
Estimating Need for Glasses and Hearing Aids in The Gambia: Results from a National Survey and Comparison of Clinical Impairment and Self-Report Assessment Approaches

 , , , , ,
, , , , ,  , , , and
, , , and
Abstract
:1. Introduction
- Estimate population-level total need, unmet need and coverage for glasses (distance and near glasses) and hearing aids, two of the five ATScale priority ADs.
- Estimate reported AD awareness, need and access barriers.
- Explore the relationship between clinical impairment and self-report assessment methods for assessing AD need within population surveys.
2. Methods
2.1. Self-Reported Functioning and AD Awareness, Need and Access Barriers
2.2. Vision Clinical Assessment
2.3. Hearing Clinical Assessment
2.4. Vision and Hearing Clinical Assessment Threshold Definitions
2.5. Data Analysis
- Met need: Needs and observed to be using an appropriate AD/total population examined.
- Undermet need: Needs and observed to be using an AD which did not correct vision/hearing to required threshold/total population examined.
- Unmet need: Needs but not observed to be using the AD/total population examined.
- Total need: (summation of met need + undermet need + unmet need)/total population examined.
- Coverage: (met need + undermet need)/total need.
- Effective coverage [18] (for glasses only): met need/total need.
2.6. Ethical Considerations
3. Results
3.1. Estimated Population AD Need and Coverage
3.1.1. Distance Glasses
3.1.2. Near Glasses
3.1.3. Hearing Aids
3.1.4. Total Need for Distance Glasses, Near Glasses and Hearing Aids by Sex, Age, Wealth Quintile and Location
3.2. Self-Reported AD Awareness, Need and Access Barriers
3.2.1. Vision ADs, Including Glasses
3.2.2. Hearing ADs, Including Hearing Aids
3.3. Relationship between AD Need Measurement Approaches
3.3.1. Self-Reported Unmet/Undermet Need for Glasses (Distance and/or Near) among People with Near Vision and/or Distance (Mild/Worse and Moderate/Worse VI) Uncorrected Refractive Error
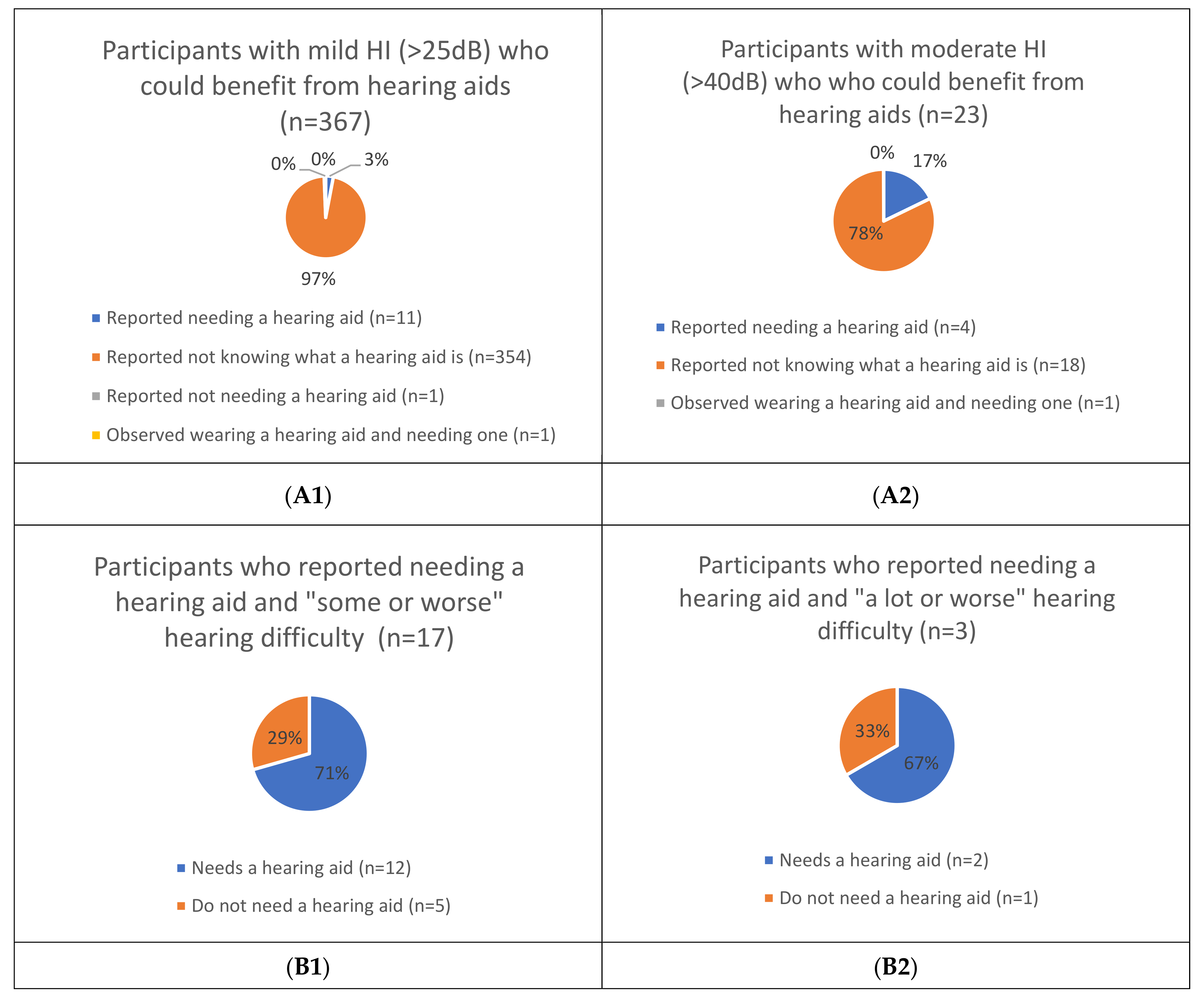
3.3.2. Self-Reported Unmet/Undermet Need for Hearing Aids among People with Mild/Worse HI (>25 dB) and Moderate/Worse HI (>40 dB)
4. Discussion
4.1. Estimated Population AD Need and Coverage
4.2. Self-Reported AD Awareness, Need and Access Barriers
4.3. Relationship between AD Need Measurement Approaches
4.4. Study Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Priority Assistive Products List; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Policy Brief: Access to Assistive Technology; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Assistive Technology: Making Universal Health Coverage Inclusive; WHO: Geneva, Switzerland, 2016; p. 3. [Google Scholar]
- ATscale. ATscale: Global Partnership for Assistive Technology. Available online: https://atscale2030.org/ (accessed on 27 January 2021).
- Pryor, W.; Nguyen, L.; Islam, Q.N.; Jalal, F.A.; Marella, M. Unmet needs and use of assistive products in two districts of bangladesh: Findings from a household survey. Int. J. Environ. Res. Public Health 2018, 15, 2901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boggs, D.; Kuper, H.; Mactaggart, I.; Murthy, G.; Oye, J.; Polack, S. Estimating assistive product need in Cameroon and India: Results of population-based surveys and comparison of self-report and clinical impairment assessment approaches. Trop. Med. Int. Health 2021, 26, 146–158. [Google Scholar] [CrossRef] [PubMed]
- Boggs, D.; Kuper, H.; Mactaggart, I.; Murthy, G.; Oye, J.; Polack, S. Estimating assistive technology need through population-based surveys: An analysis of data from Cameroon and India. In Global Perspectives on Assistive Technology, Proceedings of the GReAT Consultation, Geneva, Switzerland, 22–23 August 2019; Layton, N., Borg, J., Eds.; World Health Organization: Geneva, Switzerland, 2019; pp. 52–78. [Google Scholar]
- The Gambia Bureau of Statistics. The Gambia 2019 Statistical Abstract; GBoS: Serrekunda, Gambia, 2019. [Google Scholar]
- World Bank. The World Bank Data: Gambia. 2021. Available online: https://data.worldbank.org/country/gambia-the?view=chart (accessed on 5 February 2021).
- Nabaneh, S. Country report: The Gambia. Afr. Disabil. Rights Yearb. 2018, 6, 232–248. [Google Scholar]
- Hydara, A.; Bastawrous, A.; Bell, S.; Boggs, D.; Bright, T.; Bobat, H.; Eaton, J.; Faal, H.; Jobe, M.; Kim, M.J.; et al. The Gambia National Eye Health Survey 2019: Survey protocol. Wellcome Open Res. 2021, 6, 10. [Google Scholar] [CrossRef]
- Bright, T.; Mactaggart, I.; Kim, M.; Yip, J.; Kuper, H.; Polack, S. Rationale for a rapid methodology to assess the prevalence of hearing loss in population-based surveys. Int. J. Environ. Res. Public Health 2019, 16, 3405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakraborty, N.M.; Fry, K.; Behl, R.; Longfield, K. Simplified asset indices to measure wealth and equity in health programs: A reliability and validity analysis using survey data from 16 countries. Glob. Health Sci. Pr. 2016, 4, 141–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madans, J.H.; Loeb, M. Methods to improve international comparability of census and survey measures of disability. Disabil. Rehabil. 2013, 35, 1070–1073. [Google Scholar] [CrossRef] [PubMed]
- Washington Group on Disability Statistics Secretariat. Washington Group on Disability Statistics. 2020. Available online: http://www.washingtongroup-disability.com/ (accessed on 2 February 2021).
- Bastawrous, A.; Rono, H.; Livingstone, I.A.T.; Weiss, H.A.; Jordan, S.; Kuper, H.; Burton, M. Development and validation of a smartphone-based visual acuity test (peek acuity) for clinical practice and community-based fieldwork. JAMA Ophthalmol. 2015, 133, 930–937. [Google Scholar] [CrossRef] [PubMed]
- Swanepoel, D.W.; Myburgh, H.C.; Howe, D.M.; Mahomed, F.; Eikelboom, R.H. Smartphone hearing screening with integrated quality control and data management. Int. J. Audiol. 2014, 53, 841–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCormick, I.; Mactaggart, I.; Bastawrous, A.; Burton, M.J.; Ramke, J. Effective refractive error coverage: An eye health indicator to measure progress towards universal health coverage. Ophthalmic Physiol. Opt. 2020, 40, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OneSight. The Gambia—OneSight. 2021. Available online: https://onesight.org/the-gambia/ (accessed on 17 March 2021).
- Mulwafu, W.; Ensink, R.; Kuper, H.; Fagan, J. Survey of ENT services in sub-Saharan Africa: Little progress between 2009 and 2015. Glob. Health Action 2017, 10, 1289736. [Google Scholar] [CrossRef] [Green Version]
- Faal, H.; Minassian, D.; Sowa, S.; Foster, A. National survey of blindness and low vision in The Gambia: Results. Br. J. Ophthalmol. 1989, 73, 82–87. [Google Scholar] [CrossRef] [Green Version]
- Mashayo, E.R.; Chan, V.F.; Ramson, P.; Chinanayi, F.; Naidoo, K.S. Prevalence of refractive error, presbyopia and spectacle coverage in Kahama District, Tanzania: A rapid assessment of refractive error. Clin. Exp. Optom. 2015, 98, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Ntodie, M.; Abu, S.L.; Kyei, S.; Abokyi, S.; Abu, E.K. Near vision spectacle coverage and barriers to near vision correction among adults in the Cape Coast Metropolis of Ghana. Afr. Health Sci. 2017, 17, 549–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sapkota, Y.; Dulal, S.; Pokharel, G.P.; Pant, P.; Ellwein, L.B. Prevalence and correction of near vision impairment at Kaski, Nepal. Nepal. J. Ophthalmol. 2012, 4, 17–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bright, T.; Mulwafu, W.; Phiri, M.; Jiang, F.; Swanepoel, D.W.; Kuper, H.; Mactaggart, I.; Yip, J.L.Y.; Polack, S. Field test of the Rapid Assessment of Hearing Loss survey protocol in Ntcheu district, Malawi. Int. J. Audiol. 2020, 59, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Bright, T.; Shan, X.; Xu, J.; Liang, J.; Xiao, B.; Ensink, R.; Mactaggart, I.; Polack, S.; Yip, J.L.Y. Field-testing of a rapid survey method to assess the prevalence and causes of hearing loss in Gao’an, Jiangxi province, China. Arch. Public Health 2020, 78, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eide, A.H.; Neupane, S.; Hem, K. Living Conditions among People with Disability in Nepal; SINTEF Rapport A27656; SINTEF Technology and Society: Trondheim, Norway, 2016. [Google Scholar]
- Eide, A.H.; Bhekie, J. Living Conditions among People with Disabilities in Swaziland: A National Representative Study; SINTEF A20047; SINTEF Technology and Society: Trondheim, Norway, 2011; Available online: http://www.sintef.no/globalassets/upload/samfunn/finalreportlc_swasilandweb.pdf (accessed on 17 February 2021).
- Eide, A.H.; Kamaleri, Y. Living Conditions among People with Disabilities in Mozambique: A National Representative Study; SINTEF Report A9348; SINTEF Health Research: Trondheim, Norway, 2009. [Google Scholar]
- Eide, A.H.; Mmatli, T. Living conditions among people with disability in Botswana. Health Res. 2016, 2016. [Google Scholar]
- Eide, A.H.; Nanono, N.; Omona, J. Living Conditions among Persons with Disabilities in Uganda, a National, Representative Household Survey; SINTEF Report No. 2020–01387; SINTEF Digital: Trondheim, Norway, 2020. [Google Scholar]
- Eide, A.H.; Nhiwathiwa, S.; Muderedzi, J.; Loeb, E.M. Living Conditions among People with Activity Limitations in Zimbabwe. A Representative Regional Survey; SINTEF Rapport A24710; SINTEF Unimed: Trondheim, Norway, 2003. [Google Scholar]
- Eide, A.H.; van Rooy, G.; Loeb, M.E. Living Conditions among People with Activity Limitations in Namibia: A Representative, National Study; SINTEF Report STF78 A034503; SINTEF Unimed: Trondheim, Norway, 2003. [Google Scholar]
- Loeb, M.; Eide, A.H. Living Conditions among People with Activity Limitations in Malawi: A National Representative Study; SINTEF Report STF78 A044511; SINTEF Health research: Trondheim, Norway, 2004. [Google Scholar]
- Loeb, M.E.; Eide, A.H.; Mont, D. Approaching the measurement of disability prevalence: The case of Zambia. ALTER-Eur. J. Disabil. Res. Rev. Eur. Rech. Handicap. 2008, 2, 32–43. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. International Classification of Functioning, Disability and Health. 2001. Available online: www.who.int/classification/icf/en (accessed on 27 July 2020).



{kind=link}
{kind=link}
| Functional Domain | Total Number Participants | Prevalence ^ % (95% CI) | |
|---|---|---|---|
| Assessed (N) | With Impairment/Difficulty (N) | ||
| VISION | |||
| Vision clinically assessed | |||
| Distance vision | |||
| Mild or worse (VA < 6/12) | 9188 | 1327 | 13.4 (12.4–14.4) |
| Moderate or worse (VA < 6/18) | 9188 | 1001 | 10.0 (9.2–10.9) |
| Near vision* | 9183 | 4774 | 53.4 (51.7–55.2) |
| Self-reported vision difficulties ** | |||
| “Some or worse” difficulty | 9180 | 2530 | 26.9 (25.2–28.7) |
| “A lot of or worse” difficulty | 9180 | 179 | 2.0 (1.7–2.4) |
| HEARING | |||
| Hearing clinically assessed | |||
| Mild or worse (>25 dB) | 1393 | 402 | 28.1 (24.6–31.9) |
| Moderate or worse (>40 dB) | 1393 | 24 | 1.6 (1.0–2.6) |
| Self-reported hearing difficulties *** | |||
| “Some or worse” difficulty | 9185 | 385 | 1.7 (0.9–3.2) |
| “A lot of or worse” difficulty | 9185 | 55 | 0.2 (0.04–0.5) |
| Assistive Devices | Total Need ^,* | Unmet Need ^,** | Coverage ^,*** | Effective Coverage ^,**** | ||
|---|---|---|---|---|---|---|
| N | % (95% CI) | N | % (95% CI) | % (95% CI) | % (95% CI) | |
| Distance glasses (mild/worse VI) | 546 | 5.6 (5.0–6.3) | 529 | 5.4 (4.8–6.0) | 3.8% (2.3–6.3) | 3.3% (1.9–5.8) |
| Distance glasses (moderate/worse VI) | 435 | 4.3 (3.8–4.9) | 421 | 4.2 (3.6–4.7) | 3.5% (2.0–6.0) | 2.7% (1.4–5.0) |
| Near glasses & | 4013 | 45.9 (44.2–47.5) | 3942 | 44.9 (43.2–46.5) | 2.2% (1.6–3.0) | 0.2% (0.09–0.4) |
| Hearing aids (mild/worse HI) | 367 | 25.5 (22.2–29.2) | 366 | 25.5 (22.1–29.2) | 0.1% (0.02–1.0) | - |
| Hearing aids (moderate/worse HI) | 23 | 1.5 (0.9–2.4) | 22 | 1.5 (0.9–2.4) | 2.3% (0.3–15.9) | - |
| Distance Glasses | Near Glasses ^ | Hearing Aids | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| <6/12 (Mild/Worse VI) ^ | <6/18 (Mod/Worse VI) ^ | >25 dB (Mild/Worse HI)^ | >40 dB (Mod/Worse HI) ^ | |||||||
| N | % (95% CI) | N | % (95% CI) | N | % (95% CI) | N | % (95% CI) | N | % (95% CI) | |
| Sex | ||||||||||
| Male | 178 | 5.0 (4.2–5.8) | 128 | 3.4 (2.7–4.2) | 1440 | 48.3 (47.5–50.9) | 113 | 20.6 (16.5–25.3) | 8 | 1.3 (0.5–3.1) |
| Female | 368 | 6.3 (5.6–7.1) | 307 | 5.2 (4.5–5.9) | 2573 | 43.4 (41.8–44.9) | 254 | 30.7 (26.6–35.0) | 15 | 1.7 (1.0–3.1) |
| p-value | 0.01 | <0.001 | <0.001 | <0.001 | 0.61 | |||||
| Age groups | ||||||||||
| 35 to <50 years | 101 | 2.1 (1.6–2.8) | 73 | 1.4 (1.0–2.0) | 1283 | 29.5 (27.5–31.6) | 119 | 12.6 (9.8–16.1) | 9 | 0.8 (0.4–1.9) |
| 50 to <60 | 114 | 6.3 (5.2–7.7) | 90 | 4.8 (3.8–6.1) | 1240 | 76.3 (73.4–78.9) | 82 | 29.1 (23.5–35.3) | 1 | 0.3 (0.04–2.4) |
| 60+ years | 331 | 14.0 (12.5–15.6) | 272 | 11.2 (9.8–12.8) | 1490 | 62.2 (59.7–64.6) | 166 | 56.9 (49.5–63.9) | 13 | 4.3 (2.3–8.1) |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | 0.006 | |||||
| Socioeconomic status * | ||||||||||
| 1st quintile | 49 | 5.4 (3.9–7.4) | 32 | 3.4 (2.2–5.2) | 353 | 44.1 (39.0–49.2) | 28 | 22.7 (13.3–36.0) | 0 | - |
| 2nd quintile | 72 | 5.5 (3.9–7.6) | 59 | 4.4 (3.0–6.5) | 535 | 43.9 (40.2–47.7) | 63 | 30.8 (23.6–39.0) | 4 | 1.4 (0.5–3.5) |
| 3rd quintile | 122 | 5.0 (4.0–6.1) | 102 | 4.1 (3.2–5.1) | 973 | 45.0 (41.7–48.5) | 78 | 26.2 (21.0–32.1) | 7 | 2.4 (0.9–6.4) |
| 4th quintile | 128 | 5.9 (4.8–7.1) | 113 | 4.9 (3.9–6.1) | 927 | 46.6 (43.4–49.7) | 93 | 23.6 (18.3–29.8) | 5 | 0.9 (0.4–2.1) |
| 5th quintile | 175 | 6.2 (5.1–7.4) | 129 | 4.3 (3.5–5.2) | 1225 | 47.7 (45.4–49.9) | 105 | 25.3 (19.7–31.7) | 7 | 2.1 (1.0–4.3) |
| p-value | 0.31 | 0.46 | 0.08 | 0.67 | 0.31 | |||||
| Location | ||||||||||
| Urban | 309 | 5.8 (5.0–6.7) | 250 | 4.5 (3.8–5.2) | 2259 | 47.3 (45.4–49.2) | 222 | 24.1 (20.1–28.6) | 14 | 1.6 (1.0–2.8) |
| Rural | 237 | 5.4 (4.5–6.4) | 185 | 4.1 (3.2–5.1) | 1754 | 44.1 (41.3–47.0) | 145 | 27.9 (22.3–34.3) | 9 | 1.3 (0.5–3.4) |
| p-value | 0.54 | 0.49 | 0.07 | 0.30 | 0.66 | |||||
| Assistive Devices by Domain | VISION | HEARING | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Spectacles | Talking or Touching Watch | Magnifier or Telescope | White Cane | Braille Equip-ment | Other | None | Alarm Signallers ^ | Hearing Aids and Batteries | Personal Frequency Modulation System | Other | None | |
| Awareness of AD * | 1816 (72.8%) | 37 (1.5%) | 84 (3.3%) | 209 (8.3%) | 62 (2.5%) | 709 (28.0%) | 8 (2.1%) | 48 (12.5%) | 2 (<1%) | 331 (86.0%) | ||
| Unmet/undermet need * | 1681 (66.4%) | 12 (<1%) | 7 (<1%) | 17 (<1%) | 1 (<1%) | 8 (<1%) | 447 (17.7%) | 34 (8.8%) | 223 (58.0%) | 10 (2.6%) | 3 (<1%) | 140 (36.4%) |
| Barriers to not having AD ^ | ||||||||||||
| Unaware of AD | 544 (32%) | 5 (42%) | 2 (29%) | 8 (47%) | - | 4 (50%) | 27 (79%) | 138 (62%) | 7 (70%) | 33% | ||
| AP not locally available | 741 (44%) | 4 (33%) | 3 (43%) | 8 (47%) | 1 (100%) | 5 (63%) | 6 (18%) | 170 (76%) | 9 (90%) | 33% | ||
| Cannot afford | 581 (35%) | 5 (42%) | 2 (29%) | 12 (71%) | 1 (100%) | 4 (50%) | 5 (15%) | 122 (55%) | 6 (60%) | 33% | ||
| Not suitable for home/environment | 102 (6%) | - | 1 (14%) | 1 (6%) | - | 2 (25%) | 2 (6%) | 21 (9%) | 1 (10%) | - | ||
| No one available to instruct how to use | 567 (34%) | 5 (42%) | 3 (43%) | 6 (35%) | 1 (100%) | 2 (25%) | 5 (15%) | 131 (59%) | 6 (60%) | 33% | ||
| Transport not available | 716 (43%) | 5 (42%) | 3 (43%) | 8 (47%) | 1 (100%) | 4 (50%) | 4 (12%) | 166 (74%) | 8 (80%) | 66% | ||
| Do not like appearance | 15 (1%) | - | - | - | - | 1 (13%) | 1 (3%) | 4 (2%) | - | - | ||
| People treat users differently | 154 (9%) | 3 (25%) | 1 (14%) | 6 (35%) | - | 2 (25%) | 4 (12%) | 40 (18%) | 4 (40%) | 66% | ||
| Other | 47 (3%) | 3 (25%) | 1 (14%) | 5 (24%) | - | 2 (25%) | 2 (6%) | 9 (4%) | 3 (30%) | 66% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boggs, D.; Hydara, A.; Faal, Y.; Okoh, J.A.; Olaniyan, S.I.; Sanneh, H.; Ngett, A.; Bah, I.; Aleser, M.; Denis, E.; et al. Estimating Need for Glasses and Hearing Aids in The Gambia: Results from a National Survey and Comparison of Clinical Impairment and Self-Report Assessment Approaches. Int. J. Environ. Res. Public Health 2021, 18, 6302. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126302
Boggs D, Hydara A, Faal Y, Okoh JA, Olaniyan SI, Sanneh H, Ngett A, Bah I, Aleser M, Denis E, et al. Estimating Need for Glasses and Hearing Aids in The Gambia: Results from a National Survey and Comparison of Clinical Impairment and Self-Report Assessment Approaches. International Journal of Environmental Research and Public Health. 2021; 18(12):6302. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126302
Chicago/Turabian StyleBoggs, Dorothy, Abba Hydara, Yaka Faal, John Atta Okoh, Segun Isaac Olaniyan, Haruna Sanneh, Abdoulie Ngett, Isatou Bah, Mildred Aleser, Erima Denis, and et al. 2021. "Estimating Need for Glasses and Hearing Aids in The Gambia: Results from a National Survey and Comparison of Clinical Impairment and Self-Report Assessment Approaches" International Journal of Environmental Research and Public Health 18, no. 12: 6302. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126302