
Psychological Effects of Home Confinement and Social Distancing Derived from COVID-19 in the General Population—A Systematic Review

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
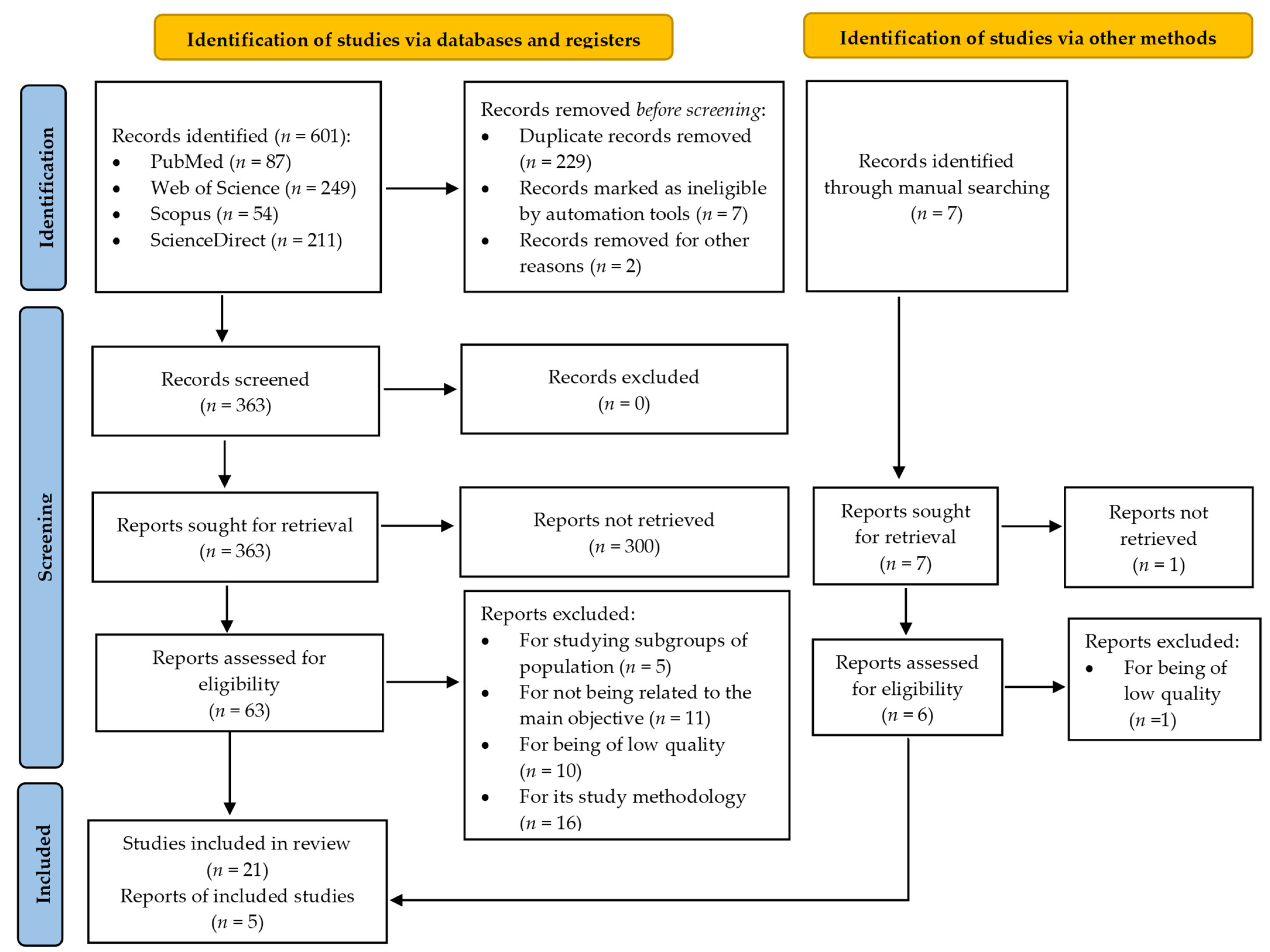
3. Results
3.1. Description of the Characteristics of the Studies
3.2. Description of the Results
3.2.1. Anxiety Symptoms and Associated Factors
3.2.2. Depressive Symptoms and Associated Factors
3.2.3. Stress Symptoms, PTSD and Associated Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV). Available online: https://www.who.int/news/item/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 17 February 2021).
- Xiao, H.; Zhang, Y.; Kong, D.; Li, S.; Yang, N. Social capital and sleep quality in individuals who self-isolated for 14 days during the coronavirus disease 2019 (COVID-19) outbreak in January 2020 in China. Med. Sci. Monit. 2020, 26, e923921. [Google Scholar] [CrossRef]
- López-Bueno, R.; Calatayud, J.; Casaña, J.; Casajús, J.A.; Smith, L.; Tully, M.A.; Andersen, L.L.; López-Sánchez, G.F. COVID-19 Confinement and Health Risk Behaviors in Spain. Front. Psychol. 2020, 11, 1426. [Google Scholar] [CrossRef]
- Hawryluck, L.; Gold, W.L.; Robinson, S.; Pogorski, S.; Galea, S.; Styra, R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg. Infect. Dis. 2004, 10, 1206–1212. [Google Scholar] [CrossRef]
- Galea, S.; Merchant, R.M.; Lurie, N. The Mental Health Consequences of COVID-19 and Physical Distancing: The Need for Prevention and Early Intervention. JAMA Intern. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dsouza, D.D.; Quadros, S.; Hyderabadwala, Z.J.; Mamun, M.A. Aggregated COVID-19 suicide incidences in India: Fear of COVID-19 infection is the prominent causative factor. Psychiatry Res. 2020, 290, 113145. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef]
- Rubin, G.J.; Wessely, S. The psychological effects of quarantining a city. BMJ 2020, 368, m313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tull, M.T.; Edmonds, K.A.; Scamaldo, K.M.; Richmond, J.R.; Rose, J.P.; Gratz, K.L. Psychological Outcomes Associated with Stay-at-Home Orders and the Perceived Impact of COVID-19 on Daily Life. Psychiatry Res. 2020, 289, 113098. [Google Scholar] [CrossRef]
- Neria, Y.; Nandi, A.; Galea, S. Post-traumatic stress disorder following disasters: A systematic review. Psychol. Med. 2008, 38, 467–480. [Google Scholar] [CrossRef]
- Tracy, M.; Norris, F.H.; Galea, S. Differences in the determinants of posttraumatic stress disorder and depression after a mass traumatic event. Depress. Anxiety 2011, 28, 666–675. [Google Scholar] [CrossRef] [Green Version]
- Galea, S.; Ahern, J.; Resnick, H. Psychological sequelae of the September 11 terrorist attacks in New York City. N. Engl. J. Med. 2002, 346, 982–987. [Google Scholar] [CrossRef] [PubMed]
- Vlahov, D.; Galea, S.; Ahern, J.; Resnick, H.; Kilpatrick, D. Sustained Increased Consumption of Cigarettes, Alcohol, and Marijuana among Manhattan Residents after September 11, 2001. Am. J. Public Health 2004, 94, 253–254. [Google Scholar] [CrossRef] [PubMed]
- Grattan, L.M.; Roberts, S.; Mahan, W.T.; McLaughlin, P.K.; Otwell, W.S.; Morris, J.G. The early psychological impacts of the deepwater horizon oil spill on florida and alabama communities. Environ. Health Perspect. 2011, 119, 838–843. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.M.; Wong, J.G.W.S.; McAlonan, G.M.; Cheung, V.; Cheung, C.; Sham, P.C.; Tsang, K.W.; Chua, S.E. Stress and psychological distress among SARS survivors 1 year after the outbreak. Can. J. Psychiatry 2007, 52, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Marques de Miranda, D.; da Silva Athanasio, B.; Sena Oliveira, A.C.; Simoes-e-Silva, A.C. How is COVID-19 pandemic impacting mental health of children and adolescents? Int. J. Disaster Risk Reduct. 2020, 51, 101845. [Google Scholar] [CrossRef]
- Shigemura, J.; Ursano, R.J.; Morganstein, J.C.; Kurosawa, M.; Benedek, D.M. Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: Mental health consequences and target populations. Psychiatry Clin. Neurosci. 2020, 74, 281–282. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Casagrande, M.; Favieri, F.; Tambelli, R.; Forte, G. The enemy who sealed the world: Effects quarantine due to the COVID-19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Med. 2020, 75, 12–20. [Google Scholar] [CrossRef]
- Urrútia, G.; Bonfill, X. PRISMA declaration: A proposal to improve the publication of systematic reviews and meta-analyses. Med. Clin. 2010, 135, 507–511. [Google Scholar] [CrossRef]
- Sackett, D.L.; Rosenberg, W.M.C.; Gray, J.A.M.; Haynes, R.B.; Richardson, W.S. Evidence based medicine: What it is and what it isn’t. 1996. Clin. Orthop. Relat. Res. 2007, 455, 3–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, Z.; Lockwood, C.; Munn, Z.; Aromataris, E. The updated Joanna Briggs Institute Model of Evidence-Based Healthcare. Int. J. Evid. Based Healthc. 2019, 17, 58–71. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetc, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic Reviews of Etiology and Risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J.; Hopp, L. Chapter 3: Systematic reviews of effectiveness. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef]
- Alkhamees, A.A.; Alrashed, S.A.; Alzunaydi, A.A.; Almohimeed, A.S.; Aljohani, M.S. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr. Psychiatry 2020, 102, 152192. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Chtourou, H.; Boukhris, O.; Trabelsi, K.; Masmoudi, L.; Brach, M.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. COVID-19 Home Confinement Negatively Impacts Social Participation and Life Satisfaction: AWorldwide Multicenter Study. Int. J. Environ. Res. Public Health 2020, 17, 6237. [Google Scholar] [CrossRef] [PubMed]
- Benke, C.; Autenrieth, L.K.; Asselmann, E.; Pané-Farré, C.A. Lockdown, quarantine measures, and social distancing: Associations with depression, anxiety and distress at the beginning of the COVID-19 pandemic among adults from Germany. Psychiatry Res. 2020, 293, 113462. [Google Scholar] [CrossRef]
- Chen, L.; Zhao, H.; Razin, D.; Song, T.; Wu, Y.; Ma, X.; Aji, H.; Wang, G.; Wang, M.; Yan, L. Anxiety levels during a second local COVID-19 pandemic breakout among quarantined people: A cross sectional survey in China. J. Psychiatr. Res. 2021, 135, 37–46. [Google Scholar] [CrossRef]
- Dean, D.J.; Tso, I.F.; Giersch, A.; Lee, H.-S.; Baxter, T.; Griffith, T.; Song, L.; Park, S. Cross-cultural comparisons of psychosocial distress in the USA, South Korea, France, and Hong Kong during the initial phase of COVID-19. Psychiatry Res. 2021, 295, 113593. [Google Scholar] [CrossRef] [PubMed]
- González-Sanguino, C.; Ausín, B.; Castellanos, M. Ángel; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef]
- Goularte, J.F.; Serafim, S.D.; Colombo, R.; Hogg, B.; Caldieraro, M.A.; Rosa, A.R. COVID-19 and mental health in Brazil: Psychiatric symptoms in the general population. J. Psychiatr. Res. 2021, 132, 32–37. [Google Scholar] [CrossRef]
- Hazarika, M.; Das, S.; Bhandari, S.S.; Sharma, P. The psychological impact of the COVID-19 pandemic and associated risk factors during the initial stage among the general population in India. Open J. Psychiatry Allied Sci. 2021, 12, 31. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef] [PubMed]
- Lal, A.; Sanaullah, A.; Saleem, M.K.; Ahmed, N.; Maqsood, A.; Ahmed, N. Psychological Distress among Adults in Home Confinement in the Midst of COVID-19 Outbreak. Eur. J. Dent. 2020, 14, S27–S33. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.S.; Dean, D.; Baxter, T.; Griffith, T.; Park, S. Deterioration of mental health despite successful control of the COVID-19 pandemic in South Korea. Psychiatry Res. 2021, 295, 113570. [Google Scholar] [CrossRef]
- Lei, L.; Huang, X.; Zhang, S.; Yang, J.; Yang, L.; Xu, M. Comparison of Prevalence and Associated Factors of Anxiety and Depression among People Affected by versus People Unaffected by Quarantine during the COVID-19 Epidemic in Southwestern China. Med Sci. Monit. 2020, 26. [Google Scholar] [CrossRef] [Green Version]
- Massad, I.; Al-Taher, R.; Massad, F. The impact of the COVID-19 pandemic on mental health: Early quarantine-related anxiety and its correlates among Jordanians | Read by QxMD. East. Mediterr. Health J. 2020, 26, 1165–1172. [Google Scholar] [CrossRef]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- Duong, K.N.C.; Le Bao, T.N.; Nguyen, P.T.L.; Van, T.V.; Lam, T.P.; Gia, A.P.; Anuratpanich, L.; Van, B.V. Psychological Impacts of Coronavirus Disease 2019 (COVID-19) during the First Nationwide Lockdown in Vietnam: An Internet-based Survey. JMIR Form. Res. 2020, 4, e24776. [Google Scholar] [CrossRef]
- Özdin, S.; Bayrak Özdin, Ş. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. [Google Scholar] [CrossRef]
- Planchuelo-Gómez, Á.; Odriozola-González, P.; Irurtia, M.J.; de Luis-García, R. Longitudinal evaluation of the psychological impact of the COVID-19 crisis in Spain. J. Affect. Disord. 2020, 277, 842–849. [Google Scholar] [CrossRef] [PubMed]
- Ripon, R.K.; Mim, S.S.; Puente, A.E.; Hossain, S.; Babor, M.H.; Sohan, S.A.; Islam, N. COVID-19: Psychological effects on a COVID-19 quarantined population in Bangladesh. Heliyon 2020, 6, e05481. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rey, R.; Garrido-Hernansaiz, H.; Collado, S. Psychological Impact and Associated Factors During the Initial Stage of the Coronavirus (COVID-19) Pandemic Among the General Population in Spain. Front Psychol. 2020, 11, 1540. [Google Scholar] [CrossRef]
- Schweda, A.; Weismüller, B.; Bäuerle, A.; Dörrie, N.; Musche, V.; Fink, M.; Kohler, H.; Teufel, M.; Skoda, E.-M. Phenotyping mental health: Age, community size, and depression differently modulate COVID-19-related fear and generalized anxiety. Compr. Psychiatry 2021, 104, 152218. [Google Scholar] [CrossRef]
- Sherman, A.C.; Williams, M.L.; Amick, B.C.; Hudson, T.J.; Messias, E.L. Mental health outcomes associated with the COVID-19 pandemic: Prevalence and risk factors in a southern US state. Psychiatry Res. 2020, 293, 113476. [Google Scholar] [CrossRef]
- Shevlin, M.; McBride, O.; Murphy, J.; Miller, J.G.; Hartman, T.K.; Levita, L.; Mason, L.; Martinez, A.P.; McKey, R.; Stocks, T.V.A.; et al. Anxiety, depression, traumatic stress and COVID-19-related anxiety in the UK general population during the COVID-19 pandemic. BJPsych Open 2020, 6. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Jacob, L.; Yakkundi, A.; McDermott, D.; Armstrong, N.C.; Barnett, Y.; López-Sánchez, G.F.; Martin, S.; Butler, L.; A Tully, M. Correlates of symptoms of anxiety and depression and mental wellbeing associated with COVID-19: A cross-sectional study of UK-based respondents. Psychiatry Res. 2020, 291, 113138. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Almeida, M.; Shrestha, A.D.; Stojanac, D.; Miller, L.J. The impact of the COVID-19 pandemic on women’s mental health. Arch. Women Ment. Health 2020, 23, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Glowacz, F.; Schmits, E. Psychological distress during the COVID-19 lockdown: The young adults most at risk. Psychiatry Res. 2020, 293, 113486. [Google Scholar] [CrossRef]
- Hertz-Palmor, N.; Moore, T.M.; Gothelf, D.; DiDomenico, G.E.; Dekel, I.; Greenberg, D.M.; Brown, L.A.; Matalon, N.; Visoki, E.; White, L.K.; et al. Association among income loss, financial strain and depressive symptoms during COVID-19: Evidence from two longitudinal studies. medRxiv 2020. [Google Scholar] [CrossRef]
- Castro-De-Araujo, L.F.S.; Machado, D.B. Impact of covid-19 on mental health in a low and middle-income country. Cienc Saude Coletiva 2020, 25, 2457–2460. [Google Scholar] [CrossRef] [PubMed]
- Goulia, P.; Mantas, C.; Dimitroula, D.; Mantis, D.; Hyphantis, T. General hospital staff worries, perceived sufficiency of information and associated psychological distress during the A/H1N1 influenza pandemic. BMC Infect. Dis. 2010, 10, 322. [Google Scholar] [CrossRef] [Green Version]
- González-Padilla, D.A.; Tortolero-Blanco, L. Social media influence in the COVID-19 pandemic. Int. Braz. J. Urol. 2020, 46, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Blanca, B.P.; Luengo-Charath, M.X.; Verónica, A.M.; Bascuñán, M.L.R.; Pacheco, I.M.M.; Patricio, M.C.; Ricardo, V.Y. The responsible use and dissemination of information in a pandemic: An ethical imperative. Rev. Chil. Pediatría 2020, 91, 794–799. [Google Scholar] [CrossRef]
- Sasidharan, S.; Harpreet Singh, D.; Vijay, S.; Manalikuzhiyil, B. COVID-19: Pan(info)demic. Turk. J. Anaesthesiol. Reanim. 2020, 48, 438–442. [Google Scholar] [CrossRef]
- Coronavirus Disease (COVID-19) Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 25 February 2021).
- Rathore, F.A.; Farooq, F. Information overload and infodemic in the COVID-19 pandemic. J. Pak. Med. Assoc. 2020, 70, S162–S165. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Vivanco, L. Unesco sobre el covid-19: Directrices éticas para una respuesta global unesco on covid-19: Ethical guidelines for a global response. Cuad. Bioética 2020, 31, 269–273. [Google Scholar] [CrossRef]
- Ruiz-Frutos, C.; Ortega-Moreno, M.; Dias, A.; Bernardes, J.M.; García-Iglesias, J.J.; Gómez-Salgado, J. Information on COVID-19 and psychological distress in a sample of non-health workers during the pandemic period. Int. J. Environ. Res. Public Health 2020, 17, 6982. [Google Scholar] [CrossRef]


{kind=link}
| Population | General adult population |
| Intervention | Measure the effect of social distancing and home confinement resulting from the COVID-19 pandemic on mental health |
| Outcomes | Depression level, stress level and anxiety level |
| Research Question | Do the social distancing and home confinement regulations resulting from the SAR-CoV-2 pandemic have repercussions on the mental health of the general population, affecting their levels of anxiety, stress or depression? |
| Database | Search Strategy |
|---|---|
| Pubmed | (“sars virus”(MeSH Terms) OR “sars virus”(Title/Abstract) OR “SARS-Cov-2”(MeSH Terms) OR “SARS-Cov-2”(Title/Abstract) OR “pandemic”(Title/Abstract) OR “severe acute respiratory syndrome coronavirus”(Title/Abstract) OR “COVID-19”(Title/Abstract)) AND (“mental health”(MeSH Terms) OR “mental health”(Title/Abstract) OR “Psychological health”(Title/Abstract)) AND (“home confinement”(Title/Abstract) OR “physical distancing”(MeSH Terms) OR “physical distancing”(Title/Abstract)) AND (“adult”(MeSH Terms) OR “adult”(Title/Abstract) OR “general population”(Title/Abstract) OR “general public”(Title/Abstract) OR “public”(Title/Abstract) OR “community”(Title/Abstract)) |
| Web of Science | TS = (sars virus OR SARS-Cov-2 OR pandemic OR severe Acute Respiratory Syndrome Coronavirus OR COVID-19) AND TS = (mental health OR Psychological health) AND TS = (home confinement OR Physical Distancing) AND TS = (adult OR general population OR general public OR public OR community) |
| Scopus | TITLE-ABS-KEY ((“sars virus”) OR (SARS-Cov-2) OR (pandemic) OR (“severe Acute Respiratory Syndrome Coronavirus”) OR (COVID-19)) AND TITLE-ABS-KEY ((“mental health”) “ OR (“Psychological health”)) AND TITLE-ABS-KEY ((“home confinement” OR “Physical Distancing”)) AND TITLE-ABS-KEY ((adult) OR (“general population”) OR (“general public”) OR (public) OR (community)) |
| Science Direct | (“sars virus” OR SARS-Cov-2 OR pandemic OR “severe Acute Respiratory Syndrome Coronavirus” OR COVID-19) AND (“mental health” OR “Psychological health”) AND (“home confinement” OR “Physical Distancing”) AND (adult OR “general population” OR “general public” OR public OR community) |
| Study/Author | Typology/Main Objective | Participants | Variables/ Instruments | Main Findings | JBI |
|---|---|---|---|---|---|
| Ahmed et al. [25], 2020 | Design: Descriptive cross-sectional, Objective: To study the psychological morbidity induced by the COVID-19 pandemic. | n = 1074 Age: >18 years Sex (f/m): 503/571 | Anxiety: BAI Depression: BDI | In total, 29% suffered high levels of anxiety, and 37.1% presented different forms of depression. The proportion of people with different levels of anxiety (p < 0.001) and depression (p < 0.001) was significantly higher in the age group 21–30 years. | 6/8 |
| Alkhamees et al. [26], 2020 | Design: Quantitative cross-sectional Objective: To assess the psychological impact of the COVID-19 pandemic during the curfew and closure. | n = 1160 Age: >18 years Sex (f/m): 741/419 | Anxiety: DASS-21 Depression: DASS-21 Stress: DASS-21 PTSD: IES-R | In total, 28.3%, 24% and 22.3% reported moderate or severe depression, anxiety and stress, respectively. The female sex, the age 18–40, and being a student were significantly associated with higher levels of PTSD, anxiety, depression and stress (p < 0.05). Experiencing shortness of breath and dizziness showed a strong association with levels of anxiety, stress and depression (p < 0.001). Social distancing decreased stress and anxiety (p < 0.05), while hand hygiene decreased depression (p < 0.05). | 8/8 |
| Ammar et al. [27], 2020 | Design: Quantitative cross-sectional Objective: To analyse the impact of COVID-19 restrictions on mental health and emotional well-being. | n = 1047 Age: >18 years Sex (f/m): 563/484 | Depression: SMFQ | A significant change was observed in mood, well-being and feelings (p < 0.001); participants showed more depressive symptoms during home confinement in relation to previous moments. | 7/8 |
| Benke et al. [28], 2020 | Design: Quantitative cross-sectional Objective: To identify predictors of worse mental health during the COVID-19 pandemic. | n = 4335 Age: >18 years Sex (f/m): 3284/1051 | Generalized Anxiety: GAD-7 Health Anxiety: Short Version of the Whitely Index Depression: PHQ-9 | In total, 31.1% exceeded the cut-off score for a depression diagnosis, 21.2% for anxiety disorder and 29.4% for health anxiety. Women reported more anxiety and depression than men. Being young, low educational level, unemployment, current or previous psychiatric treatment, belonging to a risk group, anguish related to the restriction of social contacts, and a greater perception of change predicted depression and anxiety (p < 0.001). Living alone also contributed to increased anxiety. | 8/8 |
| Chen et al. [29], 2021 | Design: Quantitative cross-sectional Objective: To compare the anxiety levels of confined people with those who were not confined during the second wave of the COVID-19 pandemic. | n = 1837 Age: >18 years Sex (f/m): 1512/325 | Anxiety: STAI | Severe anxiety increased in participants aged between 26 and 39 years, in men, in people with low incomes and in those with a level of education below a bachelor´s degree (p < 0.001). Participants who had a general feeling of good health and were not in quarantine showed less anxiety than those who felt they were in poor health and were in quarantine (p < 0.001). Furthermore, high income was an independent protective factor for anxiety (p = 0.027), and a poor state of health was an independent risk factor (p < 0.001). | 8/8 |
| Dean et al. [30], 2021 | Design: Quantitative cross-sectional Objective: To examine the psychosocial distress during the initial phase of the pandemic in four different societies. | n = 1306 Age: >18 years Sex (f/m): 904/400 | Anxiety: DASS Depression: DASS Stress: DASS | Younger age (β = −0.13; t = −2.98; p = 0.002), greater concern about COVID−19 (β = 0.15; t = 3.01; p = 0.003) and greater feelings of loneliness (β = −0.23; t = 8.20; p < 0.001) predicted a worse psychological outcome, but the magnitude of these effects varied among the four regions. | 8/8 |
| González-Sanguino et al. [31], 2020 | Design: Quantitative cross-sectional Objective: To analyse the psychological impact of the COVID-19 outbreak three weeks after the outbreak of the pandemic and declaration of the state of alarm. | n = 3480 Age: >18 years Sex (f/m): 2610/870 | Generalized anxiety: GAD-7 Depression: PHQ-9 PTSD: PCL-C2 | In total, 18.7% presented depressive symptoms, 21.6% anxiety and 15.8% PTSD. Female sex, previous mental health problems, symptoms associated with the virus or those with an infected close relative were associated with the worst results in the three variables (p < 0.05), and age, economic stability and the information received about the pandemic were negatively correlated with symptoms (p < 0.05). Spiritual well-being was a protective factor for depression and being a student or feelings of loneliness were risk factors (p < 0.001). Low spiritual well-being, feelings of loneliness, being a woman and not enough information predicted higher anxiety (p < 0.001) and post-traumatic stress (p < 0.001). | 8/8 |
| Ferraz-Goularte et al. [32], 2020 | Design: Quantitative cross-sectional Objective: To investigate the prevalence and determinants of psychiatric symptoms during the COVD-19 pandemic. | n = 1996 Age: >18 years Sex (f/m): 1676/320 | Anxiety: PROMIS anxiety v.8ª Depression: PROMIS depression v.8ª PTSD: IES-R | Anxiety (81.9%) and depression (68%) were the most frequent psychiatric symptoms, and 34.2% of the participants reported PTSD. Female sex, longer duration of social distancing measures and previous psychiatric illness were significantly associated with higher levels of stress, depression and anxiety (p < 0.01). Furthermore, young age, low education and/or income were correlated with greater symptoms (p < 0.01). Being single was only associated with greater depression and anxiety (p < 0.01). | 8/8 |
| Hazarika et al. [33], 2021 | Design: Quantitative cross-sectional Objective: To evaluate the psychological state during the initial phase of the confinement produced by COVID-19. | n = 422 Age: >18 years Sex (f/m): 255/167 | Anxiety: DASS-21 Depression: DASS-21 Stress: DASS-21 | In total, 35.5% reported stress, 32% anxiety and 34.7% depression. Single people, students, housewives, people who work in the public sector, people with a history of mental illness and those with lower educational levels were shown to be more likely to experience symptoms of stress, anxiety and depression (p < 0.05). | 6/8 |
| Huang et al. [34], 2020 | Design: Quantitative cross-sectional Objective: To assess the mental health burden during the COVID-19 outbreak and explore possible influencing factors. | n = 7236 Age: >18 years Sex (f/m): 3952/3284 | Generalized anxiety: GAD-7 Depression: CES-D | The overall prevalence of generalized anxiety disorder and depression was 35.1% and 20.1%, respectively. Younger people (<35 years) and those who spent 3 h or more/day thinking about COVID-19 reported a significantly higher prevalence of generalized anxiety disorder and depression (p < 0.05). | 7/8 |
| Lal et al. [35], 2020 | Design: Quantitative cross-sectional Objective: To evaluate the psychological distress caused by the pandemic of the COVID-19 disease. | n = 1000 Age: >18 years Sex (f/m): 427/573 | Generalized anxiety: GAD-7 Depression: PHQ-9 | Women reported more depression (p < 0.001) and anxiety (p = 0.03) than men. In addition, participants between 18 and 30 years of age disclosed greater anxiety (p = 0.001) and depression (p = 0.004). Lower-income individuals, students, healthcare workers and unemployed also showed worse results (p < 0.05). | 6/8 |
| Lee et al. [36], 2021 | Design: Quantitative cross-sectional Objective: To assess mental health and social well-being during the COVID-19 pandemic. | n = 400 Age: >18 years Sex (f/m): 110/287 | Anxiety: DASS Depression: DASS Stress: DASS | Depression was present in 36.75% of the participants, anxiety in 29.5% and stress in 24.5%. The youngest reported feeling more worried, anxious or tense (p = 0.04), while the oldest reported higher levels of stress (p = 0.02). Women reported poorer mental health in general (p = 0.001), except for anxiety, where there were no significant differences between groups. Singles showed greater depression than those married or with a partner (p = 0.03). | 6/8 |
| Lei et al. [37], 2020 | Design: Quantitative cross-sectional Objective: To evaluate and compare the prevalence and associated factors of anxiety and depression during the COVID-19 outbreak. | n = 1593 Age: >18 years Sex (f/m): 976/617 | Anxiety: SAS Depression: SDS | The prevalence of anxiety and depression was 8.3% and 14.6%, respectively. Female gender and age ≤ 30 years old were associated with greater symptoms of depression and anxiety (p < 0.05). Having knowledge about COVID-19 (β = 0.621; p = 0.032), economic losses (β = 0.634; p = 0.001), being divorced or widowed (β = 4.825; p = 0.001), bad self-perceived health (β = −2.762; p < 0.001) and concern about infection (β = 1.62; p < 0.001) predicted more anxiety. Absence of psychological support (β = 1.327; p = 0.043), being divorced or widowed (β = 7.313; p < 0.001), bad self-perceived health (β = −3.109; p < 0.001) and greater concern about infection (β = 1.232; p = 0.006) were associated with depression. | 8/8 |
| Massad et al. [38], 2020 | Design: Quantitative cross-sectional Objective: To evaluate the prevalence of psychological distress related to quarantine and to explore sociodemographic correlations. | n = 5274 Age: >18 years Sex (f/m): 2914/2360 | Anxiety: BAI | The prevalence of mild, moderate and severe anxiety was 21.5%, 10.9% and 6%, respectively. Female gender or the presence of more members in the household were correlated with higher levels of anxiety; old age, a large social network, social support and high income correlated with lower levels. | 8/8 |
| Mazza et al. [39], 2020 | Design: Cross-sectional quantitative Objective: To establish the prevalence of psychiatric symptoms and to identify risk and protective factors for psychological distress. | n = 2766 Age: >18 years Sex (f/m): 1982/784 | Anxiety: DASS-21 Depression: DASS-21 Stress: DASS-21 | In total, 17% reported a high level of depression and 15.4% an extremely high range. Regarding anxiety, 7.2% had a high level, and 11.5% were in the extremely high range. Regarding stress, 14.6% were in the high range, and 12.6% were in an extremely high range. Female sex, having family members with COVID-19, negative affect and detachment were associated with higher levels of depression, anxiety and stress (p < 0.05). Additionally, previous medical problems were associated with higher levels of depression and anxiety, and younger people reported more stress (p < 0.05). | 8/8 |
| Ngoc Cong Duong et al. [40], 2020 | Design: Quantitative cross-sectional Objective: To estimate the prevalence of psychological problems and identify the factors associated with the psychological impact of COVID-19 during the first national blockade. | n = 1412 Age: >18 years Sex (f/m): 532/880 | Anxiety: DASS-21 Depression: DASS-21 Stress: DASS-21 PTSD: IES-R | In total, 23.5% experienced depression, 14.1% anxiety and 22.3% stress. People aged ≥60 years demonstrated lower levels of depression, and unemployed people, students, housewives and people with chronic diseases had a higher risk of depression. Isolated participants were more likely to experience anxiety, and unemployed people or students reported higher levels of stress. | 8/8 |
| Özdin et al. [41], 2020 | Design: Quantitative cross-sectional Objective: To assess the levels of depression, anxiety and anxiety about health during the COVID-19 pandemic and examine the factors that affect them. | n = 343 Age: >18 years Sex (f/m): 169/174 | Anxiety: HADS Health anxiety: HAI Depression: HADS | In total, 23.6% scored above the cut-off point for depression and 45.1% for anxiety. Living in urban areas was associated with higher levels of depression and anxiety. Female gender (β = 0.105; p = 0.047), suffering from a chronic illness (β = 0.160; p = 0.003) and having a previous psychiatric illness (β = 0.176; p = 0.001) were risk factors for predicting health anxiety. | 8/8 |
| Panchuelo-Gómez et al. [42], 2020 | Design: Quantitative longitudinal Objective: To evaluate the temporal evolution of the psychological impact of the crisis and closure of COVID-19. | n = 4724 Age: >18 years | Anxiety: DASS-21 Depression: DASS-21 Stress: DASS-21 PTSD: IES-R | Anxiety, depression and stress levels were significantly higher over time, with a prevalence of 37.22%, 46.42% and 49.66%, respectively. More anxiety and stress were found in younger people, and more depression in single subjects. The frequency of consumption of news about COVID-19 was a factor clearly associated with higher levels of anxiety, depression and stress. | 7/9 |
| Ripon et al. [43], 2020 | Design: Quantitative cross-sectional Objective: To assess the prevalence of depression and PTSD among quarantined people during the COVID-19 outbreak. | n = 5792 Age: >18 years | Depression: CES-D PTSD: IES-R | In total, 85.9% reported depressive symptoms and 81.8% PTSD, of which 20% had a probable diagnosis of PTSD, and 24.3% demonstrated PTSD as a clinical problem. Depression and PTSD were more frequent in people aged 31–45 years, with low income, with higher education, single and in-home quarantine (p < 0.05). Women showed higher levels of depression, while PTSD was more frequent in men (p < 0.05). | 6/8 |
| Rodríguez-Rey et al. [44], 2020 | Design: Cross-sectional quantitative Objective: To explore the mental health during the early stages of the COVID-19 outbreak. | n = 3055 Age: >18 years Sex (f/m/o): 2293/744/18 | Anxiety: DASS-21 Depression: DASS-21 Stress: DASS-21 PTSD: IES-R | In total, 36% of the participants reported moderate to severe psychological impact, 25% mild to severe anxiety levels, 41% depressive symptoms, and 41% felt stressed. Women, young people and those who lost their jobs during the pandemic had worse results (p < 0.05). A higher self-perceived health was associated with less anxiety and depression (p < 0.001), and doing leisure activities during the day reduced stress, anxiety and depression (p < 0.001). | 7/8 |
| Schweda et al. [45], 2020 | Design: Quantitative cross-sectional Objective: To investigate the psychological reactions in response to real or perceived threats of SARS-Cov-2 infection. | n = 15308 Age: >18 years Sex (f/m/o): 10824/4433/51 | Generalized anxiety: GAD-7 Depression: PHQ-2 | Women, young people, those residing in rural areas, people with previous psychiatric illness and who did not trust government actions against COVID-19 reported higher levels of anxiety (p < 0.001). | 8/8 |
| Sherman et al. [46], 2020 | Design: Quantitative cross-sectional Objective: To examine some of the burdens of the pandemic, the prevalence of mental health problems and the risk factors for psychosocial morbidity. | n = 591 Age: >18 years Sex (f/m): 458/133 | Generalized anxiety: GAD-7 Depression: PHQ-9 PTSD: PCL-5 | Young people, women and participants with lower incomes were more likely to have depression and anxiety (p < 0.005), and people with a lower educational level suffered from depressive symptoms (p = 0.005). Depression was associated with previous mental illness (p < 0.0001), not being married (p = 0.008) and a greater alteration in daily life (p < 0.001). Higher levels of anxiety were linked to younger age (p < 0.005), previous mental illness (p < 0.0001) and greater disruption in daily life (p < 0.001). PTSD was associated with previous mental illness (p < 0.001) and greater disruption in daily life (p < 0.0002). | 8/8 |
| Shevlin et al. [47], 2020 | Design: Quantitative cross-sectional Objective: To investigate the prevalence of symptoms of anxiety, generalized anxiety, depression and trauma related to COVID-19 during an early phase of the pandemic and to estimate associations with variables. | n = 2025 Age: >18 years Sex (f/m/o): 1047/972/6 | Generalized anxiety: GAD-7 Depression: PHQ-9 PTSD: ITQ | In total, 22.1% had depression symptoms, 21.6% anxiety and 16.79% PTSD. In the case of PTSD, there was a significant gender difference, with a higher prevalence in men (p < 0.01), the same situation that was observed with anxiety, but in this case with women (p < 0.01). Symptoms of anxiety, depression and PTSD were predicted by a young age, children at home and elevated risk perception. Low or loss of income and previous health problems also predicted anxiety and depression. | 8/8 |
| Smith et al. [48], 2020 | Design: Cross-sectional quantitative Objective: To assess the impact of social distancing during COVID-19 on mental health. | n = 932 Age: >18 years Sex (f/m/o): 590/334/8 | Anxiety: BAI Depression: BDI | The prevalence of poor mental health due to the pandemic was 36.8%. Female sex, aged 25–34 years, a lower annual income, smoke and suffering from physical multimorbidity were associated with higher levels of anxiety and depression (p < 0.05). | 8/8 |
| Wang et al. [49], 2020 | Design: Cross-sectional quantitative Objective: To establish the prevalence of psychiatric symptoms and to identify risk and protector factors of psychological stress. | n = 1210 Age: >18 years Sex (f/m): 814/396 | Anxiety: DASS-21 Depression: DASS-21 Stress: DASS-21 PTSD: IES-R | In total, 16.5% showed moderate to severe depressive symptoms, 28.8% moderate to severe anxiety symptoms and 8.1% moderate to severe stress. Men had less PTSD but greater symptoms of anxiety, depression and stress (p < 0.05), and students demonstrated more PTSD, stress and anxiety (p < 0.05). Contact with an infected person or material was shown to be a risk factor for anxiety and depression (p < 0.01). People with lower educational levels had greater depressive symptoms (p < 0.01), and dissatisfaction with the amount of information received was associated with greater stress (p < 0.05). | 8/8 |
| Wang et al. [50], 2020 | Design: Quantitative longitudinal Objective: To assess the temporary psychological impact and adverse mental health status during the initial and peak outbreak of the COVID-19 pandemic and identify risk and protective factors. | n = 1738 Age: >18 years | Anxiety: DASS-21 Depression: DASS-21 Stress: DASS-21 PTSD: IES-R | PTSD increased over the time (p <0.01), but not the levels of anxiety, depression and stress (p > 0.05). Younger participants demonstrated higher levels of PTSD (B = 0.77, t = 2.28, p <0.05) and subjects who lived in a household with 3–5 people (B = 1.32, t = 2.04, p < 0.05) and more than 6 people (B = 1.44, t = 2.20, p <0.05) reported more PTSD compared to people who lived alone. Radio broadcast of information about COVID-19 was associated with higher anxiety and depression scores (p < 0.05). | 7/9 |
| Study | JBI | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 |
|---|---|---|---|---|---|---|---|---|---|---|
| Panchuelo-Gómez et al. [42] | 7/9 | + | + | − | − | + | + | + | + | + |
| Wang et al. [50] | 7/9 | + | + | − | − | + | + | + | + | + |
| Study | JBI | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 |
|---|---|---|---|---|---|---|---|---|---|
| Ahmed et al. [25] | 6/8 | + | + | + | + | − | − | + | + |
| Alkhamees et al. [26] | 8/8 | + | + | + | + | + | + | + | + |
| Ammar et al. [27] | 7/8 | + | + | + | + | + | − | + | + |
| Benke et al. [28] | 8/8 | + | + | + | + | + | + | + | + |
| Chen et al. [29] | 8/8 | + | + | + | + | + | + | + | + |
| Dean et al. [30] | 8/8 | + | + | + | + | + | + | + | + |
| González-Sanguino et al. [31] | 8/8 | + | + | + | + | + | + | + | + |
| Goularte et al. [32] | 8/8 | + | + | + | + | + | + | + | + |
| Hazarika et al. [33] | 6/8 | + | + | + | + | − | − | + | + |
| Huang et al. [34] | 7/8 | + | + | + | + | + | − | + | + |
| Lal et al. [35] | 6/8 | + | + | + | + | − | − | + | + |
| Lee et al. [36] | 6/8 | + | + | + | + | − | − | + | + |
| Lei et al. [37] | 8/8 | + | + | + | + | + | + | + | + |
| Massad et al. [38] | 8/8 | + | + | + | + | + | + | + | + |
| Mazza et al. [39] | 8/8 | + | + | + | + | + | + | + | + |
| Ngoc Cong Duong et al. [40] | 8/8 | + | + | + | + | + | + | + | + |
| Özdin et al. [41] | 8/8 | + | + | + | + | + | + | + | + |
| Ripon et al. [43] | 6/8 | + | + | + | + | − | − | + | + |
| Rodríguez-Rey et al. [44] | 7/8 | + | + | + | + | + | − | + | + |
| Schweda et al. [45] | 8/8 | + | + | + | + | + | + | + | + |
| Sherman et al. [46] | 8/8 | + | + | + | + | + | + | + | + |
| Shevlin et al. [47] | 8/8 | + | + | + | + | + | + | + | + |
| Smith et al. [48] | 8/8 | + | + | + | + | + | + | + | + |
| Wang et al. [49] | 8/8 | + | + | + | + | + | + | + | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Fernández, P.; González-Santos, J.; Santamaría-Peláez, M.; Soto-Cámara, R.; Sánchez-González, E.; González-Bernal, J.J. Psychological Effects of Home Confinement and Social Distancing Derived from COVID-19 in the General Population—A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6528. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126528
Rodríguez-Fernández P, González-Santos J, Santamaría-Peláez M, Soto-Cámara R, Sánchez-González E, González-Bernal JJ. Psychological Effects of Home Confinement and Social Distancing Derived from COVID-19 in the General Population—A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(12):6528. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126528
Chicago/Turabian StyleRodríguez-Fernández, Paula, Josefa González-Santos, Mirian Santamaría-Peláez, Raúl Soto-Cámara, Esteban Sánchez-González, and Jerónimo J. González-Bernal. 2021. "Psychological Effects of Home Confinement and Social Distancing Derived from COVID-19 in the General Population—A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 12: 6528. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126528