
Association between Occupational Dysfunction and Social Isolation in Japanese Older Adults: A Cross-Sectional Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
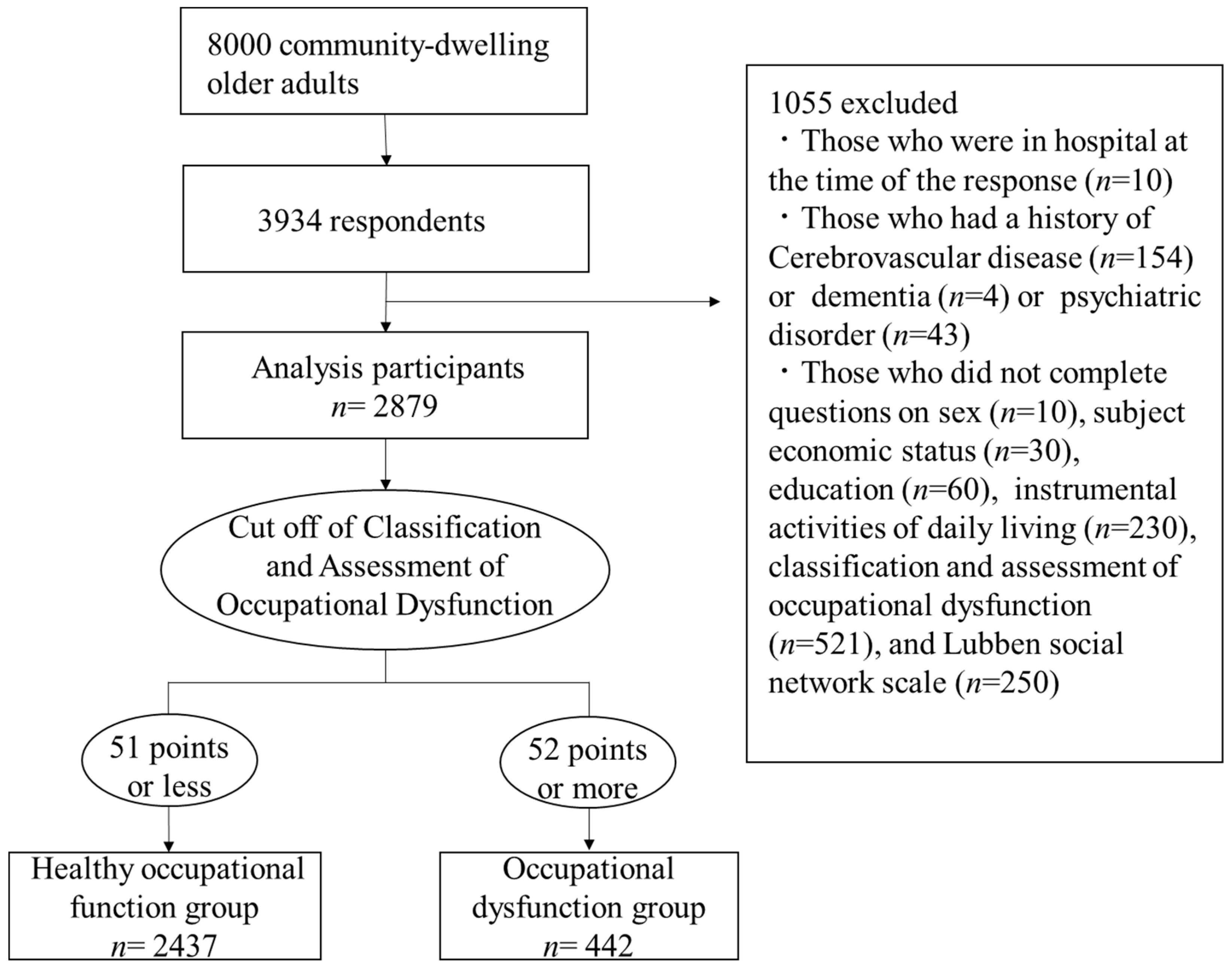
2.1. Participants and Data Collection
2.2. Measurement Variables
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health, Labour and Welfare. Summary Report of Comprehensive Survey of Living Conditions 2019. 2019. Available online: https://www.mhlw.go.jp/english/database/db-hss/dl/report_gaikyo_2019.pdf (accessed on 5 June 2021).
- Nicholson, N.R., Jr. Social isolation in older adults: An evolutionary concept Analysis. J. Adv. Nurs. 2009, 65, 1342–1352. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.; Kondo, K.; Ojima, T.; Hirai, H.; The JAGES Group. Criteria for social isolation based on associations with health indicators among older people. A 10-year follow-up of the Aichi Gerontological Evaluation Study. Jpn. J. Public Health 2015, 62, 95–105. [Google Scholar] [CrossRef]
- Courtin, E.; Knapp, M. Social isolation, loneliness and health in old age: A scoping review. Health Soc. Care Community 2017, 25, 799–812. [Google Scholar] [CrossRef]
- Kuiper, J.S.; Zuidersma, M.; Oude Voshaar, R.C.; Zuidema, S.U.; van den Heuvel, E.R.; Stolk, R.P.; Smidt, N. Social relationships and risk of dementia: A systematic review and meta-analysis of longitudinal cohort studies. Ageing Res. Rev. 2015, 22, 39–57. [Google Scholar] [CrossRef] [PubMed]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspect. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef] [Green Version]
- Steptoe, A.; Shankar, A.; Demakakos, P.; Wardle, J. Social isolation, loneliness, and all-cause mortality in older men and women. Proc. Natl. Acad. Sci. USA 2013, 110, 5797–5801. [Google Scholar] [CrossRef] [Green Version]
- Miyake, Y.; Eguchi, E.; Ito, H.; Nakamura, K.; Ito, T.; Nagaoka, K.; Ogino, N.; Ogino, K. Association between occupational dysfunction and metabolic syndrome in community-dwelling Japanese adults in a cross-sectional study: Ibara Study. Int. J. Environ. Res. Public Health 2018, 15, 2575. [Google Scholar] [CrossRef] [Green Version]
- Kielhofner, G.; Braveman, B.; Baron, K.; Fisher, G.; Hammel, J.; Littleton, M. The model of human occupation: Understanding the worker who is injured or disabled. Work 1999, 12, 37–45. [Google Scholar]
- Teraoka, M.; Kyougoku, M. Development of the final version of the Classification and Assessment of Occupational Dysfunction Scale. PLoS ONE 2015, 10, e0134695. [Google Scholar] [CrossRef]
- Townsend, E.; Wilcock, A.A. Occupational justice and client-centred practice: A dialogue in progress. Can. J. Occup. Ther. 2004, 71, 75–87. [Google Scholar] [CrossRef]
- Anaby, D.; Jarus, T.; Backman, C.L.; Zumbo, B.D. The role of occupational characteristics and occupational imbalance in explaining well-being. Appl. Res. Qual. Life 2010, 5, 81–104. [Google Scholar] [CrossRef]
- Bryant, W.; Craik, C.; McKay, E.A. Living in a glasshouse: Exploring occupational alienation. Can. J. Occup. Ther. 2004, 71, 282–289. [Google Scholar] [CrossRef] [Green Version]
- Whiteford, G. Occupational deprivation: Global challenge in the new millennium. Br. J. Occup. Ther. 2000, 63, 200–204. [Google Scholar] [CrossRef]
- Teraoka, M.; Kyougoku, M. Analysis of structural relationship among the occupational dysfunction on the psychological problem in healthcare workers: A study using structural equation modeling. PeerJ 2015, 19, e1389. [Google Scholar] [CrossRef] [Green Version]
- Morohoshi, N.; Kyougoku, M. Analysis of structural relationships among occupational challenge, occupational participation, occupational dysfunction, depression, and health-related qol in community dwelling elderly with physical disabilities. Jpn. Occup. Ther. Res. 2019, 38, 294–303. [Google Scholar]
- Ge, L.; Yap, C.W.; Ong, R.; Heng, B.H. Social isolation, loneliness and their relationships with depressive symptoms: A population-based study. PLoS ONE 2017, 12, e0182145. [Google Scholar] [CrossRef] [PubMed]
- Hawton, A.; Green, C.; Dickens, A.P.; Richards, S.H.; Taylor, R.S.; Edwards, R.; Greaves, C.J.; Campbell, J.L. The impact of social isolation on the health status and health-related quality of life of older people. Qual. Life Res. 2011, 20, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Matthews, T.; Danese, A.; Wertz, J.; Odgers, C.L.; Ambler, A.; Moffitt, T.E.; Arseneault, L. Social isolation, loneliness and depression in young adulthood: A behavioural genetic analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 339–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papageorgiou, N.; Marquis, R.; Dare, J.; Batten, R. Occupational Therapy and Occupational Participation in Community Dwelling Older Adults: A Review of the Evidence. Phys. Occup. Ther. Geriatr. 2016, 34, 21–42. [Google Scholar] [CrossRef]
- Government of Kasama City. Statistical Information of Kasama City. 2018. Available online: https://www.city.kasama.lg.jp/data/doc/1547708244_doc_81_0.pdf (accessed on 16 April 2021).
- Furukawa, T.A.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y.; Tachimori, H.; Iwata, N.; Uda, H.; Nakane, H.; et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res. 2008, 17, 152–158. [Google Scholar] [CrossRef]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Tomioka, K.; Kurumatani, N.; Hosoi, H. Association between social participation and 3-year change in instrumental activities of daily living in community-dwelling elderly adults. J. Am. Geriatr. Soc. 2017, 65, 107–113. [Google Scholar] [CrossRef]
- Tomioka, K.; Kurumatani, N.; Saeki, K. The differential effects of type and frequency of social participation on IADL declines of older people. PLoS ONE 2018, 13, e0207426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koyano, W.; Shibata, H.; Nakazato, K.; Haga, H.; Suyama, Y. Measurement of competence in the elderly living at home: Development of an index of competence. Nippon Koshu Eisei Zasshi 1987, 34, 109–114. [Google Scholar]
- Lubben, J.; Blozik, E.; Gillmann, G.; Iliffe, S.; von Renteln Kruse, W.; Beck, J.C.; Stuck, A.E. Performance of an abbreviated version of the lubben social network scale among three european community-dwelling older adult populations. Gerontologist 2006, 46, 503–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsson-Lund, M.; Nyman, A. Participation and occupation in occupational therapy models of practice: A discussion of possibilities and challenges. Scand. J. Occup. Ther. 2017, 24, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Collins, T.; Davys, D.; Martin, R.; Russell, R.; Kenney, C. Occupational therapy, loneliness and social isolation: A thematic review of the literature. Int. J. Ther. Rehabil. 2020, 27, 1–23. [Google Scholar] [CrossRef]
- Giorgi, G.; Lecca, L.I.; Leon-Perez, J.M.; Pignata, S.; Topa, G.; Mucci, N. Emerging Issues in Occupational Disease: Mental Health in the Aging Working Population and Cognitive Impairment—A Narrative Review. Biomed. Res. Int. 2020, 2020, 1742123. [Google Scholar] [CrossRef]
- American Occupational Therapy Association [AOTA]. Occupational therapy practice framework: Domain and process (3rd ed.). Am. J. Occup. Ther. 2014, 68, S1–S48. [Google Scholar] [CrossRef]
- Stav, W.B.; Hallenen, T.; Lane, J.; Arbesman, M. Systematic review of occupational engagement and health outcomes among community-dwelling older adults. Am. J. Occup. Ther. 2012, 66, 301–310. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristic | Healthy Occupational Function Group (n = 2437) | Occupational Dysfunction Group (n = 442) | p-Value |
|---|---|---|---|
| %(n) | %(n) | ||
| Age (years), Mean ± SD | 72.6 ± 5.2 | 72.7 ± 5.6 | 0.795 |
| Female, %(n) | 49.3 (1202) | 46.2 (204) | 0.220 |
| Household (living alone), %(n) | 12.7 (310) | 12.7 (56) | 0.976 |
| Educational background (≧high school), %(n) | 84.1 (2030) | 77.8 (339) | 0.001 |
| Subjective economic status (poor), %(n) | 17.0 (413) | 31.9 (553) | p < 0.001 |
| IADL ability (disability), %(n) | 7.4 (181) | 7.9 (35) | 0.718 |
| K6 (score), Mean ± SD | 2.8 ± 3.0 | 6.2 ± 4.0 | p < 0.001 |
| Social isolation, %(n) | 18.4 (448) | 31.5 (139) | p < 0.001 |
| CAOD (score), Mean ± SD | 30.0 ± 10.5 | 60.6 ± 7.1 | p < 0.001 |
| Occupational imbalance (score), Mean ± SD | 7.5 ± 3.8 | 14.8 ± 3.8 | p < 0.001 |
| Occupational deprivation (score), Mean ± SD | 6.2 ± 3.2 | 12.8 ± 2.7 | p < 0.001 |
| Occupational alienation (score), Mean ± SD | 6.4 ± 3.4 | 12.1 ± 2.8 | p < 0.001 |
| Occupational marginalization (score), Mean ± SD | 9.9 ± 3.8 | 20.8 ± 3.8 | p < 0.001 |
| Crude Model | Adjusted Model | |||||
|---|---|---|---|---|---|---|
| OR | 95%CI | p-Value | OR | 95%CI | p-Value | |
| Healthy occupational function group | Ref. | Ref. | ||||
| Occupational dysfunction group | 2.04 | 1.63–2.55 | p < 0.001 | 1.51 | 1.17–1.94 | 0.001 |
| Occupational Dysfunction Type | Crude Model | Adjusted Model | ||||
|---|---|---|---|---|---|---|
| OR | 95%CI | p-Value | OR | 95%CI | p-Value | |
| Occupational imbalance | 1.01 | 0.99–1.03 | 0.248 | 0.93 | 0.90–0.96 | p < 0.001 |
| Occupational deprivation | 1.10 | 1.08–1.13 | p < 0.001 | 1.03 | 0.99–1.06 | 0.134 |
| Occupational alienation | 1.15 | 1.12–1.78 | p < 0.001 | 1.10 | 1.06–1.13 | p < 0.001 |
| Occupational marginalization | 1.07 | 1.05–1.09 | p < 0.001 | 1.04 | 1.01–1.07 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujii, K.; Fujii, Y.; Kubo, Y.; Tateoka, K.; Liu, J.; Nagata, K.; Wakayama, S.; Okura, T. Association between Occupational Dysfunction and Social Isolation in Japanese Older Adults: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 6648. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126648
Fujii K, Fujii Y, Kubo Y, Tateoka K, Liu J, Nagata K, Wakayama S, Okura T. Association between Occupational Dysfunction and Social Isolation in Japanese Older Adults: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(12):6648. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126648
Chicago/Turabian StyleFujii, Keisuke, Yuya Fujii, Yuta Kubo, Korin Tateoka, Jue Liu, Koki Nagata, Shuichi Wakayama, and Tomohiro Okura. 2021. "Association between Occupational Dysfunction and Social Isolation in Japanese Older Adults: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 12: 6648. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126648