
Effect of High-Intensity Interval Training and Intermittent Fasting on Body Composition and Physical Performance in Active Women

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
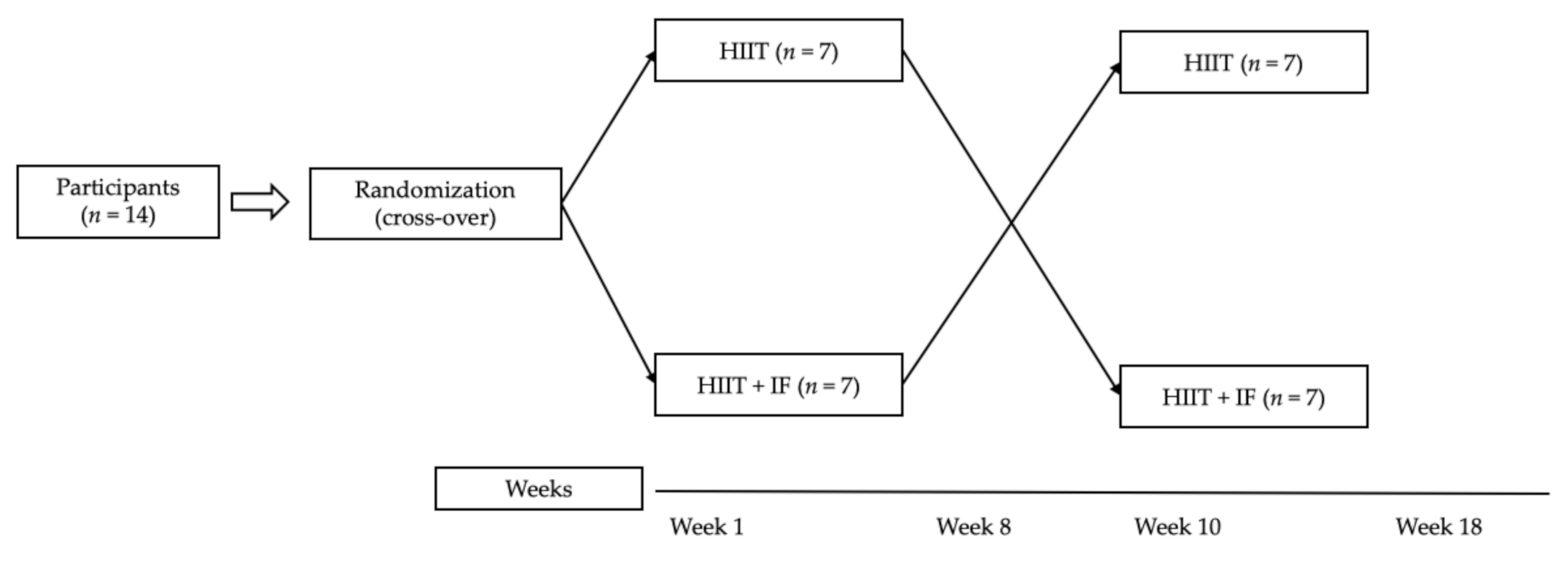
2.1. Study Design
2.2. Participants
2.3. Body-Composition Assessment
2.4. Physical Performance Assessment
2.4.1. Hand-Grip Strength
2.4.2. Counter-Movement Jump
2.4.3. Wingate Anaerobic 30 s Cycling Test
2.5. Nutrition Program: Intermittent Fasting
2.6. Training Program
2.7. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. American College of Sports Medicine. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Patterson, R.E.; Sears, D.D. Metabolic Effects of Intermittent Fasting. Annu. Rev. Nutr. 2017, 37, 371–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinsley, G.M.; La Bounty, P.M. Effects of intermittent fasting on body composition and clinical health markers in humans. Nutr. Rev. 2015, 73, 661–674. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.O.; Wyatt, H.R.; Peters, J.C. Energy balance and obesity. Circulation 2012, 126, 126–132. [Google Scholar] [CrossRef]
- de Cabo, R.; Mattson, M.P. Effects of Intermittent Fasting on Health, Aging, and Disease. N. Engl. J. Med. 2019, 381, 2541–2551. [Google Scholar] [CrossRef]
- Brown, J.E.; Mosley, M.; Aldred, S. Intermittent fasting: A dietary intervention for pre-vention of diabetes and cardiovascular disease? Br. J. Diabetes Vasc. Dis. 2013, 13, 68–72. [Google Scholar] [CrossRef]
- Rothschild, J.; Hoddy, K.K.; Jambazian, P.; Varady, K.A. Time-restricted feeding and risk of metabolic disease: A review of human and animal studies. Nutr. Rev. 2014, 72, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Razenek, R.; Salassi, J.W.; Pinto, N.M.; Fleming, J.D. Acute Cardiopulmonary and Metabolic Responses to High-Intensity Interval Training Protocols Using 60 s ofWork and 60 s Recovery. J. Strength Cond. Res. 2016, 30, 3014–3023. [Google Scholar] [CrossRef] [PubMed]
- Bangsbo, J.; Iaia, F.M.; Krustrup, P. The Yo-Yo intermittent recovery test: A useful tool for evaluation of physical performance in intermittent sports. Sports Med. 2008, 38, 37–51. [Google Scholar] [CrossRef]
- Billat, V. Interval training for performance: A scientific and empirical practice. Special recommendations for middle- and long-distance running. Part II: Anaerobic interval training. Sports Med. 2001, 31, 75–90. [Google Scholar] [CrossRef]
- Hazell, T.J.; Macpherson, R.E.; Gravelle, B.M.; Lemon, P.W. 10 or 30-s sprint interval training bouts enhance both aerobic and anaerobic performance. Eur. J. Appl. Physiol. 2010, 110, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Talanian, J.L.; Galloway, S.D.; Heigenhauser, G.J.; Bonen, A.; Spriet, L.L. Two weeks of high-intensity aerobic interval training increases the capacity for fat oxidation during exercise in women. J. Appl. Physiol. 2007, 102, 1439–1447. [Google Scholar] [CrossRef] [PubMed]
- Astorino, T.A.; Roberson, D.W. Efficacy of acute caffeine ingestion for short-term high-intensity exercise performance: A systematic review. J. Strength Cond. Res. 2010, 24, 257–265. [Google Scholar] [CrossRef]
- Tjønna, A.E.; Lee, S.J.; Rognmo, Ø.; Stølen, T.O.; Bye, A.; Haram, P.M.; Loennechen, J.P.; Al-Share, Q.Y.; Skogvoll, E.; Slørdahl, S.A. Aerobic interval training versus continuous moderate exercise as a treatment for the metabolic syndrome: A pilot study. Circulation 2008, 118, 346–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazell, T.J.; Hamilton, C.D.; Olver, T.D.; Lemon, P.W. Running sprint interval training induces fat loss in women. Appl. Physiol. Nutr. Metab. 2014, 39, 944–950. [Google Scholar] [CrossRef]
- Kemi, O.J.; Wisloff, U. High-intensity aerobic exercise training improves the heart in health and disease. J. Cardiopulm. Rehabil. Prev. 2010, 30, 2–11. [Google Scholar] [CrossRef]
- Gibala, M.J.; Little, J.P.; MacDonald, M.J.; Hawley, J.A. Physiological adaptations to low-volume, high-intensity interval training in health and disease. J. Physiol. 2012, 590, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Guiraud, T.; Nigam, A.; Gremeaux, V.; Meyer, P.; Juneau, M.; Bosquet, L. High-intensity interval training in cardiac rehabilitation. Sports Med. 2012, 42, 587–605. [Google Scholar] [CrossRef]
- Tschakert, G.; Kroepfl, J.; Mueller, A.; Moser, O.; Groeschl, W.; Hofmann, P. How to regulate the acute physiological response to “aerobic” high-intensity interval exercise? J. Sports Sci. Med. 2015, 14, 9–36. [Google Scholar]
- Martin, S.B.; Morrow, J.R.; Jackson, A.W.; Dunn, A.L. Variables related to meeting the CDC/ACSM physical activity guidelines. Med. Sci. Sports Exerc. 2000, 32, 2087–2092. [Google Scholar] [CrossRef] [Green Version]
- Bruinvels, G.; Burden, R.J.; McGregor, A.J.; Ackerman, K.E.; Dooley, M.; Richards, T.; Pedlar, C. Sport, exercise and the menstrual cycle: Where is the research. Br. J. Sports Med. 2017, 51, 487–488. [Google Scholar] [CrossRef] [PubMed]
- Madden, A.M.; Smith, S. Body composition and morphological assessment of nutritional status in adults: A review of anthropometric variables. J. Hum. Nutr. Diet. 2016, 29, 7–25. [Google Scholar] [CrossRef]
- Carter, J.E.L. The Heath-Carter Somatotype Method, 3rd ed.; San Diego State University Syllabus Service: San Diego, CA, USA, 1980. [Google Scholar]
- Lee, R.C.; Wang, Z.; Heo, M.; Ross, R.; Janssen, I.; Heymsfield, S.B. Total-body skeletal muscle mass: Development and cross-validation of anthropometric prediction models. Am. J. Clin. Nutr. 2000, 72, 796–803. [Google Scholar] [CrossRef]
- Wang, Y.C.; Bohannon, R.W.; Li, X.; Sindhu, B.; Kapellusch, J. Hand-Grip Strength: Normative Reference Values and Equations for Individuals 18 to 85 Years of Age Residing in the United States. J. Orthop. Sports Phys. Ther. 2018, 48, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Pizzigalli, L.; Micheletti Cremasco, M.; LA Torre, A.; Rainoldi, A.; Benis, R. Hand grip strength and anthropometric characteristics in Italian female national basketball teams. J. Sports Med. Phys. Fit. 2017, 57, 521–528. [Google Scholar]
- García-Pinillos, F.; Ruiz-Ariza, A.; Moreno del Castillo, R.; Latorre-Román, P.Á. Impact of limited hamstring flexibility on vertical jump, kicking speed, sprint, and agility in young football players. J. Sports Sci. 2015, 33, 1293–1297. [Google Scholar] [CrossRef] [PubMed]
- Bosco, C.; Luhtanen, P.; Komi, P.V. A simple method for measurement of mechanical power in jumping. Eur. J. Appl. Physiol. Occup. Physiol. 1983, 50, 273–282. [Google Scholar] [CrossRef]
- De Blas, X. Proyecto Chronojump-Boscosystem. Herramienta Informática Libre para el Estudio Cinemático del Salto Vertical: Medición del Tiempo, Detección del Ángulo de f Lexión sin Marcadores y Elaboración de Tablas de Percentiles [Chronojump-Boscosystem Project: Free Tool to Study Kinematics Data on Vertical Jump: Time Measurement, Markerless Flexion Angle Detection and Percentile Data]. Ph.D. Thesis, Universitat Ramon Llull, Barcelona, Spain, 2012. [Google Scholar]
- Müller, D.C.; Izquierdo, M.; Boeno, F.P.; Aagaard, P.; Teodoro, J.L.; Grazioli, R.; Radaelli, R.; Bayer, H.; Neske, R.; Pinto, R.S.; et al. Adaptations in mechanical muscle function, muscle morphology, and aerobic power to high-intensity endurance training combined with either traditional or power strength training in older adults: A randomized clinical trial. Eur. J. Appl. Physiol. 2020, 120, 1165–1177. [Google Scholar] [CrossRef]
- Rubio-Arias, J.Á.; Ramos-Campo, D.J.; Esteban, P.; Martínez, F.; Jiménez, J.F. Effect of 6-weeks WBVT on the behaviour of the lower limb muscle fibres during vertical jumping. J. Sports Sci. 2018, 36, 398–406. [Google Scholar] [CrossRef]
- Ziemann, E.; Grzywacz, T.; Łuszczyk, M.; Laskowski, R.; Olek, R.A.; Gibson, A.L. Aerobic and anaerobic changes with high-intensity interval training inactive college-aged men. J. Strength Cond. Res. 2011, 25, 1104. [Google Scholar] [CrossRef]
- Bar-Or, O. The Wingate anaerobic test an update on methodology, reliability and validity. Sports Med. 1987, 4, 381–394. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance. Med. Sci. Sports Exerc. 2016, 48, 543–568. [Google Scholar] [PubMed]
- Dobrowolski, H.; Karczemna, A.; Włodarek, D. Nutrition for Female Soccer Players-Recommendations. Medicina 2020, 56, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Condo, D.; Lohman, R.; Kelly, M.; Carr, A. Nutritional Intake, Sports Nutrition Knowledge and Energy Availability in Female Australian Rules Football Players. Nutrients 2019, 11, 971. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Rodriguez, A.; Vicente-Salar, N.; Montero-Carretero, C.; Cervello, E.; Roche, E. Nutritional strategies to reach the weight category in judo and karate athletes. Arch. Budo. 2015, 11, 381–391. [Google Scholar]
- Catenacci, V.A.; Pan, Z.; Ostendorf, D.; Brannon, S.; Gozansky, W.S.; Mattson, M.P.; Martin, B.; MacLean, P.S.; Melanson, E.L.; Troy Donahoo, W. A randomized pilot study comparing zero-calorie alternate-day fasting to daily caloric restriction in adults with obesity. Obesity 2016, 24, 1874–1883. [Google Scholar] [CrossRef]
- Cho, A.R.; Moon, J.Y.; Kim, S.; An, K.Y.; Oh, M.; Jeon, J.Y.; Jung, D.H.; Choi, M.H.; Lee, J.W. Effects of alternate day fasting and exercise on cholesterol metabolism in overweight or obese adults: A pilot randomized controlled trial. Metabolism 2019, 93, 52–60. [Google Scholar] [CrossRef]
- Hutchison, A.T.; Liu, B.; Wood, R.E.; Vincent, A.D.; Thompson, C.H.; O’Callaghan, N.J.; Wittert, G.A.; Heilbronn, L.K. Effects of Intermittent Versus Continuous Energy Intakes on Insulin Sensitivity and Metabolic Risk in Women with Overweight. Obesity 2019, 27, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Seiler, S.; Jøranson, K.; Olesen, B.V.; Hetlelid, K.J. Adaptations to aerobic interval training: Interactive effects of exercise intensity and total work duration. Scand. J. Med. Sci. Sports 2013, 23, 74–83. [Google Scholar] [CrossRef]
- Buchheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle: Part I: Cardiopulmonary emphasis. Sports Med. 2013, 43, 313–338. [Google Scholar] [CrossRef]
- Follador, L.; Alves, R.C.; Ferreira, S.D.; Buzzachera, C.F.; Andrade, V.S.; Garcia, E.D.; Osiecki, R.; Barbosa, S.C.; Oliveira, L.M.; Silva, S.G. Physiological, Perceptual, and Affective Responses to Six High-Intensity Interval Training Protocols. Percept. Mot. Skills 2018, 125, 329–350. [Google Scholar] [CrossRef]
- Lunt, H.; Draper, N.; Marshall, H.C.; Logan, F.J.; Hamlin, M.J.; Shearman, J.P.; Cotter, J.D.; Kimber, N.E.; Blackwell, G.; Frampton, C.M. High intensity interval training in a real world setting: A randomized controlled feasibility study in overweight inactive adults, measuring change in maximal oxygen uptake. PLoS ONE 2014, 9, e92651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson-John, T.E. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Kunduraci, Y.E.; Ozbek, H. Does the Energy Restriction Intermittent Fasting Diet Alleviate Metabolic Syndrome Biomarkers? A Randomized Controlled Trial. Nutrients 2020, 12, 3213. [Google Scholar] [CrossRef] [PubMed]
- Goodpaster, B.H.; Sparks, L.M. Metabolic Flexibility in Health and Disease. Cell Metab. 2017, 25, 1027–1036. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira-Maranhão-Pureza, I.R.; da Silva-Junior, A.E.; Silva-Praxedes, D.R.; Lessa-Vasconcelos, L.G.; de Lima-Macena, M.; Vieira de Melo, I.S.; de Menezes Toledo Florêncio, T.M.; Bueno, N.B. Effects of time-restricted feeding on body weight, body composition and vital signs in low-income women with obesity: A 12-month randomized clinical trial. Clin. Nutr. 2021, 40, 759–766. [Google Scholar] [CrossRef]
- Sandoval-Insausti, H.; Jiménez-Onsurbe, M.; Donat-Vargas, C.; Rey-García, J.; Banegas, J.R.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Ultra-Processed Food Consumption Is Associated with Abdominal Obesity: A Prospective Cohort Study in Older Adults. Nutrients 2020, 12, 2368. [Google Scholar] [CrossRef]
- Zuo, L.; He, F.; Tinsley, G.M.; Pannell, B.K.; Ward, E.; Arciero, P.J. Comparison of High-Protein, Intermittent Fasting Low-Calorie Diet and Heart Healthy Diet for Vascular Health of the Obese. Front. Physiol. 2016, 29, 350. [Google Scholar] [CrossRef] [Green Version]
- Amstrup, A.K.; Sikjaer, T.; Pedersen, S.B.; Heickendorff, L.; Mosekilde, L.; Rejnmark, L. Reduced fat mass and increased lean mass in response to 1 year of melatonin treatment in postmenopausal women: A randomized placebo-controlled trial. Clin. Endocrinol. 2016, 84, 342–347. [Google Scholar] [CrossRef]
- Lucas, R.W.D.C.; Nassif, P.A.N.; Tabushi, F.I.; Nassif, D.S.B.; Ariede, B.L.; Brites-Neto, J.; Malafaia, O. Can stature, abdominal perimeter and BMI index predict possible cardiometabolic risk in future obesity? Arq. Bras. Cir. Dig. 2020, 33, 1529. [Google Scholar] [CrossRef]
- Ruiz-Moreno, M.I.; Vilches-Perez, A.; Gallardo-Escribano, C.; Vargas-Candela, A.; Lopez-Carmona, M.D.; Pérez-Belmonte, L.M.; Ruiz-Moreno, A.; Gomez-Huelgas, R.; Bernal-Lopez, M.R. Metabolically Healthy Obesity: Presence of Arterial Stiffness in the Prepubescent Population. Int. J. Environ. Res. Public Health 2020, 17, 6995. [Google Scholar] [CrossRef] [PubMed]
- Hottenrott, K.; Werner, T.; Hottenrott, L.; Meyer, T.P.; Vormann, J. Exercise Training, Intermittent Fasting and Alkaline Supplementation as an Effective Strategy for Body Weight Loss: A 12-Week Placebo-Controlled Double-Blind Intervention with Overweight Subjects. Life 2020, 10, 74. [Google Scholar] [CrossRef] [PubMed]
- Moro, T.; Tinsley, G.; Longo, G.; Grigoletto, D.; Bianco, A.; Ferraris, C.; Guglielmetti, M.; Veneto, A.; Tagliabue, A.; Marcolin, G.; et al. Time-restricted eating effects on performance, immune function, and body composition in elite cyclists: A randomized controlled trial. J. Int. Soc. Sports Nutr. 2020, 17, 65. [Google Scholar] [CrossRef] [PubMed]
- Stratton, M.T.; Tinsley, G.M.; Alesi, M.G.; Hester, G.M.; Olmos, A.A.; Serafini, P.R.; Modjeski, A.S.; Mangine, G.T.; King, K.; Savage, S.N.; et al. Four Weeks of Time-Restricted Feeding Combined with Resistance Training Does Not Differentially Influence Measures of Body Composition, Muscle Performance, Resting Energy Expenditure, and Blood Biomarkers. Nutrients 2020, 12, 1126. [Google Scholar] [CrossRef]
- Domaszewski, P.; Konieczny, M.; Pakosz, P.; Bączkowicz, D.; Sadowska-Krępa, E. Effect of a Six-Week Intermittent Fasting Intervention Program on the Composition of the Human Body in Women over 60 Years of Age. Int. J. Environ. Res. Public Health 2020, 17, 4138. [Google Scholar] [CrossRef]
- Ivy, J.L.; Goforth, H.W., Jr.; Damon, B.M.; McCauley, T.R.; Parsons, E.C.; Price, T.B. Early postexercise muscle glycogen recovery is enhanced with a carbohydrate-protein supplement. J. Appl. Physiol. 2002, 93, 337–344. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ANOVA Main Effects | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Training Effects | Group Effects | Main Effects (Training x Group) | ||||||||||||
| Variables | Group | Pre | SD | Post | SD | F | p | η2 p | F | p | η2 p | F | p | η2 p |
| Body mass (kg) | HIIT | 58.9 | 6.2 | 59 | 5.8 | 1.099 | 0.314 | 0.078 | 0.814 | 0.383 | 0.059 | 1.802 | 0.202 | 0.122 |
| HIIT + IF | 59.9 | 5.7 | 58.8 | 6.4 | ||||||||||
| Skinfolds (mm) | Factor | Pre | SD | Post | SD | F | p | η2 p | F | p | η2 p | F | p | η2 p |
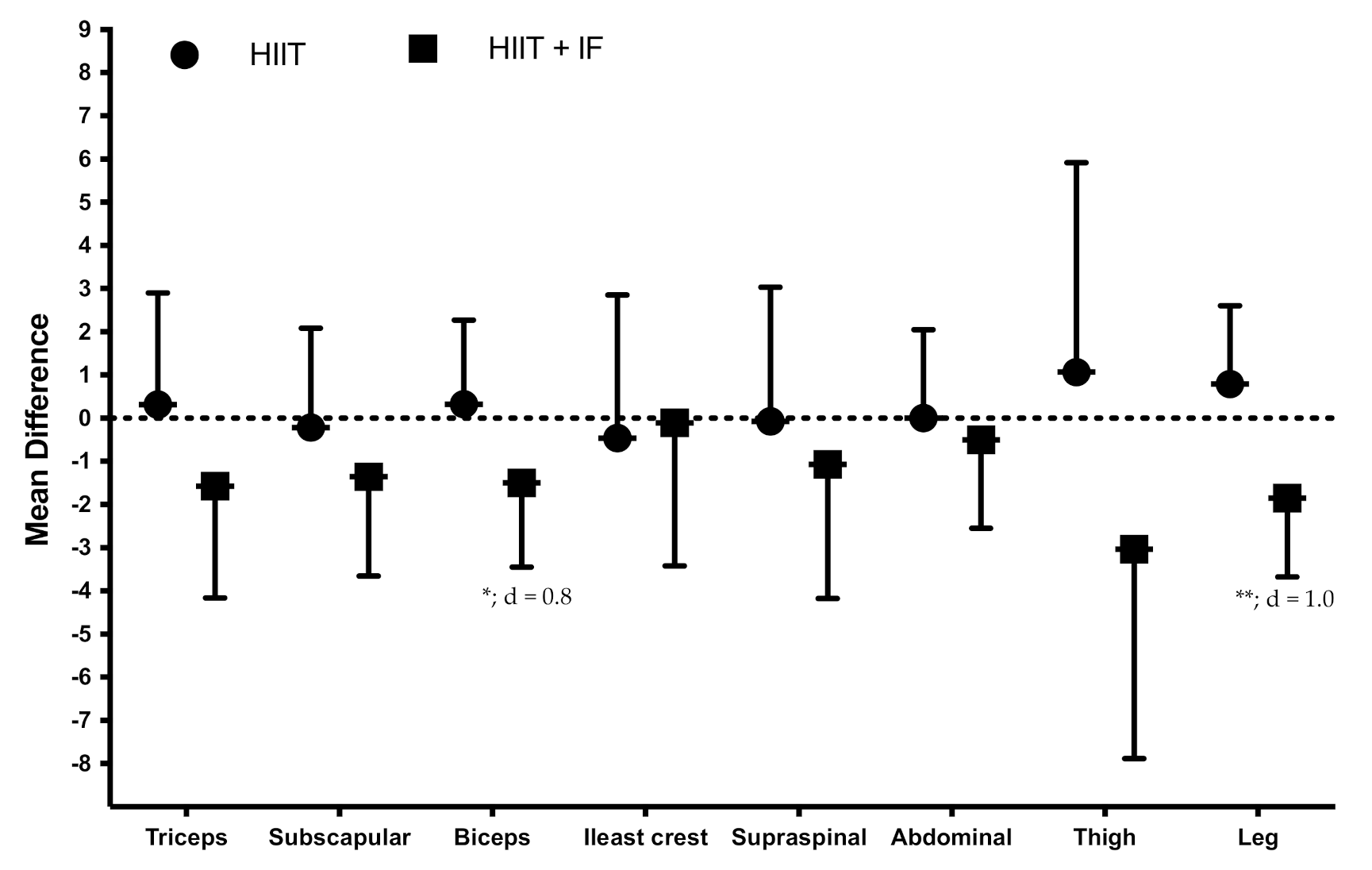
| Triceps | HIIT | 16.5 | 5 | 16.9 | 3.3 | 1.099 | 0.314 | 0.078 | 0.814 | 0.383 | 0.059 | 7.407 | 0.017 | 0.363 |
| HIIT + IF | 17 | 4.8 | 15.4 | 3.9 | ||||||||||
| Subscapular | HIIT | 10.3 | 2.4 | 10.1 | 1.7 | 1.099 | 0.314 | 0.078 | 0.814 | 0.383 | 0.059 | 2.177 | 0.164 | 0.143 |
| HIIT + IF | 11.2 | 2.3 | 9.9 | 1.6 | ||||||||||
| Biceps | HIIT | 5.1 | 2.3 | 5.5 | 2.4 | 3.402 | 0.088 | 0.207 | 1.968 | 0.215 | 0.116 | 4.937 | 0.045 | 0.275 |
| HIIT + IF | 6.5 | 2.4 | 5.0 | 2.1 | ||||||||||
| Iliac crest | HIIT | 13.5 | 3.9 | 13.1 | 3.8 | 0.256 | 0.621 | 0.019 | 1.849 | 0.197 | 0.125 | 0.068 | 0.798 | 0.005 |
| HIIT + IF | 14.3 | 3.6 | 14.1 | 3.9 | ||||||||||
| Supraspinal | HIIT | 10.9 | 4.7 | 10.8 | 3.5 | 0.825 | 0.380 | 0.060 | 0.066 | 0.801 | 0.005 | 0.852 | 0.373 | 0.062 |
| HIIT + IF | 11.3 | 4.1 | 10.3 | 3.3 | ||||||||||
| Abdominal | HIIT | 12.9 | 2.5 | 12.9 | 2.7 | 0.552 | 0.471 | 0.041 | 1.099 | 0.314 | 0.078 | 0.333 | 0.574 | 0.025 |
| HIIT + IF | 13.6 | 3.4 | 13.1 | 3.1 | ||||||||||
| Thigh | HIIT | 23.4 | 5.1 | 24.4 | 7.1 | 1.595 | 0.229 | 0.109 | 0.244 | 0.630 | 0.018 | 3.931 | 0.069 | 0.232 |
| HIIT + IF | 25.7 | 7.1 | 22.6 | 4.3 | ||||||||||
| Leg | HIIT | 16.4 | 4.7 | 17.2 | 4.9 | 2.336 | 0.155 | 0.152 | 0.412 | 0.532 | 0.031 | 15.369 | 0.002 | 0.542 |
| HIIT + IF | 18.1 | 6 | 16.2 | 6 | ||||||||||
| Girths (cm) | Factor | Pre | SD | Post | SD | F | p | η2 p | F | p | η2 p | F | p | η2 p |
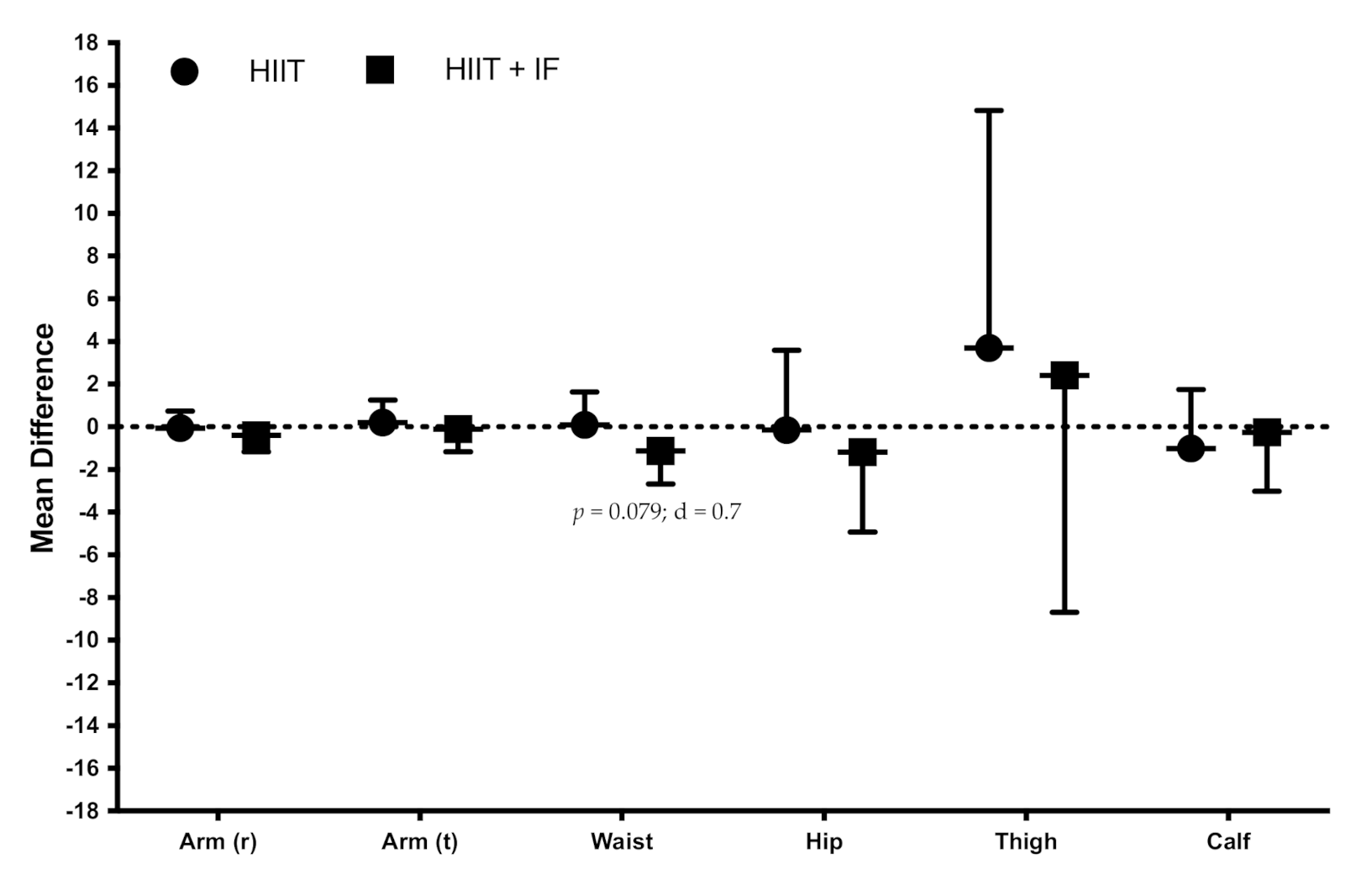
| Arm (relaxed) | HIIT | 26.4 | 2.2 | 26.4 | 1.8 | 2.210 | 0.161 | 0.145 | 0.356 | 0.561 | 0.027 | 1.273 | 0.28 | 0.089 |
| HIIT + IF | 26.7 | 2.1 | 26.3 | 2.1 | ||||||||||
| Arm (flexed and tensed) | HIIT | 26.6 | 1.9 | 26.5 | 1.9 | 0.095 | 0.763 | 0.007 | 0.295 | 0.596 | 0.022 | 0.470 | 0.505 | 0.035 |
| HIIT + IF | 26.3 | 1.9 | 26.2 | 1.9 | ||||||||||
| Waist | HIIT | 68.5 | 3.8 | 68.6 | 3.8 | 3.954 | 0.068 | 0.233 | 11.220 | 0.005 | 0.463 | 3.382 | 0.089 | 0.206 |
| HIIT + IF | 68.2 | 3.7 | 67.1 | 3.5 | ||||||||||
| Hip | HIIT | 95.9 | 4.4 | 95.8 | 7.5 | 0.723 | 0.411 | 0.053 | 0.204 | 0.659 | 0.015 | 0.684 | 0.423 | 0.05 |
| HIIT + IF | 96.9 | 6.4 | 95.7 | 6 | ||||||||||
| Thigh | HIIT | 44.2 | 8.6 | 48.0 | 5.9 | 2.409 | 0.145 | 0.156 | 3.105 | 0.102 | 0.193 | 0.083 | 0.778 | 0.006 |
| HIIT + IF | 48.4 | 5.9 | 50.8 | 12.5 | ||||||||||
| Calf | HIIT | 36.21 | 2.31 | 35.21 | 4.996 | 1.409 | 0.256 | 0.098 | 0.010 | 0.923 | 0.001 | 0.534 | 0.478 | 0.039 |
| HIIT + IF | 35.89 | 2.5 | 35.63 | 2.95 | ||||||||||
| ANOVA Main Effects | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Training Effects | Group Effects | Main Effects (Time x Group) | ||||||||||||
| Variable | Group | Pre | SD | Post | SD | F | p | η2 p | F | p | η2 p | F | p | η2 p |
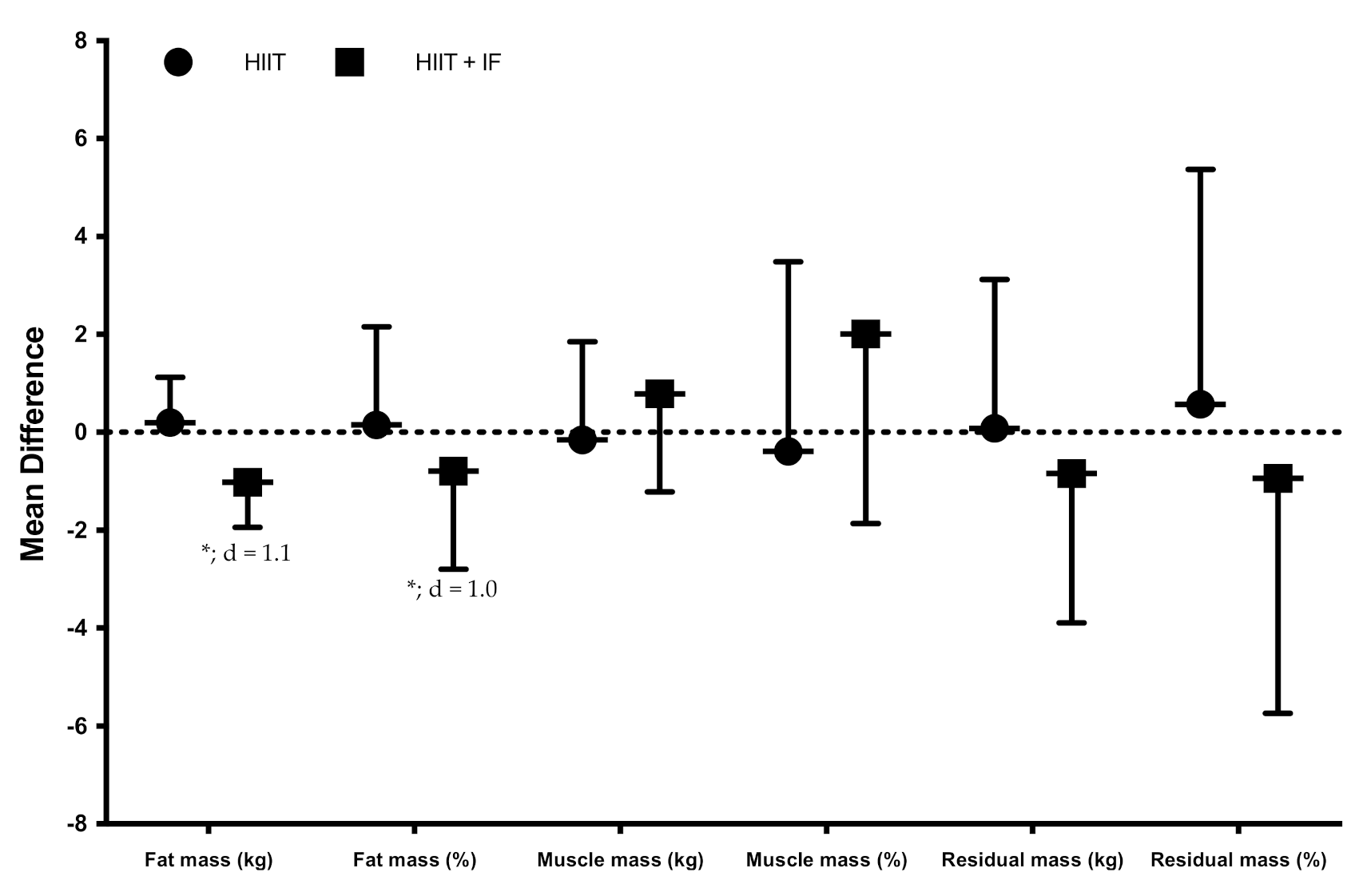
| Fat mass (kg) | HIIT | 10.4 | 2.4 | 10.6 | 2.41 | 3.492 | 0.084 | 0.212 | 0.976 | 0.341 | 0.07 | 26.421 | <0.001 | 0.67 |
| HIIT + IF | 11.2 | 2.7 | 10.2 | 2.6 | ||||||||||
| Fat mass (%) | HIIT | 17.6 | 2.9 | 17.9 | 2.8 | 3.466 | 0.085 | 0.211 | 0.535 | 0.477 | 0.044 | 14.084 | 0.002 | 0.52 |
| HIIT + IF | 18.6 | 3.3 | 17.1 | 2.8 | ||||||||||
| Muscle mass (kg) | HIIT | 21.0 | 2.2 | 20.81 | 2.83 | 0.684 | 0.423 | 0.05 | 1.797 | 0.203 | 0.121 | 1.632 | 0.224 | 0.112 |
| HIIT + IF | 21.0 | 1.9 | 21.8 | 2.7 | ||||||||||
| Muscle mass (%) | HIIT | 35.7 | 2.5 | 35.3 | 3.5 | 1.083 | 0.317 | 0.077 | 0.994 | 0.337 | 0.071 | 3.111 | 0.101 | 0.193 |
| HIIT + IF | 35.2 | 2.9 | 37.2 | 4.9 | ||||||||||
| Residual mass (kg) | HIIT | 18.1 | 2.9 | 18.17 | 2.1 | 0.392 | 0.542 | 0.029 | 0.241 | 0.631 | 0.018 | 0.737 | 0.406 | 0.054 |
| HIIT + IF | 18.3 | 3.4 | 17.4 | 3.7 | ||||||||||
| Residual mass (%) | HIIT | 30.5 | 3.5 | 31.0 | 3.3 | 0.032 | 0.86 | 0.003 | 0.687 | 0.424 | 0.054 | 0.906 | 0.36 | 0.07 |
| HIIT + IF | 30.5 | 4.4 | 29.5 | 5.3 | ||||||||||
| ANOVA Main Effects | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Training Effects | Group Effects | Main Effects (Training x Group) | ||||||||||||
| Group | Pre | SD | Post | SD | F | p | η2 p | F | p | η2 p | F | p | η2 p | |
| Left HGS (kg) | HIIT | 29.3 | 3.9 | 27.4 | 3.4 | 6.626 | 0.023 | 0.338 | 0.769 | 0.369 | 0.056 | 0.326 | 0.578 | 0.024 |
| HIIT + IF | 29.4 | 3.8 | 28.1 | 3.0 | ||||||||||
| Right HGS (kg) | HIIT | 29.6 | 4.2 | 28.4 | 3.3 | 0.435 | 0.521 | 0.032 | 1.266 | 0.281 | 0.089 | 3.265 | 0.094 | 0.201 |
| HIIT + IF | 29.2 | 4.1 | 29.7 | 3.0 | ||||||||||
| CMJ (cm) | HIIT | 17.5 | 4.3 | 18.5 | 3.9 | 30.21 | <0.001 | 0.699 | 21.15 | <0.001 | 0.662 | 22.46 | <0.001 | 0.633 |
| HIIT + IF | 17.5 | 4.2 | 23.7 | 4.4 | ||||||||||
| RMP (W) | HIIT | 148.4 | 27.9 | 149.1 | 28.5 | 0.07 | 0.795 | 0.005 | 13.000 | 0.003 | 0.5 | 0.003 | 0.955 | 0.000 |
| HIIT + IF | 134.6 | 30.9 | 135.0 | 20.9 | ||||||||||
| RPP (W) | HIIT | 295.3 | 37.8 | 295.6 | 40.7 | 0.761 | 0.399 | 0.055 | 0.036 | 0.852 | 0.003 | 0.817 | 0.382 | 0.059 |
| HIIT + IF | 297.0 | 42.1 | 289.6 | 46.8 | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Rodríguez, A.; Rubio-Arias, J.A.; García-De Frutos, J.M.; Vicente-Martínez, M.; Gunnarsson, T.P. Effect of High-Intensity Interval Training and Intermittent Fasting on Body Composition and Physical Performance in Active Women. Int. J. Environ. Res. Public Health 2021, 18, 6431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126431
Martínez-Rodríguez A, Rubio-Arias JA, García-De Frutos JM, Vicente-Martínez M, Gunnarsson TP. Effect of High-Intensity Interval Training and Intermittent Fasting on Body Composition and Physical Performance in Active Women. International Journal of Environmental Research and Public Health. 2021; 18(12):6431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126431
Chicago/Turabian StyleMartínez-Rodríguez, Alejandro, Jacobo A. Rubio-Arias, José M. García-De Frutos, Manuel Vicente-Martínez, and Thomas P. Gunnarsson. 2021. "Effect of High-Intensity Interval Training and Intermittent Fasting on Body Composition and Physical Performance in Active Women" International Journal of Environmental Research and Public Health 18, no. 12: 6431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126431