bostrom, A. Smoking Prevalence in Addiction Treatment: A Review. Nicotine Tob. Res. 2011, 13, 401–411. [Google Scholar] [CrossRef] [Green Version]
- Conway, K.P.; Compton, W.; Stinson, F.S.; Grant, B.F. Lifetime comorbidity of DSM-IV mood and anxiety disorders and specific drug use disorders: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. J. Clin. Psychiatry 2006, 67, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, S.F.; Back, S.E.; Lawson, K.; Brady, K.T. Substance Abuse in Women. Psychiatr. Clin. 2010, 33, 339–355. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Delucchi, K.; Hall, S.M. A Meta-Analysis of Smoking Cessation Interventions with Individuals in Substance Abuse Treatment or Recovery. J. Consult. Clin. Psychol. 2004, 72, 1144–1156. [Google Scholar] [CrossRef] [Green Version]
- Fuller, B.E.; Guydish, J.; Tsoh, J.; Reid, M.S.; Resnick, M.; Zammarelli, L.; Ziedonis, D.M.; Sears, C.; Mccarty, D. Attitudes toward the integration of smoking cessation treatment into drug abuse clinics. J. Subst. Abus. Treat. 2007, 32, 53–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eby, L.T.; Laschober, T.C.; Muilenburg, J.L. Sustained, New, Never, and Discontinued Tobacco Cessation Services Adopters. J. Subst. Abus. Treat. 2015, 49, 8–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, K.P.; Gibson, C.A.; Ahluwalia, J.S.; Schmelzle, K.H. Tobacco use and quit attempts among methadone maintenance clients. Am. J. Public Health 2001, 91, 296–299. [Google Scholar] [CrossRef] [Green Version]
- Cavazos-Rehg, P.A.; Breslau, N.; Hatsukami, D.; Krauss, M.J.; Spitznagel, E.L.; Grucza, R.A.; Salyer, P.; Hartz, S.M.; Bierut, L.J. Smoking cessation is associated with lower rates of mood/anxiety and alcohol use disorders. Psychol. Med. 2014, 44, 2523–2535. [Google Scholar] [CrossRef] [Green Version]
- Prochaska, J.J.; Das, S.; Young-Wolff, K.C. Smoking, Mental Illness, and Public Health. Annu. Rev. Public Health 2017, 38, 165–185. [Google Scholar] [CrossRef] [Green Version]
- Taylor, G.; McNeill, A.; Girling, A.; Farley, A.; Lindson, N.; Aveyard, P. Change in mental health after smoking cessation: Systematic review and meta-analysis. BMJ 2014, 348, g1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatley, J.M.; Callaghan, R.C. Tobacco-Related Mortality among Individuals with Alcohol or Drug Use Disorders. In Neuropathology of Drug Addictions and Substance Misuse; Academic Press: San Diego, CA, USA, 2016; pp. 104–114. [Google Scholar] [CrossRef]
- Helstrom, A.W.; Bell, M.E.; Pineles, S.L. Feeling Better and Smoking Less: The Relationship between Trauma Symptoms and Smoking over Time. Cogn. Ther. Res. 2008, 33, 235–240. [Google Scholar] [CrossRef]
- Amstadter, A.B.; Resnick, H.S.; Nugent, N.R.; Acierno, R.; Rheingold, A.A.; Minhinnett, R.; Kilpatrick, D.G. Longitudinal trajectories of cigarette smoking following rape. J. Trauma. Stress 2009, 22, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Greaves, L.; Poole, N.; Hemsing, N. Tailored Intervention for Smoking Reduction and Cessation for Young and Socially Disadvantaged Women during Pregnancy. J. Obstet. Gynecol. Neonatal Nurs. 2019, 48, 90–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bottorff, J.L.; Haines-Saah, R.; Kelly, M.T.; Oliffe, J.L.; Torchalla, I.; Poole, N.; Greaves, L.; Robinson, C.A.; Ensom, M.H.; Okoli, C.T.; et al. Gender, smoking and tobacco reduction and cessation: A scoping review. Int. J. Equity Health 2014, 13, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Taking Texas Tobbaco Free. Available online: http://www.takingtexastobaccofree.com (accessed on 27 October 2020).
- Correa-Fernández, V.; Wilson, W.T.; Kyburz, B.; O’Connor, D.P.; Stacey, T.; Williams, T.; Lam, C.Y.; Reitzel, L.R. Evaluation of the Taking Texas Tobacco Free Workplace Program within behavioral health centers. Transl. Behav. Med. 2018, 9, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Correa-Fernández, V.; Wilson, W.T.; Shedrick, D.A.; Kyburz, B.; Samaha, H.L.; Stacey, T.; Williams, T.; Lam, C.Y.; Reitzel, L.R. Implementation of a tobacco-free workplace program at a local mental health authority. Transl. Behav. Med. 2017, 7, 204–211. [Google Scholar] [CrossRef] [Green Version]
- Garey, L.; Neighbors, C.; Leal, I.M.; Lam, C.Y.; Wilson, W.T.; Kyburz, B.; Stacey, T.; Correa-Fernández, V.; Williams, T.; Zvolensky, M.J.; et al. Tobacco-related knowledge following a comprehensive tobacco-free workplace program within behavioral health facilities: Identifying organizational moderators. Patient Educ. Couns. 2019, 102, 1680–1686. [Google Scholar] [CrossRef]
- Samaha, H.L.; Correa-Fernández, V.; Lam, C.; Wilson, W.T.; Kyburz, B.; Stacey, T.; Williams, T.; Reitzel, L.R. Addressing Tobacco Use Among Consumers and Staff at Behavioral Health Treatment Facilities Through Comprehensive Workplace Programming. Health Promot. Pract. 2017, 18, 561–570. [Google Scholar] [CrossRef]
- Nitturi, V.; Chen, T.-A.; Kyburz, B.; Leal, I.M.; Correa-Fernandez, V.; O’Connor, D.P.; Williams, T.; Garey, L.; Stacey, T.; Wilson, W.T.; et al. Organizational Characteristics and Readiness for Tobacco-Free Workplace Program Implementation Moderates Changes in Clinician’s Delivery of Smoking Interventions within Behavioral Health Treatment Clinics. Nicotine Tob. Res. 2021, 23, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Le, K.; Correa-Fernández, V.; Leal, I.M.; Kyburz, B.; Chen, T.-A.; Barrientos, D.; Saenz, E.; Williams, T.; O’Connor, D.P.; Obasi, E.M.; et al. Tobacco-free Workplace Program at a Substance Use Treatment Center. Am. J. Health Behav. 2020, 44, 652–665. [Google Scholar] [CrossRef]
- Leal, I.M.; Chen, T.-A.; Correa-Fernández, V.; Le, K.; O’Connor, D.P.; Kyburz, B.; Wilson, W.T.; Williams, T.; Reitzel, L.R. Adapting and Evaluating Implementation of a Tobacco-Free Workplace Program in Behavioral Health Centers. Am. J. Health Behav. 2020, 44, 820–839. [Google Scholar] [CrossRef] [PubMed]
- Taing, M.; Kyburz, B.; Leal, I.M.; Le, K.; Chen, T.-A.; Correa-Fernandez, V.; Williams, T.; O’Connor, D.P.; Obasi, E.M.; Casey, K.; et al. Clinician Training in the Adaptation of a Comprehensive Tobacco-Free Workplace Program in Agencies Serving the Homeless and Vulnerably Housed. Int. J. Environ. Res. Public Health 2020, 17, 6154. [Google Scholar] [CrossRef]
- Graham, H. Women’s smoking and family health. Soc. Sci. Med. 1987, 25, 47–56. [Google Scholar] [CrossRef]
- Graham, H.; Inskip, H.M.; Francis, B.; Harman, J. Pathways of disadvantage and smoking careers: Evidence and policy implications. J. Epidemiol. Community Health 2006, 60, ii7–ii12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, M.J.; Greaves, L.; Kushner, K.E.; Letourneau, N.L.; Spitzer, D.L.; Boscoe, M. Where There Is Smoke, There is Stress: Low-Income Women Identify Support Needs and Preferences for Smoking Reduction. Health Care Women Int. 2011, 32, 359–383. [Google Scholar] [CrossRef]
- Greaves, L.; Devries, K. Expecting to Quit: A Best Practices Review of Smoking Cessation Interventions for Pregnant and Postpartum Girls and Women; Health Canada: Vancouver, BC, Canada, 2003. [Google Scholar]
- Triandafilidis, Z.; Ussher, J.M.; Perz, J.; Huppatz, K. An Intersectional Analysis of Women’s Experiences of Smoking-Related Stigma. Qual. Health Res. 2016, 27, 1445–1460. [Google Scholar] [CrossRef]
- Antin, T.M.J.; Annechino, R.; Hunt, G.; Lipperman-Kreda, S.; Young, M. The gendered experience of smoking stigma: Implications for tobacco control. Crit. Public Health 2016, 27, 443–454. [Google Scholar] [CrossRef] [Green Version]
- Crenshaw, K. Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color. Stanf. Law Rev. 1991, 43, 1241. [Google Scholar] [CrossRef]
- Bowleg, L. The Problem With the PhraseWomen and Minorities:Intersectionality—An Important Theoretical Framework for Public Health. Am. J. Public Health 2012, 102, 1267–1273. [Google Scholar] [CrossRef]
- Condon, E.M.; Sadler, L.S. Toxic Stress and Vulnerable Mothers: A Multilevel Framework of Stressors and Strengths. West. J. Nurs. Res. 2019, 41, 872–900. [Google Scholar] [CrossRef]
- Banderali, G.; Martelli, A.; Landi, M.; Moretti, F.; Betti, F.; Radaelli, G.; Lassandro, C.; Verduci, E. Short and long term health effects of parental tobacco smoking during pregnancy and lactation: A descriptive review. J. Transl. Med. 2015, 13, 327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tagai, E.K.; Miller, S.M.; Belfiglio, A.; Xu, J.; Wen, K.Y.; Hernandez, E. Persistent Barriers to Smoking Cessation Among Urban, Underserved Women: A Feasibility Study of Tailored Barriers Text Messages. Matern. Child Health J. 2020, 24, 1308–1317. [Google Scholar] [CrossRef]
- Walker, C.A. Social constructionism and qualitative research. J. Theory Constr. Test. 2015, 19, 37. [Google Scholar]
- Patton, M.Q. Qualitative Research & Evaluation Methods: Integrating Theory and Practice; Sage Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Sheffer, C.; Al-Zalabani, A.; Aubrey, A.; Bader, R.; Beltrez, C.; Bennett, S.; Carl, E.; Cranos, C.; Darville, A.; Greyber, J.; et al. The Emerging Global Tobacco Treatment Workforce: Characteristics of Tobacco Treatment Specialists Trained in Council-Accredited Training Programs from 2017 to 2019. Int. J. Environ. Res. Public Health 2021, 18, 2416. [Google Scholar] [CrossRef] [PubMed]
- Archibald, M.M.; Ambagtsheer, R.C.; Casey, M.G.; Lawless, M. Using Zoom Videoconferencing for Qualitative Data Collection: Perceptions and Experiences of Researchers and Participants. Int. J. Qual. Methods 2019, 18, 1609406919874596. [Google Scholar] [CrossRef] [Green Version]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic analysis: Striving to meet the trustworthiness criteria. Int. J. Methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- Morse, J.M.; Field, P.A. Qualitative Research Methods for Health Professionals; Sage Publications: Thousand Oaks, CA, USA, 1995. [Google Scholar]
- Siu, A.L. Behavioral and Pharmacotherapy Interventions for Tobacco Smoking Cessation in Adults, Including Pregnant Women: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2015, 163, 622–634. [Google Scholar] [CrossRef] [Green Version]
- Gamble, J.; Grant, J.; Tsourtos, G. Missed opportunities: A qualitative exploration of the experiences of smoking cessation interventions among socially disadvantaged pregnant women. Women Birth 2015, 28, 8–15. [Google Scholar] [CrossRef]
- Gould, G.S.; Havard, A.; Lim, L.L.; Kumar, R.; The PSANZ Smoking in Pregnancy Expert Group. The PSANZ Smoking in Pregnancy Expert Group Exposure to Tobacco, Environmental Tobacco Smoke and Nicotine in Pregnancy: A Pragmatic Overview of Reviews of Maternal and Child Outcomes, Effectiveness of Interventions and Barriers and Facilitators to Quitting. Int. J. Environ. Res. Public Health 2020, 17, 2034. [Google Scholar] [CrossRef] [Green Version]
- Akerman, S.C.; Brunette, M.F.; Green, A.I.; Goodman, D.J.; Blunt, H.; Heil, S.H. Treating Tobacco Use Disorder in Pregnant Women in Medication-Assisted Treatment for an Opioid Use Disorder: A Systematic Review. J. Subst. Abus. Treat. 2015, 52, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Greaves, L. The Meanings of Smoking to Women and Their Implications for Cessation. Int. J. Environ. Res. Public Health 2015, 12, 1449–1465. [Google Scholar] [CrossRef]
- Slopen, N.; Kontos, E.Z.; Ryff, C.D.; Ayanian, J.Z.; Albert, M.A.; Williams, D.R. Psychosocial stress and cigarette smoking persistence, cessation, and relapse over 9–10 years: A prospective study of middle-aged adults in the United States. Cancer Causes Control. 2013, 24, 1849–1863. [Google Scholar] [CrossRef] [Green Version]
- Moylan, S.; Jacka, F.N.; Pasco, J.A.; Berk, M. Cigarette smoking, nicotine dependence and anxiety disorders: A systematic review of population-based, epidemiological studies. BMC Med. 2012, 10, 123. [Google Scholar] [CrossRef] [Green Version]
- Prochaska, J.J. Failure to treat tobacco use in mental health and addiction treatment settings: A form of harm reduction? Drug Alcohol Depend. 2010, 110, 177–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurt, R.D.; Offord, K.P.; Croghan, I.T.; Gomez-Dahl, L.; Kottke, T.E.; Morse, R.M.; Melton, L.J. Mortality following inpatient addictions treatment: Role of tobacco use in a community-based cohort. JAMA 1996, 275, 1097–1103. [Google Scholar] [CrossRef]
- Weinberger, A.H.; Platt, J.; Esan, H.; Galea, S.; Erlich, D.; Goodwin, R.D. Cigarette smoking is associated with increased risk of substance use disorder relapse: A nationally representative, prospective longitudinal investigation. J. Clin. Psychiatry 2017, 78, 152–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, J.R. Effects of abstinence from tobacco: Valid symptoms and time course. Nicotine Tob. Res. 2007, 9, 315–327. [Google Scholar] [CrossRef] [Green Version]
- Bottorff, J.L.; Kalaw, C.; Johnson, J.L.; Stewart, M.; Greaves, L.; Carey, J. Couple dynamics during women’s tobacco reduction in pregnancy and postpartum. Nicotine Tob. Res. 2006, 8, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Farrimond, H.R.; Joffe, H. Pollution, peril and poverty: A British study of the stigmatization of smokers. J. Community Appl. Soc. Psychol. 2006, 16, 481–491. [Google Scholar] [CrossRef]
- Buczkowski, K.; Marcinowicz, L.; Czachowski, S.; Piszczek, E. Motivations toward smoking cessation, reasons for relapse, and modes of quitting: Results from a qualitative study among former and current smokers. Patient Prefer. Adherence 2014, 8, 1353–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reitzel, L.R.; Vidrine, J.I.; Businelle, M.S.; Kendzor, D.E.; Costello, T.J.; Li, Y.; Daza, P.; Mullen, P.D.; Velasquez, M.M.; Cinciripini, P.M.; et al. Preventing postpartum smoking relapse among diverse low-income women: A randomized clinical trial. Nicotine Tob. Res. 2010, 12, 326–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Businelle, M.S.; Kendzor, D.E.; Reitzel, L.R.; Vidrine, J.I.; Castro, Y.; Mullen, P.D.; Velasquez, M.M.; Cofta-Woerpel, L.; Cinciripini, P.M.; Greisinger, A.J.; et al. Pathways Linking Socioeconomic Status and Postpartum Smoking Relapse. Ann. Behav. Med. 2013, 45, 180–191. [Google Scholar] [CrossRef] [Green Version]
- Thompson, L.; Pearce, J.; Barnett, J.R. Moralising geographies: Stigma, smoking islands and responsible subjects. Area 2007, 39, 508–517. [Google Scholar] [CrossRef]
- Stott, N.C.H.; Kinnersley, P.; Rollnick, S. The limits to health promotion. BMJ 1994, 309, 971–972. [Google Scholar] [CrossRef] [Green Version]
- Vidrine, J.I.; Reitzel, L.R.; Figueroa, P.Y.; Velasquez, M.M.; Mazas, C.A.; Cinciripini, P.M.; Wetter, D. Motivation and Problem Solving (MAPS): Motivationally Based Skills Training for Treating Substance Use. Cogn. Behav. Pract. 2013, 20, 501–516. [Google Scholar] [CrossRef]
- Acquavita, S.P.; Talks, A.; Fiser, K. Facilitators and Barriers to Cigarette Smoking While Pregnant for Women With Substance Use Disorders. Nicotine Tob. Res. 2017, 19, 555–561. [Google Scholar] [CrossRef]
- Williams, J.M.; Steinberg, M.L.; Griffiths, K.G.; Cooperman, N. Smokers With Behavioral Health Comorbidity Should Be Designated a Tobacco Use Disparity Group. Am. J. Public Health 2013, 103, 1549–1555. [Google Scholar] [CrossRef]
- Haasova, M.; Warren, F.C.; Ussher, M.; Van Rensburg, K.J.; Faulkner, G.; Cropley, M.; Byron-Daniel, J.; Everson-Hock, E.S.; Oh, H.; Taylor, A.H. The acute effects of physical activity on cigarette cravings: Systematic review and meta-analysis with individual participant data. Addiction 2013, 108, 26–37. [Google Scholar] [CrossRef] [Green Version]
- Hudson, N.L.; Mannino, D.M. Tobacco Use: A Chronic Illness? J. Community Health 2010, 35, 549–553. [Google Scholar] [CrossRef]
- Andrews, J.O.; Felton, G.; Wewers, M.E.; Waller, J.; Tingen, M. The effect of a multi-component smoking cessation intervention in African American women residing in public housing. Res. Nurs. Health 2007, 30, 45–60. [Google Scholar] [CrossRef] [PubMed]
- Dinno, A.; Glantz, S. Tobacco control policies are egalitarian: A vulnerabilities perspective on clean indoor air laws, cigarette prices, and tobacco use disparities. Soc. Sci. Med. 2009, 68, 1439–1447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behbod, B.; Sharma, M.; Baxi, R.; Roseby, R.; Webster, P. Family and carer smoking control programmes for reducing children’s exposure to environmental tobacco smoke. Cochrane Database Syst. Rev. 2018, 1, 1–148. [Google Scholar] [CrossRef] [Green Version]
- Kegler, M.C.; Escoffery, C.; Bundy, L.; Berg, C.J.; Haardörfer, R.; Yembra, D.; Schauer, G. Pilot Study Results from a Brief Intervention to Create Smoke-Free Homes. J. Environ. Public Health 2012, 2012, 951426. [Google Scholar] [CrossRef] [Green Version]
- Wilson, I.S.; Ritchie, D.; Amos, A.; Shaw, A.; O’Donnell, R.; Mills, L.M.; Semple, S.E.; Turner, S.W. ’I’m not doing this for me’: Mothers’ accounts of creating smoke-free homes. Health Educ. Res. 2012, 28, 165–178. [Google Scholar] [CrossRef]
- Voigt, K. “If you smoke, you stink.” Denormalisation strategies for the improvement of health-related behaviours: The case of tobacco. In Ethics in Public Health and Health Policy; Springer: Dordrecht, Germany, 2013; pp. 47–61. [Google Scholar]
- Tobacco. A clinical practice guideline for treating tobacco use and dependence: 2008 update: A US public health service report. Am. J. Prev. Med. 2008, 35, 158–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correa-Fernández, V.; Díaz-Toro, E.C.; Reitzel, L.R.; Guo, L.; Chen, M.; Li, Y.; Calo, W.A.; Shih, Y.-C.T.; Wetter, D.W. Combined treatment for at-risk drinking and smoking cessation among Puerto Ricans: A randomized clinical trial. Addict. Behav. 2017, 65, 185–192. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Center | # Clinics | # Clinical Staff | % Smokers | Total Annual Unique Clients | Total Annual Contacts | Residential/ Outpatient |
|---|---|---|---|---|---|---|
| SUTC1 | 2 | 131 | 74 | 1004 | 1004 | Both |
| SUTC2 | 1 | 22 | 75 | 1135 | 1670 | Both |
| SUTC3 | 1 | 45 | 66 | 1216 | 22,052 | Both |
| Women’s Center | 2 | 11 | 65 | 77 | 77 | Both |
| Client Characteristics | SUTC1 | SUTC2 | SUTC3 | Women’s Center |
|---|---|---|---|---|
| Unemployed | 94% | 86% | 84% | 100% |
| Housing-no stable or permanent housing | 89% | 50% | 87% | 100% |
| Prior criminal justice system history | 64% | 74% | 64% | 33% |
| CPS active status | 43% | 32% | 45% | 33% |
| Domestic violence/ abuse/trauma history | 95% | 88% | 82% | 66% |
| Substance use disorder | 100% | 100% | 100% | 27% |
| Psychiatric disorder (co-occurring) | 78% | 54% | 52% | 11.8% |
| At or below poverty level | 100% | 64% | 73% | 100% |
| Participant Quotes | |
|---|---|
| Varied NRT | If we could get the gum in here it would help me a lot… because I cannot wear the patch. It makes me sicker than a dog. I’ve tried lozenges and they are just too strong. I could only suck on it for a little bit then had to get rid of it because it was too strong. (Kat, SUTC1) |
| Smoking cessation group | It’d be good if we had a smoking group, once a week, that would really help us. (LaToya, SUTC1) |
| Exercise options | I wish we had a place so we could work out vs. smoking. I know that sounds stupid, but if we had another place to get rid of the stress, and there’s not that here. (Amy, SUTC1) |
| Smoke-free living environment | Brenda: yeah, if you stick those people who are at the same level, on wanting to quit together and have them all be neighbors… in their non-smoking neighborhoods. That could be beneficial, they could support each other. Because you don’t want to stick somebody who’s trying to quit, right in the middle of all these people who are smoking, it’ll make it 10 times harder for you to quit. Caitlyn: Yeah, it’s an incentive to take care of yourself and your kids… (Women’s Center 1) |
| NRT for family | Is there help for our families? Like when we get out of here, it would be great to be able to get some sort of assistance or discounts, as far as continuing the NRT, to help them also. (Lucy, SUTC3) |
| Education on link between stress and smoking | Showing and teaching them consistently how to get past the cravings and the connection between stress and smoking… bringing that attention to the benefits of stopping would really help the ladies. (Marla, Recovery coach, SUTC1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez Leal, I.; Taing, M.; Correa-Fernández, V.; Obasi, E.M.; Kyburz, B.; Le, K.; Koshy, L.; Chen, T.A.; Williams, T.; Casey, K.; et al. Addressing Smoking Cessation among Women in Substance Use Treatment: A Qualitative Approach to Guiding Tailored Interventions. Int. J. Environ. Res. Public Health 2021, 18, 5764. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115764
Martinez Leal I, Taing M, Correa-Fernández V, Obasi EM, Kyburz B, Le K, Koshy L, Chen TA, Williams T, Casey K, et al. Addressing Smoking Cessation among Women in Substance Use Treatment: A Qualitative Approach to Guiding Tailored Interventions. International Journal of Environmental Research and Public Health. 2021; 18(11):5764. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115764
Chicago/Turabian StyleMartinez Leal, Isabel, Matthew Taing, Virmarie Correa-Fernández, Ezemenari M. Obasi, Bryce Kyburz, Kathy Le, Litty Koshy, Tzuan A. Chen, Teresa Williams, Kathleen Casey, and et al. 2021. "Addressing Smoking Cessation among Women in Substance Use Treatment: A Qualitative Approach to Guiding Tailored Interventions" International Journal of Environmental Research and Public Health 18, no. 11: 5764. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115764