
The Effects of Interval Training and Continuous Training on Cardiopulmonary Fitness and Exercise Tolerance of Patients with Heart Failure—A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
- To compare the effects of IT and CT on cardiorespiratory fitness and exercise tolerance of patients with HF (subanalysis with different durations and isocaloric consumption).
- To compare difference high or moderate intensities of IT on cardiorespiratory fitness and exercise tolerance, to provide an optimal exercise prescription for patients with HF.
- To collect rehabilitation recommendations for future research on this topic.
2. Methods
2.1. Literature Search
2.2. Study Selection
2.3. Measured Outcomes
2.4. Data Extraction and Analysis
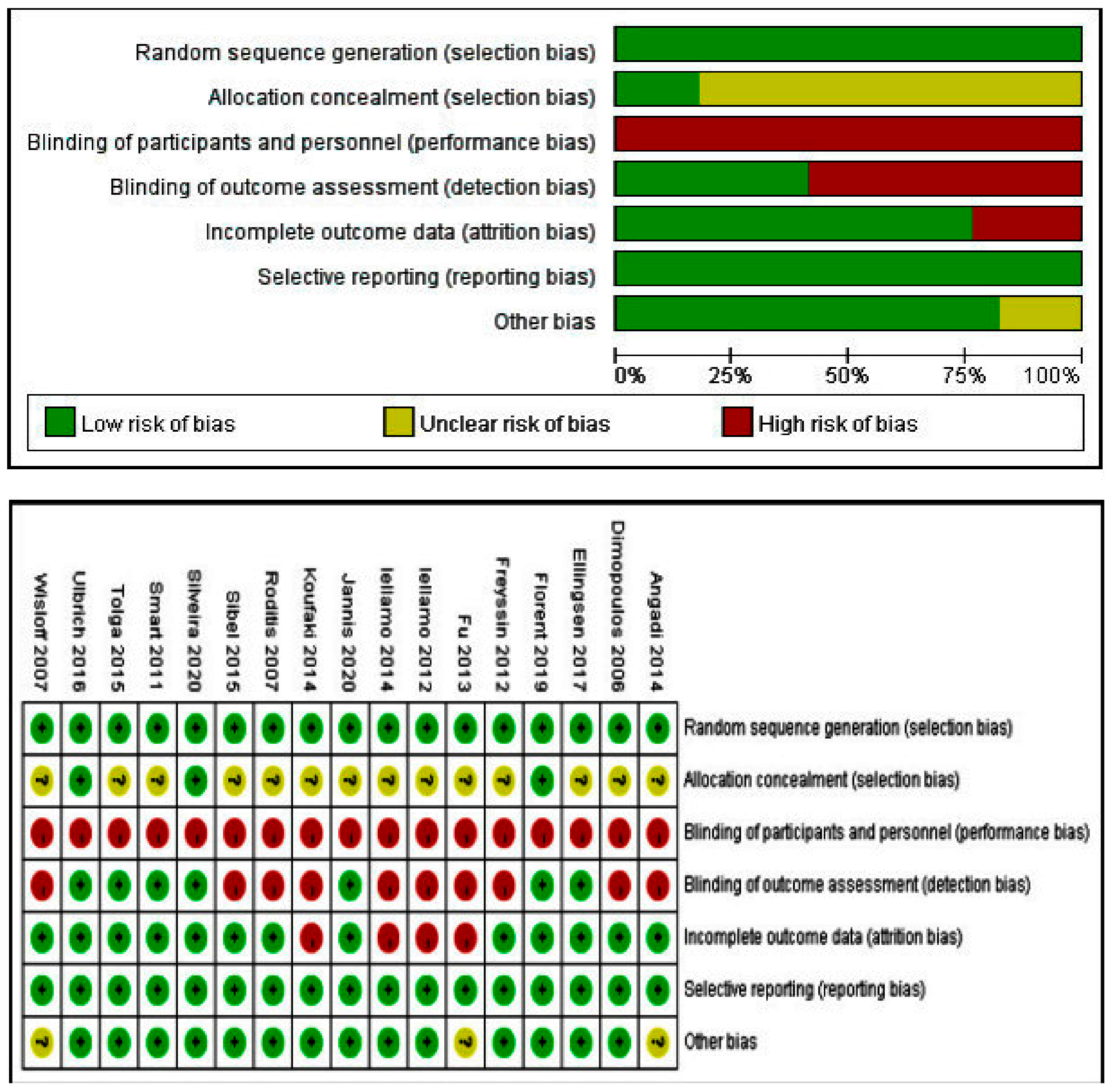
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
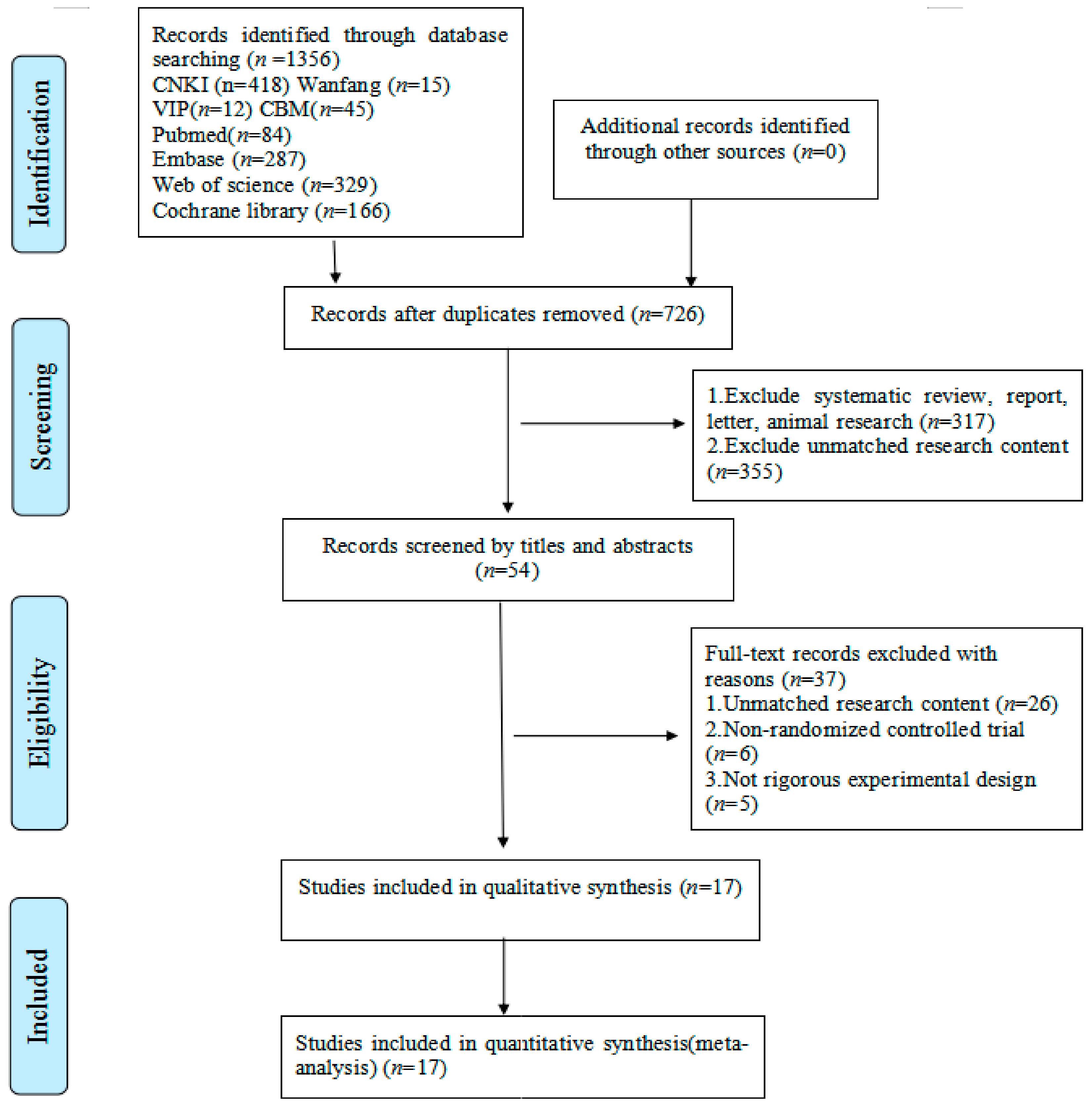
3.1. Identified Studies
3.2. Study Characteristics
3.3. Effects of the Intervention
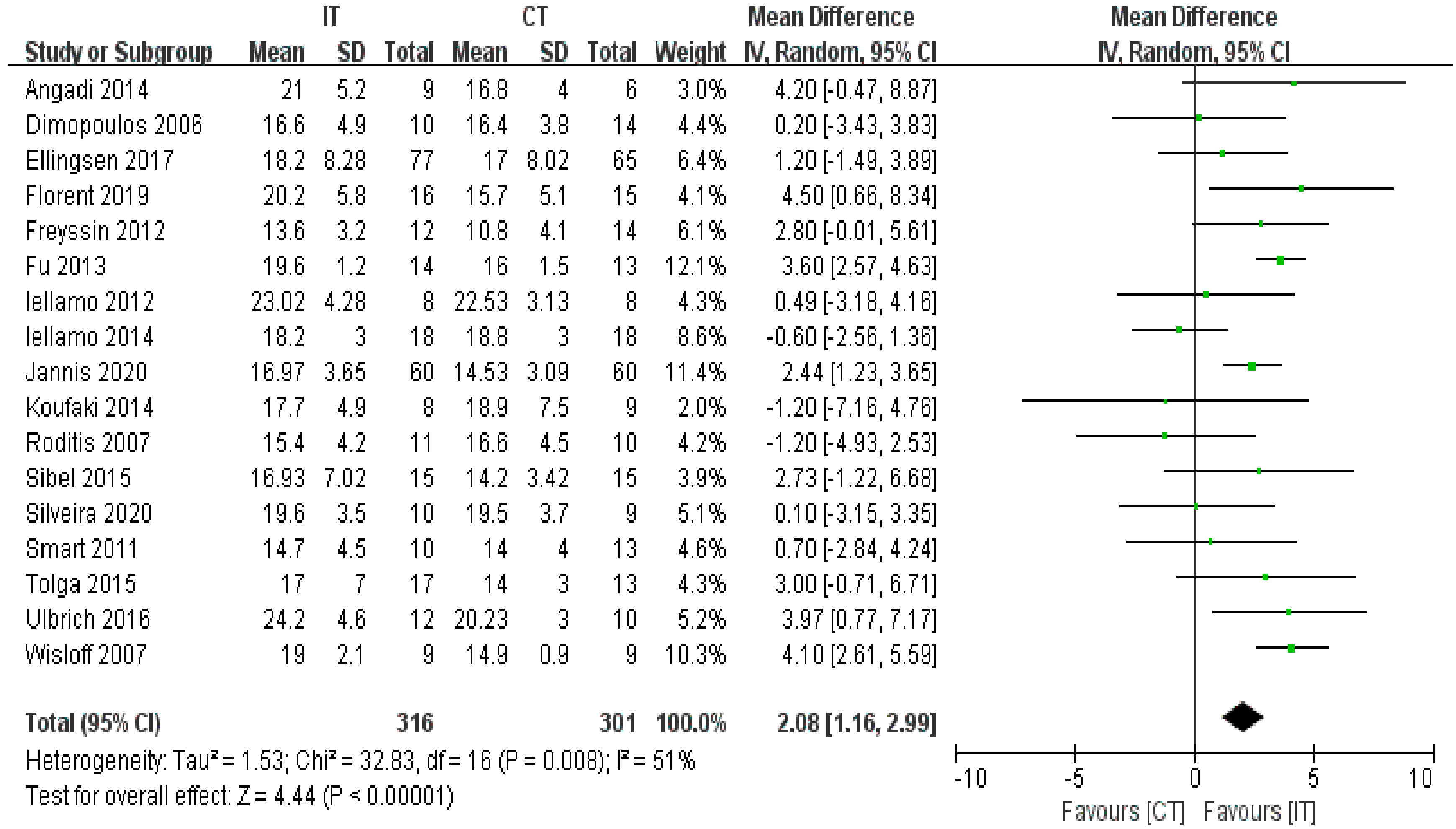
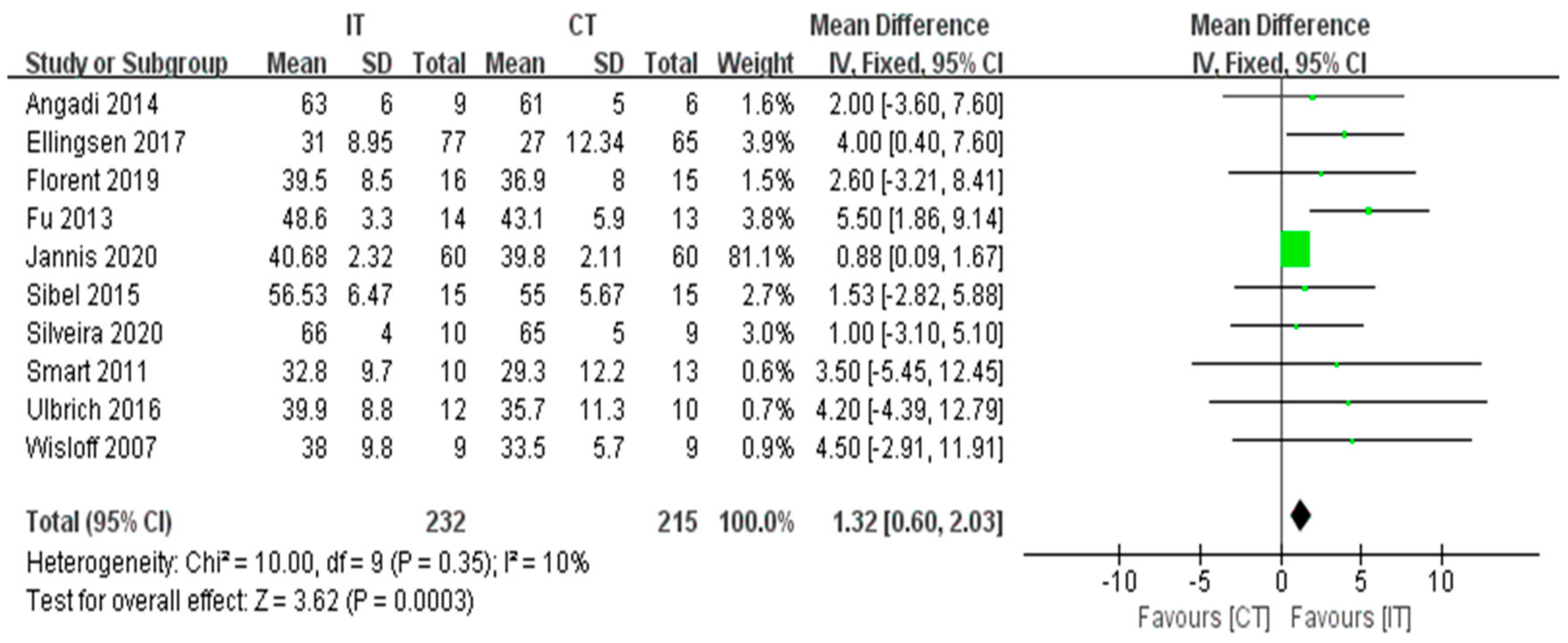
3.3.1. VO2peak
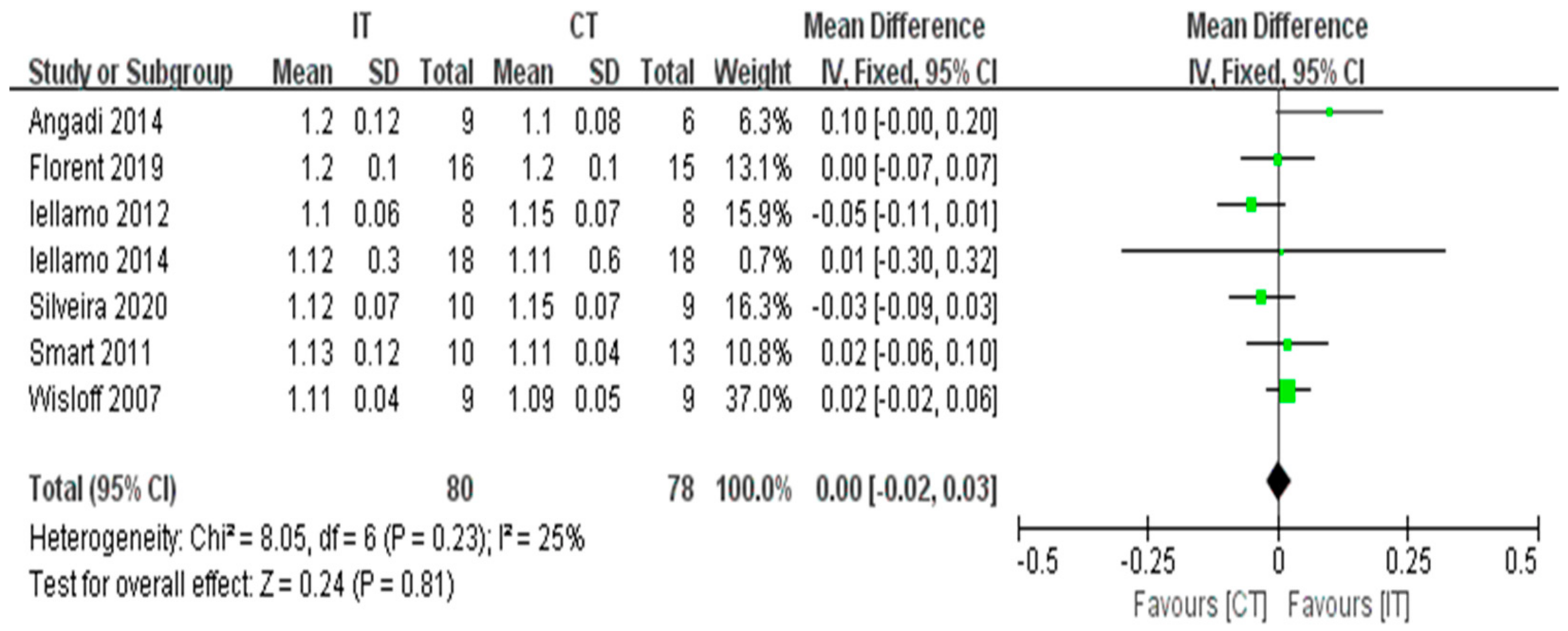
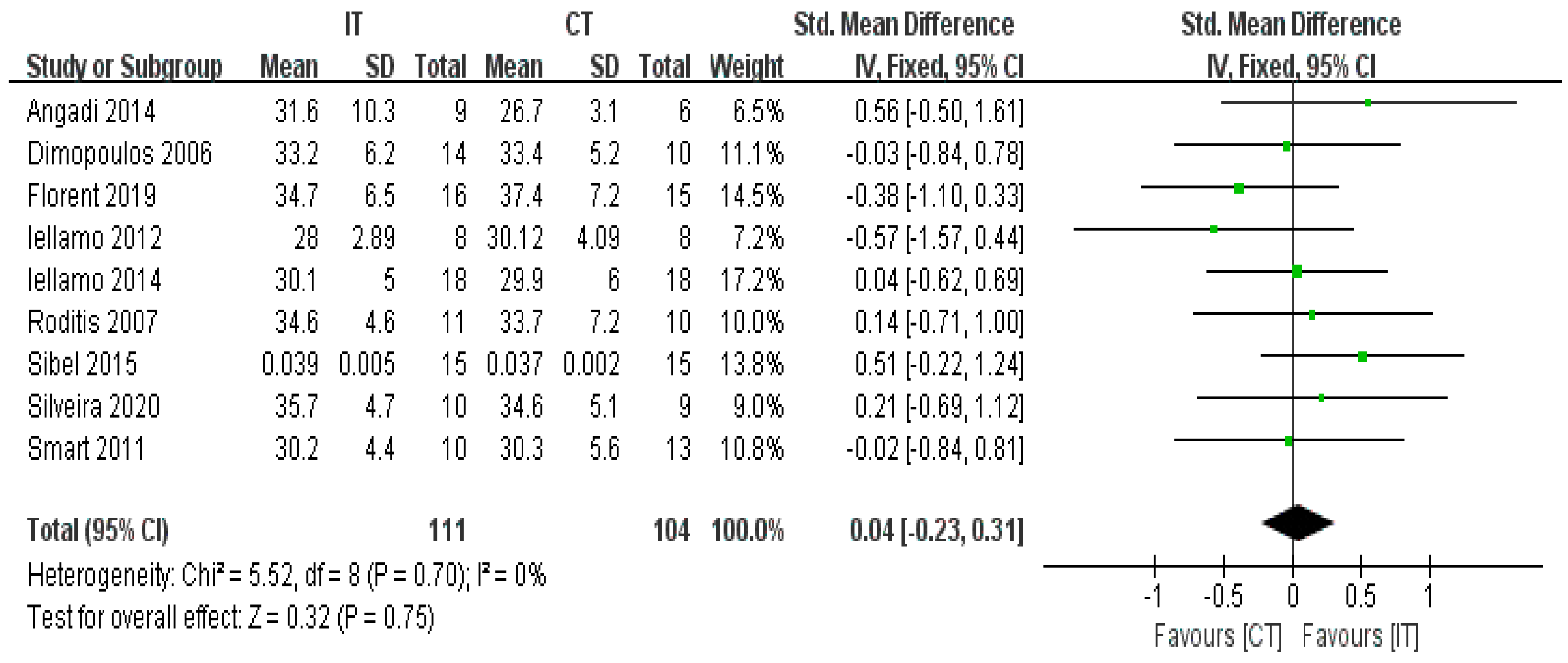
3.3.2. RER
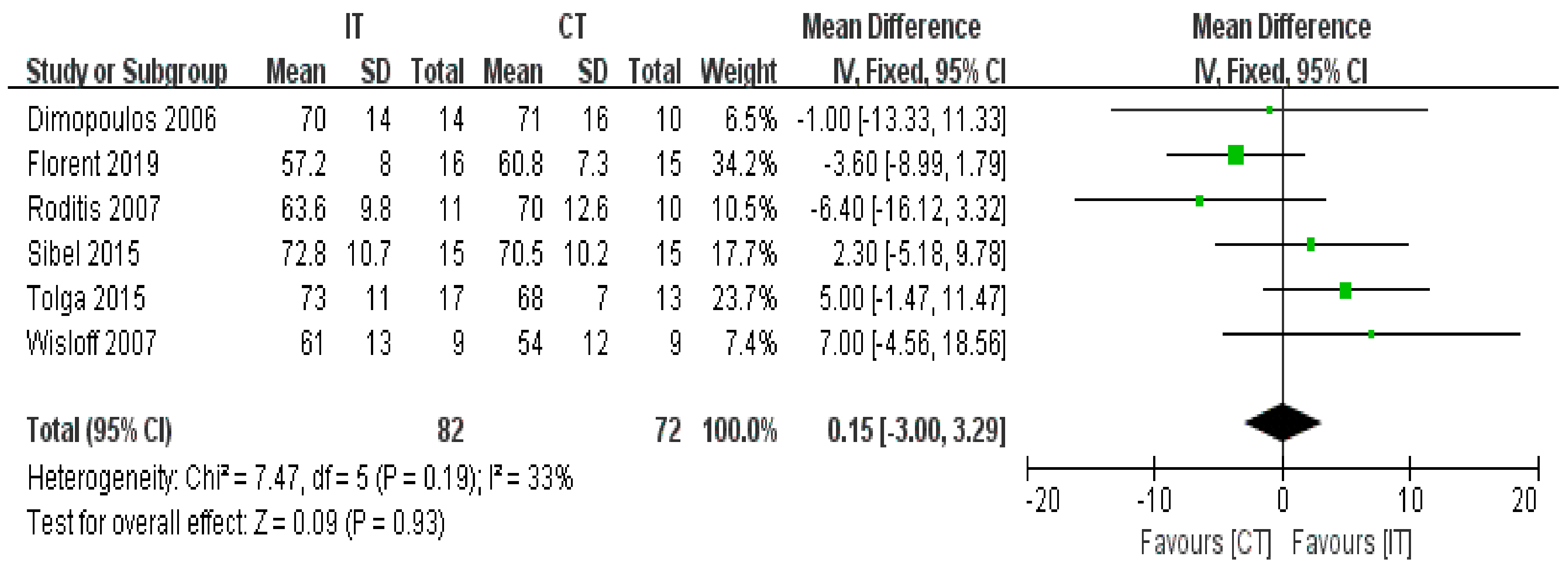
3.3.3. VE/VCO2 Slope
3.3.4. LVEF
3.3.5. HRrest
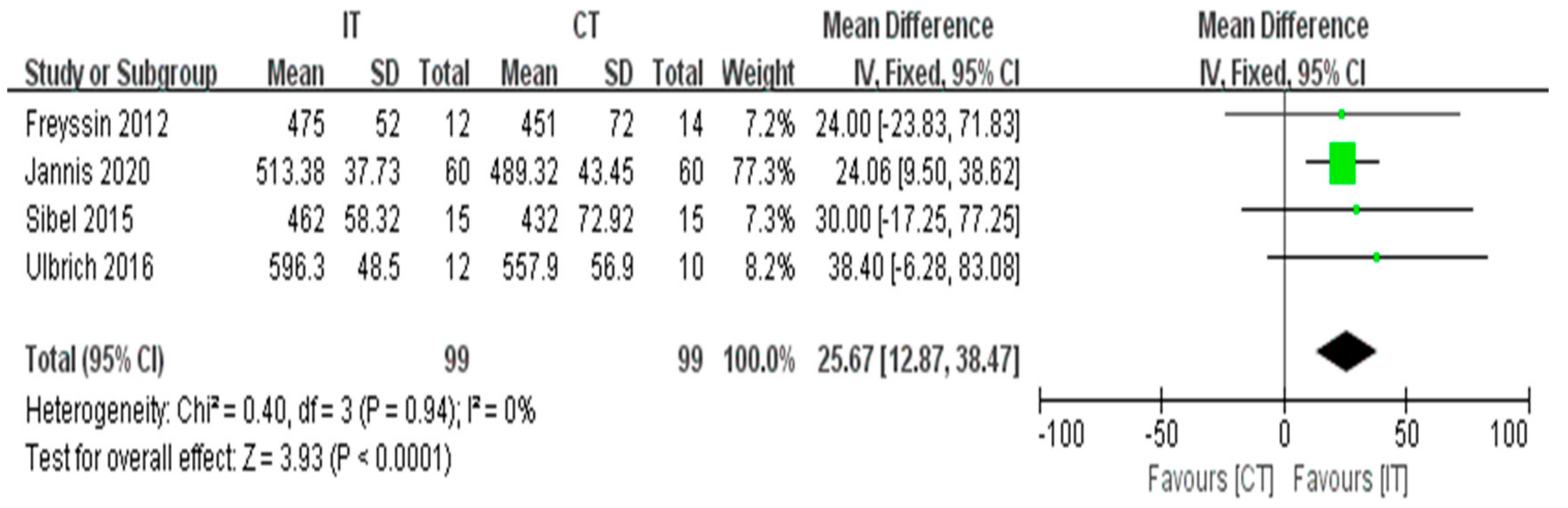
3.3.6. MWD
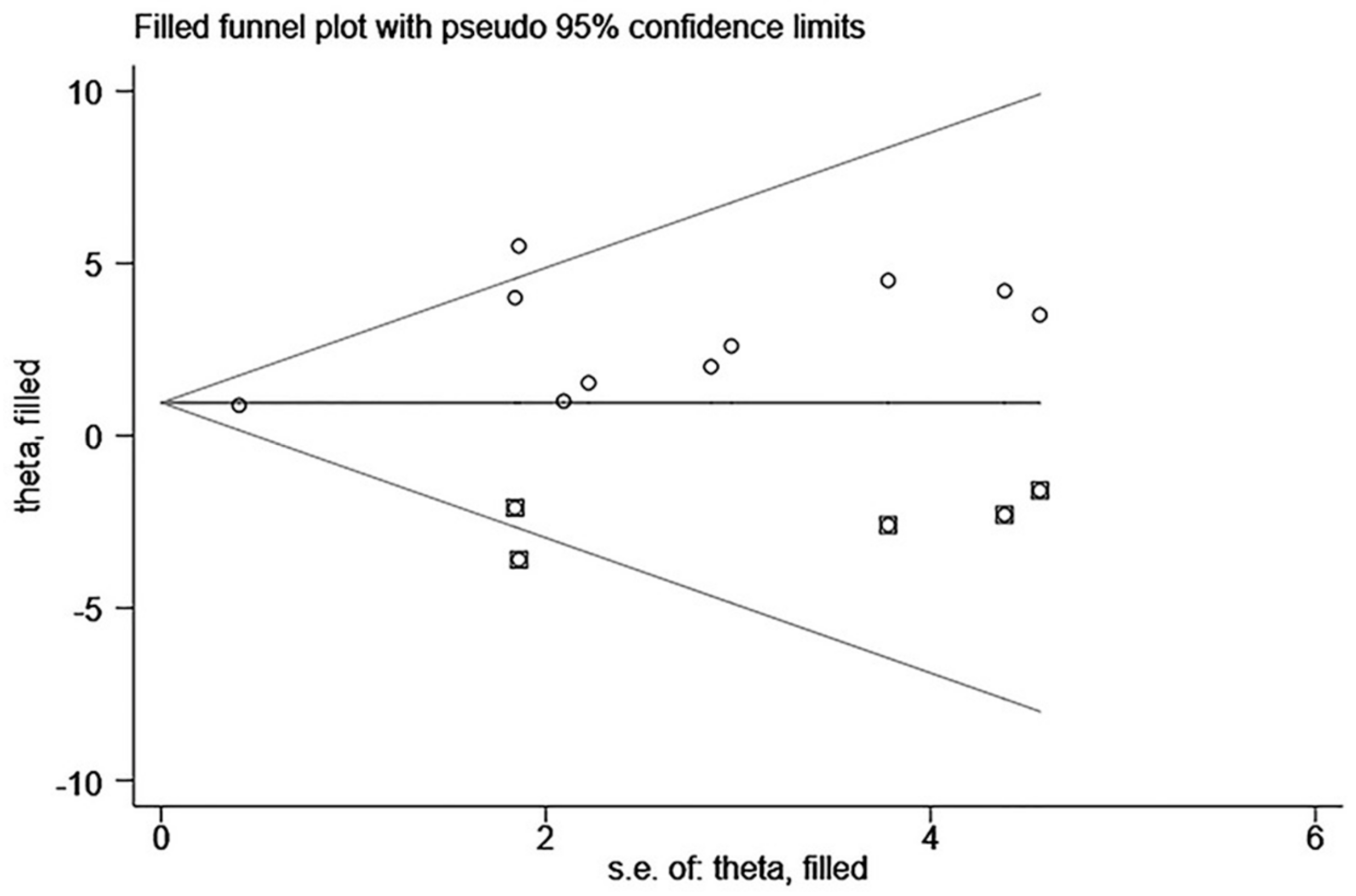
3.3.7. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benda, N.M.M.; Seeger, J.P.H.; Stevens, G.G.C.F.; Hijmans-Kersten, B.T.P.; van Dijk, A.; Bellersen, L.; Lamfers, E.J.P.; Hopman, M.T.E.; Thijssen, D.H.J. Effects of High-Intensity Interval Training versus Continuous Training on Physical Fitness, Cardiovascular Function and Quality of Life in Heart Failure Patients. PLoS ONE 2015, 10, e0141256. [Google Scholar] [CrossRef] [Green Version]
- Long, L.; Mordi, I.; Bridges, C.; Sagar, A.V.; Davies, E.J.; Coats, A.J.; Dalal, H.; Rees, K.; Singh, S.J.; Taylor, R.S. Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database Syst. Rev. 2019, 1, CD003331. [Google Scholar] [CrossRef] [Green Version]
- Isaksen, K.; Halvorsen, B.; Munk, P.S.; Aukrust, P.; Larsen, A.I. Effects of interval training on inflammatory biomarkers in patients with ischemic heart failure. Scand. Cardiovasc. J. 2019, 53, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Araújo, B.T.; Leite, J.C.; Fuzari, H.K.; de Souza, R.J.P.; Remígio, M.I.; de Andrade, A.D.; Campos, S.L.; Brandão, D.C. Influence of High-Intensity Interval Training Versus Continuous Training on Functional Capacity in Individuals with Heart Failure: A Systematic Review and Meta-Analysis. J. Cardiopulm. Rehabil. 2019, 39, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Van Tol, B.A.; Huijsmans, R.J.; Kroon, D.W.; Schothorst, M.; Kwakkel, G. Effects of exercise training on cardiac performance, exercise capacity and quality of life in patients with heart failure: A meta-analysis. Eur. J. Heart Fail. 2006, 8, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Rector, T.S.; Cohn, J.N. Assessment of patient outcome with the Minnesota Living with Heart Failure questionnaire: Reliability and validity during a randomized, double-blind, placebo-controlled trial of pimobendan. Am. Heart J. 1992, 124, 1017–1025. [Google Scholar] [CrossRef]
- Nilsson, B.B.; Westheim, A.; Risberg, M.A. Effects of Group-Based High-Intensity Aerobic Interval Training in Patients with Chronic Heart Failure. Am. J. Cardiol. 2008, 102, 1361–1365. [Google Scholar] [CrossRef]
- The Metabolic Fitness Program. J. Cardiopulm. Rehabil. Prev. 2011, 31, E1. [CrossRef]
- Meckel, Y.; Zach, S.; Eliakim, A.; Sindiani, M. The interval-training paradox: Physiological responses vs. subjective rate of perceived exertion. Physiol. Behav. 2018, 196, 144–149. [Google Scholar] [CrossRef]
- Hambrecht, R.; Niebauer, J.; Fiehn, E.; Kälberer, B.; Offner, B.; Hauer, K.; Riede, U.; Schlierf, G.; Kübler, W.; Schuler, G. Physical training in patients with stable chronic heart failure: Effects on cardiorespiratory fitness and ultrastructural abnormalities of leg muscles. J. Am. Coll. Cardiol. 1995, 25, 1239–1249. [Google Scholar] [CrossRef] [Green Version]
- Belardinelli, R.; Georgiou, D.; Cianci, G.; Purcaro, A. Randomized, Controlled Trial of Long-Term Moderate Exercise Training in Chronic Heart Failure. Circulation 1999, 99, 1173–1182. [Google Scholar] [CrossRef] [Green Version]
- Exercise training meta-analysis of trials in patients with chronic heart failure (ExTraMATCH). BMJ 2004, 328, 189. [CrossRef] [PubMed] [Green Version]
- Wang, L.M.; Shen, Y.Q. Consensus of Chinese Experts on Exercise Rehabilitation of Chronic Stable Heart Failure. Chin. J. Cardiol. 2014, 42, 714–720. [Google Scholar]
- Dun, Y.; Smith, J.R.; Liu, S.; Olson, T.P. High-Intensity Interval Training in Cardiac Rehabilitation. Clin. Geriatr. Med. 2019, 35, 469–487. [Google Scholar] [CrossRef]
- Rognmo, Ø.; Moholdt, T.; Bakken, H.; Hole, T.; Mølstad, P.; Myhr, N.E.; Grimsmo, J.; Wisløff, U. Cardiovascular Risk of High- Versus Moderate-Intensity Aerobic Exercise in Coronary Heart Disease Patients. Circulation 2012, 126, 1436–1440. [Google Scholar] [CrossRef] [Green Version]
- Meyer, K.; Schwaibolda, M.; Westbrook, S.; Beneke, R.; Hajric, R.; Lehmann, M.; Roskamm, H. Effects of exercise training and activity restriction on 6-minute walking test performance in patients with chronic heart failure. Am. Heart J. 1997, 133, 447–453. [Google Scholar] [CrossRef]
- Freyssin, C.; Verkindt, C.; Prieur, F.; Benaich, P.; Maunier, S.; Blanc, P. Cardiac Rehabilitation in Chronic Heart Failure: Effect of an 8-Week, High-Intensity Interval Training Versus Continuous Training. Arch. Phys. Med. Rehabil. 2012, 93, 1359–1364. [Google Scholar] [CrossRef] [Green Version]
- Iellamo, F.; Manzi, V.; Caminiti, G.; Vitale, C.; Castagna, C.; Massaro, M.; Franchini, A.; Rosano, G.; Volterrani, M. Matched dose interval and continuous exercise training induce similar cardiorespiratory and metabolic adaptations in patients with heart failure. Int. J. Cardiol. 2013, 167, 2561–2565. [Google Scholar] [CrossRef] [PubMed]
- Ulbrich, A.Z.; Angarten, V.G.; Netto, A.S.; Sties, S.W.; Bündchen, D.C.; De Mara, L.S.; Cornelissen, V.A.; De Carvalho, T. Comparative effects of high intensity interval training versus moderate intensity continuous training on quality of life in patients with heart failure: Study protocol for a randomized controlled trial. Clin. Trials Regul. Sci. Cardiol. 2016, 13, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Smart, N.A.; Steele, M. A Comparison of 16 Weeks of Continuous vs Intermittent Exercise Training in Chronic Heart Failure Patients. Congest. Heart Fail. 2011, 18, 205–211. [Google Scholar] [CrossRef] [Green Version]
- Keteyian, S.J.; Brawner, C.A.; Savage, P.D.; Ehrman, J.K.; Schairer, J.; Divine, G.; Aldred, H.; Ophaug, K.; Ades, P.A. Peak aerobic capacity predicts prognosis in patients with coronary heart disease. Am. Heart J. 2008, 156, 292–300. [Google Scholar] [CrossRef]
- Arena, R.; Myers, J.; Aslam, S.S.; Varughese, E.B.; Peberdy, M.A. Peak VO2 and VE/VCO2 slope in patients with heart failure: A prognostic comparison. Am. Heart J. 2004, 147, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.-C.; Wang, C.-H.; Lin, P.-S.; Hsu, C.-C.; Cherng, W.-J.; Huang, S.-C.; Liu, M.-H.; Chiang, C.-L.; Wang, J.-S. Aerobic interval training improves oxygen uptake efficiency by enhancing cerebral and muscular hemodynamics in patients with heart failure. Int. J. Cardiol. 2013, 167, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Koufaki, P.; Mercer, T.; George, K.; Nolan, J. Low-volume high-intensity interval training vs continuous aerobic cycling in patients with chronic heart failure: A pragmatic randomised clinical trial of feasibility and effectiveness. J. Rehabil. Med. 2014, 46, 348–356. [Google Scholar] [CrossRef] [Green Version]
- Iellamo, F.; Caminiti, G.; Sposato, B.; Vitale, C.; Massaro, M.; Rosano, G.; Volterrani, M. Effect of High-Intensity interval training versus moderate continuous training on 24-h blood pressure profile and insulin resistance in patients with chronic heart failure. Intern. Emerg. Med. 2013, 9, 547–552. [Google Scholar] [CrossRef]
- Aksoy, S.; Findikoglu, G.; Ardic, F.; Rota, S.; Dursunoglu, D. Effect of 10-Week Supervised Moderate-Intensity Intermittent vs. Continuous Aerobic Exercise Programs on Vascular Adhesion Molecules in Patients with Heart Failure. Am. J. Phys. Med. Rehabil. 2015, 94, 898–911. [Google Scholar] [CrossRef]
- Besnier, F.; Labrunée, M.; Richard, L.; Faggianelli, F.; Kerros, H.; Soukarié, L.; Bousquet, M.; Garcia, J.-L.; Pathak, A.; Gales, C.; et al. Short-term effects of a 3-week interval training program on heart rate variability in chronic heart failure. A randomised controlled trial. Ann. Phys. Rehabil. Med. 2019, 62, 321–328. [Google Scholar] [CrossRef]
- Wang, G.H.; Deng, Y.L.; Wang, H.; Li, L. Correlation analysis between clinical examination indexes and heart function of elderly patients with heart failure. Chin. J. Gerontol. 2009, 23, 3033–3035. [Google Scholar]
- Wisløff, U.; Støylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, Ø.; Haram, P.M.; Tjønna, A.E.; Helgerud, J.; Slørdahl, S.A.; Lee, S.J.; et al. Superior Cardiovascular Effect of Aerobic Interval Training Versus Moderate Continuous Training in Heart Failure Patients. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef] [Green Version]
- Ellingsen, Ø.; Halle, M.; Conraads, V.; Støylen, A.; Dalen, H.; Delagardelle, C.; Larsen, A.-I.; Hole, T.; Mezzani, A.; Van Craenenbroeck, E.M.; et al. High-Intensity Interval Training in Patients with Heart Failure with Reduced Ejection Fraction. Circulation 2017, 135, 839–849. [Google Scholar] [CrossRef] [PubMed]
- Neto, M.G.; Durães, A.R.; Conceição, L.S.R.; Saquetto, M.B.; Ellingsen, Ø.; Carvalho, V. High intensity interval training versus moderate intensity continuous training on exercise capacity and quality of life in patients with heart failure with reduced ejection fraction: A systematic review and meta-analysis. Int. J. Cardiol. 2018, 261, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Cochrane Collab. 2011. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stavros, D.; Maria, A.; Dimitrios, S.; Stavros, D.; Smaragdo, K.; George, M.; Nanas, S. Effects of exercise rehabilitation program on heart rate recovery in patients with chronic heart failure. Eur. J. Cardiov. Prev. R. 2006, 13, 67–73. [Google Scholar] [CrossRef]
- Roditis, P.; Dimopoulos, S.; Sakellariou, D.; Sarafoglou, S.; Kaldara, E.; Venetsanakos, J.; Vogiatzis, J.; Anastasiou-Nana, M.; Roussos, C.; Nanas, S. The effects of exercise training on the kinetics of oxygen uptake in patients with chronic heart failure. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Angadi, S.S.; Mookadam, F.; Lee, C.D.; Tucker, W.J.; Haykowsky, M.J.; Gaesser, G.A. High-intensity interval training vs. moderate-intensity continuous exercise training in heart failure with preserved ejection fraction: A pilot study. J. Appl. Physiol. 2015, 119, 753–758. [Google Scholar] [CrossRef]
- Yalın, T.Y.; Gülin, F.M.Y.; Sibel, K.; Hande, S. The effects of baseline heart rate recovery normality and exercise training protocol on heart rate recovery in patients with heart failure. Anatol. J. Cardiol. 2015, 15, 727–734. [Google Scholar] [CrossRef]
- Papathanasiou, J.V.; Petrov, I.; Tokmakova, M.P.; Dimitrova, D.D.; Spasov, L.; Dzhafer, N.S.; Tsekoura, D.; Dionyssiotis, Y.; Ferreira, A.S.; Lopes, A.J.; et al. Group-based cardiac rehabilitation interven-tions. A challenge for physical and rehabilitation medicine physicians: A randomized controlled trial. Eur. J. Phys. Rehab. Med. 2020, 56, 479–488. [Google Scholar] [CrossRef]
- Da Silveira, A.D.; De Lima, J.B.; Piardi, D.D.S.; Macedo, D.D.S.; Zanini, M.; Nery, R.; Laukkanen, J.A.; Stein, R. High-intensity interval training is effective and superior to moderate continuous training in patients with heart failure with preserved ejection fraction: A randomized clinical trial. Eur. J. Prev. Cardiol. 2020, 27, 1733–1743. [Google Scholar] [CrossRef]
- Moore, B.; Brubaker, P.H.; Stewart, K.P.; Kitzman, D.W. VE/VCO2 Slope in Older Heart Failure Patients with Normal Versus Reduced Ejection Fraction Compared with Age-Matched Healthy Controls. J. Card. Fail. 2007, 13, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Osibogun, O.; Ogunmoroti, O.; Spatz, E.S.; Fashanu, O.E.; Michos, E.D. Ideal cardiovascular health and resting heart rate in the Multi-Ethnic Study of Atherosclerosis. Prev. Med. 2020, 130, 105890. [Google Scholar] [CrossRef]
- Smart, N.A.; Dieberg, G.; Giallauria, F. Intermittent versus continuous exercise training in chronic heart failure: A meta-analysis. Int. J. Cardiol. 2013, 166, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Pattyn, N.; Coeckelberghs, E.; Buys, R.; Cornelissen, V.A.; Vanhees, L. Aerobic Interval Training vs. Moderate Continuous Training in Coronary Artery Disease Patients: A Systematic Review and Meta-Analysis. Sports Med. 2014, 44, 687–700. [Google Scholar] [CrossRef]
- Gomes-Neto, M.; Durães, A.R.; Dos Reis, H.F.C.; Neves, V.R.; Martinez, B.P.; Carvalho, V. High-intensity interval training versus moderate-intensity continuous training on exercise capacity and quality of life in patients with coronary artery disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2017, 24, 1696–1707. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Atwood, J.E. Exercise Capacity and Mortality among Men Referred for Exercise Testing. N. Engl. J. Med. 2002, 346, 793–801. [Google Scholar] [CrossRef]
- Kavanagh, T.; Mertens, D.J.; Hamm, L.F.; Beyene, J.; Kennedy, J.; Corey, P.; Shephard, R.J. Prediction of Long-Term Prognosis in 12 169 Men Referred for Cardiac Rehabilitation. Circulation 2002, 106, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Opasich, C.; Pinna, G.D.; Bobbio, M.; Sisti, M.; Demichelis, B.; Febo, O.; Forni, G.; Riccardi, R.; Riccardi, P.; Capomolla, S.; et al. Peak exercise oxygen consumption in chronic heart failure: Toward efficient use in the individual patient. J. Am. Coll. Cardiol. 1998, 31, 766–775. [Google Scholar] [CrossRef] [Green Version]
- Mancini, D.M.; Eisen, H.; Kussmaul, W.; Mull, R.; Edmunds, L.H.; Wilson, J.R. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation 1991, 83, 778–786. [Google Scholar] [CrossRef] [Green Version]
- Montero, D.; Diaz-Cañestro, C.; Lundby, C. Endurance Training and VO2max. Med. Sci. Sports Exerc. 2015, 47, 2024–2033. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Després, J.-P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e653–e699. [Google Scholar] [CrossRef] [PubMed]
- Tomczak, C.R.; Thompson, R.B.; Paterson, D.I.; Schulte, F.; Cheng-Baron, J.; Haennel, R.G.; Haykowsky, M.J. Effect of acute high-intensity interval exercise on postexercise biventricular function in mild heart failure. J. Appl. Physiol. 2011, 110, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Xie, B.; Yan, X.; Cai, X.; Li, J. Effects of High-Intensity Interval Training on Aerobic Capacity in Cardiac Patients: A Systematic Review with Meta-Analysis. BioMed Res. Int. 2017, 2017, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Shave, R.; Oxborough, D. Exercise-Induced Cardiac Injury: Evidence from Novel Imaging Techniques and Highly Sensitive Cardiac Troponin Assays. Prog. Cardiovasc. Dis. 2012, 54, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, J.A.; Wiles, J.D.; Coleman, D.A.; Papadakis, M.; Sharma, R.; O’Driscoll, J.M. Left Ventricular Function and Cardiac Biomarker Release—The Influence of Exercise Intensity, Duration and Mode: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 1275–1289. [Google Scholar] [CrossRef] [PubMed]
- Erbs, S.; Höllriegel, R.; Linke, A.; Beck, E.B.; Adams, V.; Gielen, S.; Möbius-Winkler, S.; Sandri, M.; Kränkel, N.; Hambrecht, R.; et al. Exercise Training in Patients with Advanced Chronic Heart Failure (NYHA IIIb) Promotes Restoration of Peripheral Vasomotor Function, Induction of Endogenous Regeneration, and Improvement of Left Ventricular Function. Circ. Heart Fail. 2010, 3, 486–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farber, H.W.; Miller, D.; McGoon, M.D.; Frost, A.E.; Benton, W.W.; Benza, R.L. Predicting outcomes in pulmonary arterial hypertension based on the 6-minute walk distance. J. Heart Lung Transplant. 2015, 34, 362–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Layec, G.; Blain, G.M.; Rossman, M.J.; Park, S.Y.; Hart, C.R.; Trinity, J.D.; Gifford, J.R.; Sidhu, S.; Weavil, J.C.; Hureau, T.J.; et al. Acute High-Intensity Exercise Impairs Skeletal Muscle Respiratory Capacity. Med. Sci. Sports Exerc. 2018, 50, 2409–2417. [Google Scholar] [CrossRef]
- Mezzani, A.; Corrà, U.; Bosimini, E.; Giordano, A.; Giannuzzi, P. Contribution of peak respiratory exchange ratio to peak VO2 prognostic reliability in patients with chronic heart failure and severely reduced exercise capacity. Am. Heart J. 2003, 145, 1102–1107. [Google Scholar] [CrossRef]
- Francis, D.P.; Shamim, W.; Davies, L.C.; Piepoli, M.F.; Ponikowski, P.; Anker, S.D.; Coats, A.S. Cardiopulmonary exercise testing for prognosis in chronic heart failure: Continuous and independent prognostic value from VE/VCO2slope and peak VO2. Eur. Heart J. 2000, 21, 154–161. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Characteristics of Patients | Outcome | Quality Assessment | |||
|---|---|---|---|---|---|---|---|
| Sample Size (IT/CT) | Gender (M/F) | Age (years) (Mean ± SD) | Diagnosis Standard of HF | ||||
| Dimopoulos 2006 [34] | Greece | 24 (14/10) | IT (9/1) CT (14/0) | IT (59.2 ± 12.2) CT (61.5 ± 7.1) | HFrEF HFmrEF HFpEF | VO2peak, VE/VCO2 Slope, HRrest | 4 |
| Roditis 2007 [35] | Greece | 21 (11/10) | IT (10/1) CT (9/1) | IT (63 ± 2) CT (61 ± 3) | HFrEF HFmrEF | VO2peak, VE/VCO2 Slope, HRrest | 4 |
| Wisloff 2007 [29] | Norway | 18 (9/9) | IT (7/2) CT (7/2) | IT (76.5 ± 9) CT (74.4 ± 12) | HFrEF | VO2peak, RER, LVEF, HRrest | 3 |
| Smart 2011 [20] | Australia | 23 (10/13) | IT (8/2) CT (13/0) | IT (59.1 ± 11) CT (62.9 ± 9.3) | HFrEF | VO2peak, RER, VE/VCO2 slope, LVEF | 5 |
| Freyssin 2012 [17] | France | 26 (12/14) | IT (6/6) CT (7/7) | IT (54 ± 9) CT(55 ± 12) | HFrEF | VO2peak, 6WMT | 4 |
| Iellamo 2012 [18] | Italy | 16 (8/8) dropout 20% | NI | IT(62.2 ± 8) CT (62.6 ± 9) | HFrEF | VO2peak, RER, VE/VCO2 slope | 3 |
| Fu 2013 [23] | Taiwan | 30 (15/15) dropout 10% | IT (10/5) CT (9/6) | IT (67.5 ± 1.8) CT (66.3 ± 2.1) | HFrEF HFmrEF | VO2peak, LVEF | 2 |
| Koufaki 2014 [24] | England | 33 (16/17) dropout 48% | IT (14/2) CT (13/4) | IT (59.8 ± 7.4) CT (59.7 ± 10.8) | HFrEF HFmrEF | VO2peak | 3 |
| Angadi 2014 [36] | America | 15 (9/6) | IT (8/1) CT (4/2) | IT (69 ± 6.1) CT (71.5 ± 11.7) | HFpEF | VO2peak, RER, VE/VCO2 slope, LVEF | 3 |
| Iellamo 2014 [25] | Italy | 36 (18/18) dropout 8% | IT (16/2) CT (15/3) | IT (67.2 ± 6) CT (68.4 ± 8) | HFrEF | VO2peak, RER, VE/VCO2 slope | 3 |
| Tolga 2015 [37] | Turkey | 30 (17/13) | IT (13/4) CT (13/0) | IT (63.7 ± 8.8) CT (59.6 ± 6.8) | HFrEF HFmrEF | VO2peak, HRrest | 5 |
| Sibel 2015 [26] | Turkey | 30 (15/15) | IT (13/2) CT (13/2) | IT (63.7 ± 8.8) CT (59.6 ± 6.9) | HFrEF HFmrEF HFpEF | VO2peak, VE/VCO2 slope, LVEF, HRrest, 6WMT | 4 |
| Ulbrich 2016 [19] | Brazil | 22 (12/10) | IT (12/0) CT (10/0) | IT (53.15 ± 7) CT (54.02 ± 9.9) | HFrEF HFmrEF | VO2peak, LVEF, HRrest, 6WMT | 6 |
| Ellingsen 2017 [30] | Norway | 142 (77/65) | IT (59/18) CT (53/12) | IT (63 ± 22.4) CT (61.5 ± 14.4) | HFrEF | VO2peak, LVEF | 5 |
| Florent 2019 [27] | France | 31 (16/15) | IT (11/5) CT (11/4) | IT (59 ± 13) CT (59.5 ± 12) | HFrEF HFmrEF | VO2peak, RER, VE/VCO2 slope, LVEF, HRrest | 6 |
| Jannis 2020 [38] | Bulgaria | 120 (60/60) | IT (35/25) CT (35/25) | IT (63.7 ± 6.7) CT (63.8 ± 6.7) | HFrEF | VO2peak, LVEF, 6WMT | 5 |
| Silveira 2020 [39] | Brazil | 19 (10/9) | IT (3/7) CT (4/5) | IT (60 ± 10) CT (60 ± 9) | HFpEF | VO2peak, RER, VE/VCO2 slope, LVEF | 6 |
| Study | Intervention | |||
|---|---|---|---|---|
| Mode | Duration | Exercise Program | ||
| IT | CT | |||
| Dimopoulos 2006 [34] | Cycle ergometer | 12 weeks, 3 d/week | Total: 40 min ① 40 × 30 s interval (100–120% WR peak) ② 40 × 30 s recovery | Total: 40 min 40 min cycling (50–70% WR peak) |
| Roditis 2007 [35] | Cycle ergometer | 12 weeks, 3 d/week | Total: 40 min ① 40 × 30 s interval (100–120% WR peak) ② 40 × 30 s recovery | Total: 40 min 40 min cycling (50–60% WR peak) |
| Wisloff 2007 [29] | Treadmill | 12 weeks, 3 d/week | Total: 38 min ① 10 min warm-up (60–70% HRpeak) ② 4 × 4 min interval (90–95% HRmax) ③ 3 × 3 min recovery (50–70% HRmax) ④ 3 min cool-down | Total: 47 min 47 min running (70–75% HRmax) |
| Smart 2011 [20] | Cycle ergometer | 16 weeks, 3 d/week | Total: 60 min ① 30 × 60 s interval (70% VO2peak) ②3 0 × 60 s recovery | Total: 30 min 30 min cycling (70% VO2peak) |
| Freyssin 2012 [17] | Cycle ergometer/Treadmill | 8 weeks, 5 d/week | Total: 74 min ① 10 min warm-up (5 W) ② (12 repetitions of 30 s of exercise and 60 s of recovery)*3 (50–80 W), separated by 5 min recovery | Total: 60 min ① 10 min warm-up ② 45 min running/cycling (HRVT1) ③ 5 min cool-down |
| Iellamo 2012 [18] | Treadmill | 12 weeks, 2 d/1–3 weeks, 3 d/4–6 weeks, 4 d/7–9 weeks, 5 d/10–12 weeks | Total: 37 min ① 9 min warm-up ② 4 × 4 min interval (75–80% HRR) ③ 4 × 3 min recovery (45–50% HRR) | Total: 30–45 min 30–45 min running (45–60% HRR) |
| Fu 2013 [23] | Cycle ergometer | 12 weeks, 3 d/week | Total: 60 min ① 30 × 60 s interval (60–70% VO2peak) ② 30 × 60 s recovery | Total: 30 min 30 min cycling (60–70% VO2peak) |
| Koufaki 2014 [24] | Cycle ergometer | 24 weeks, 3 d/week | Total: 30 min (30 s × 10 interval (100% WR peak) 60 s × 10 recovery (20–30% WR peak) × 2 | Total: 40 min 40 min cycling (40–60% VO2peak) |
| Angadi 2014 [36] | Treadmill | 4 weeks, 3 d/week | Total: 31–43 min ① 10 min warm-up (50% HR peak) ② 4 × 2–4 min interval (80–90% HRpeak) ③ 4 × 2–3 min recovery (50% HR peak) ④ 5 min cool-down (50% HR peak) | Total: 30–45 min ① 10 min warm-up (50% HRpeak) ② 15–30 min running (60–70% HR peak) ③ 5 min cool-down (50% HRpeak) |
| Iellamo 2014 [25] | Treadmill | 12 weeks, 3 d/week | Total: 48 min ① 10 min warm-up ② 4 × 4 min interval (75–80% HRR) ③ 4 × 3 min recovery (45–50% HRR) ④ 10 min cool-down | Total: 55–60 min ① 10 min warm-up ② 30–45 min running (45–60% HRR) ③ 10 min cool-down |
| Tolga 2015 [37] | Cycle ergometer | 12 weeks, 3 d/week | ① 5 min warm-up ② 30 s interval (50–75% HRR) with 30 s recovery (50–75% HRR) ③ 5 min cool-down | Total: 40 min ① 5 min warm-up ② 30 min cycling (50–75% HRR) ③ 5 min cool-down |
| Sibel 2015 [26] | Cycle ergometer | 10 weeks, 3 d/week | Total: 35 min ① 10 min warm-up/cool-down (20 W) ② 17 × 60 s interval (50–75% VO2peak) ③ 17 × 30 s recovery (30 W) | Total: 35 min ① 10 min warm-up/cool-down (20 W) ② 25 min cycling (50–75% VO2peak) |
| Ulbrich 2016 [19] | Treadmill | 12 weeks, 3 d/week | Total: 36–51 min ① 7–10 min warm-up (70% HR peak) ② 4–6 × 3 min interval (95% HR peak) ③ 4–6 × 3 min recovery (70% HRpeak) ④ 5 min cool-down (50% VO2peak) | Total: 42–45 min ① 7–10 min warm-up (70% HRpeak) ② 30 min Running (75% HRpeak) ③ 5 min cool-down (50% VO2peak) |
| Ellingsen 2017 [30] | Cycle ergometer/treadmill | 12 weeks, 3 d/week | Total: 38 min ① 5 min warm-up ② 4 × 4 min interval (90–95% HRpeak) ③ 4 × 3 min recovery ④ 5 min cool-down | Total: 47 min 47 min cycling or running (60–70% HRpeak) |
| Florent 2019 [27] | Cycle ergometer | 3 weeks, 5 d/week | Total: 30 min ① 5 min warm-up (30% WR peak) ② 2 × (30 s interval following 30 s recovery × 8)(100% WR peak), seperated by 4 min recovery ③ 5 min cool-down (30% WR peak) | Total: 40 min ① 5 min warm-up (30% WR peak) ② 30 min cycling (60% WR peak) ③ 5 min cool-down (30% WRpeak) |
| Jannis 2020 [38] | Cycle ergometer | 12 weeks, 2 d/week | Total: 40 min ① Warm-up ② 3 bouts of interval (90% HRpeak) ③ 2 bouts of recovery (70% HRpeak) ④ Cool-down | Total: 40 min 40 min cycling (70% HRpeak) |
| Silveira 2020 [39] | Treadmill | 12 weeks, 3 d/week | Total: 38 min ① 10 min warm-up ② 4 × 4 min interval (85–95% HRpeak) ③ 3 × 3 min recovery ④ 3 min cool-down | Total: 47 min 47 min running (60–70% HRpeak) |
| Outcome | Subgroup | Potential Factors | Included Studies | Sample Size | 95% Confidence Intervals | Heterogeneity | p-Value |
|---|---|---|---|---|---|---|---|
| VO2 peak | Intervention duration | Duration < 12 weeks | 4 | 102 | 3.38 (1.56, 5.19) | I2 = 0% p = 0.87 | p = 0.0003 |
| Duration ≥ 12 weeks | 13 | 515 | 1.73 (0.65, 2.82) | I2 = 62% p = 0.002 | p = 0.002 | ||
| Exercise intensity of IT | Intensity of 60–80% HRpeak | 5 | 136 | 3.26 (2.38, 4.15) | I2 = 0% p = 0.62 | p < 0.00001 | |
| Intensity of 80–100% HRpeak | 12 | 481 | 1.70 (0.47, 2.92) | I2 =58% p = 0.007 | p = 0.007 | ||
| Isocaloric consumption | Yes | 7 | 267 | 1.80 (0.28, 3.31) | I2 = 65% p = 0.009 | p = 0.02 | |
| No | 10 | 350 | 2.14 (0.99, 3.29) | I2 = 33% p = 0.14 | p = 0.0003 |
| Outcomes | n | Std. Err | t | p > |t| | 95% CI | Interval |
|---|---|---|---|---|---|---|
| VO2peak | 17 | 0.656 | −1.87 | 0.081 | −2.625 | 0.170 |
| VE/VCO2 slope | 9 | 2.093 | 0.18 | 0.862 | −4.570 | 5.326 |
| LVEF | 10 | 0.340 | 2.84 | 0.022 | 0.182 | 1.746 |
| HRrest | 6 | 1.890 | 0.35 | 0.745 | −4.590 | 5.905 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, D.; Chen, P.; Zhu, J. The Effects of Interval Training and Continuous Training on Cardiopulmonary Fitness and Exercise Tolerance of Patients with Heart Failure—A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 6761. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136761
Li D, Chen P, Zhu J. The Effects of Interval Training and Continuous Training on Cardiopulmonary Fitness and Exercise Tolerance of Patients with Heart Failure—A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(13):6761. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136761
Chicago/Turabian StyleLi, Daxin, Ping Chen, and Junying Zhu. 2021. "The Effects of Interval Training and Continuous Training on Cardiopulmonary Fitness and Exercise Tolerance of Patients with Heart Failure—A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 13: 6761. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136761