
Typology of Family Support in Home Care for Iranian Older People: A Qualitative Study



{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Data Collection
2.3. Data Analysis
2.4. Ethical Considerations
2.5. Trustworthiness
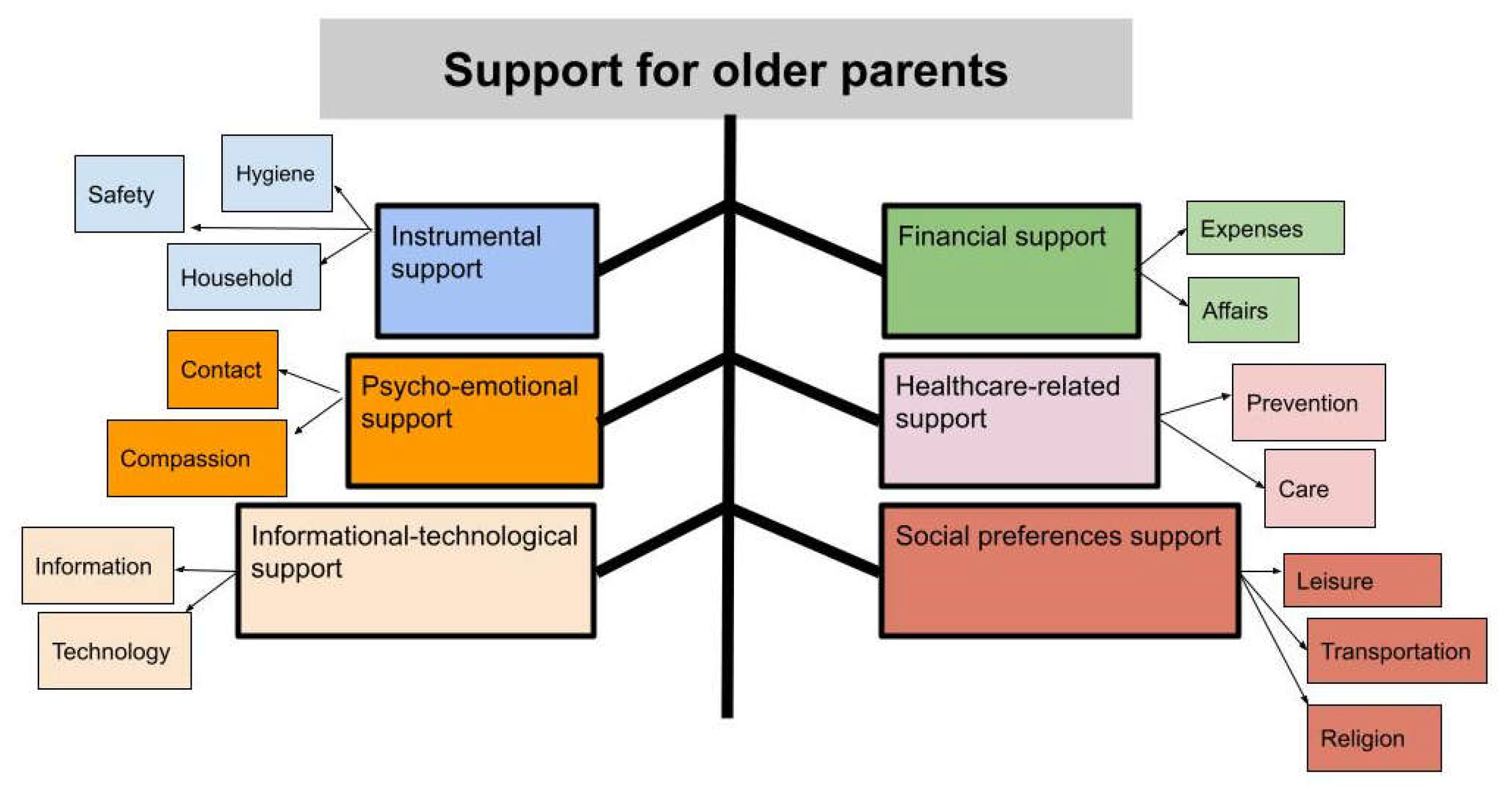
3. Results
3.1. Instrumental Support
3.1.1. Support for Personal Hygiene and Home Cleaning
I don’t have the physical ability that I had in my youth to clean my home. Therefore, my daughters and grandchildren alternately come and clean my home every other week or every month. Moreover, they bought a small vacuum cleaner by which I can clean around myself.(Participant 23; a 68-year-old woman)
3.1.2. Support for Maintaining and Fixing Household Appliances
My children should come here before the onset of the cold and the warm seasons to assess and prepare warmers or cooler. My older son performs simple fixings. For example, if there is a stuck-out nail in the furniture, which tears clothes, my son brings a hammer and fixes it. Or, if he sees that the water faucet is dripping, he fixes it.(Participant 7; a 72-year-old woman)
3.1.3. Support for Structural Safety
Nowadays, homes have not been designed to be appropriate for older people. I had to take extreme care in order not to slip on floor ceramic tiles, because fractures in older people do not heal. I have slipped several times so far. Thanks God! I just experienced a wrist sprain and now, my wrist aches when it gets cold. Previously, homes were not like this and floor was covered with mosaic tiles. My children have bought me slippers in order not to slip and have installed grab bars in the rest room and the bathroom. They have also covered the kitchen floor with moquette.(Participant 8; a 79-year-old man)
3.1.4. Support for Cooking
I can make simple foods. Of course, my younger daughter prepares and packs necessary food stuffs for me. For example, she cuts and packs meat for each meal and brings me fried onion so that I don’t need to stand on the feet for long time for cooking. My daughter-in-law also makes appropriate foods for me as she knows that I have no teeth.(Participant 4; a 80-year-old woman)
3.1.5. Support for Cloth Washing
My hands are not strong enough anymore to wash clothes and, hence, I use washing machine. I put dirty clothes in a basket and my daughters come here at the weekend, wash them with the machine, and hang them from the clothesline.(Participant 19; a 67-year-old woman)
3.2. Financial Support
3.2.1. Support for Household Expenses
My income is inadequate. Although we [have a private house] don’t pay rent, we can’t afford all expenses. I have a single boy whose expenses are with me. My wife also has knee pain and receives physiotherapy, while insurance companies don’t cover all treatment-related costs. I’m also sick and have healthcare-related costs. However, my daughter financially helps me though she is married and doesn’t live with us.(Participant 1; a 69-year-old man)
3.2.2. Support for Doing Financial Affairs
I have memory impairment. My children perform the affairs related to my installments so that I can decide for my other expenses.(Participant 15; a 68-year-old woman)
3.3. Psycho-Emotional Support
3.3.1. Frequent Greeting Contacts
I’ve become old. What do we need except for happiness? I like my sons and daughters-in-law to pay more attention to me and visit me every two to three days and contact me every day. My children’s support and attention are very valuable and make me happy.(Participant 20; a 68-year-old woman)
3.3.2. Showing Compassion
When I had a work or some home appliance had been out of work, they knew what to do and how to help. For example, when I had a party, they came and performed shopping. When I wanted to move something at home, they willingly did it for me.(Participant 9; a 72-year-old man)
3.4. Healthcare-Related Support
3.4.1. Preventive Measures
My children frequently recommend me what to eat and not to eat. For example, they don’t put saltshaker at the table, remind me that salt and fat are not good to my hypertension, and warn me against excessive use of salt and sugar. They also recommend me to take fruits. They are very sensitive to my eating.(Participant 7; a 71-year-old man)
3.4.2. Care Measures
I don’t know how to take my medications. My daughter has bought me a pill organizer and puts my morning, noon, and evening medications in it. Then, I can easily take them.(Participant 23; an 85-year-old woman)
I like to use self-treatment for my health problems such as common cold. However, my children disagree with me mostly and take me to the doctor or oblige me to go to the doctor.(Participant 15; a 68-year-old woman)
3.5. Informational-Technological Support
3.5.1. Informational Support
My daughter and son-in-law have frequently emphasized that I should see the face of those who ring my home bell through the video door-phone. My son-in-law tells me about cheatings and asks me not to disclose personal information over telephone.(Participant 25; a 76-year-old woman)
3.5.2. Technological Support
My children have bought me a new mobile phone; but I’m illiterate and can’t use it. My children have put their photos in the contact list of the phone, and I can easily contact them by taping their photos.(Participant 18; a 69-year-old woman)
My daughter washes my clothes using washing machine because I can’t use it. She has trained me how to use the machine for several times, but I cannot learn it. Of course, I could use my previous washing machine, but can’t use this new one.(Participant 22; a 80-year-old man)
3.6. Social Preference Support
3.6.1. Support for Leisure Activities
My children bought me two puzzles to entertain me. I do them many times. It is good for my memory. I also like painting. One of my grandchildren brought me several drawing notebooks and color pencils and told me, ‘Grandmother! Do drawing to pass your time.’ They also have put a chair in a safe place in the balcony for me to seat and watch people and children in the park.(Participant 4; a 80-year-old woman)
3.6.2. Support for Transportation
My children take me on trips since they have private car and I’m comfortable with them. They take me wherever I want to go such as to doctor, hospital, and parties. I even perform heavy shopping with their help.(Participant 7, a 71-year-old man)
3.6.3. Support for Religious Affairs
Each year, I hold a religious ritual at home and invite friends and relatives. Now, I can’t do such things due to pain in my limbs. However, my children always help me hold the ritual at my home and do all things from the beginning to the end.(Participant 14; a 67-year-old woman)
My children are attentive to anniversaries. For example, they come here in the Yalda night, Mother’s Day, and Father’s Day. I’m very happy when they are here.(Participant 17; a 66-year-old woman)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 4 May 2021).
- Mehri, N.; Messkoub, M.; Kunkel, S. Trends, Determinants and the Implications of Population Aging in Iran: Working Paper No. 646. Available online: https://ideas.repec.org/p/ems/euriss/118519.html (accessed on 4 May 2021).
- Dziechciaż, M.; Filip, R. Biological psychological and social determinants of old age: Bio-psycho-social aspects of human aging. Ann. Agric. Environ. Med. 2014, 21, 835–838. [Google Scholar] [CrossRef]
- Rattan, S.I.S. Aging is not a disease: Implications for intervention. Aging Dis. 2014, 5, 196–202. [Google Scholar] [CrossRef]
- Sigalingging, G.; Sitopu, S.D. Measuring Family Support in the Elderl™ s Independence in Performing Activities of Daily Living (A Case Study in Medan Tuntungan District, Medan City, Indonesia). IOSR J. Nurs. Health Sci. 2017, 6, 1–5. [Google Scholar] [CrossRef]
- Doblhammer, G.; Scholz, R. Ageing, Care Need and Quality of Life: The Perspective of Care Givers and People in Need of Care, 1th ed.; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Gardiner, C.; Geldenhuys, G.; Gott, M. Interventions to reduce social isolation and loneliness among older people: An integrative review. Health Soc. Care Community 2018, 26, 147–157. [Google Scholar] [CrossRef]
- Mohagheghi Kamal, S.H.; Sajadi, H.; Zare, H.; Biglarian, A. Need Assessment Among the Elders of Social Security Organization & National Retirement Fund. Salmand Iran. J. Ageing 2008, 3, 8–15. [Google Scholar]
- Carpenter, B.D.; Mulligan, E.A. Chapter 11—Assessment with Late-Life Families: Issues and Instruments. In Handbook of Assessment in Clinical Gerontology, 2nd ed.; Lichtenberg, P.A., Ed.; Academic Press: San Diego, CA, USA, 2010; pp. 273–304. [Google Scholar] [CrossRef]
- Ingersoll-Dayton, B.; Saengtienchai, C.; Kespichayawattana, J.; Aungsuroch, Y. Measuring psychological well-being: Insights from Thai elders. Gerontologist 2004, 44, 596–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thanakwang, K. Family support, anticipated support, negative interaction, and psychological well-being of older parents in Thailand. Psychogeriatrics 2015, 15, 171–178. [Google Scholar] [CrossRef]
- Nazari, S.; Farhadi, A.; Sadeghmoghadam, L.; Namazi shabestari, A. Perceived affective support From the Iranian older adult´s viewpoint: A directed content analysis. J. Gerontol. 2017, 2, 51–64. [Google Scholar] [CrossRef] [Green Version]
- Tajvar, M.; Arab, M.; Montazeri, A. Determinants of health-related quality of life in elderly in Tehran, Iran. BMC Public Health 2008, 8, 323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidari, M.; Ghodusi Borujeni, M.; Naseh, L. Comparison of Self-Efficacy and Loneliness Between Community-Dwelling & Institutionalized Older People. Salmand Iran. J. Ageing 2016, 11, 142–151. [Google Scholar] [CrossRef] [Green Version]
- Davey, A.; Femia, E.E.; Zarit, S.H.; Shea, D.G.; Sundström, G.; Berg, S.; Smyer, M.A.; Savla, J. Life on the edge: Patterns of formal and informal help to older adults in the United States and Sweden. J. Gerontol. B Psychol. Sci. Soc. Sci. 2005, 60, S281–S288. [Google Scholar] [CrossRef] [Green Version]
- Davey, A.; Patsios, D. Formal and Informal Community Care to Older Adults: Comparative Analysis of the United States and Great Britain. J. Fam. Econ. Issues 1999, 20, 271–299. [Google Scholar] [CrossRef]
- Kingston, A.; Comas-Herrera, A.; Jagger, C. Forecasting the care needs of the older population in England over the next 20 years: Estimates from the Population Ageing and Care Simulation (PACSim) modelling study. Lancet Public Health 2018, 3, e447–e455. [Google Scholar] [CrossRef] [Green Version]
- Asadzadeh, m.; Maher, A.; Jafari, M.; AliMohammadzadeh, K.; Hosseini, M. The provision of care services for older adults—A narrative review (2015 to 2020). J. Gerontol. 2020, 5, 1–13. [Google Scholar]
- Walker, A.; Mollenkopf, H. International and Multi-Disciplinary Perspectives on Quality of Life in Old Age: Conceptual Issues. Quality of Life in Old Age; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Poulin, J.; Deng, R.; Ingersoll, T.S.; Witt, H.; Swain, M. Perceived family and friend support and the psychological well-being of American and Chinese elderly persons. J. Cross Cult. Gerontol 2012, 27, 305–317. [Google Scholar] [CrossRef] [PubMed]
- Gariépy, G.; Honkaniemi, H.; Quesnel-Vallée, A. Social support and protection from depression: Systematic review of current findings in Western countries. Br. J. Psychiatry 2016, 209, 284–293. [Google Scholar] [CrossRef]
- Lewis, J.S. Housing and social support needs of elderly persons: A needs assessment in an independent living facility. Eval. Program. Plan. 1997, 20, 269–277. [Google Scholar] [CrossRef]
- Iecovich, E.; Lankri, M. Attitudes of elderly persons towards receiving financial support from adult children. J. Aging Stud. 2002, 16, 121–133. [Google Scholar] [CrossRef]
- Rittirong, J.; Prasartkul, P.; Rindfuss, R.R. From whom do older persons prefer support? The case of rural Thailand. J. Aging Stud. 2014, 31, 171–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdollahpour, I.; Noroozian, M.; Nedjat, S.; Majdzadeh, R. Caregiver Burden and its Determinants among the Family Members of Patients with Dementia in Iran. Int. J. Prev. Med. 2012, 3, 544–551. [Google Scholar]
- Rejeh, N.; Heravi-Karimooi, M.; Vaismoradi, M. Iranian nursing students' perspectives regarding caring for elderly patients. Nurs. Health Sci. 2011, 13, 118–125. [Google Scholar] [CrossRef]
- Alipoor, F.; Sajadi, H.; Forozan, A.; Biglarian, A. The role of social support in elderly quality of life. Soc. Welf. 2009, 8, 149–167. [Google Scholar]
- Garousi, S.; Safizadeh, H.; Samadian, F. The Study of Relationship between Social Support and Quality of Life among Elderly People in Kerman. Jundishapur Sci. Med. J. 2012, 11, 303–315. [Google Scholar]
- Motamedi, S.A.; Ezhehei, J.; Azad, F.P.; Kiamanesh, A. The role of social support on life satisfaction, general well-being, and sense of loneliness among the elderly. J. Psychol. 2002, 6, 115–133. [Google Scholar]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Assarroudi, A.; Heshmati Nabavi, F.; Armat, M.R.; Ebadi, A.; Vaismoradi, M. Directed qualitative content analysis: The description and elaboration of its underpinning methods and data analysis process. J. Res. Nurs. 2018, 23, 42–55. [Google Scholar] [CrossRef] [Green Version]
- Komjakraphan, P.; Isalamalai, S.-A.; Boonyasopun, U.; Schneider, J. Development of the Thai Family Support Scale for Elderly Parents (TFSS-EP). Pac. Rim Int. J. Nurs. Res. 2009, 13, 118–132. [Google Scholar]
- National Academies of Sciences, E. ; Medicine. Families Caring for an Aging America; The National Academies Press: Washington, DC, USA, 2016; p. 366. [Google Scholar] [CrossRef]
- Uddi, M.; Bhuiyan, A. Development of the family support scale (FSS) for elderly people. Moj Gerontol. Geriatr. 2019, 4, 17–20. [Google Scholar] [CrossRef]
- Vaismoradi, M.; Jones, J.; Turunen, H.; Snelgrove, S. Theme development in qualitative content analysis and thematic analysis. J. Nurs. Educ. Pract. 2016, 6, 100–110. [Google Scholar] [CrossRef] [Green Version]
- Johnson, S.; Rasulova, S. Qualitative research and the evaluation of development impact: Incorporating authenticity into the assessment of rigour. J. Dev. Eff. 2017, 9, 263–276. [Google Scholar] [CrossRef]
- Stončikaitė, I. Care, dementia, and the fourth age in Erica Jong’s later work. Gerontologist 2021. [Google Scholar] [CrossRef]
- Djundeva, M.; Mills, M.; Wittek, R.; Steverink, N. Receiving Instrumental Support in Late Parent–Child Relationships and Parental Depression. J. Gerontol. Ser. B 2014, 70, 981–994. [Google Scholar] [CrossRef] [Green Version]
- Sato, S.; Demura, S.; Tanaka, K.; Kasuga, K.; Kobayashi, H. ADL ability characteristics of partially dependent older people: Gender and age differences in ADL ability. Environ. Health Prev. Med. 2001, 6, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Lapena, C.; Continente, X.; Sánchez Mascuñano, A.; Pons Vigués, M.; Pujol Ribera, E.; López, M.J. Qualitative evaluation of a community-based intervention to reduce social isolation among older people in disadvantaged urban areas of Barcelona. Health Soc. Care Community 2020, 28, 1488–1503. [Google Scholar] [CrossRef]
- Rath, T.; Panigrahi, D. Instrumental social support for the rural elderly: Study of a rural block of a costal district of Odisha. Int. J. Community Med. Public Health 2017, 4. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Ji, Y.; Chen, T. The roles of different sources of social support on emotional well-being among Chinese elderly. PLoS ONE 2014, 9, e90051. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.H.C.; Lin, J.-H.; Chen, H.-G. Explore the needs of the elderly with social awareness. Educ. Gerontol. 2019, 45, 310–323. [Google Scholar] [CrossRef]
- Bagheri Ruchi, A.; Mohammadi, F.; Mafi, M.; Motalebi, S.A. Prevalence and External Factors of Home Falls Among the Elderly in Qazvin. J. Inflamm. Dis. 2019, 23, 440–451. [Google Scholar] [CrossRef]
- Shariat, F.; Moradi, F.; Ghahramani, R. Study of Social, Cultural, Economic, Well-Being, and Urban Structure Needs of Tehran Seniors Association Members. Salmand Iran. J. Ageing 2015, 10, 8–25. [Google Scholar]
- Lette, M.; Stoop, A.; Gadsby, E.; Ambugo, E.A.; Mateu, N.C.; Reynolds, J.; Nijpels, G.; Baan, C.; de Bruin, S.R. Supporting Older People to Live Safely at Home—Findings from Thirteen Case Studies on Integrated Care Across Europe. Int. J. Integr. Care 2020, 20, 1. [Google Scholar] [CrossRef]
- Lai, N.; Tung, A. Who supports the elderly? The changing economic lifecycle reallocation in Taiwan, 1985 and 2005. J. Econ. Ageing 2015, 5, 63–68. [Google Scholar] [CrossRef]
- Lee, S.Y.; Chou, K.L. Assessing the relative contribution of social exclusion, income-poverty, and financial strain on depressive symptoms among older people in Hong Kong. Aging Ment. Health 2019, 23, 1487–1495. [Google Scholar] [CrossRef]
- Tabari, F.; Khaghanizade, M.; Dehghan-Nayeri, N.; Najafi-Mehri, S. Explain the concept of autonomy in the maintain dignity elderly: A qualitative study. Iran. J. Nurs. Res. 2016, 11, 17–27. [Google Scholar]
- Mason, A.; Lee, R. Population aging and the generational economy: Key findings. In Population Aging and the Generational Economy; Edward Elgar Publishing: Cheltenham, UK, 2011. [Google Scholar]
- Akinrolie, O.; Okoh, A.C.; Kalu, M.E. Intergenerational Support between Older Adults and Adult Children in Nigeria: The Role of Reciprocity. J. Gerontol Soc. Work 2020, 63, 478–498. [Google Scholar] [CrossRef] [PubMed]
- Rahayu, S.; Catharina Daulima, N.H.; Eka Putri, Y.S. The experience of older people living in an elderly residential home (Panti Sosial Tresna Werdha): A phenomenology. Enferm. Clin. 2018, 28 (Suppl. 1), 79–82. [Google Scholar] [CrossRef]
- Wang, L.; Yang, L.; Di, X.; Dai, X. Family Support, Multidimensional Health, and Living Satisfaction among the Elderly: A Case from Shaanxi Province, China. Int. J. Environ. Res. Public Health 2020, 17, 8434. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi, S.; Keshavarz Mohammadi, N.; Mohammadi Shahboulaghi, F.; Ramezankhani, A.; Mehrabi, Y. Physical Health Status and Frailty Index in Community Dwelling Older Adults in Tehran. Salmand Iran. J. Ageing 2019, 13, 652–665. [Google Scholar] [CrossRef] [Green Version]
- Rashedi, S.; Bahrami, M. Factors related to the health promoting life style among among geriartric patient. Nurs. Midwifery J. 2015, 13, 90–98. [Google Scholar]
- Golinowska, S.; Groot, W.; Baji, P.; Pavlova, M. Health promotion targeting older people. BMC Health Serv. Res. 2016, 16, 345. [Google Scholar] [CrossRef] [Green Version]
- Abedi, H.A.; Alavi, M. The experiences of health care team and elderly in-patients about concept of “elderly patients' education'' in a hospital affiliated to isfahan university of medical sciences. Iran. J. Med. Educ. 2007, 7, 93–100. [Google Scholar]
- Dolu, İ.; Naharcı, M.; Logan, P.A.; Paal, P.; Vaismoradi, M. A Qualitative Study of Older Patients’ and Family Caregivers' Perspectives of Transitional Care From Hospital to Home. Res. Theory Nurs. Pract. 2021. [Google Scholar] [CrossRef]
- Habibi, A.; Nikpour, S.; Seyedoshohadaei, M.; Haghani, H. Health Promoting Behaviors and its Related Factors in Elderly. Iran. J. Nurs. 2006, 19, 35–48. [Google Scholar]
- Sigurdardottir, S.H.; Sundstrom, G.; Malmberg, B.; Bravell, M.E. Needs and care of older people living at home in Iceland. Scand. J. Public Health 2012, 40, 1–9. [Google Scholar] [CrossRef]
- Cobb, S. Social support as a moderator of life stress. Psychosom. Med. 1976, 38, 300–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasco, A.C.; Morse, J.M.; Olson, J.K. The cross-cultural relationships between nurses and Filipino Canadian patients. J. Nurs. Sch. 2004, 36, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, F.; Dabbaghi, F.; Nikravesh, M. Facilitator and Barriers Factors in Family Caregiving Process of Iranian Frail Elderly: Qualitative study. Iran. J. Nurs. 2008, 21, 55–65. [Google Scholar]
- Hashizume, Y. Salient factors that influence the meaning of family caregiving for frail elderly parents in Japan from a historical perspective. Sch. Inq. Nurs. Pract. 1998, 12, 123–134, discussion 135–141. [Google Scholar]
- Hashizume, Y. Gender issues and Japanese family-centered caregiving for frail elderly parents or parents-in-law in modern Japan: From the sociocultural and historical perspectives. Public Health Nurs 2000, 17, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Sharma, N.; Chakrabarti, S.; Grover, S. Gender differences in caregiving among family—Caregivers of people with mental illnesses. World J. Psychiatry 2016, 6, 7–17. [Google Scholar] [CrossRef]
- Ringer, T.; Hazzan, A.A.; Agarwal, A.; Mutsaers, A.; Papaioannou, A. Relationship between family caregiver burden and physical frailty in older adults without dementia: A systematic review. Syst. Rev. 2017, 6, 55. [Google Scholar] [CrossRef] [Green Version]
- Chiao, C.Y.; Wu, H.S.; Hsiao, C.Y. Caregiver burden for informal caregivers of patients with dementia: A systematic review. Int. Nurs. Rev. 2015, 62, 340–350. [Google Scholar] [CrossRef]
- Beach, S.R.; Schulz, R. Family Caregiver Factors Associated with Unmet Needs for Care of Older Adults. J. Am. Geriatr. Soc. 2017, 65, 560–566. [Google Scholar] [CrossRef]
- Orfila, F.; Coma-Solé, M.; Cabanas, M.; Cegri-Lombardo, F.; Moleras-Serra, A.; Pujol-Ribera, E. Family caregiver mistreatment of the elderly: Prevalence of risk and associated factors. BMC Public Health 2018, 18, 167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camak, D.J. Addressing the burden of stroke caregivers: A literature review. J. Clin. Nurs. 2015, 24, 2376–2382. [Google Scholar] [CrossRef]
- Stensletten, K.; Bruvik, F.; Espehaug, B.; Drageset, J. Burden of care, social support, and sense of coherence in elderly caregivers living with individuals with symptoms of dementia. Dementia 2016, 15, 1422–1435. [Google Scholar] [CrossRef] [PubMed]
- Wagner, N.; Hassanein, K.; Head, M. Computer use by older adults: A multi-disciplinary review. Comput. Hum. Behav. 2010, 26, 870–882. [Google Scholar] [CrossRef]
- Elers, P.; Hunter, I.; Whiddett, D.; Lockhart, C.; Guesgen, H.; Singh, A. User Requirements for Technology to Assist Aging in Place: Qualitative Study of Older People and Their Informal Support Networks. JMIR Mhealth Uhealth 2018, 6, e10741. [Google Scholar] [CrossRef] [Green Version]
- Gitlow, L. Technology Use by Older Adults and Barriers to Using Technology. Phys. Occup. Ther. Geriatr. 2014, 32, 271–280. [Google Scholar] [CrossRef]
- Vaportzis, E.; Clausen, M.G.; Gow, A.J. Older Adults Perceptions of Technology and Barriers to Interacting with Tablet Computers: A Focus Group Study. Front. Psychol 2017, 8, 1687. [Google Scholar] [CrossRef] [Green Version]
- Basakha, M.; Mohaqeqi Kamal, S.H.; Pashazadeh, H. Acceptance of Information and Communication Technology by the Elderly People Living in Tehran. Salmand Iran. J. Ageing 2019, 13, 550–563. [Google Scholar] [CrossRef] [Green Version]
- Alvseike, H.; Brønnick, K. Feasibility of the iPad as a hub for smart house technology in the elderly; effects of cognition, self-efficacy, and technology experience. J. Multidiscip Healthc. 2012, 5, 299–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, B.; Kim, J.; Baumgartner, L.M. Informal Learning of Older Adults in Using Mobile Devices: A Review of the Literature. Adult Educ. Q. 2019, 69, 120–141. [Google Scholar] [CrossRef]
- Luijkx, K.; Peek, S.; Wouters, E. “Grandma, You Should Do It--It’s Cool” Older Adults and the Role of Family Members in Their Acceptance of Technology. Int. J. Environ. Res. Public Health 2015, 12, 15470–15485. [Google Scholar] [CrossRef] [Green Version]
- Hosseinizare, S.M.; Tajvar, M.; Abdi, K.; Esfahani, P.; Geravand, B.; Pourreza, A. Leisure Spending Patterns and their Relationship with Mental Health in the Elderly in Iran. Salmand Iran. J. Ageing 2020, 15, 366–379. [Google Scholar] [CrossRef]
- Szanton, S.L.; Walker, R.K.; Roberts, L.; Thorpe, R.J., Jr.; Wolff, J.; Agree, E.; Roth, D.L.; Gitlin, L.N.; Seplaki, C. Older adults' favorite activities are resoundingly active: Findings from the NHATS study. Geriatr. Nurs. 2015, 36, 131–135. [Google Scholar] [CrossRef] [Green Version]
- Dehi Aroogh, M.; Mohammadi Shahboulaghi, F. Social Participation of Older Adults: A Concept Analysis. Int. J. Community Based Nurs. Midwifery 2020, 8, 55–72. [Google Scholar] [CrossRef]
- Mancini, J.A.; Simon, J. Older Adults’ Expectations of Support from Family and Friends. J. Appl. Gerontol. 1984, 3, 150–160. [Google Scholar] [CrossRef]
- Crist, J.D. The meaning for elders of receiving family care. J. Adv. Nurs. 2005, 49, 485–493. [Google Scholar] [CrossRef]
- Sala, G.; Jopp, D.; Gobet, F.; Ogawa, M.; Ishioka, Y.; Masui, Y.; Inagaki, H.; Nakagawa, T.; Yasumoto, S.; Ishizaki, T.; et al. The impact of leisure activities on older adults' cognitive function, physical function, and mental health. PLoS ONE 2019, 14, e0225006. [Google Scholar] [CrossRef] [Green Version]
- Viscogliosi, C.; Asselin, H.; Basile, S.; Borwick, K.; Couturier, Y.; Drolet, M.J.; Gagnon, D.; Obradovic, N.; Torrie, J.; Zhou, D.; et al. Importance of Indigenous elders’ contributions to individual and community wellness: Results from a scoping review on social participation and intergenerational solidarity. Can. J. Public Health 2020, 111, 667–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aw, S.; Koh, G.; Oh, Y.J.; Wong, M.L.; Vrijhoef, H.J.M.; Harding, S.C.; Geronimo, M.A.B.; Lai, C.Y.F.; Hildon, Z.J.L. Explaining the continuum of social participation among older adults in Singapore: From ‘closed doors’ to active ageing in multi-ethnic community settings. J. Aging Stud. 2017, 42, 46–55. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shamsikhani, S.; Ahmadi, F.; Kazemnejad, A.; Vaismoradi, M. Typology of Family Support in Home Care for Iranian Older People: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 6361. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126361
Shamsikhani S, Ahmadi F, Kazemnejad A, Vaismoradi M. Typology of Family Support in Home Care for Iranian Older People: A Qualitative Study. International Journal of Environmental Research and Public Health. 2021; 18(12):6361. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126361
Chicago/Turabian StyleShamsikhani, Soheila, Fazlollah Ahmadi, Anoshirvan Kazemnejad, and Mojtaba Vaismoradi. 2021. "Typology of Family Support in Home Care for Iranian Older People: A Qualitative Study" International Journal of Environmental Research and Public Health 18, no. 12: 6361. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126361