
Medication for Opioid Use Disorder Service Provision and Telephone Counseling: A Concurrent Mixed-Methods Approach

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Data Collection
2.2. Concurrent Mixed-Methods Analysis Approach
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Medical Association. Issue Brief: Reports of Increases in Opioid-and Other Drug-Related Overdose and Other Concerns during COVID Pandemic. AMA Advocacy Resource Center Updated. 2020: 2020–2010. Available online: http://www.asapnys.org/wp-content/uploads/2020/07/Issue-brief_-Reports-of-increases-in-opioid-related-overdose-and-other-concerns-during-COVID-pandemic.pdf (accessed on 1 May 2021).
- Holland, K.M.; Jones, C.; Vivolo-Kantor, A.M.; Idaikkadar, N.; Zwald, M.; Hoots, B.; Yard, E.; D’Inverno, A.; Swedo, E.; Chen, M.S.; et al. Trends in US Emergency Department Visits for Mental Health, Overdose, and Violence Outcomes before and during the COVID-19 Pandemic. JAMA Psychiatry 2021, 78, 372. [Google Scholar] [CrossRef] [PubMed]
- Livingston, N.A.; Ameral, V.; Banducci, A.N.; Weisberg, R.B. Unprecedented need and recommendations for harnessing data to guide future policy and practice for opioid use disorder treatment following COVID-19. J. Subst. Abus. Treat. 2021, 122, 108222. [Google Scholar] [CrossRef]
- Drug Enforcement Administration. Implementation of the Ryan Haight Online Pharmacy Consumer Protection Act of 2008. Interim final rule with request for comments. Fed. Regist. 2009, 4, 15595–15625. [Google Scholar]
- Bliley, T.H.R. 2634—Drug Addiction Treatment Act of 2000. 2000. Available online: https://www.congress.gov/bill/106th-congress/house-bill/2634 (accessed on 1 May 2021).
- Electronic Code of Federal Regulations. 42CFR Part 8. 2021. Available online: https://www.ecfr.gov/cgi-bin/retrieveECFR?gp=3&SID=7282616ac574225f795d5849935efc45&ty=HTML&h=L&n=pt42.1.8&r=PAR (accessed on 1 May 2021).
- Koonin, L.M.; Hoots, B.; Tsang, C.A.; Leroy, Z.; Farris, K.; Jolly, B.; Antall, P.; McCabe, B.; Zelis, C.B.; Tong, I.; et al. Trends in the use of telehealth during the emergence of the COVID-19 pandemic—United States, January–March 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1595. [Google Scholar] [CrossRef] [PubMed]
- Hansel, T.C.; Saltzman, L.Y.; Bordnick, P.S. Behavioral Health and Response for COVID-19. Disaster Med. Public Health Prep. 2020, 14, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Pinals, D.A.; Hepburn, B.; Parks, J.; Stephenson, A.H. The Behavioral Health System and Its Response to COVID-19: A Snapshot Perspective. Psychiatr. Serv. 2020, 71, 1070–1074. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.H.; Caudill, R. Remote Treatment Delivery in Response to the COVID-19 Pandemic. Psychother. Psychosom. 2020, 89, 130–132. [Google Scholar] [CrossRef]
- Backhaus, A.; Agha, Z.; Maglione, M.L.; Repp, A.; Ross, B.; Zuest, D.; Rice-Thorp, N.M.; Lohr, J.; Thorp, S.R. Videoconferencing psychotherapy: A systematic review. Psychol. Serv. 2012, 9, 111–131. [Google Scholar] [CrossRef]
- Bashshur, R.L.; Shannon, G.W.; Bashshur, N.; Yellowlees, P.M. The Empirical Evidence for Telemedicine Interventions in Mental Disorders. Telemed. E-Health 2016, 22, 87–113. [Google Scholar] [CrossRef] [Green Version]
- Batastini, A.B.; Jones, A.C.T.; Lester, M.E.; Davis, R.M. Initiation of a multidisciplinary telemental health clinic for rural justice-involved populations: Rationale, recommendations, and lessons learned. J. Community Psychol. 2020, 48, 2156–2173. [Google Scholar] [CrossRef]
- Kruse, C.S.; Krowski, N.; Rodriguez, B.; Tran, L.; Vela, J.; Brooks, M. Telehealth and patient satisfaction: A systematic review and narrative analysis. BMJ Open 2017, 7, e016242. [Google Scholar] [CrossRef] [PubMed]
- Huskamp, H.A.; Busch, A.B.; Souza, J.; Uscher-Pines, L.; Rose, S.; Wilcock, A.; Landon, B.E.; Mehrotra, A. How is telemedicine being used in opioid and other substance use disorder treat-ment? Health Aff. 2018, 37, 1940–1947. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Casteel, D.; Shigekawa, E.; Weyrich, M.S.; Roby, D.H.; McMenamin, S.B. Telemedicine-delivered treatment interventions for substance use disorders: A systematic review. J. Subst. Abus. Treat. 2019, 101, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Tarp, K.; Bojesen, A.B.; Mejldal, A.; Nielsen, A.S. Effectiveness of optional videoconferencing-based treatment of alcohol use dis-orders: Randomized controlled trial. JMIR Ment. Health 2017, 4, e38. [Google Scholar] [CrossRef]
- King, V.L.; Brooner, R.K.; Peirce, J.M.; Kolodner, K.; Kidorf, M.S. A randomized trial of Web-based videoconferencing for substance abuse counseling. J. Subst. Abus. Treat. 2014, 46, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Eibl, J.K.; Gauthier, G.; Pellegrini, D.; Daiter, J.; Varenbut, M.; Hogenbirk, J.C.; Marsh, D.C. The effectiveness of telemedicine-delivered opioid agonist therapy in a supervised clinical setting. Drug Alcohol Depend. 2017, 176, 133–138. [Google Scholar] [CrossRef]
- Arnow, B.A.; Steidtmann, D.; Blasey, C.; Manber, R.; Constantino, M.J.; Klein, D.N.; Markowitz, J.C.; Rothbaum, B.O.; Thase, M.E.; Fisher, A.J.; et al. The relationship between the therapeutic alliance and treatment outcome in two distinct psychotherapies for chronic depression. J. Consult. Clin. Psychol. 2013, 81, 627–638. [Google Scholar] [CrossRef] [Green Version]
- Sugarman, D.E.; Horvitz, L.E.; Greenfield, S.F.; Busch, A.B. Clinicians’ Perceptions of Rapid Scale-up of Telehealth Services in Outpatient Mental Health Treatment. Telemed. E-Health 2021. [Google Scholar] [CrossRef]
- Connolly, S.L.; Miller, C.J.; Lindsay, J.A.; Bauer, M.S. A systematic review of providers’ attitudes toward telemental health via videoconferencing. Clin. Psychol. Sci. Pract. 2020, 27. [Google Scholar] [CrossRef]
- Thomas, N.; McDonald, C.; De Boer, K.; Brand, R.M.; Nedeljkovic, M.; Seabrook, L. Review of the current empirical literature on using videoconferencing to deliver individual psychotherapies to adults with mental health problems. Psychol. Psychother. Theory Res. Pract. 2021. [Google Scholar] [CrossRef]
- Nittari, G.; Khuman, R.; Baldoni, S.; Pallotta, G.; Battineni, G.; Sirignano, A.; Amenta, F.; Ricci, G. Telemedicine Practice: Review of the Current Ethical and Legal Challenges. Telemed. E-Health 2020, 26, 1427–1437. [Google Scholar] [CrossRef] [Green Version]
- Gilmore, A.K.; Ward-Ciesielski, E.F. Perceived risks and use of psychotherapy via telemedicine for patients at risk for suicide. J. Telemed. Telecare 2017, 25, 59–63. [Google Scholar] [CrossRef]
- Creswell, J.W.; Clark, V.L.P. Designing and Conducting Mixed Methods Research; Sage Publications: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- IBM SPSS Statistics for Windows, [Computer Program], Version Version 26.0; IMB Corp.: Armonk, NY, USA, 2019.
- Donelan, K.; Barreto, E.A.; Sossong, S.; Michael, C.; Estrada, J.J.; Cohen, A.B.; Wozniak, J.; Schwamm, L.H. Patient and clinician experiences with telehealth for patient follow-up care. Am. J. Manag. Care 2019, 25, 40–44. [Google Scholar]
- Petersen, D.; Salazar, B.; Kertz, S.J. Therapist and Treatment-Seeking Students’ Perceptions of Telemental Health. J. Technol. Behav. Sci. 2019, 5, 113–120. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Selmes, T. Why don’t patients attend their appointments? Maintaining engagement with psychiatric services. Adv. Psychiatr. Treat. 2007, 13, 423–434. [Google Scholar] [CrossRef] [Green Version]
- Rubin, R. Using Telemedicine to Treat Opioid Use Disorder in Rural Areas. JAMA 2019, 322, 1029. [Google Scholar] [CrossRef] [PubMed]
- Marsh, J.C.; Angell, B.; Andrews, C.M.; Curry, A. Client-Provider Relationship and Treatment Outcome: A Systematic Review of Substance Abuse, Child Welfare, and Mental Health Services Research. J. Soc. Soc. Work Res. 2012, 3, 233–267. [Google Scholar] [CrossRef] [Green Version]
- Leibert, T.W.; Dunne-Bryant, A. Do Common Factors Account for Counseling Outcome? J. Couns. Dev. 2015, 93, 225–235. [Google Scholar] [CrossRef]
- Connors, G.J.; Carroll, K.M.; DiClemente, C.C.; Longabaugh, R.; Donovan, D.M. The therapeutic alliance and its relationship to alcoholism treatment participation and outcome. J. Consult. Clin. Psychol. 1997, 65, 588–598. [Google Scholar] [CrossRef] [PubMed]
- Dundon, W.; Pettinati, H.; Lynch, K.; Xie, H.; Varillo, K.; Makadon, C.; Oslin, D. The therapeutic alliance in medical-based interventions impacts outcome in treating alcohol dependence. Drug Alcohol Depend. 2008, 95, 230–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagnild, G.; Leenknecht, C.; Zauher, J. Psychiatrists’ Satisfaction with Telepsychiatry. Telemed. E-Health 2006, 12, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Yellowlees, P.; Nakagawa, K.; Pakyurek, M.; Hanson, A.; Elder, J.; Kales, H.C. Rapid Conversion of an Outpatient Psychiatric Clinic to a 100% Virtual Telepsychiatry Clinic in Response to COVID-19. Psychiatr. Serv. 2020, 71, 749–752. [Google Scholar] [CrossRef] [PubMed]
- Reay, R.E.; Looi, J.C.; Keightley, P. Telehealth mental health services during COVID-19: Summary of evidence and clinical practice. Australas. Psychiatry 2020, 28, 514–516. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Predictor | n | Less | The Same | More |
|---|---|---|---|---|
| Anxiety | 40 | 13 (32.5) | 18 (45.0) | 9 (22.5) |
| Depression | 40 | 13 (32.5) | 23 (57.5) | 4 (10.0) |
| Anger | 37 | 17 (45.9) | 16 (43.2) | 4 (10.8) |
| Substance | 40 | 11 (27.5) | 22 (55.0) | 7 (17.5) |
| Recovery | 40 | 11 (27.5) | 21 (52.5) | 8 (20.0) |
| Comfort | 42 | 9 (21.4) | 28 (66.7) | 5 (11.9) |
| Convenience | 42 | 13 (31.0) | 8 (19.0) | 21 (50.0) |
| Relationship with Patients | 42 | 4 (9.5) | 25 (59.5) | 13 (31.0) |
| Very Dissatisfied/Dissatisfied | Neither | Somewhat/Very Satisfied | ||
| Overall Satisfaction with Telephone Counseling | 42 | 5 (11.9) | 8 (19.0) | 29 (69.0) |
| Predictor | M ± SD | B | SE | Wald | df | p | Exp(B) | 95% CI of Exp(B) |
|---|---|---|---|---|---|---|---|---|
| Anxiety | 0.310 | 0.544 | 0.325 | 1 | 0.569 | 1.363 | (0.470, 3.955) | |
| Positive (n = 8) Mixed/Negative (n = 30) | 2.00 ± 0.76 1.83 ±.75 | |||||||
| Depression | 0.499 | 0.678 | 0.541 | 1 | 0.462 | 1.646 | (0.436, 6.218) | |
| Positive (n = 8) Mixed/Negative (n = 30) | 1.88 ± 0.64 1.70 ± 0.60 | |||||||
| Anger | 0.850 | 0.744 | 1.306 | 1 | 0.253 | 2.339 | (0.545, 10.050) | |
| Positive (n = 6) Mixed/Negative (n = 29) | 1.83 ± 0.41 1.52 ± 0.63 | |||||||
| Substance | 1.725 | 0.768 | 5.049 | 1 | 0.025 * | 5.611 | (1.246, 25.255) | |
| Positive (n = 8) Mixed/Negative (n = 30) | 2.38 ± 0.74 1.73 ± 0.58 | |||||||
| Recovery | 1.472 | 0.703 | 4.382 | 1 | 0.036 * | 4.360 | (1.098, 17.306) | |
| Positive (n = 8) Mixed/Negative (n = 30) | 2.38 ± 0.74 1.77 ± 0.63 | |||||||
| Comfort | 1.683 | 0.859 | 3.845 | 1 | 0.049 * | 5.384 | (1.001, 28.971) | |
| Positive (n = 9) Mixed/Negative (n = 30) | 2.22 ± 0.44 1.77 ± 0.57 | |||||||
| Convenience | 2.143 | 0.973 | 4.854 | 1 | 0.028 * | 8.523 | (1.267, 57.366) | |
| Positive (n = 9) Mixed/Negative (n = 30) | 2.89 ± 0.33 1.90 ± 0.88 | |||||||
| Relationship with Patients | 1.571 | 0.754 | 4.339 | 1 | 0.037 * | 4.812 | (1.097, 21.105) | |
| Positive (n = 9) Mixed/Negative (n = 30) | 2.56 ± 0.53 2.07 ± 0.58 | |||||||
| Overall Satisfaction | 1.543 | 0.672 | 5.269 | 1 | 0.022 * | 4.677 | (1.253, 17.457) | |
| Positive (n = 9) Mixed/Negative (n = 30) | 4.44 ± 0.53 3.47 ± 1.07 |
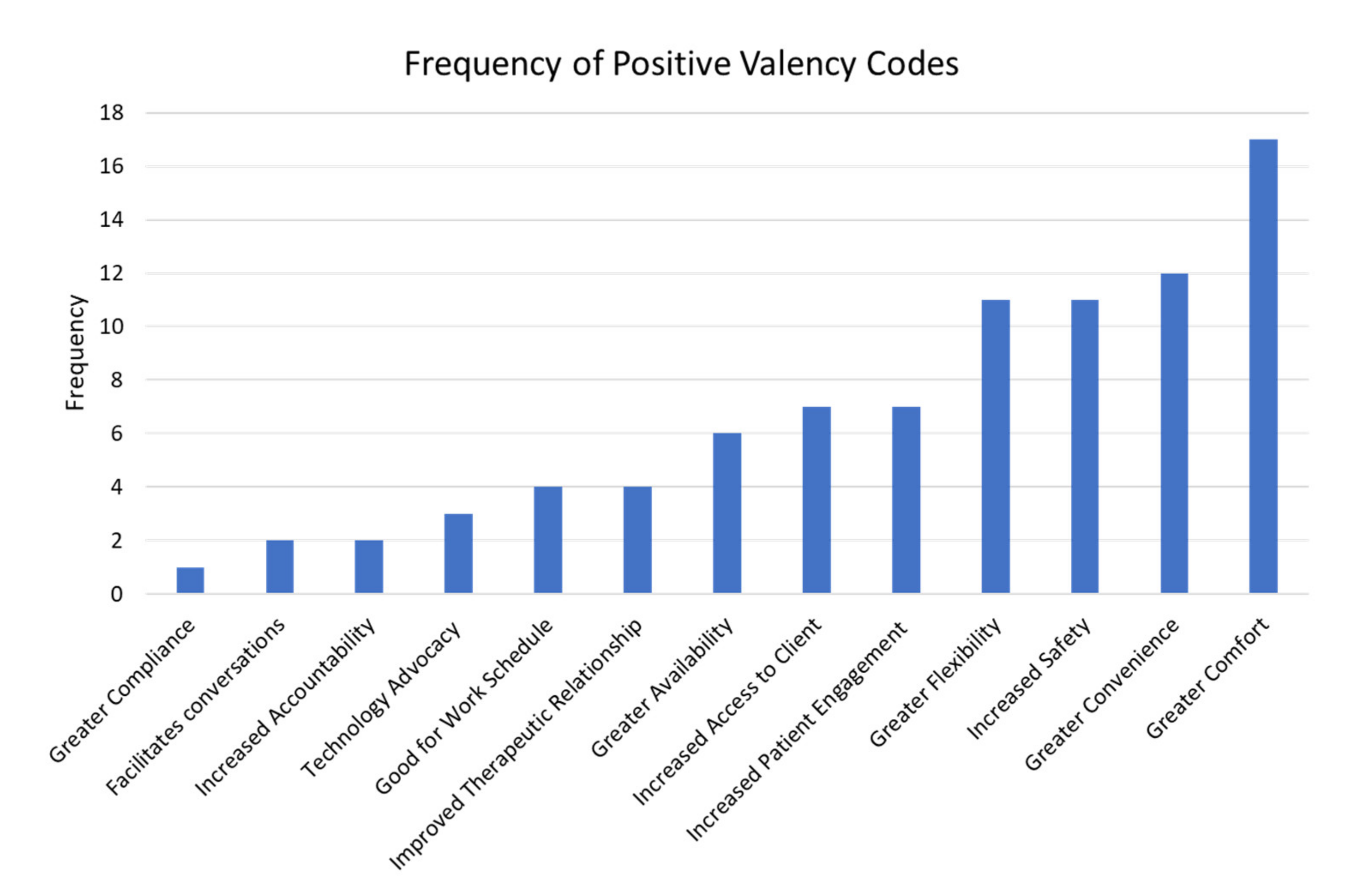
| Example Quote | Name of Code |
|---|---|
| Positive Valency Theme | |
| More convenient as patients who are typically rushed to dose and leave (because of transportation or whatnot) | Convenience |
| I think some of the patients are better able to express themselves without having the feeling of being stared at or judged in some way in an office setting. | Facilitates Conversations |
| It is easier for patients who work early or receive rides to the clinic to complete sessions, as there is more flexibility. Patients seem to be more engaged in sessions because they are not feeling rushed. | Good for Work Schedule |
| Patients are more comfortable with phone sessions and availability is better. | Greater Availability |
| I think it has provided more comfort to clients and easier access to clinical staff if necessary compared to counseling requirements needing to be completed in person. | Greater Comfort |
| I get more compliance with sessions with some patients/clients. | Greater Compliance |
| i am able to coordinate session times with more flexibility throughout the day rather than being dependent on the dosing hour window | Greater Flexibility |
| Keeping in touch with patients when they are outside the clinic has helped a lot of patients who have little/no supports otherwise. I feel that my rapport with my clients has increased substantially over the past several months due to telephonic counseling. | Improved Therapeutic Relationship |
| … I’ve also had the opportunity to touch base with my patients more frequently since we’re not not constrained to dosing schedules (Ex. maybe only in the clinic 2–4 times per month) and we don’t have to juggle multiple patients waiting to be seen when they come to the clinic. | Increased Access to Client |
| For some patients it is easier for them to take accountability for their use over the telephone and work on recovery supports and treatment goals. | Increased Accountability |
| Patients are more engaged in phone sessions and are not in a rush to end session. | Increased Patient Engagement |
| Tele-health calling is a way to contact patients and provide safe effective measure of counseling and release for our patients. Allowing them to remain at a safe distance for all involved. | Increased Safety |
| … I think in the future when Covid-19 is no longer a major threat and we do face to face office visits we should keep either telephone, or Zoom individual sessions also in case someone has no ride or we have a snow day etc to stop having to cancel sessions. | Technology Advocacy |
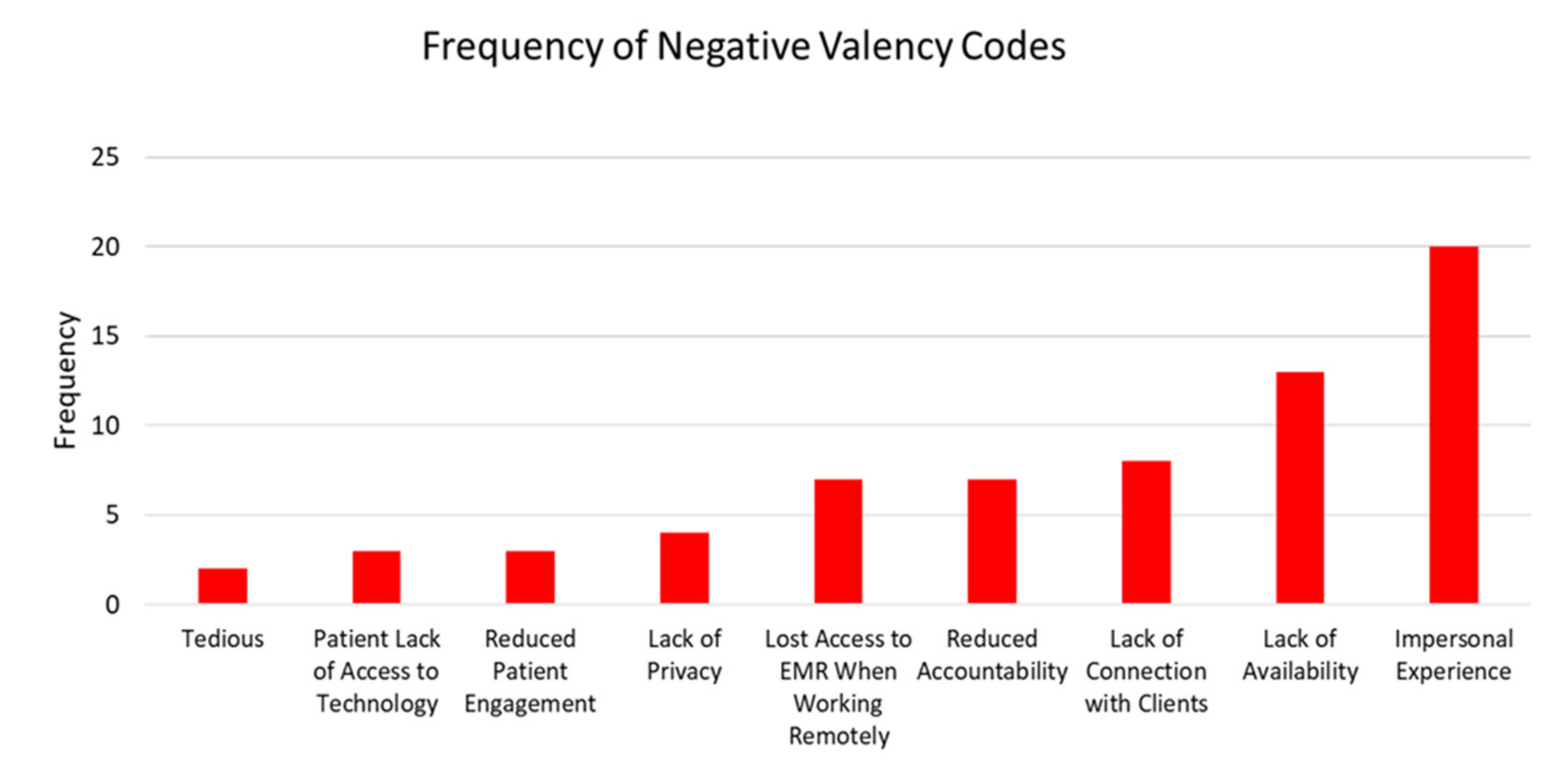
| Negative Valency Theme | |
| I don’t think telephone counseling sessions are as valuable as face-to-face counseling. | Impersonal Experience |
| I don’t mind doing telehealth sessions, but it is a lot harder to reach patient’s. I feel like I am always scrambling near the end of the month to see people who don’t answer the phone. | Lack of Availability |
| …patients often have limited privacy, this is amplified by patients children and family member being at home more often due to COVID-19 resulting in more adults and children being at home due to loss of employment and distance learning for students… | Lack of Privacy |
| All services provided would have been more manageable with off site access to SMART system. Moving forward should tele counseling continue, off site access would enable counselors to complete documentation more thoroughly in order to manage their caseload more effectively. While also promoting better communication between staff. | Lost Access to EMR When Working Remotely |
| The counselor has to be straight forward and ask are you depressed? how is your anxiety? are you using any substances? Its really the same on the phone. | No Difference |
| phones not working, voice mail box is full, patients cannot always pay phone bill on time, patients don’t always check voice mail | Patient Lack of Access to Technology |
| Lessens rapport, accountability, structure and consistency. All essential in the road to recovery and abstinence. | Reduced Accountability |
| I think the conversations telephonically can be just as supportive as face to face; however some patients do not engage in phone conversations as well as in person. | Reduced Patient Engagement |
| It works on a level but then it does not. It was fine at first but now it is very tedious to do the phone calls | Tedious |
| I think overall it is harder to provide clinical care as effectively over the phone as it would be in person. Body language and facial expressions can give us a lot of information, it can make it more difficult not having that in front of us to observe. However, given the circumstances I think it is the best alternative we have available. | Telephone Counseling Lacks Communication/Connection With Clients |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, R.; Kang, A.W.; DeBritz, A.A.; Walton, M.R.; Hoadley, A.; DelaCuesta, C.; Hurley, L. Medication for Opioid Use Disorder Service Provision and Telephone Counseling: A Concurrent Mixed-Methods Approach. Int. J. Environ. Res. Public Health 2021, 18, 6163. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116163
Martin R, Kang AW, DeBritz AA, Walton MR, Hoadley A, DelaCuesta C, Hurley L. Medication for Opioid Use Disorder Service Provision and Telephone Counseling: A Concurrent Mixed-Methods Approach. International Journal of Environmental Research and Public Health. 2021; 18(11):6163. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116163
Chicago/Turabian StyleMartin, Rosemarie, Augustine W. Kang, Audrey A. DeBritz, Mary R. Walton, Ariel Hoadley, Courtney DelaCuesta, and Linda Hurley. 2021. "Medication for Opioid Use Disorder Service Provision and Telephone Counseling: A Concurrent Mixed-Methods Approach" International Journal of Environmental Research and Public Health 18, no. 11: 6163. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116163