
Implementing Public Health Strategies—The Need for Educational Initiatives: A Systematic Review




Abstract
:1. Introduction
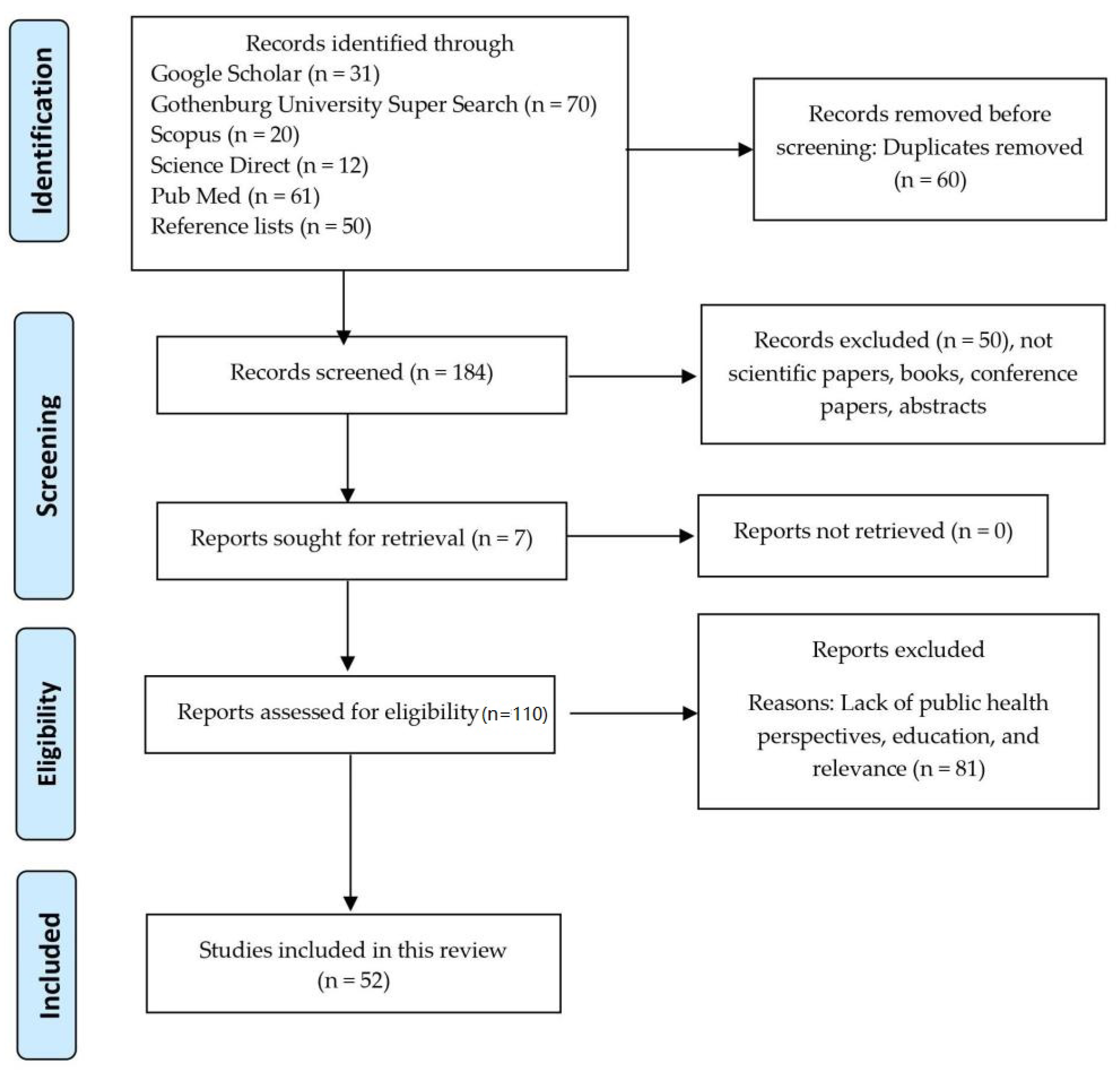
2. Materials and Methods
- Public Health Strategies
- Public Health Emergency
- Contact Tracing
- Isolation
- Quarantine
- Public Education
3. Results
3.1. Practical Aspects
3.2. Ethical Aspects
3.3. Psychological Aspects
3.4. Educational Initiatives at the Community Level
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Searching Procedures
| Search Engine | Searching Keywords | Hits |
| Google Scholar Reviewed 31 Duplicates 10, Irrelevant 19, Included 12 | Public Health Strategies | >4 million |
| “Public Health Strategies” | 21,000 | |
| “Public Health emergency” AND [(Contact Tracing) OR (Isolation) OR (Quarantine)] | 31,100 | |
| “Public Health emergency” AND “[(Contact Tracing) OR (Isolation) OR (Quarantine)]” | 6690 | |
| “Public Health emergency” AND “Contact Tracing” AND “Isolation” AND “Quarantine” AND Public Education | 2850 | |
| “Public Health emergency” AND “[(Contact Tracing) OR (Isolation) OR (Quarantine)]” AND “Public Education” | 354 | |
| “Public Health emergency” AND “[(Contact Tracing) OR (Isolation) OR (Quarantine)]” AND “Public Education” AND “Community resilience” | 31 | |
| Gothenburg University Super Search Reviewed 70 Duplicates 50, Irrelevant 15, Included 7 | “Public Health emergency” AND “Contact Tracing” | 2281 |
| “Public Health emergency” AND “Contact Tracing” AND “Isolation” | 1223 | |
| “Public Health emergency” AND “Contact Tracing” AND “Isolation” AND “Quarantine” | 803 | |
| “Public Health emergency” AND “Contact Tracing” AND “Isolation” AND “Quarantine” AND Public Education | 437 | |
| “Public Health emergency” AND “Contact Tracing” AND “Isolation” AND “Quarantine” AND “Public Education” | 70 | |
| Science Direct Reviewed 15, Irrelevant 10, Included 5 | “Public Health emergency” AND [(Contact Tracing) OR (Isolation) OR (Quarantine)] | 456 |
| “Public Health emergency” AND “[(Contact Tracing) OR (Isolation) OR (Quarantine)]” | 313 | |
| “Public Health emergency” AND “[(Contact Tracing) OR (Isolation) OR (Quarantine)]” AND Public Education | 218 | |
| “Public Health emergency” AND “[(Contact Tracing) OR (Isolation) OR (Quarantine)]” AND “Public Education” | 113 | |
| “Public Health emergency” AND “Contact Tracing” AND “Isolation” AND “Quarantine” AND Public Education | 15 | |
| Scopus Reviewed 20, Irrelevant 13, Included 8 | “Public Health emergency” AND “Contact Tracing” | 286 |
| “Public Health emergency” AND “Contact Tracing” AND “Isolation” | 117 | |
| “Public Health emergency” AND “Contact Tracing” AND “Isolation” AND “Quarantine” | 63 | |
| “Public Health emergency” AND “Contact Tracing” AND “Isolation” AND “Quarantine” AND Public Education | 20 | |
| “Public Health emergency” AND “Contact Tracing” AND “Isolation” AND “Quarantine” AND “Public Education” | 0 | |
| PubMed Reviewed 61, Irrelevant 33, Included 15 | “Public Health emergency” AND [(Contact Tracing) OR (Isolation) OR (Quarantine)] | >2 million |
| “Public Health emergency” AND “[(Contact Tracing) OR (Isolation) OR (Quarantine)]” | 466 | |
| “Public Health emergency” AND “[(Contact Tracing) OR (Isolation) OR (Quarantine)]” AND Public Education | 62 | |
| “Public Health emergency” AND “[(Contact Tracing) OR (Isolation) OR (Quarantine)]” AND “Public Education” | 0 |
Appendix B. PRISMA Checklist Abstract
| Section and Topic | Item Number | Checklist Item | Reported (Yes/No) |
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | YES |
| BACKGROUND | |||
| Objectives | 2 | Provide an explicit statement of the main objective(s) or question(s) the review addresses. | YES |
| METHODS | |||
| Eligibility criteria | 3 | Specify the inclusion and exclusion criteria for the review. | YES |
| Information sources | 4 | Specify the information sources (e.g., databases, registers) used to identify studies and the date when each was last searched. | YES |
| Risk of bias | 5 | Specify the methods used to assess risk of bias in the included studies. | No |
| Synthesis of results | 6 | Specify the methods used to present and synthesise results. | No |
| RESULTS | |||
| Included studies | 7 | Give the total number of included studies and participants and summarise relevant characteristics of studies. | No |
| Synthesis of results | 8 | Present results for main outcomes, preferably indicating the number of included studies and participants for each. If meta-analysis was done, report the summary estimate and confidence/credible interval. If comparing groups, indicate the direction of the effect (i.e., which group is favoured). | YES |
| DISCUSSION | |||
| Limitations of evidence | 9 | Provide a brief summary of the limitations of the evidence included in the review (e.g., study risk of bias, inconsistency and imprecision). | YES |
| Interpretation | 10 | Provide a general interpretation of the results and important implications. | No |
| OTHER | |||
| Funding | 11 | Specify the primary source of funding for the review. | None |
| Registration | 12 | Provide the register name and registration number. | None |
| From: Page M.J., McKenzie J.E., Bossuyt P.M., Boutron I., Hoffmann T.C., Mulrow C.D., et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi:10.1136/bmj.n71. | |||
Appendix C. PRISMA Checklist Manuscript
| Section and Topic | Item Number | Checklist Item | Location Where Item Is Reported |
| TITLE | |||
| Title | 1 | Implementing contact tracing and other public health strategies; needs for educational initiatives—A Systematic Review | Page 1 |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | Page 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | Page 1–3 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | Page 1 & 3 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | Method page 2–3 |
| Information sources | 6 | Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | Method page 2 |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | Appendix. |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. | Method page 2–3 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process. | Method page 2–3 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses), and if not, the methods used to decide which results to collect. | Figure 1 page 4, Table 1, page 5 |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | See point 10a | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | Method page 2–3 |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | NA |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | Result page 3–4 |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. | NA | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | - | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | Method page 2–3 | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis, meta-regression). | - | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | - | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | - |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | Method page 2 |
| HEQAT | |||
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | Results, Page 3 |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. | Figure 1 | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | Page 5–7 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | – |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | – |
| Results of syntheses | 20a | For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. | – |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | – | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | – | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | – | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | – |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | Table 1, page 5–7 |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | Page 9–11 |
| 23b | Discuss any limitations of the evidence included in the review. | Page 9–11 | |
| 23c | Discuss any limitations of the review processes used. | Page 9–11 | |
| 23d | Discuss implications of the results for practice, policy, and future research. | Page 9–11 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | Page 11 |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | Journals homepage | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | – | |
| Support | 25 | Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. | None |
| Competing interests | 26 | Declare any competing interests of review authors. | None |
| Availability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | Journals homepage |
| From: Page M.J., McKenzie J.E., Bossuyt P.M., Boutron I., Hoffmann T.C., Mulrow C.D., et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi:10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/ (accessed on 25 April 2021). | |||
Appendix D

References
- Humanitarian and Development Research Initiative (HADRI). State Responses to COVID-19: A Global Snapshot at 1 June 2020; Georgeou, N., Hawksley, C., Eds.; Western Sydney University: Sydney, Australia, 2020. [Google Scholar] [CrossRef]
- Capano, G.; Howlett, M.; Jarvis, D.S.; Ramesh, M.; Goyal, N. Mobilizing Policy (In)Capacity to Fight COVID-19: Understanding Variations in State Responses. Policy Soc. 2020, 39, 285–308. [Google Scholar] [CrossRef]
- Khorram-Manesh, A.; Carlström, E.; Hertelendy, A.J.; Goniewicz, K.; Casady, C.B.; Burkle, F.M. Does the prosperity of a country play a role in COVID-19 outcomes? Disaster Med. Public Health Prep. 2020, 1–20. [Google Scholar] [CrossRef]
- Alanezi, F.; Aljahdali, A.; Alyousef, S.; Alrashed, H.; Mushcab, H.; AlThani, B.; Alghamedy, F.; Alotaibi, H.; Saadah, A.; Alanzi, T. A Comparative Study on the Strategies Adopted by the United Kingdom, India, China, Italy, and Saudi Arabia to Contain the Spread of the COVID-19 Pandemic. J. Healthc. Leadersh. 2020, 12, 117–131. [Google Scholar] [CrossRef]
- Ferguson, N.; Laydon, D.; Nedjati-Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Imperial College COVID-19 Response Team. Impact of Nonpharmaceutical Interventions (NPIs) to Reduce COVID19 Mortality and Healthcare Demand; Imperial College: London, UK, 2020; pp. 1–20. [Google Scholar]
- Nazareth, J.; Minhas, J.; Jenkins, D.R.; Sahota, A.; Khunti, K.; Haldar, P.; Pareek, M. Early lessons from a second COVID-19 lockdown in Leicester, UK. Lancet 2020, 396, e4–e5. [Google Scholar] [CrossRef]
- Abeler, J.; Bäcker, M.; Buermeyer, U.; Zillessen, H. COVID-19 Contact Tracing and Data Protection Can Go Together. JMIR mHealth uHealth 2020, 8, e19359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez-Quevedo, C.; Scarpetti, G.; Webb, E. How Do Countries Structure Contact Tracing Operations and What Is the Role of Apps? The Health System Response Monitor. Covid-19. Available online: https://analysis.covid19healthsystem.org/index.php/2020/06/18/how-do-countries-structure-contact-tracing-operations-and-what-is-the-role-of-apps/ (accessed on 25 April 2021).
- Howell O’Neill, P.; Ryan-Mosley, T.; Johnson, B. A Flood of Coronavirus Apps Is Tracking Us. Now It’s Time to Keep Track of Them. MIT Technology Review, 2020. Available online: https://www.technologyreview.com/2020/05/07/1000961/launching-mittr-covid-tracing-tracker/(accessed on 25 April 2021).
- Du, L.; Raposo, V.L.; Wang, M. COVID-19 Contact Tracing Apps: A Technologic Tower of Babel and the Gap for International Pandemic Control. JMIR mHealth uHealth 2020, 8, e23194. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 National Emergency Response Center, Epidemiology & Case Management Team, Korea Centers for Disease Control & Prevention Contact Transmission of COVID-19 in South Korea: Novel Investigation Techniques for Tracing Contacts. Osong Public Health Res. Perspect. 2020, 11, 60–63. [CrossRef] [Green Version]
- Goniewicz, K.; Khorram-Manesh, A. Maintaining Social Distancing during the COVID-19 Outbreak. Soc. Sci. 2021, 10, 14. [Google Scholar] [CrossRef]
- Rowe, F.; Ngwenyama, O.; Richet, J.-L. Contact-tracing apps and alienation in the age of COVID-19. Eur. J. Inf. Syst. 2020, 29, 545–562. [Google Scholar] [CrossRef]
- McGrail, K.M. Contact-Tracing Apps: Time to Confront Broader Societal Change. Am. J. Public Health 2021, 111, 369–370. [Google Scholar] [CrossRef]
- Bernard, R.; Bowsher, G.; Sullivan, R. COVID-19 and the Rise of Participatory SIGINT: An Examination of the Rise in Government Surveillance through Mobile Applications. Am. J. Public Health 2020, 110, 1780–1785. [Google Scholar] [CrossRef]
- Lund University in Collaboration with Uppsala University and Kings’s College London. COVID Symptom Study. Available online: https://www.covid19app.lu.se/ (accessed on 25 April 2021).
- Shuja, J.; Alanazi, E.; Alasmary, W.; Alashaikh, A. COVID-19 open source data sets: A comprehensive survey. Appl. Intell. 2021, 51, 1296–1325. [Google Scholar] [CrossRef]
- Michael, K.; Abbas, R. Behind COVID-19 Contact Trace Apps: The Google–Apple Partnership. IEEE Consum. Electron. Mag. 2020, 9, 71–76. [Google Scholar] [CrossRef]
- Baumgart, D.C. Digital advantage in the COVID-19 response: Perspective from Canada’s largest integrated digitalized healthcare system. NPJ Digit. Med. 2020, 3, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.; Lawarée, J. The adoption of contact tracing applications of COVID-19 by European governments. Policy Des. Pract. 2020, 4, 1–15. [Google Scholar] [CrossRef]
- Information Commissioner’s Office. Guide to the General Data Protection Regulation (GDPR). Information Commissioner’s Office, 2018. Available online: https://ico.org.uk/media/for-organisations/guide-to-the-general-data-protection-regulation-gdpr-1-0.pdf (accessed on 25 April 2021).
- Alanzi, T. A Review of Mobile Applications Available in the App and Google Play Stores Used during the COVID-19 Outbreak. J. Multidiscip. Health 2021, 14, 45–57. [Google Scholar] [CrossRef]
- Maghdid, H.S.; Ghafoor, K.Z. A Smartphone Enabled Approach to Manage COVID-19 Lockdown and Economic Crisis. SN Comput. Sci. 2020, 1, 1–9. [Google Scholar] [CrossRef]
- Sowmiya, B.; Abhijith, V.; Sudersan, S.; Sundar, R.S.J.; Thangavel, M.; Varalakshmi, P. A Survey on Security and Privacy Issues in Contact Tracing Application of Covid-19. SN Comput. Sci. 2021, 2, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Davalbhakta, S.; Advani, S.; Kumar, S.; Agarwal, V.; Bhoyar, S.; Fedirko, E.; Prasanna Misra, D.; Goel, A.; Gupta, L.; Agarwal, V. A Systematic Review of Smartphone Applications Available for Corona Virus Disease 2019 (COVID19) and the Assessment of their Quality Using the Mobile Application Rating Scale (MARS). J. Med. Syst. 2020, 44, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Chen, Q.; Feng, L.; Rodewald, L.; Xia, Y.; Yu, H.; Zhang, R.; An, Z.; Yin, W.; China CDC COVID-19 Emergency Response Strategy Team; et al. Active case finding with case management: The key to tackling the COVID-19 pandemic. Lancet 2020, 396, 63–70. [Google Scholar] [CrossRef]
- Sultan, M.; Sørensen, J.L.; Carlström, E.; Mortelmans, L.; Khorram-Manesh, A. Emergency Healthcare Providers’ Perceptions of Preparedness and Willingness to Work during Disasters and Public Health Emergencies. Healthcare 2020, 8, 442. [Google Scholar] [CrossRef]
- Guillon, M.; Kergall, P. Attitudes and opinions on quarantine and support for a contact-tracing application in France during the COVID-19 outbreak. Public Health 2020, 188, 21–31. [Google Scholar] [CrossRef]
- Gerli, P.; Arakpogun, E.O.; Elsahn, Z.; Olan, F.; Prime, K.S. Beyond Contact-Tracing: The Public Value of eHealth Application in a Pandemic. Gov. Inf. Q. 2021, 101581. [Google Scholar] [CrossRef]
- Ben Jaffel, H.; Hoffmann, A.; Kearns, O.; Larsson, S. Collective Discussion: Toward Critical Approaches to Intelligence as a Social Phenomenon. Int. Political Sociol. 2020, 14, 323–344. [Google Scholar] [CrossRef]
- Abdullahi, L.; Onyango, J.; Mukiira, C.; Wamicwe, J.; Githiomi, R.; Kariuki, D.; Mugambi, C.; Wanjohi, P.; Githuka, G.; Nzioka, C.; et al. Community interventions in Low—And Middle-Income Countries to inform COVID-19 control implementation decisions in Kenya: A rapid systematic review. PLoS ONE 2020, 15, e0242403. [Google Scholar] [CrossRef] [PubMed]
- Niccolai, L.; Shelby, T.; Weeks, B.; Schenck, C.; Goodwin, J.; Hennein, R.; Rossini, M.; Vazquez, J.; van Rhijn, D.; Meek, J.; et al. Community Trace: Rapid Establishment of a Volunteer Contact Tracing Program for COVID-19. Am. J. Public Health 2021, 111, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Abuhammad, S.; Khabour, O.F.; Alzoubi, K.H. COVID-19 Contact-Tracing Technology: Acceptability and Ethical Issues of Use. Patient Prefer. Adherence 2020, 14, 1639–1647. [Google Scholar] [CrossRef]
- Shivaji, B.; Anindhya, S. COVID-19: Implications on the Data Protection Framework in India. Mondaq Business Briefing, 6 May 2020. Available online: https://www.mondaq.com/india/data-protection/928998/covid-19-implications-on-the-data-protection-framework-in-india(accessed on 26 April 2021).
- Riemer, K.; Ciriello, R.; Peter, S.; Schlagwein, D. Digital contact-tracing adoption in the COVID-19 pandemic: IT gov-ernance for collective action at the societal level. Eur. J. Inf. Syst. 2020, 29, 731–745. [Google Scholar] [CrossRef]
- Basu, S. Effective Contact Tracing for COVID-19 Using Mobile Phones: An Ethical Analysis of the Mandatory Use of the Aarogya Setu Application in India. Camb. Q. Health Ethics 2021, 30, 262–271. [Google Scholar] [CrossRef]
- Collins, E.C. Evolving Considerations for Multinational Employers: COVID-19 Contact Tracing Applications. Natl. Law Rev. 2021, XI, 116. [Google Scholar]
- Ling, G.H.T.; Suhud, N.A.B.M.; Leng, P.C.; Yeo, L.B.; Cheng, C.T.; Ahmad, M.H.H.; Matusin, A.M.R.A. Factors Influencing Asia-Pacific Countries’ Success Level in Curbing COVID-19: A Review Using a Social–Ecological System (SES) Framework. Int. J. Environ. Res. Public Health 2021, 18, 1704. [Google Scholar] [CrossRef]
- Maati, A.; Švedkauskas, Ž. Framing the Pandemic and the Rise of the Digital Surveilance State. Czech J. Int. Relat. 2020, 55, 48–71. [Google Scholar] [CrossRef]
- Rothstein, M.A. From SARS to Ebola: Legal and Ethical Considerations for Modern Quarantine. Indiana Health Law Rev. 2015, 12, 227–280. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.V.; Tran, Q.D.; Phan, L.T.; Vu, L.N.; Truong, D.T.T.; Truong, H.C.; Le, T.N.; Vien, L.D.K.; Nguyen, T.V.; Luong, Q.C.; et al. In the interest of public safety: Rapid response to the COVID-19 epidemic in Vietnam. BMJ Glob. Health 2021, 6, e004100. [Google Scholar] [CrossRef] [PubMed]
- Hassandoust, F.; Akhlaghpour, S.; Johnston, A.C. Individuals’ privacy concerns and adoption of contact tracing mobile applications in a pandemic: A situational privacy calculus perspective. J. Am. Med. Inform. Assoc. 2021, 28, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, E.L.; Ryan, R.M.; Noetel, M.; Saeri, A.K.; Slattery, P.; Grundy, E.; Calvo, R. Information Safety Assurances Increase Intentions to Use COVID-19 Contact Tracing Applications, Regardless of Autonomy-Supportive or Controlling Message Framing. Front. Psychol. 2021, 11, 591638. [Google Scholar] [CrossRef] [PubMed]
- United Nation Disaster Risk Reduction (UNDRR). Sendai Framework for Disaster Risk Reduction 2015–2030. Available online: https://www.undrr.org/implementing-sendai-framework/what-sendai-framework (accessed on 26 April 2021).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Health Evidence Quality Assessment Tool. Available online: https://www.healthevidence.org/documents/our-appraisal-tools/QA_Tool&Dictionary_10Nov16.pdf (accessed on 26 April 2021).
- Stemler, S. An Overview of content analysis. Practical Assessment. Res. Eval. 2000, 7, 17. [Google Scholar] [CrossRef]
- Center for Disease Control (CDC) Contact Tracing Resources. Available online: https://www.cdc.gov/coronavirus/2019-ncov/php/open-america/contact-tracing-resources.html (accessed on 25 April 2021).
- Legendre, F.; Humbert, M.; Mermoud, A.; Lenders, V. Contact Tracing: An overview of technologies and cyber risks. arXiv 2007, arXiv:2007.02806. [Google Scholar]
- Bachtiger, P.; Adamson, A.; Quint, J.K.; Peters, N.S. Belief of previous COVID-19 infection and unclear government policy are associated with reduced willingness to participate in App-based contact tracing: A UK-wide observational study of 13,000 people. medRxiv 2020. [Google Scholar] [CrossRef]
- Ekong, I.; Chukwu, E.; Chukwu, M. COVID-19 Mobile Positioning Data Contact Tracing and Patient Privacy Regulations: Exploratory Search of Global Response Strategies and the Use of Digital Tools in Nigeria. JMIR mHealth uHealth 2020, 8, e19139. [Google Scholar] [CrossRef]
- Goniewicz, K.; Khorram-Manesh, A.; Hertelendy, A.J.; Goniewicz, M.; Naylor, K.; Burkle, J.F.M. Current Response and Management Decisions of the European Union to the COVID-19 Outbreak: A Review. Sustainability 2020, 12, 3838. [Google Scholar] [CrossRef]
- Williams, S.N.; Armitage, C.J.; Tampe, T.; Dienes, K. Public attitudes towards COVID-19 contact tracing apps: A UK-based focus group study. Health Expect. 2021, 24, 377–385. [Google Scholar] [CrossRef]
- Chen, A.T.; Ge, S.; Cho, S.; Teng, A.K.; Chu, F.; Demiris, G.; Zaslavsky, O. Reactions to COVID-19, information and technology use, and social connectedness among older adults with pre-frailty and frailty. Geriatr. Nurs. 2021, 42, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Dong, W.; Tao, J.; Xia, X.; Ye, L.; Xu, H.; Jiang, P.; Liu, Y. Public Emotions and Rumors Spread During the COVID-19 Epidemic in China: Web-Based Correlation Study. J. Med. Internet Res. 2020, 22, e21933. [Google Scholar] [CrossRef]
- Sfendla, A.; Hadrya, F. Factors Associated with Psychological Distress and Physical Activity during the COVID-19 Pandemic. Health Secur. 2020, 18, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Amlȏt, R.; Lambert, H.; Oliver, I.; Robin, C.; Yardley, L.; Rubin, G. Factors associated with adherence to self-isolation and lockdown measures in the UK: A cross-sectional survey. Public Health 2020, 187, 41–52. [Google Scholar] [CrossRef]
- Shah, A.; Aacharya, R.P. Combating COVID-19 Pandemic in Nepal: Ethical Challenges in an Outbreak. J. Nepal Med. Assoc. 2020, 58, 276–279. [Google Scholar] [CrossRef] [PubMed]
- O’Callaghan, M.E.; Buckley, J.; Fitzgerald, B.; Johnson, K.; Laffey, J.; McNicholas, B.; Nuseibeh, B.; O’Keeffe, D.; O’Keeffe, I.; Razzaq, A.; et al. A national survey of attitudes to COVID-19 digital contact tracing in the Republic of Ireland. Ir. J. Med. Sci. 2020, 1–25. [Google Scholar] [CrossRef]
- Charania, N.A.; Tsuji, L.J. The 2009 H1N1 pandemic response in remote First Nation communities of Subarctic Ontario: Barriers and improvements from a health care services perspective. Int. J. Circumpolar Health 2011, 70, 564–575. [Google Scholar] [CrossRef]
- Cantey, P.T.; Chuk, M.G.; Kohl, K.S.; Herrmann, J.; Weiss, P.; Graffunder, C.M.; Averhoff, F.; Kahn, E.B.; Painter, J. Public health emergency preparedness: Lessons learned about monitoring of interventions from the National Association of County and City Health Official’s survey of nonpharmaceutical interventions for pandemic H1N1. J. Public Health Manag. Pract. 2013, 19, 70–76. [Google Scholar] [CrossRef] [PubMed]
- A Charania, N.; Tsuji, L.J.S. A community-based participatory approach and engagement process creates culturally appropriate and community informed pandemic plans after the 2009 H1N1 influenza pandemic: Remote and isolated First Nations communities of sub-arctic Ontario, Canada. BMC Public Health 2012, 12, 268. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.-J.; Tu, W.-X.; Wang, X.-C.; Shi, G.-Q.; Yin, Z.-D.; Su, H.-J.; Shen, T.; Zhang, D.-P.; Li, J.-D.; Lv, S.; et al. A practical community-based response strategy to interrupt Ebola transmission in sierra Leone, 2014–2015. Infect. Dis. Poverty 2016, 5, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, J. Pediatric Mental and Behavioral Health in the Period of Quarantine and Social Distancing with COVID-19. JMIR Pediatr. Parent. 2020, 3, e19867. [Google Scholar] [CrossRef]
- Kim, J.; Park, H.-A. Development of a Health Information Technology Acceptance Model Using Consumers’ Health Behavior Intention. J. Med. Internet Res. 2012, 14, e133. [Google Scholar] [CrossRef] [PubMed]
- Neupane, H.C.; Shrestha, N.; Adhikari, S.; Gauli, B. COVID 19 and Nepal: Identification of Critical Public Health Measures. J. Nepal Med. Assoc. 2020, 58, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Rothstein, M.A. The Coronavirus Pandemic: Public Health and American Values. J. Law Med. Ethics 2020, 48, 354–359. [Google Scholar] [CrossRef]
- Smith, C.L.; Hughes, S.M.; Karwowski, M.P.; Chevalier, M.S.; Hall, E.; Joyner, S.N.; Ritch, J.; Smith, J.C.; Weil, L.M.; Chung, W.M.; et al. Addressing Needs of Contacts of Ebola Patients During an Investigation of an Ebola Cluster in the United States—Dallas, Texas, 2014. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 121–123. [Google Scholar] [PubMed]
- Joo, J.; Shin, M.M. Resolving the tension between full utilization of contact tracing app services and user stress as an effort to control the COVID-19 pandemic. Serv. Bus. 2020, 14, 461–478. [Google Scholar] [CrossRef]
- Torous, J.; Myrick, K.J.; Rauseo-Ricupero, N.; Firth, J. Digital Mental Health and COVID-19: Using Technology Today to Accelerate the Curve on Access and Quality Tomorrow. JMIR Ment. Health 2020, 7, e18848. [Google Scholar] [CrossRef]
- DeWalt, D.A.; Berkman, N.D.; Sheridan, S.L.; Lohr, K.N.; Pignone, M.P. Literacy and health outcomes. J. Gen. Intern. Med. 2004, 19, 1228–1239. [Google Scholar] [CrossRef]
- AHRQ (Agency for Healthcare Research and Quality). National Healthcare Disparities Report; AHRQ: Rockville, MD, USA, 2007.
- Paasche-Orlow, M.K.; Parker, R.M.; Gazmararian, J.A.; Nielsen-Bohlman, L.T.; Rudd, R.R. The prevalence of limited health literacy. J. Gen. Intern. Med. 2005, 20, 175–184. [Google Scholar] [CrossRef]
- Rajah, R.; Hassali, M.; Murugiah, M. A systematic review of the prevalence of limited health literacy in Southeast Asian countries. Public Health 2019, 167, 8–15. [Google Scholar] [CrossRef]
- Baccolini, V.; Rosso, A.; Di Paolo, C.; Isonne, C.; Salerno, C.; Migliara, G.; Prencipe, G.P.; Massimi, A.; Marzuillo, C.; De Vito, C.; et al. What is the Prevalence of Low Health Literacy in European Union Member States? A Systematic Review and Meta-analysis. J. Gen. Intern. Med. 2021, 36, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Tambo, E.; Djuikoue, I.C.; Tazemda, G.K.; Fotsing, M.F.; Zhou, X.N. Early stage risk communication and community engagement (RCCE) strategies and measures against the coronavirus disearse 2019 (COVID-19) pandemic crisis. Glob. Health J. 2021, 5, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Simon, S. Subtle Connections: Pandemic and the Authoritarian Impulse. Survival 2020, 62, 103–111. [Google Scholar] [CrossRef]
- Nelson, C.; Lurie, N.; Wasserman, J.; Zakowski, S. Conceptualizing and Defining Public Health Emergency Preparedness. Am. J. Public Health 2007, 97, S9–S11. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No. | Health Evidence | Author(s) | Year | Topic | Country | Journal | Subject |
|---|---|---|---|---|---|---|---|
| 1 | M | Nelson et al. | 2007 | P | USA | Am J Public Health | Conceptualizing and defining public health emergency preparedness |
| 2 | M | Charania et al. | 2011 | Ed, P | Canada | Int J Circumpolar Health | The 2009 H1N1 pandemic response in remote First Nation communities of Subarctic Ontario: barriers and improvements from a health care services perspective |
| 3 | S | Charania et al. | 2012 | Ed, P | Canada | BMC Public Health | A community-based participatory approach and engagement process create culturally appropriate and community informed pandemic plans after the 2009 H1N1 influenza pandemic |
| 4 | S | Kim et al. | 2012 | Ed, Ps | S. Korea | J Med Intern Res | Development of a health information technology acceptance model using consumers’ health behavior intention |
| 5 | S | Cantey et al. | 2013 | Ed, P | USA | J Public Health Manag Pract | Public health emergency preparedness: lessons learned about monitoring of interventions from the National Association of County and City Health Official’s survey of nonpharmaceutical interventions for pandemic H1N1 |
| 6 | M | Rothstein | 2015 | E, P | USA | SSRN. Ind Health Law Rev | Legal and ethical considerations for modern quarantine |
| 7 | M | Bachtiger et al. | 2020 | P, Ps | UK | medRxiv | Government policy and reduced willingness to participate in app-based contact tracing |
| 8 | S | Joo et al. | 2020 | Ed, P, Ps | S. Korea | Service Business | Resolving the tension between full utilization of contact tracing app services and user stress as an effort to control the COVID-19 pandemic |
| 9 | M | Khorram-Manesh et al. | 2020 | E, P, Ed | Sweden | Disaster Med Public Health Prep | Association between welfare, developed infrastructure and prosperity of a country with infectious disease spread |
| 10 | M | Alanezi et al. | 2020 | P, Ed | Saudi Arabia | J Healthcare Leadership | A comparative study on the strategies adopted by several countries to contain the spread of the COVID-19 pandemic |
| 11 | M | Nazareth et al. | 2020 | P, Ed | UK | Lancet | Early lessons from a second COVID-19 lockdown in Leicester, UK |
| 12 | M | Abeler et al. | 2020 | P, E | UK | JMIR mHealth uHealth | COVID-19 contact tracing and data protection |
| 13 | M | Hernandez-Quevedo et al. | 2020 | P, E | European Union | The Health System Response Monitor | How do countries structure contact tracing operations and what is the role of apps? |
| 14 | M | Du et al. | 2020 | P, E | China | JMIR | COVID-19 contact tracing apps and gaps for international pandemic control |
| 15 | S | Korea CDC | 2020 | P | S. Korea | Osong Public Health Res | Contact transmission of COVID-19 in South Korea and novel investigation techniques for tracing contacts |
| 16 | M | Rowe et al. | 2020 | E, P | France | Eur J Info Sys | Contact-tracing apps and alienation in the age of COVID-19 |
| 17 | S | McGrail et al. | 2020 | E, P, Ps | Canada | AJPH | Contact-tracing apps and broader societal change |
| 18 | S | Bernard et al. | 2020 | E, Ps | UK | AJPH | An examination of the rise in government surveillance through mobile applications |
| 19 | M | Maghdid et al. | 2020 | P | Iraq | SN Computer Science | A smartphone-enabled approach to manage COVID-19 lockdown and economic crisis |
| 20 | M | Li et al. | 2020 | P | China | Lancet | Active case finding and case management: the key to tackling the COVID-19 pandemic |
| 21 | S | Guillon et al. | 2020 | E, Ps | France | Public Health | Attitudes and opinions on quarantine and support for a contact-tracing application in France during the COVID-19 outbreak |
| 22 | M | Hager et al. | 2020 | E, P | European Union | Int Political Sociolog | Collective discussion: toward critical approaches to intelligence as a social phenomenon |
| 23 | M | Abuhammad et al. | 2020 | E, Ed, P | Jordan | Patient Preference and Adherence | COVID-19 contact-tracing technology: acceptability and ethical issues of use |
| 24 | M | Reimer et al. | 2020 | E, P | Australia | Eur J Info Sys | Digital contact-tracing adoption in the COVID-19 pandemic |
| 25 | M | Basu et al. | 2020 | E | India | Camb Quart Healthcare Ethics | Mobile phones and contact tracing |
| 26 | W | Colins | 2020 | E, P | USA | Mondaq Bus Brief | Evolving considerations for multinational employers |
| 27 | W | Maati et al. | 2020 | E, P | Germany | Czech J Int Relations | Framing the pandemic and the rise of the digital surveillance state |
| 28 | M | Ekong et al. | 2020 | E, P | Nigeria | JMIR Mhealth Uhealth | Mobile positioning data contact tracing and patient privacy regulations |
| 29 | M | Dong et al. | 2020 | E, Ps | China | J Med Internet Res | Public emotions and rumors spread during the COVID-19 epidemic |
| 30 | S | Sfendla et al. | 2020 | Ps | Morocco | Health Secur | Factors associated with psychological distress and physical activity during the COVID-19 pandemic |
| 31 | S | Smith et al. | 2020 | E, P | UK | Public Health | Factors associated with adherence to self-isolation and lockdown measures in the UK: a cross-sectional survey |
| 32 | M | Shah et al. | 2020 | E | Nepal | Nepal Med Assoc | Combating the COVID-19 pandemic in Nepal: Ethical challenges in an outbreak |
| 33 | M | O’Callaghan et al. | 2020 | E, P | Ireland | Ir J Med Sci | A national survey of attitudes to COVID-19 digital contact tracing in the Republic of Ireland |
| 34 | M | Ye | 2020 | P, Ps | US | JMIR Pediatr Parent | Pediatric mental and behavioral health in the period of quarantine and social distancing with COVID-19 |
| 35 | M | Rothstein | 2020 | E, P | US | J Law Med and Ethic | The coronavirus pandemic: public health and American values. |
| 36 | M | Torous et al. | 2020 | P, Ps | US | JMIR Mental Health | Digital mental health and COVID-19: using technology today to accelerate the curve on access and quality tomorrow |
| 37 | S | Tambo et al. | 2020 | Ed, P | Cameron | Global Health J | Early stage risk communication and community engagement (RCCE) strategies and measures against the coronavirus disease 2019 (COVID-19) pandemic crisis |
| 38 | W | Simon | 2020 | E | USA | Survival | Subtle connections: pandemic and the authoritarian impulse |
| 39 | M | EU | 2021 | E, P | European Union | Commissioners’ Office Web | Guide to the general data protection regulation (GDPR) |
| 40 | M | Shuja | 2021 | E | Pakistan | Applied Intelligence | COVID-19 open source data sets |
| 41 | M | Baumgart et al. | 2021 | Ed, P | Canada | NPI Digital Medicine | Digital advantage in the COVID-19 response: perspective from Canada |
| 42 | M | Jacob et al. | 2021 | P | Canada | Policy design and practice | The adoption of contact tracing applications for COVID-19 by the European governments |
| 43 | S | Sowmiya et al. | 2021 | E | India | SN Computer Science | A survey on security and privacy issues in contact tracing applications |
| 44 | M | Gerli et al. | 2021 | P | UK | Government Info Quarterly | The public value of eHealth application in a pandemic |
| 45 | M | Niccolai et al. | 2021 | P | USA | AJPH | Rapid establishment of a volunteer contact tracing program for COVID-19 |
| 46 | M | Thoung et al. | 2021 | P | Vietnam | BMJ Global Health | Public safety and response to the COVID-19 epidemic in Vietnam |
| 47 | M | Hassandoust et al. | 2021 | Ed, P | New Zealand | JAMIA | Individuals’ privacy concerns and adoption of contact tracing mobile applications in a pandemic |
| 48 | S | Bradshaw et al. | 2021 | Ps | Australia | Frontiers in Psychology | The information safety assurance increases intentions to use COVID-19 contact tracing applications |
| 49 | M | Legendre et al. | 2021 | P | Switzerland | arXiv | Contact tracing technologies and cyber risks |
| 50 | S | CDC | 2021 | P | USA | Web | Contact tracing resources |
| 51 | S | Williams et al. | 2021 | E, Ps | UK | Health Expectations | Public attitudes towards COVID-19 contact tracing apps |
| 52 | S | Chen et al. | 2021 | P, Ps | USA | Geriatr Nurs | Reactions to COVID-19, information and technology use, and social connectedness among older adults with pre-frailty and frailty |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khorram-Manesh, A.; Dulebenets, M.A.; Goniewicz, K. Implementing Public Health Strategies—The Need for Educational Initiatives: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 5888. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115888
Khorram-Manesh A, Dulebenets MA, Goniewicz K. Implementing Public Health Strategies—The Need for Educational Initiatives: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(11):5888. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115888
Chicago/Turabian StyleKhorram-Manesh, Amir, Maxim A. Dulebenets, and Krzysztof Goniewicz. 2021. "Implementing Public Health Strategies—The Need for Educational Initiatives: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 11: 5888. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115888