
Clinical and Therapeutic Characteristics of Cancer Patients in the Southern Region of Saudi Arabia: A Cross-Sectional Study

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Study Population
2.2. Statistical Analysis
2.3. Ethical Considerations
3. Results
3.1. Patients’ Baseline Characteristics
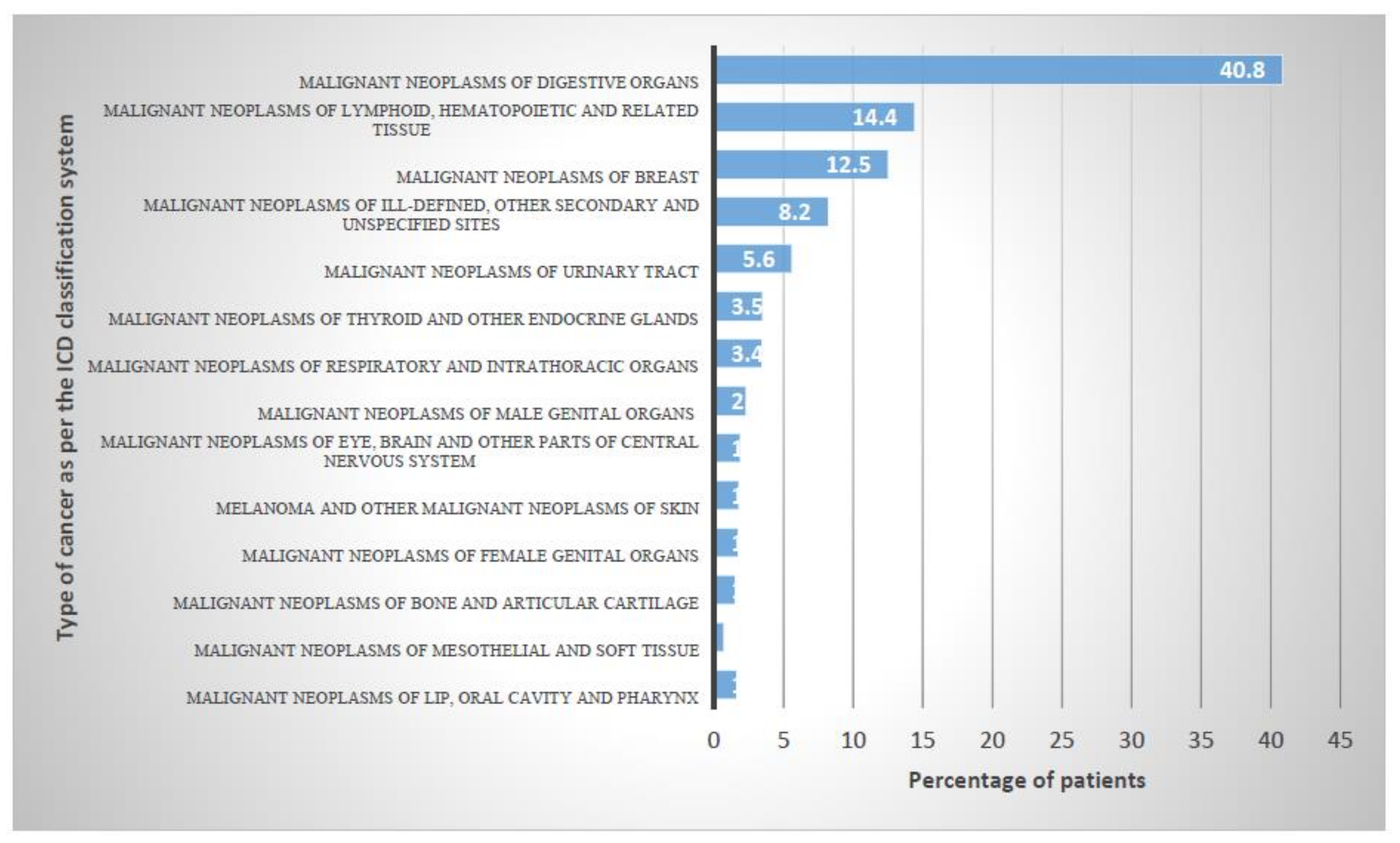
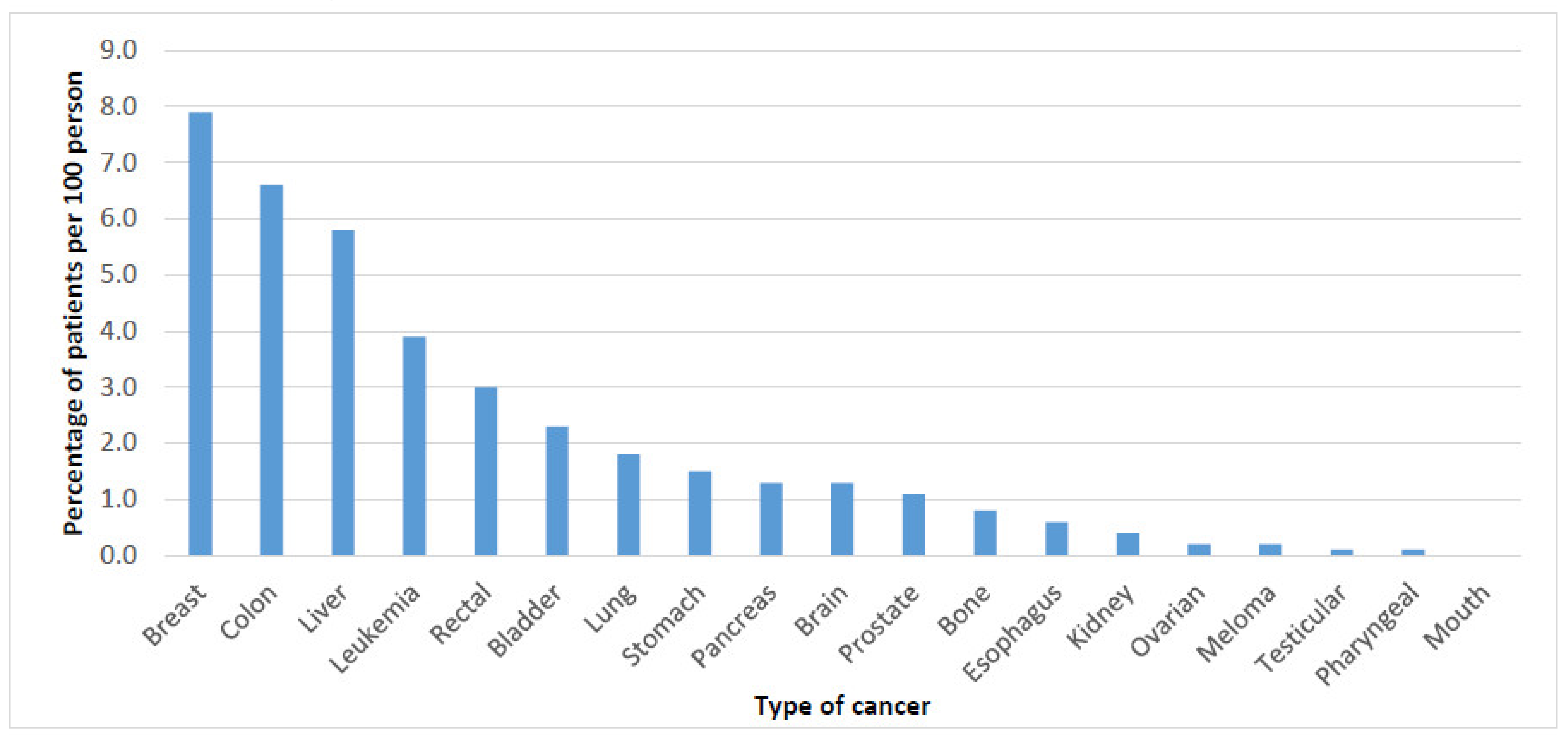
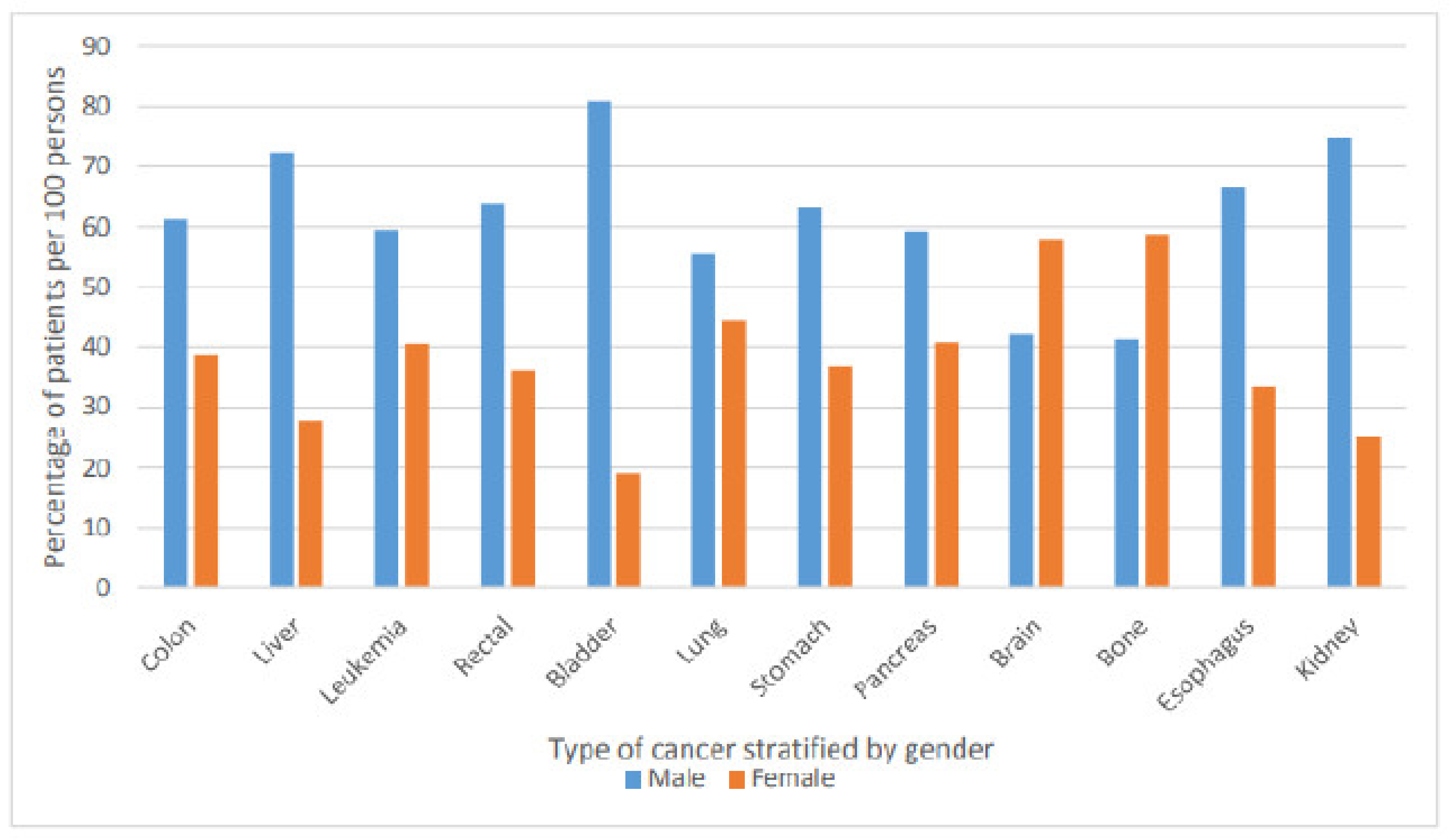
3.2. Epidemiology of Cancer
3.3. Cancer-Related Death and ICU Admission Risk Factors
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bazarbashi, S.; Al Eid, H.; Minguet, J. Cancer Incidence in Saudi Arabia: 2012 Data from the Saudi Cancer Registry. Asian Pac. J. Cancer Prev. 2017, 18, 2437–2444. [Google Scholar] [CrossRef] [PubMed]
- Abdelhadi, M. Breast cancer awareness campaign: Will it make a difference? J. Fam. Community Med. 2006, 13, 115–118. [Google Scholar]
- Ravichandran, K.; Al-Hamdan, N.A.; Mohamed, G. Knowledge, attitude, and behavior among Saudis toward cancer preventive practice. J. Fam. Community Med. 2011, 18, 135–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radi, S.M. Breast Cancer awareness among Saudi females in Jeddah. Asian Pac. J. Cancer Prev. 2013, 14, 4307–4312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Midhet, F.M.; Sharaf, F.K. Impact of health education on lifestyles in central Saudi Arabia. Saudi. Med. J. 2011, 32, 71–76. [Google Scholar]
- National Cancer Institute. Risk Factors for Cancer 23 December 2020, 13 May 2015, 2020. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk (accessed on 27 October 2020).
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef] [PubMed]
- The Geographer. Jordan–Saudi Arabia Boundary; Office of the Geographer Bureau of Intelligence and Research: Washington, DC, USA, 1965.
- Hussain, A.; Lafta, R. Cancer Trends in Iraq 2000–2016. Oman Med. J. 2021, 36, e219. [Google Scholar] [CrossRef]
- Accone, F.; Artigas, A.; Sprung, C.; Moreno, R.; Sakr, Y.; Vincent, J. Characteristics and outcomes of cancer patients in European ICUs. Crit. Care 2009, 13, 1–10. [Google Scholar]
- World Health Organization. International Agency for Research on Cancer: Saudi Arabia Fact Sheet. Available online: https://gco.iarc.fr/today/data/factsheets/populations/682-saudi-arabia-fact-sheets.pdf (accessed on 2 November 2020).
- Althubiti, M.A.; Nour Eldein, M.M. Trends in the incidence and mortality of cancer in Saudi Arabia. Saudi. Med. J. 2018, 39, 1259–1262. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. Tobacco Smoke and Involuntary Smoking. IARC Monogr. Eval. Carcinog. Risks Hum. 2004, 83, 1–1438. [Google Scholar]
- Bassiony, M. Smoking in Saudi Arabia. Saudi Med. J. 2009, 30, 876–881. [Google Scholar]
- Salama, R. Challenges facing smokers in Saudi Arabia. Int. J. Health Sci. 2012, 6, 5–6. [Google Scholar] [CrossRef] [PubMed]
- Jazieh, A.; Da’ar, O.; Alkaiyat, M.; Zaatreh, Y.; Saad, A.; Bustami, R.; Alrujaib, M.; Alkattan, K. Cancer Incidence Trends from 1999 to 2015 and Contributions of Various Cancer Types to the Overall Burden: Projections to 2030 and Extrapolation of Economic Burden in Saudi Arabia. Cancer Manag. Res. 2019, 11, 9665–9674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alessy, S.A.; Davies, E.A.; Jazieh, A.R. Cancer care during the COVID-19 pandemic: A perspective from Saudi Arabia. Ecancermedicalscience 2020, 14, 1076. [Google Scholar] [CrossRef] [PubMed]
- Khoja, T.; Rawaf, S.; Qidwai, W.; Rawaf, D.; Nanji, K.; Hamad, A. Health Care in Gulf Cooperation Council Countries: A Review of Challenges and Opportunities. Cureus 2017, 9, e1586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Guide to Cancer Early Diagnosis; World Health Organization: Geneva, Switzerland, 2017; p. 39. [Google Scholar]
- Alshehri, B.M. The changing patterns of liver cancer in Saudi Arabia over a 22-year period. Int. J. Res. Med Sci. 2020, 8. [Google Scholar] [CrossRef]
- Abdo, A.A.; Sanai, F.M.; Al-Faleh, F.Z. Epidemiology of viral hepatitis in Saudi Arabia: Are we off the hook? Saudi. J. Gastroenterol. 2012, 18, 349–357. [Google Scholar] [CrossRef]
- Ayoola, A.; Tobaigy, M.; Gadour, M.; Ahmad, B.; Hamza, M.; Ageel, A. The decline of hepatitis B viral infection in South-Western Saudi Arabia. Saudi Med. J. 2003, 24, 991–995. [Google Scholar]
- Al-Othaimeen, A.; Al-Nozha, M.; Osman, A. Obesity: An emerging problem in Saudi Arabia. Analysis of data from the National Nutrition Survey. East. Mediterr. Health J. 2007, 13, 441–448. [Google Scholar]
- Bebe, F.N.; Hu, S.; Brown, T.L.; Tulp, O.L. Role, Extent, and Impact of Comorbidity on Prognosis and Survival in Advanced Metastatic Melanoma: A Review. J. Clin. Aesthet. Dermatol. 2019, 12, 16–23. [Google Scholar]
- Sogaard, M.; Thomsen, R.W.; Bossen, K.S.; Sorensen, H.T.; Norgaard, M. The impact of comorbidity on cancer survival: A review. Clin. Epidemiol. 2013, 5, 3–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Extermann, M. Interaction between comorbidity and cancer. Cancer Control. 2007, 14, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Read, W.L.; Tierney, R.M.; Page, N.C.; Costas, I.; Govindan, R.; Spitznagel, E.L.; Piccirillo, J.F. Differential prognostic impact of comorbidity. J. Clin. Oncol. 2004, 22, 3099–3103. [Google Scholar] [CrossRef]
- Kennedy, G.D.; Rajamanickam, V.; O’Connor, E.S.; Loconte, N.K.; Foley, E.F.; Leverson, G.; Heise, C.P. Optimizing surgical care of colon cancer in the older adult population. Ann. Surg. 2011, 253, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Rueth, N.M.; Parsons, H.M.; Habermann, E.B.; Groth, S.S.; Virnig, B.A.; Tuttle, T.M.; Andrade, R.S.; Maddaus, M.A.; D’Cunha, J. Surgical treatment of lung cancer: Predicting postoperative morbidity in the elderly population. J. Thorac. Cardiovasc. Surg. 2012, 143, 1314–1323. [Google Scholar] [CrossRef] [Green Version]
- Morris, E.J.; Taylor, E.F.; Thomas, J.D.; Quirke, P.; Finan, P.J.; Coleman, M.P.; Rachet, B.; Forman, D. Thirty-day postoperative mortality after colorectal cancer surgery in England. Gut 2011, 60, 806–813. [Google Scholar] [CrossRef] [Green Version]
- Bradley, C.; Given, C.; Dahman, B.; Fitzgerald, T. Adjuvant chemotherapy after resection in elderly Medicare and Medicaid patients with colon cancer. Arch. Intern. Med. 2008, 168, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Gray, S.W.; Landrum, M.B.; Lamont, E.B.; McNeil, B.J.; Jaklitsch, M.T.; Keating, N.L. Improved outcomes associated with higher surgery rates for older patients with early stage nonsmall cell lung cancer. Cancer 2012, 118, 1404–1411. [Google Scholar] [CrossRef] [Green Version]
- Gross, C.; Guo, Z.; McAvay, G.; Allore, H.; Young, M.; Tinetti, M. Multimorbidity and survival in older persons with colorectal cancer. J. Am. Geriatr. Soc. 2006, 54, 1898–1904. [Google Scholar] [CrossRef]
- Luo, R.; Giordano, S.; Freeman, J.; Zhang, D.; Goodwin, J. Referral to medical oncology: A crucial step in the treatment of older patients with stage III colon cancer. Oncologist 2006, 11, 1025–1033. [Google Scholar] [CrossRef] [Green Version]
- Van Steenbergen, L.N.; Rutten, H.J.T.; Creemers, G.J.; Pruijt, J.F.M.; Coebergh, J.W.W.; Lemmens, V. Large age and hospital-dependent variation in administration of adjuvant chemotherapy for stage III colon cancer in southern Netherlands. Ann. Oncol. 2010, 21, 1273–1278. [Google Scholar] [CrossRef] [PubMed]
- Pasetto, L.; Falci, C.; Basso, U.; Gasparini, G.; D’Andrea, M.; Bonginelli, P.; Bajetta, E.; Platania, M.; Alabiso, O.; Miraglia, S.; et al. Adjuvant treatment for elderly patients with colon cancer. An observational study. Anticancer Res. 2008, 28, 2513–2518. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Overall (n = 2038) | Men (n = 1038) | Women (n = 1000) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Age at diagnosis (mean (SD)) (years) | 60.9 (19.0) | 62.0 (20.0) | 59.7 (17.7) | 0.007 | |||
| Demographic variable | Frequency | Percentage | Frequency | Percentage | Frequency | Percentage | |
| Gender | |||||||
| Men | 1038 | 50.9 | |||||
| Marital status | |||||||
| Single | 1365 | 67.0 | 612 | 59.0 | 753 | 75.3 | 0.000 |
| Married | 605 | 29.7 | 376 | 36.2 | 229 | 22.9 | |
| Divorced | 1 | 0.0 | 1 | 0.1 | 0 | 0 | |
| Widowed | 67 | 3.3 | 49 | 4.7 | 18 | 1.8 | |
| Income category | |||||||
| Low | 133 | 6.5 | 59 | 5.7 | 74 | 7.4 | 0.000 |
| Middle | 481 | 23.6 | 205 | 19.7 | 276 | 27.6 | |
| High | 1424 | 69.9 | 774 | 74.6 | 650 | 65.0 | |
| Employment status | |||||||
| Student | 27 | 1.3 | 16 | 1.5 | 11 | 1.1 | 0.000 |
| Unemployed | 368 | 18.1 | 128 | 12.3 | 240 | 24.0 | |
| Employed | 1594 | 78.2 | 874 | 84.2 | 720 | 72.0 | |
| Retired | 49 | 2.4 | 20 | 1.9 | 29 | 2.9 | |
| Nationality | |||||||
| Saudi | 874 | 42.9 | 432 | 41.6 | 442 | 44.2 | 0.129 |
| Non-Saudi | 1164 | 57.1 | 606 | 58.4 | 558 | 55.8 | |
| Previous surgery | |||||||
| Yes | 1425 | 69.9 | 770 | 74.2 | 655 | 65.5 | 0.000 |
| Smoking history | |||||||
| Yes | 1304 | 64.0 | 693 | 66.8 | 611 | 61.1 | 0.004 |
| Comorbidities | |||||||
| Dyslipidemia | 333 | 16.3 | 177 | 17.1 | 156 | 15.6 | 0.204 |
| Diabetes mellitus | 299 | 14.7 | 163 | 15.7 | 136 | 13.6 | 0.100 |
| Hypertension | 280 | 13.7 | 145 | 14.0 | 135 | 13.5 | 0.741 |
| Neuropathy | 180 | 8.8 | 93 | 9.0 | 87 | 8.7 | 0.079 |
| Heart diseases | 85 | 4.2 | 45 | 4.3 | 40 | 4.0 | 0.235 |
| Liver diseases | 59 | 2.9 | 27 | 2.6 | 32 | 3.2 | 0.121 |
| Thyroid disorders | 34 | 1.7 | 24 | 23.1 | 10 | 1.0 | 0.007 |
| Asthma | 26 | 1.3 | 15 | 1.4 | 11 | 1.1 | 0.275 |
| Epilepsy | 17 | 0.8 | 7 | 0.7 | 10 | 1.0 | 0.024 |
| Arthritis | 15 | 0.7 | 8 | 0.8 | 7 | 0.7 | 0.830 |
| Tuberculosis | 7 | 0.3 | 3 | 0.3 | 4 | 0.4 | 0.210 |
| Depression/Anxiety | 5 | 0.2 | 1 | 0.0 | 4 | 0.4 | 0.030 |
| Nephropathy | 3 | 0.1 | 2 | 0.2 | 1 | 0.1 | 0.176 |
| GERD/Acid reflux diseases | 3 | 0.1 | 1 | 0.1 | 2 | 0.2 | 0.543 |
| Eye disorders | 2 | 0.1 | 2 | 0.2 | 0 | 0 | 0.317 |
| Drug use history | |||||||
| Statin | 613 | 30.1 | 296 | 28.5 | 317 | 31.7 | 0.064 |
| Inhaled corticosteroid | 258 | 12.7 | 99 | 9.5 | 159 | 15.9 | 0.000 |
| Heparin | 210 | 10.3 | 111 | 10.7 | 99 | 9.9 | 0.303 |
| Neuropathy treatment | 180 | 8.8 | 106 | 10.2 | 74 | 7.4 | 0.015 |
| B-Blocker | 179 | 8.8 | 87 | 8.4 | 92 | 9.2 | 0.283 |
| Antipsychotic | 163 | 8.0 | 92 | 8.9 | 71 | 7.1 | 0.083 |
| Angiotensin receptor blocker | 154 | 7.6 | 86 | 8.3 | 68 | 6.8 | 0.118 |
| Diuretic | 141 | 6.9 | 59 | 5.7 | 82 | 8.2 | 0.016 |
| Antidepressant | 139 | 6.8 | 67 | 6.5 | 72 | 7.2 | 0.281 |
| Insulin | 132 | 6.5 | 55 | 5.3 | 77 | 7.7 | 0.017 |
| Nitrate | 128 | 6.3 | 70 | 6.7 | 58 | 5.8 | 0.216 |
| Angiotensin-converting enzyme | 95 | 4.7 | 47 | 4.5 | 48 | 4.8 | 0.426 |
| Antiplatelet | 87 | 4.3 | 33 | 3.2 | 54 | 5.4 | 0.009 |
| Corticosteroid | 78 | 3.8 | 46 | 4.4 | 32 | 3.2 | 0.091 |
| Ulcer treatment | 58 | 2.8 | 23 | 2.2 | 35 | 3.5 | 0.053 |
| Anticoagulant (warfarin) | 50 | 2.5 | 29 | 2.8 | 21 | 2.1 | 0.193 |
| Aspirin | 46 | 2.3 | 30 | 2.9 | 16 | 1.6 | 0.034 |
| Oral antidiabetic | 43 | 2.1 | 24 | 2.3 | 19 | 1.9 | 0.311 |
| Anxiolytic | 42 | 2.1 | 11 | 1.1 | 31 | 3.1 | 0.001 |
| Anticonvulsant | 16 | 0.8 | 5 | 0.5 | 11 | 1.1 | 0.091 |
| Calcium channel blockers | 3 | 0.1 | 2 | 0.2 | 1 | 0.1 | 0.514 |
| Variable | Frequency | Percentage |
|---|---|---|
| Duration of disease (median (IQR) (years) | 4.00 (2.00–6.00) | |
| Required ICU admission | ||
| Yes | 94 | 4.6 |
| Duration of stay at the ICU (median (IQR) (days) (n = 94) | 9.00 (5.00–14.75) | |
| Status on discharge from the inpatient department (n = 828) | ||
| Improved | 510 | 61.6 |
| Transferred | 135 | 16.3 |
| Died | 90 | 10.9 |
| Stable | 81 | 9.8 |
| Unstable | 12 | 1.4 |
| Metastasis | ||
| Yes | 424 | 20.8 |
| Metastasis stage (n = 424) | ||
| Stage 1 | 2 | 0.5 |
| Stage 2 | 33 | 7.8 |
| Stage 3 | 59 | 13.9 |
| Stage 4 | 330 | 77.8 |
| Type of treatment | ||
| Chemotherapy | 402 | 19.7 |
| Surgery | 359 | 17.6 |
| Radiotherapy | 29 | 1.4 |
| Combination therapy | 1248 | 61.2 |
| First degree relative with cancer history | ||
| Yes | 7 | 0.3 |
| If yes, was it the same type of cancer that the patient suffers from? (n = 7) | ||
| Yes | 6 | 85.7 |
| Variable | Odds Ratio (95% CI) for Death | Odds Ratio (95% CI) for ICU Admission |
|---|---|---|
| Age | ||
| (below 60 years) (Reference) | 1.00 | 1.00 |
| (60 years and above) | 1.65 (1.05–2.59) * | 1.01 (0.65–1.58) |
| Gender | ||
| Women (Reference) | 1.00 | 1.00 |
| Men | 1.05 (0.68–1.61) | 0.97 (0.62–1.51) |
| Marital status | ||
| Single (Reference) | 1.00 | 1.00 |
| Married | 1.49 (0.76–2.90) | 0.63 (0.36–1.09) |
| Divorced | - | - |
| Widowed | 0.72 (0.28–1.86) | 1.63 (0.78–3.38) |
| Income category | ||
| Low (Reference) | 1.00 | 1.00 |
| Middle | 0.41 (0.11–1.52) | 0.56 (0.12–2.65) |
| High | 2.43 (0.66–9.05) | 1.78 (0.38–8.41) |
| Employment status | ||
| Student (Reference) | 1.00 | 1.00 |
| Unemployed | 1.94 (0.98–3.87) | 1.11 (0.60–2.08) |
| Employed | 0.32 (0.12–0.82) * | 0.87 (0.43–1.75) |
| Retired | 1.28 (0.52–3.16) | 1.02 (0.35–3.02) |
| Previous surgery | ||
| No (Reference) | 1.00 | 1.00 |
| Yes | 1.04 (0.62–1.72) | 2.91 (1.77–4.78) *** |
| Smoking history | ||
| No (Reference) | 1.00 | 1.00 |
| Yes | 0.69 (0.40–1.22) | 2.05 (1.19–3.51) ** |
| Drug use history | ||
| Not using the medication (Reference) | 1.00 | 1.00 |
| Statin | 2.01 (1.22–3.31) ** | 1.27 (0.79–2.06) |
| Inhaled corticosteroid | 2.15 (1.39–3.35) ** | 3.31 (2.10–5.21) *** |
| Heparin | 2.04 (1.28–3.24) ** | 2.03 (1.25–3.27) ** |
| Neuropathy treatment | 1.81 (1.10–2.96) * | 1.93 (1.16–3.23) * |
| B-Blocker | 1.35 (0.81–2.27) | 1.49 (0.89–2.51) |
| Antipsychotic | 1.45 (0.85–2.45) | 1.58 (0.91–2.74) |
| Angiotensin receptor blocker | 1.85 (1.10–3.09) * | 2.25 (1.33–3.80) ** |
| Diuretics | 3.21 (1.99–5.19) *** | 2.05 (1.19–3.51) ** |
| Antidepressant | 1.20 (0.67–2.17) | 1.19 (0.64–2.19) |
| Insulin | 0.96 (0.51–1.81) | 1.56 (0.86–2.81) |
| Nitrate | 1.28 (0.71–2.31) | 1.68 (0.94–2.99) |
| Angiotensin-converting enzyme | 1.21 (0.60–2.43) | 1.33 (0.67 –2.64) |
| Antiplatelet | 1.73 (0.92–3.27) | 2.01 (1.07–3.79) * |
| Corticosteroid | 1.97 (1.01–3.81) * | 2.43 (1.22–4.85) * |
| Ulcer treatment | 1.07 (0.45–2.58) | 0.41 (0.13–1.34) |
| Anticoagulant (warfarin) | 2.23 (1.04–4.77) * | 2.40 (1.10–5.26) * |
| Aspirin | 1.40 (0.57–3.39) | 1.73 (0.69–4.33) |
| Oral antidiabetic | 1.56 (0.64–3.82) | 2.46 (1.07–5.64) * |
| Anxiolytic | 0.96 (0.34–2.76) | 1.37 (0.51–3.65) |
| Anticonvulsant | 0.78 (0.18–3.50) | 0.96 (0.22–4.30) |
| Calcium channel blockers | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alyami, H.S.; Naser, A.Y.; Dahmash, E.Z.; Alyami, M.H.; Belali, O.M.; Assiri, A.M.; Rehman, A.; Alsaleh, A.M.; Alsaleh, H.A.; Hussein, S.H.; et al. Clinical and Therapeutic Characteristics of Cancer Patients in the Southern Region of Saudi Arabia: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 6654. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126654
Alyami HS, Naser AY, Dahmash EZ, Alyami MH, Belali OM, Assiri AM, Rehman A, Alsaleh AM, Alsaleh HA, Hussein SH, et al. Clinical and Therapeutic Characteristics of Cancer Patients in the Southern Region of Saudi Arabia: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(12):6654. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126654
Chicago/Turabian StyleAlyami, Hamad S., Abdallah Y. Naser, Eman Zmaily Dahmash, Mohammad H. Alyami, Osamah M. Belali, Ahmad M. Assiri, Amjad Rehman, Abdulrhman M. Alsaleh, Hind A. Alsaleh, Shahad H. Hussein, and et al. 2021. "Clinical and Therapeutic Characteristics of Cancer Patients in the Southern Region of Saudi Arabia: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 12: 6654. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126654