
Investigation of Four Clusters of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in Rwanda, 2020


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Identification
2.2. Epidemiological Investigations
3. Results
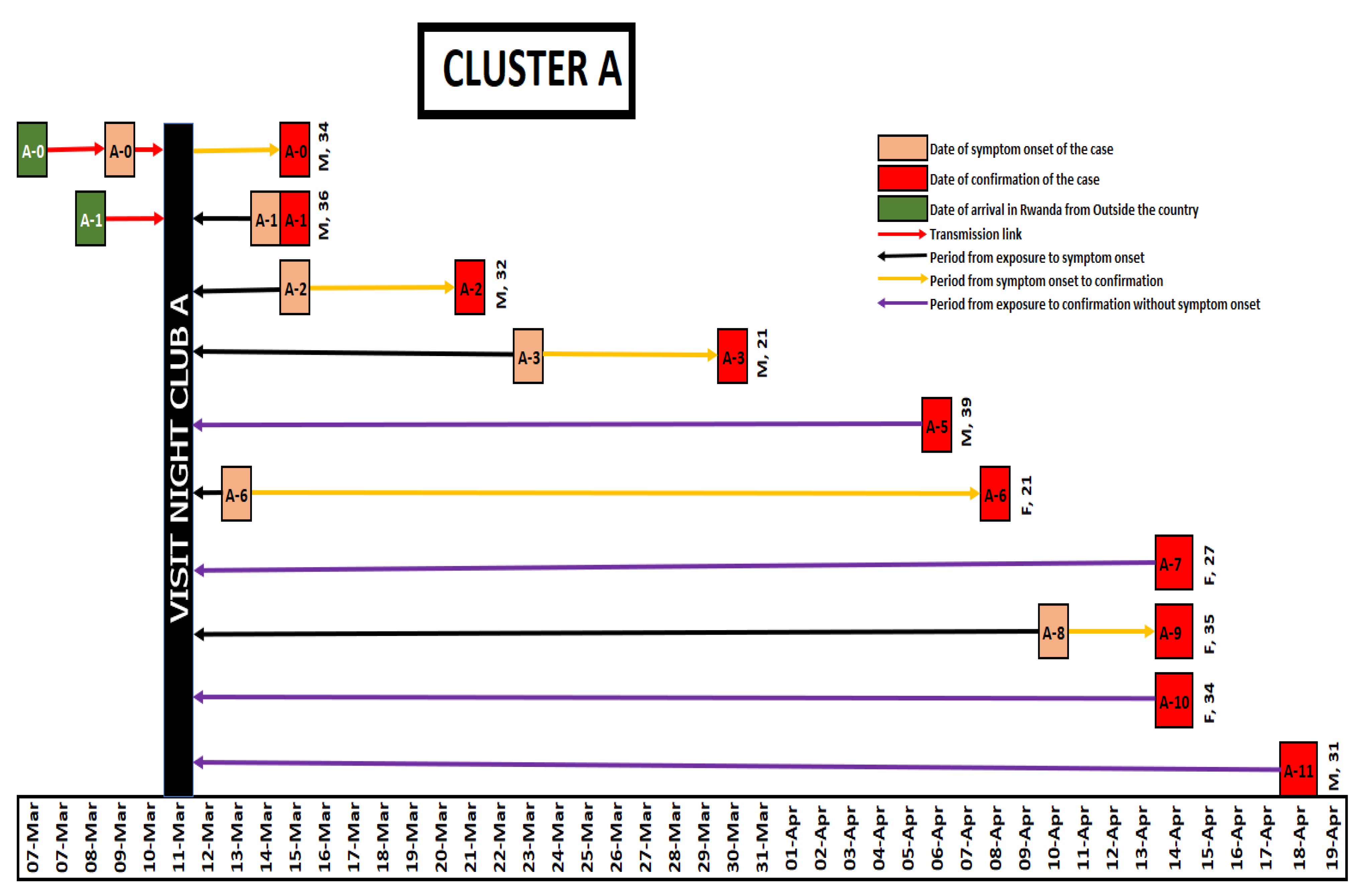
3.1. Cluster A
3.2. Cluster B
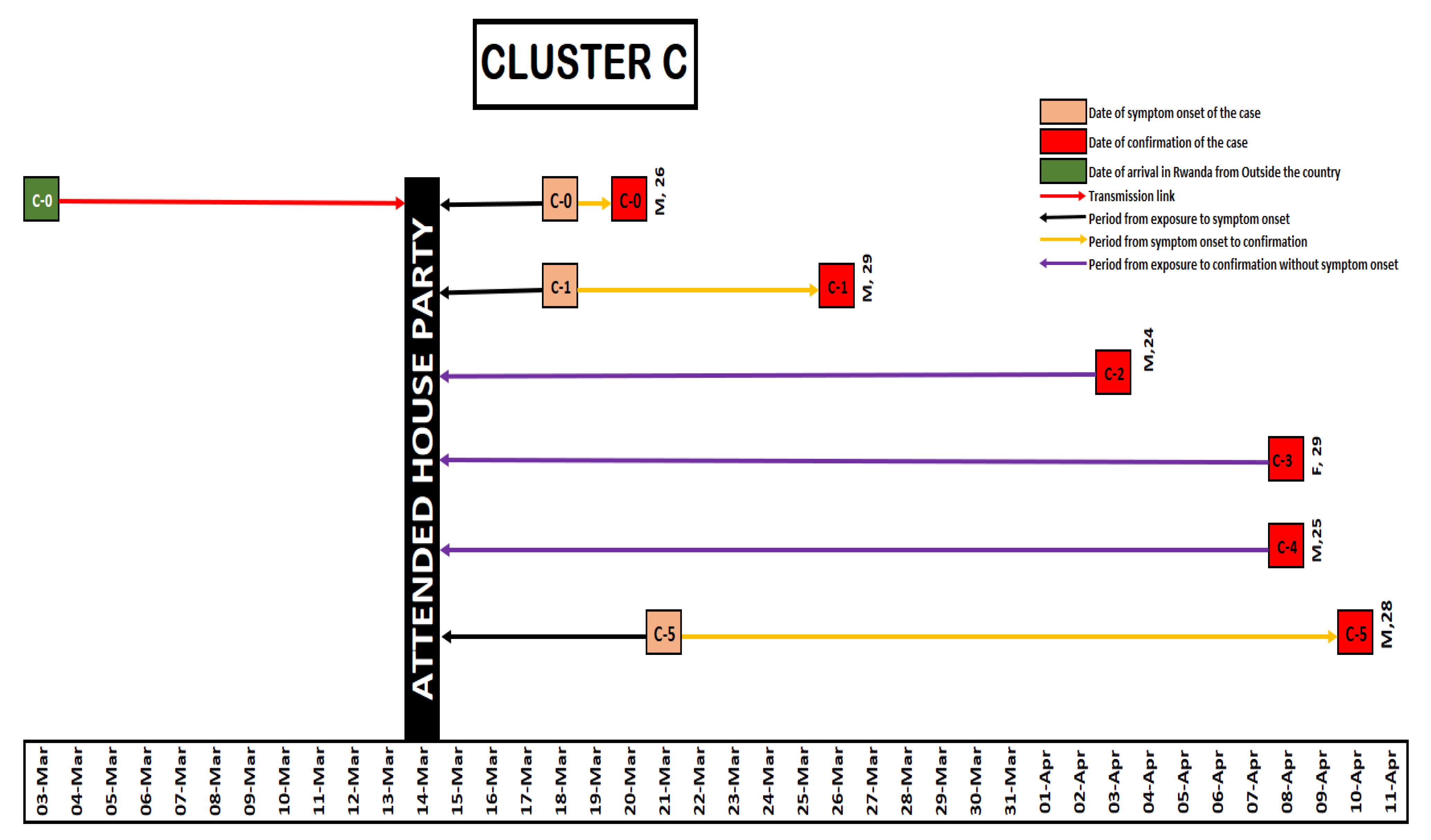
3.3. Cluster C
3.4. Cluster D
3.5. Epidemiological and Clinical Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Novel Coronavirus (2019-nCoV) Situation Report-1; WHO: Geneva, Switzerland, 2020; pp. 1–7. [Google Scholar]
- Ghinai, I.; McPherson, T.D.; Hunter, J.C.; Kirking, H.L.; Christiansen, D.; Joshi, K.; Rubin, R.; Morales-Estrada, S.; Black, S.R.; Pacilli, M.; et al. First known person-to-person transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in the USA. Lancet 2020, 395, 1137–1144. [Google Scholar] [CrossRef]
- Culp; William, C. Coronavirus Disease 2019/Situation Report-138. A A Pract. 2020, 14, e01218. [Google Scholar] [CrossRef] [PubMed]
- Lone, S.A.; Ahmad, A. COVID-19 pandemic—An African perspective. Emerg. Microbes Infect. 2020, 9, 1300–1308. [Google Scholar] [CrossRef] [PubMed]
- WHO Africa. First Case of COVID-19 Confirmed in Rwanda. 2020. p. 1. Available online: https://www.afro.who.int/news/first-case-covid-19-confirmed-rwanda (accessed on 10 June 2020).
- Nachega, J.B.; Atteh, R.; Ihekweazu, C.; Sam-Agudu, N.A.; Adejumo, P.; Nsanzimana, S.; Rwagasore, E.; Condo, J.; Paleker, M.; Mahomed, H.; et al. Contact tracing and the COVID-19 response in Africa: Best practices, Key Challenges, and lessons learned from Nigeria, Rwanda, South Africa, and Uganda. Am. J. Trop. Med. Hyg. 2021, 104, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Jing, Q.L.; Li, Y.G.; Ma, M.M.; Gu, Y.Z.; Li, K.; Ma, Y.; Wu, D.; Wu, Y.; Luo, L.; Zhang, Z.B. Contagiousness and secondary attack rate of 2019 novel coronavirus based on cluster epidemics of COVID-19 in Guangzhou. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 1623–1626. [Google Scholar] [PubMed]
- Migisha, R.; Kwesiga, B.; Mirembe, B.B.; Amanya, G.; Kabwama, S.N.; Kadobera, D.; Bulage, L.; Nsereko, G.; Wadunde, I.; Tindyebwa, T.; et al. Early cases of SARS-CoV-2 infection in Uganda: Epidemiology and lessons learned from risk-based testing approaches—March–April 2020. Glob. Health 2020, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Pung, R.; Chiew, C.J.; Young, B.E.; Chin, S.; Chen, M.I.; Clapham, H.E.; Cook, A.R.; Maurer-Stroh, S.; Toh, M.P.H.S.; Poh, C.; et al. Investigation of three clusters of COVID-19 in Singapore: Implications for surveillance and response measures. Lancet 2020, 395, 1039–1046. [Google Scholar] [CrossRef]
- Böhmer, M.M.; Buchholz, U.; Corman, V.M.; Hoch, M.; Katz, K.; Marosevic, D.V.; Böhm, S.; Woudenberg, T.; Ackermann, N.; Konrad, R.; et al. Investigation of a COVID-19 outbreak in Germany resulting from a single travel-associated primary case: A case series. Lancet Infect. Dis. 2020, 20, 920–928. [Google Scholar] [CrossRef]
- Kontou, P.I.; Braliou, G.G.; Dimou, N.L.; Nikolopoulos, G.; Bagos, P.G. Antibody tests in detecting SARS-CoV-2 infection: A meta-analysis. Diagnostics 2020, 10, 319. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number of Contacts Traced | Infected | Secondary Attack Rate |
|---|---|---|---|
| Clusters | N = 1035 | N = 36 | |
| Cluster A | 264 (25.5%) | 9 (25%) | 3.4% |
| Cluster B | 526 (50.8%) | 16 (44.4%) | 3.0% |
| Cluster C | 90 (8.7%) | 5 (13.8%) | 5.5% |
| Cluster D | 155 (15.0%) | 6 (16.6%) | 3.9% |
| Sex | N = 1035 | N = 36 | |
| Woman | 376 (36.3%) | 16 (44.4%) | 4.3% |
| Man | 659 (63.7%) | 20 (55.6%) | 3.0% |
| Age (years) | N = 1035 | N = 36 | |
| 0–9 | 36 (3.5%) | 1 (2.7%) | 2.7% |
| 10–19 | 42 (4.1%) | 4 (11.1%) | 9.5% |
| 20–29 | 379 (36.6%) | 16 (44.4%) | 4.2% |
| 30–39 | 538 (52.0%) | 13 (36.1%) | 2.4% |
| 40–49 | 6 (0.6%) | 1 (2.7%) | 16.7% |
| 50–59 | 34 (3.3%) | 1 (2.7%) | 2.9% |
| Type of contact | N = 1035 | N = 36 | |
| High risk | 236 (22.8%) | 24 (66.7%) | 10.2% |
| Low risk | 799 (77.2%) | 12 (33.3%) | 1.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nsekuye, O.; Rwagasore, E.; Muhimpundu, M.A.; El-Khatib, Z.; Ntabanganyimana, D.; Kamayirese, E.N.; Ruyange, L.; Umutoni, A.; Adeline, A.K.; Ntaganira, J.; et al. Investigation of Four Clusters of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in Rwanda, 2020. Int. J. Environ. Res. Public Health 2021, 18, 7018. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137018
Nsekuye O, Rwagasore E, Muhimpundu MA, El-Khatib Z, Ntabanganyimana D, Kamayirese EN, Ruyange L, Umutoni A, Adeline AK, Ntaganira J, et al. Investigation of Four Clusters of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in Rwanda, 2020. International Journal of Environmental Research and Public Health. 2021; 18(13):7018. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137018
Chicago/Turabian StyleNsekuye, Olivier, Edson Rwagasore, Marie Aime Muhimpundu, Ziad El-Khatib, Daniel Ntabanganyimana, Eric Noël Kamayirese, Laurent Ruyange, Angela Umutoni, Adeline Kabeja Adeline, Joseph Ntaganira, and et al. 2021. "Investigation of Four Clusters of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in Rwanda, 2020" International Journal of Environmental Research and Public Health 18, no. 13: 7018. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137018