
Exposure to Second-Hand Smoke in Public Places and Barriers to the Implementation of Smoke-Free Regulations in The Gambia: A Population-Based Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
2.2. Study Instrument/Questionnaire
2.3. Sampling Framework and Sample Size
2.4. Exposure and Outcome Measures
2.5. Data Management and Analysis
3. Results
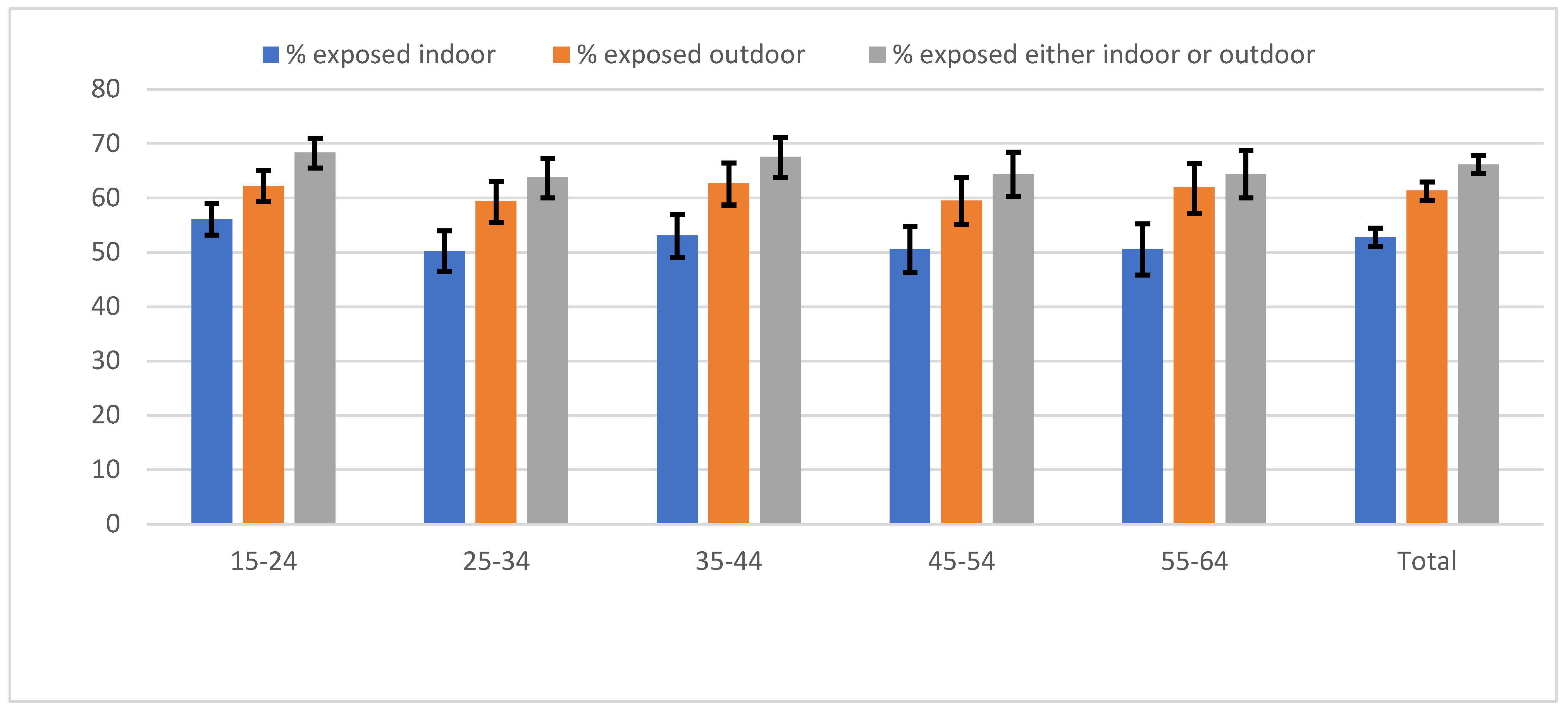
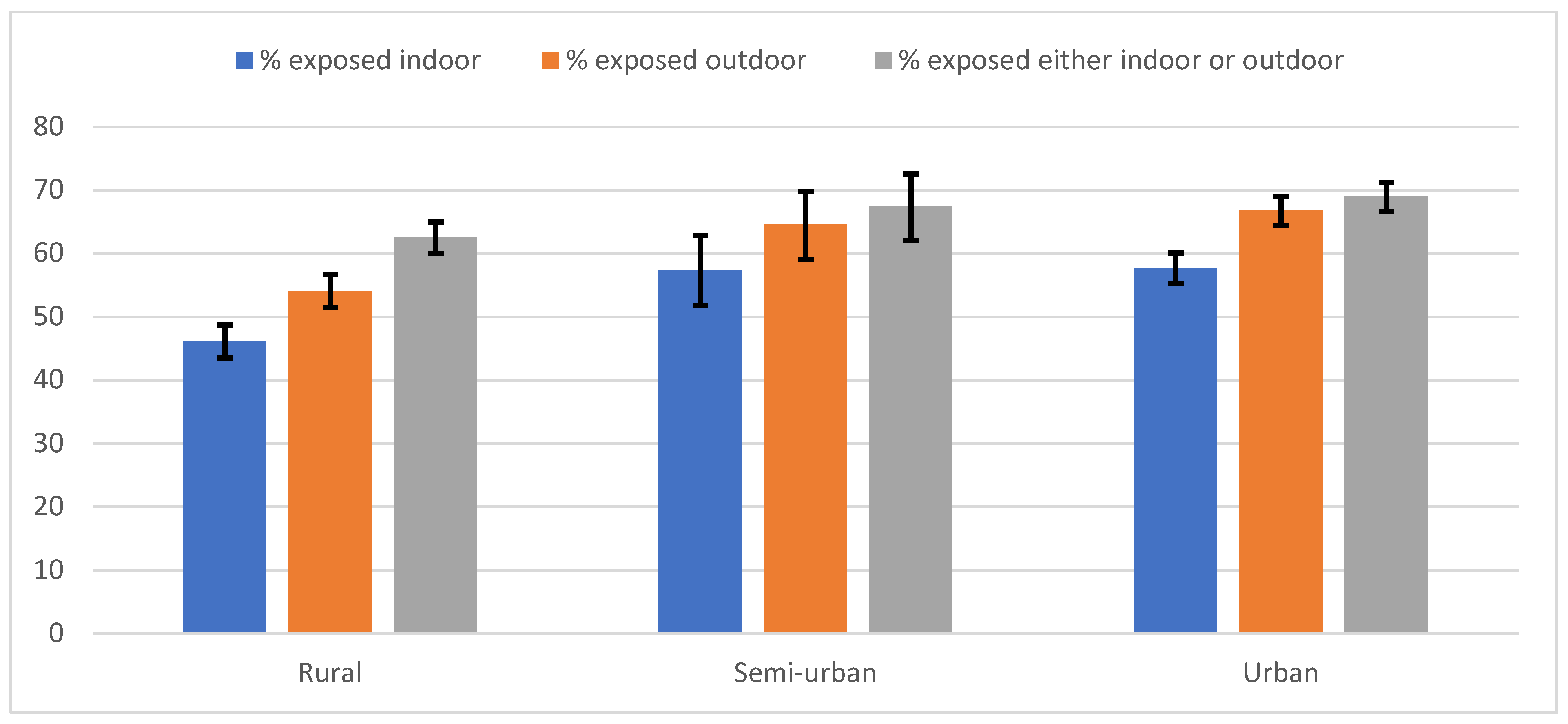
3.1. The Prevalence of Exposure to Second-Hand Smoke
3.2. Factors Associated with Exposure to Second-Hand Smoke in Indoor and Outdoor Public Places
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Öberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Prüss-Ustün, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet 2011, 377, 139–146. [Google Scholar] [CrossRef]
- World Health Organization. WHO Framework Convention on Tobacco Controli; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). The Gambia 2017 Global Youth Tobacco Survey (GYTS) Factsheet; CDC: Atlanta, GA, USA, 2017. [Google Scholar]
- Jallow, I.K.; Britton, J.; Langley, T. Prevalence and factors associated with exposure to secondhand smoke (SHS) among young people: A cross-sectional study from the Gambia. BMJ Open 2018, 8, e019524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Republic of The Gambia. Prohibition of Smoking (Public Places) Act; The Gambia Government: Banjul, The Gambia, 1998.
- Campaign for Tobacco-Free Kids. Tobacco Control Laws: Legislation by Country. 2018. Available online: https://www.tobaccocontrollaws.org/legislation/country/gambia/summary (accessed on 10 August 2019).
- Republic of The Gambia. Tobacco Control Regulations 2019; The Gambia Government: Banjul, The Gambia, 2019.
- Jasseh, M.; Gomez, P.; Greenwood, B.M.; Howie, S.R.; Scott, S.; Snell, P.C.; Bojang, K.; Cham, M.; Corrah, T.; D’Alessandro, U. Health & Demographic Surveillance System Profile: Farafenni Health and Demographic Surveillance System in The Gambia. Int. J. Epidemiol. 2015, 44, 837–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. World Health Organization STEPS Surveillance Manual: The WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- World Health Organization. Global Adult Tobacco Survey (GATS) Core Questionnaire with Optional Questions. Version 2.0. 2010. Available online: https://www.who.int/tobacco/surveillance/en_tfi_gats_corequestionnairewithoptionalquestions_v2_FINAL_03Nov2010.pdf (accessed on 16 July 2019).
- Cham, B.; Scholes, S.; Fat, L.N.; Badjie, O.; Mindell, J.S. Burden of hypertension in The Gambia: Evidence from a national World Health Organization (WHO) STEP survey. Int. J. Epidemiol. 2018, 47, 860–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngobese, S.P.; Egbe, C.O.; Londani, M.; Ayo-Yusuf, O.A. Non-Smoker’s Exposure to Second-Hand Smoke in South Africa during 2017. Int. J. Environ. Res. Public Health 2020, 17, 8112. [Google Scholar] [CrossRef] [PubMed]
- Tripathy, J.P. Secondhand smoke exposure at home and public places among smokers and non-smokers in India: Findings from the Global Adult Tobacco Survey 2016–2017. Environ. Sci. Pollut. Res. 2019, 27, 6033–6041. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lim, S.; Kim, J.; Lee, H.; June, K.J. Socioeconomic disparities in household secondhand smoke exposure among non-smoking adolescents in the Republic of Korea. Glob. Public Health 2015, 12, 1104–1121. [Google Scholar] [CrossRef] [PubMed]
- Nazar, G.P.; Lee, J.T.; Arora, M.; Millett, C. Socioeconomic Inequalities in Secondhand Smoke Exposure at Home and at Work in 15 Low- and Middle-Income Countries. Nicotine Tob. Res. 2015, 18, 1230–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wipfli, H.L.; Samet, J.M. Second-hand smoke’s worldwide disease toll. Lancet 2011, 377, 101–102. [Google Scholar] [CrossRef]
- Drope, J.; Eriksen, M.P.; Mackay, J.; Ross, H. The Tobacco Atlas; American Cancer Society Inc.; Vital Strategies, A Global Public Health Organization: Atlanta, GA, USA, 2018. [Google Scholar]



{kind=link}
{kind=link}
| Variable | N | % |
|---|---|---|
| Age group | ||
| 15–24 | 1101 | 32.9 |
| 25–34 | 679 | 20.3 |
| 35–44 | 616 | 18.4 |
| 45–54 | 514 | 15.4 |
| 55–64 | 433 | 13.0 |
| Mean age | 34.6 ± 14.5 | |
| Sex | ||
| Male | 1175 | 35.2 |
| Female | 2168 | 64.9 |
| Residence | ||
| Rural | 1634 | 48.9 |
| Semi-urban | 305 | 9.1 |
| Urban | 1404 | 42.0 |
| Marital status | ||
| Single (Never married) | 989 | 29.6 |
| Married | 2222 | 66.5 |
| Divorced/Separated | 38 | 1.1 |
| Widowed | 94 | 2.8 |
| Ethnicity | ||
| Wollof | 1569 | 46.9 |
| Fula | 716 | 21.4 |
| Mandinka | 920 | 27.5 |
| Others | 138 | 4.1 |
| Education | ||
| No formal education | 284 | 8.5 |
| Lower Basic | 288 | 8.6 |
| Upper Basic/Jun Sec | 384 | 11.5 |
| Senior Sec/College/Uni | 358 | 10.7 |
| Madrassa | 655 | 19.6 |
| Quranic school | 1349 | 40.4 |
| Senegalese | 25 | 0.8 |
| Household income (in Dalasi) | ||
| Under 10,000 | 640 | 19.1 |
| 10,000–19,999 | 508 | 15.2 |
| 20,000–29,999 | 383 | 11.5 |
| 30,000–39,999 | 266 | 8.0 |
| 40,000–50,000 | 722 | 21.6 |
| Do not know | 824 | 24.7 |
| Current smoking | ||
| Yes | 177 | 5.2 |
| No | 3166 | 94.7 |
| Awareness of smoking in public regulations | ||
| Aware | 2095 | 62.7 |
| Not aware | 1248 | 37.3 |
| Model I Indoor Public Places | Model II Outdoor Public Places | Model III Indoor and/or Outdoor Public Places | ||||
|---|---|---|---|---|---|---|
| OR | AOR | OR | AOR | OR | AOR | |
| Age group | ||||||
| 15–24 | Reference | Reference | Reference | Reference | Reference | Reference |
| 25–34 | 1.20(1.03–1.41) * | 1.05(0.81–1.35) | 1.12(0.95–1.31) | 1.04(0.81–1.35) | 1.13(0.95–1.34) | 1.05 (0.81–1.37) |
| 35–44 | 1.02(0.86–1.21) | 0.78(0.59–1.04) | 0.92(0.77–1.10) | 0.78(0.59–1.04) | 0.92(0.77–1.11) | 0.74(0.55–1.00) |
| 45–54 | 1.18(0.98–1.41) | 0.87(0.64–1.18) | 1.06(0.87–1.28) | 0.90(0.67–1.23) | 1.13(0.93–1.37) | 0.88(0.64–1.20) |
| 55–64 | 1.18(0.97–1.44) | 0.95 (0.69–1.31) | 0.97(0.79–1.19) | 0.90(0.65–1.25) | 1.11(0.90–1.37) | 0.95(0.68–1.33) |
| Sex | ||||||
| Female | Reference | Reference | Reference | Reference | Reference | Reference |
| Male | 2.02(1.78–2.29) *** | 1.78(1.51–2.10) *** | 2.62(2.29–3.01) *** | 2.40(2.02–2.86) *** | 2.78(2.40–3.21) *** | 2.49 (2.08–2.99) *** |
| Residence | ||||||
| Rural | Reference | Reference | Reference | Reference | ||
| Semi–urban | 1.13(0.92–1.38) | 0.95(0.72–1.24) | 1.10(0.89–1.35) | 1.09(0.82–1.45) | 1.02(0.82–1.26) | 1.04 (0.78–2.25) |
| Urban | 1.44(1.28–1.63) | 2.68 (2.24–3.21) *** | 1.55(1.37–1.76) *** | 2.34(1.96–2.80) *** | 1.23(1.08–1.40) ** | 1.88 (1.56–2.25) *** |
| Marital status | ||||||
| Single | Reference | Reference | Reference | Reference | Reference | Reference |
| Married | 1.41(1.23–1.61) *** | 1.13(0.89–1.45) | 1.27(1.11–1.46) *** | 1.05(0.81–1.35) | 1.44(1.25–1.66) *** | 1.09 (0.84–1.41) |
| Divorced/Separated | 1.76(1.05–2.96) * | 1.64(0.79–3.39) | 1.50(0.89–2.52) | 1.00(0.50–2.02) | 1.92(0.91.13–3.23) * | 1.48(0.73–2.99) |
| Widowed | 2.26(1.55–3.31) *** | 1.13(0.67–1.91) | 1.98(1.37–2.87) *** | 1.28(0.77–2.15) | 2.38(1.64–3.46) *** | 1.35(0.80–2.27) |
| Ethnicity | ||||||
| Wollof | Reference | Reference | Reference | Reference | Reference | Reference |
| Fula | 1.15(0.98–1.34) | 1.28(1.06–1.55) ** | 1.02(0.88–1.20) | 1.16(0.96–1.41) | 1.02(0.87–1.19) | 1.16(0.95–1.41) |
| Mandinka | 0.44(0.38–0.51) *** | 0.43(0.36–0.52) *** | 0.72(0.63–0.84) ** | 0.73(0.60–0.89) ** | 0.56(0.48–0.66) *** | 0.62(0.50–0.75) *** |
| Others | 0.49(0.36–0.66) *** | 0.53(0.36–0.78) *** | 0.56(0.40–0.77) ** | 0.60(0.40–0.90) ** | 0.48(0.34–0.68) *** | 0.57(0.37–0.88) * |
| Education | ||||||
| No formal education | Reference | Reference | Reference | Reference | Reference | Reference |
| Lower Basic | 0.55(0.41–0.75) *** | 0.62 (0.43–0.91) * | 0.64(0.47–0.88) ** | 0.67(0.46–0.98) * | 0.61(0.44–0.84) ** | 0.67(0.45–0.99) * |
| Upper basic/Jun Sec | 0.57(0.43–0.75) *** | 0.58(0.41–0.83) ** | 0.70(0.52–0.93) * | 0.68(0.48–0.96) * | 0.61(0.44–82) *** | 0.60(0.42–0.88) ** |
| Senior Sec/College/Uni | 0.65(0.49–0.86) *** | 0.63(0.44–0.89) ** | 0.60(0.45–0.81) ** | 0.57(0.40–0.81) ** | 0.57(0.42–0.78) *** | 0.58(0.40–0.84) ** |
| Madrassa | 0.96(0.74–1.24) | 1.08(0.79–1.47) | 0.91(0.75–1.21) | 0.92(0.67–1.28) | 1.03(0.79–1.35) | 1.01(0.74–1.40) |
| Quranic school | 1.16(0.92–1.47) | 1.27(0.96–1.69) | 0.95(0.75–1.21) | 0.99(0.75–1.31) | 1.09(0.85–1.39) | 1.10(0.83–1.46) |
| Senegalese | 0.88(0.43–1.82) | 0.70(0.30–1.66) | 0.62(0.29–1.36) | 0.59(0.251.42) | 0.70(0.32–1.57) | 0.71(0.29–1.72) |
| Household income | ||||||
| Under 10,000 | Reference | Reference | Reference | Reference | Reference | Reference |
| 10,000–19,999 | 1.17(0.94–1.45) | 1.54 (1.20–1.99) *** | 1.04(0.84–1.30) | 1.36(1.05–1.75) * | 1.06(0.85–1.32) | 1.24(0.96–1.60) |
| 20,000–29,999 | 0.88(0.70–1.13) | 1.16(0.89–1.53) | 0.84(0.66–1.07) | 1.02(0.78–1.35) | 0.83(0.65–1.07) | 0.96(0.73–1.28) |
| 30,000–39,999 | 0.90(0.69–1.18) | 1.09(0.80–1.49) | 0.69(0.52–0.91) ** | 0.72(0.53–1.00) | 0.67(0.50–0.90) ** | 0.68(0.49–0.95) * |
| 40,000–50,000 | 0.86(0.70–1.04) | 0.82(0.65–1.04) | 0.80(0.66–0.98) * | 0.71(0.56–0.90) ** | 0.73(0.60–0.90) *** | 0.70(0.55–0.90) *** |
| Do not know | 0.84(0.70–1.02) | 0.93(0.75–1.17) | 0.80(0.66–0.98) | 0.82(0.65–1.02) | 0.88(0.37–2.15) | 0.73(0.58–0.92) ** |
| Awareness of smoking in public regulation | ||||||
| Aware | Reference | Reference | Reference | Reference | Reference | Reference |
| Not aware | 1.68(1.49–1.90) *** | 1.46(1.25–1.71) *** | 1.76(1.56–1.99) *** | 1.47(1.26–1.73) *** | 1.80(1.59–2.04) *** | 1.48(1.26–1.73) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cham, B.; Mdege, N.D.; Bauld, L.; Britton, J.; D’Alessandro, U. Exposure to Second-Hand Smoke in Public Places and Barriers to the Implementation of Smoke-Free Regulations in The Gambia: A Population-Based Survey. Int. J. Environ. Res. Public Health 2021, 18, 6263. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126263
Cham B, Mdege ND, Bauld L, Britton J, D’Alessandro U. Exposure to Second-Hand Smoke in Public Places and Barriers to the Implementation of Smoke-Free Regulations in The Gambia: A Population-Based Survey. International Journal of Environmental Research and Public Health. 2021; 18(12):6263. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126263
Chicago/Turabian StyleCham, Bai, Noreen Dadirai Mdege, Linda Bauld, John Britton, and Umberto D’Alessandro. 2021. "Exposure to Second-Hand Smoke in Public Places and Barriers to the Implementation of Smoke-Free Regulations in The Gambia: A Population-Based Survey" International Journal of Environmental Research and Public Health 18, no. 12: 6263. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126263