
Knowledge, Attitudes and Practices toward Hepatitis B Virus Infection among Students of Medicine in Vietnam

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire
2.2. Definitions for Scoring Knowledge, Attitudes and Practices (KAP)
2.3. Data Collection and Analysis
2.4. Ethical Consideration
3. Results
3.1. Demographics of Survey Participants
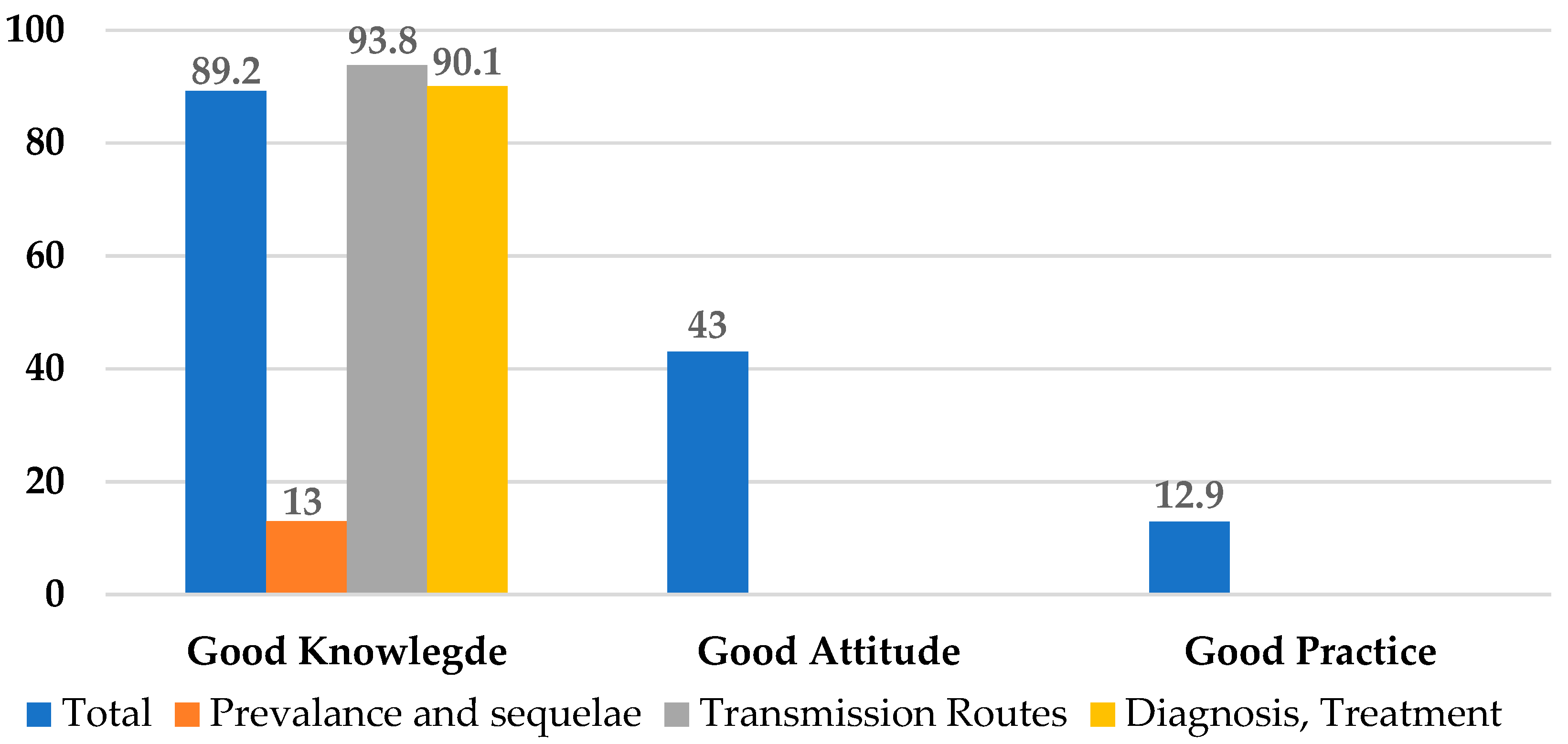
3.2. Knowledge about Hepatitis B Prevention, Screening and Treatment
3.3. Attitudes about Hepatitis B
3.4. HBV Preventive Practices
3.5. Knowledge, Attitudes and Practice Scores Associated Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Globocan International Agency for Reseach on Cancer; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- WHO Western Pacific Region Firm Action Is Needed to Eliminate Viral Hepatitis in Viet Nam. Available online: https://www.who.int/vietnam/news/detail/28-07-2017-firm-action-is-needed-to-eliminate-viral-hepatitis-in-viet-nam (accessed on 9 March 2021).
- André, F.E.; Zuckerman, A.J. Review: Protective Efficacy of Hepatitis B Vaccines in Neonates. J. Med. Virol. 1994, 44, 144–151. [Google Scholar] [CrossRef]
- Clements, C.J.; Baoping, Y.; Crouch, A.; Hipgrave, D.; Mansoor, O.; Nelson, C.B.; Treleaven, S.; van Konkelenberg, R.; Wiersma, S. Progress in the Control of Hepatitis B Infection in the Western Pacific Region. Vaccine 2006, 24, 1975–1982. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, D.P. Pediatric Experience with Recombinant Hepatitis B Vaccines and Relevant Safety and Immunogenicity Studies. Pediatr. Infect. Dis. J. 1993, 12, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.H.; Vu, M.H.; Nguyen, V.C.; Nguyen, L.H.; Toda, K.; Nguyen, T.N.; Dao, S.; Wannemuehler, K.A.; Hennessey, K.A. A Reduction in Chronic Hepatitis B Virus Infection Prevalence among Children in Vietnam Demonstrates the Importance of Vaccination. Vaccine 2014, 32, 217–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khosravanifard, B.; Rakhshan, V.; Najafi-Salehi, L.; Sherafat, S. Tehran Dentists’ Knowledge and Attitudes towards Hepatitis B and Their Willingness to Treat Simulated Hepatitis B Positive Patients. East Mediterr. Health J. 2014, 20, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Prüss-Ustün, A.; Rapiti, E.; Hutin, Y. Estimation of the Global Burden of Disease Attributable to Contaminated Sharps Injuries among Health-Care Workers. Am. J. Ind. Med. 2005, 48, 482–490. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Regional Office for the Western Pacific Hepatitis B Control through Immunization a Reference Guide; World Health Organization: Geneva, Switzerland, 2015; ISBN 978-92-9061-669-6. [Google Scholar]
- Pham, T.T.H.; Le, T.X.; Nguyen, D.T.; Luu, C.M.; Truong, B.D.; Tran, P.D.; Toy, M.; Bozkurt, S.; So, S. Knowledge, Attitudes and Medical Practice Regarding Hepatitis B Prevention and Management among Healthcare Workers in Northern Vietnam. PLoS ONE 2019, 14, e0223733. [Google Scholar] [CrossRef] [Green Version]
- Halboub, E.S.; Al-Maweri, S.A.; Al-Jamaei, A.A.; Tarakji, B.; Al-Soneidar, W.A. Knowledge, Attitudes, and Practice of Infection Control among Dental Students at Sana’a University, Yemen. J. Int. Oral Health 2015, 7, 15–19. [Google Scholar]
- Al-Shamiri, H.-M.; AlShalawi, F.-E.; AlJumah, T.-M.; AlHarthi, M.-M.; AlAli, E.-M.; AlHarthi, H.-M. Knowledge, Attitude and Practice of Hepatitis B Virus Infection among Dental Students and Interns in Saudi Arabia. J. Clin. Exp. Dent. 2018, 10, e54–e60. [Google Scholar] [CrossRef]
- Linh, G.H.N.; Son, N.; Minh, N.; Han, P. Knowledge, Attitude, Practice towards Hepatitis B Transmission Prevention of Students of Hai Phong University of Medicine and Pharmacy 2015. Vietnam J. Pre. Med. 2016, 14, 11–20. [Google Scholar]
- Ibrahim, N.; Idris, A. Hepatitis B Awareness among Medical Students and Their Vaccination Status at Syrian Private University. Hepat. Res. Treat. 2014, 2014, 131920. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Ahmed, S.M.; Khalid, M.M.; Siddiqui, S.H.; Merchant, A.A. Effect of Gender and Age on the Knowledge, Attitude and Practice Regarding Hepatitis B and C and Vaccination Status of Hepatitis B among Medical Students of Karachi, Pakistan. J. Pak. Med. Assoc. 2010, 60, 450–455. [Google Scholar]
- Abdela, A.; Woldu, B.; Haile, K.; Mathewos, B.; Deressa, T. Assessment of Knowledge, Attitudes and Practices toward Prevention of Hepatitis B Virus Infection among Students of Medicine and Health Sciences in Northwest Ethiopia. BMC Res. Notes 2016, 9. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Expanded Programme on Immunization. In Global Summary. Vaccine—Preventable Diseases: Monitoring System; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Ministry of Health National Guidelines for Hepatitis B Diagnosis and Treatment; Ministry of Health: Hanoi, Vietnam, 2014.
- Ghomraoui, F.A.; Alfaqeeh, F.A.; Algadheeb, A.S.; Al-alsheikh, A.S.; Al-Hamoudi, W.K.; Alswat, K.A. Medical Students’ Awareness of and Compliance with the Hepatitis B Vaccine in a Tertiary Care Academic Hospital: An Epidemiological Study. J. Infect. Public Health 2016, 9, 60–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuong, T.D.N.; Ngan, N.; Phan, H. Knowledge, Attitude and Practice of Hepatitis B Virus Infection among Health Care Workers in Hospitals of Quang Binh Province in 2012. Vietnam J. Prev. Med. 2016, 7, 47–54. [Google Scholar]
- Nagandla, K.; Kumar, K.; Bhardwaj, A.; Muthalagan, D.A.; Yhmin, C.; Lun, L.W.; Shi, W.W.; Razak, N.I.B.A. Prevalence of Needle Stick Injuries and Their Underreporting among Healthcare Workers in the Department of Obstetrics and Gynaecology. Int. Arch. Med. 2015, 8. [Google Scholar] [CrossRef] [Green Version]
- Schweitzer, A.; Horn, J.; Mikolajczyk, R.T.; Krause, G.; Ott, J.J. Estimations of Worldwide Prevalence of Chronic Hepatitis B Virus Infection: A Systematic Review of Data Published between 1965 and 2013. Lancet 2015, 386, 1546–1555. [Google Scholar] [CrossRef]
- Askarian, M.; Malekmakan, L. The Prevalence of Needle Stick Injuries in Medical, Dental, Nursing and Midwifery Students at the University Teaching Hospitals of Shiraz, Iran. Indian J. Med. Sci. 2006, 60, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Bhattarai, S.; Smriti, K.C.; Pradhan, P.M.S.; Lama, S.; Rijal, S. Hepatitis B Vaccination Status and Needle-Stick and Sharps-Related Injuries among Medical School Students in Nepal: A Cross-Sectional Study. BMC Res. Notes 2014, 7, 774. [Google Scholar] [CrossRef] [Green Version]
- Shindano, T.A.; Bahizire, E.; Fiasse, R.; Horsmans, Y. Knowledge, Attitudes, and Practices of Health-Care Workers About Viral Hepatitis B and C in South Kivu. Am. J. Trop. Med. Hyg. 2017, 96, 400–404. [Google Scholar] [CrossRef] [Green Version]
- Pathoumthong, K.; Khampanisong, P.; Quet, F.; Latthaphasavang, V.; Souvong, V.; Buisson, Y. Vaccination Status, Knowledge and Awareness towards Hepatitis B among Students of Health Professions in Vientiane, Lao PDR. Vaccine 2014, 32. [Google Scholar] [CrossRef]
- Childs, L.; Roesel, S.; Tohme, R.A. Status and Progress of Hepatitis B Control through Vaccination in the South-East Asia Region, 1992–2015. Vaccine 2018, 36, 6–14. [Google Scholar] [CrossRef]
- World Health Organization. Safety of Quinvaxem (DTwP-HepB-Hib) Pentavalent Vaccine; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- An, D.T.M.; Lee, J.-K.; Minh, A.D.; Trang, N.T.H.; Huong, N.T.T.; Nam, Y.-S.; Van Dung, D. Timely Immunization Completion among Children in Vietnam from 2000 to 2011: A Multilevel Analysis of Individual and Contextual Factors. Glob. Health Action 2016, 9, 29189. [Google Scholar] [CrossRef]
- Eguchi, H.; Wada, K. Knowledge of HBV and HCV and Individuals’ Attitudes Toward HBV- and HCV-Infected Colleagues: A National Cross-Sectional Study among a Working Population in Japan. PLoS ONE 2013, 8, e76921. [Google Scholar] [CrossRef] [Green Version]
- Wada, K.; Smith, D.R.; Ishimaru, T. Reluctance to Care for Patients with HIV or Hepatitis B/C in Japan. BMC Pregnancy Childbirth 2016, 16, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishimaru, T.; Wada, K.; Arphorn, S.; Smith, D.R. Barriers to the Acceptance of Work Colleagues Infected with Hepatitis B and Hepatitis C in Japan. J. Occup. Health 2016, 58, 269–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokaya, J.; McNaughton, A.L.; Burbridge, L.; Maponga, T.; O’Hara, G.; Andersson, M.; Seeley, J.; Matthews, P.C. A Blind Spot? Confronting the Stigma of Hepatitis B Virus (HBV) Infection—A Systematic Review. Wellcome Open Res. 2018, 3. [Google Scholar] [CrossRef] [Green Version]
- Ishimaru, T.; Wada, K.; Hoang, H.T.X.; Bui, A.T.M.; Nguyen, H.D.; Le, H.; Smith, D.R. Nurses’ Willingness to Care for Patients Infected with HIV or Hepatitis B/C in Vietnam. Environ. Health Prev. Med. 2017, 22, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akazong, E.; Tume, C.; Njouom, R.; Ayong, L.; Fondoh, V.; Kuiate, J.-R. Knowledge, Attitude and Prevalence of Hepatitis B Virus among Healthcare Workers: A Cross-Sectional, Hospital-Based Study in Bamenda Health District, NWR, Cameroon. BMJ Open 2020, 10, e031075. [Google Scholar] [CrossRef] [Green Version]
- Mansour-Ghanaei, R.; Joukar, F.; Souti, F.; Atrkar-Roushan, Z. Knowledge and Attitude of Medical Science Students toward Hepatitis B and C Infections. Int. J. Clin. Exp. Med. 2013, 6, 197–205. [Google Scholar]


{kind=link}
| Respondents’ Demographics | n | % | |
|---|---|---|---|
| Age | Mean: 23.7 (SD 0.9, Range 21–30) | ||
| Gender | Male | 910 | 45.5 |
| Female | 1090 | 54.4 | |
| Medical school location in Vietnam (Region) | North | 1000 | 50.0 |
| Central | 250 | 12.5 | |
| South | 750 | 37.5 | |
| Medical school year | 5th year | 1250 | 62.5 |
| 6th (final) year | 750 | 37.5 | |
| Have you been tested for hepatitis B? | No | 315 | 15.8 |
| Yes | 1685 | 84.2 | |
| Positive | 83 | 4.9 | |
| Negative | 1581 | 93.8 | |
| Unknown | 21 | 1.3 | |
| Did you receive the hepatitis B vaccine? | Yes | 1678 | 83.9 |
| No | 230 | 11.5 | |
| Unknown | 92 | 4.6 | |
| Have you encountered any CHB patient before? | Yes | 1885 | 94.3 |
| No | 115 | 5.8 | |
| Questions | Correct Answers | |
|---|---|---|
| n | % | |
| Prevalence and Sequelae | ||
| A4. What percentage of the Vietnam population has chronic hepatitis B (CHB)? | 783 | 39.2 |
| A5. How did most people who have CHB in Vietnam get infected? | 704 | 35.2 |
| A6. Which age group is most likely to develop CHB after the initial infection? | 890 | 44.5 |
| A7. What are the consequences of chronic hepatitis B? | 1767 | 88.4 |
| A52. Without proper monitoring and treatment, what is the chance a patient would die of CHB complications? | 414 | 20.7 |
| Transmission Routes | ||
| A8. Can hepatitis B be transmitted through handshake? | 1949 | 97.5 |
| A9. Can hepatitis B be transmitted through unprotected sex? | 1936 | 96.8 |
| A10. Can hepatitis B be transmitted through blood transfusion? | 1933 | 96.7 |
| A11. Can hepatitis B be transmitted through sneezing or coughing? | 1898 | 94.9 |
| A12. Can hepatitis B be transmitted through from mother to child at birth? | 1933 | 96.7 |
| A13. Can hepatitis B be transmitted through sharing food or utensils? | 1729 | 86.5 |
| Prevention | ||
| Prevention Measures | ||
| A14. Can cleaning and cooking food thoroughly prevent HBV transmission? | 1501 | 86.5 |
| A15. Can the hepatitis B vaccine prevent HBV transmission? | 1949 | 97.5 |
| A16. Can HBV transmission be prevented by not reusing or sharing needles/syringes? | 1945 | 97.3 |
| A17. Can HBV transmission be prevented by avoid sharing food/utensils or eating with a person with chronic HBV? | 1600 | 80.0 |
| A18. Can using a condom prevent HBV transmission? | 1918 | 95.9 |
| A19.What is the most effective preventive measure for infants born to mothers with chronic HBsAg? | 1475 | 73.8 |
| A21. Who needs the hepatitis B vaccine? | 1881 | 94.1 |
| A23. Prevention of mother-to-child transmission | 1712 | 85.6 |
| A24. The first dose of hepatitis B vaccine for baby | 1823 | 91.2 |
| A33. Is it necessary to have sharp-proof containers at clinics for disposing of needles and sharp objects? | 1910 | 95.5 |
| What would you do to prevent needle-stick injury? | ||
| A30. Wash hands with soap or disinfectant after each clinical procedure? | 1694 | 84.7 |
| A31. Recap needle with two hands after use and discard immediately in a sharp-proof container | 1131 | 56.6 |
| A32. Do not recap needle and discard immediately in a sharp-proof container | 1409 | 70.5 |
| Diagnosis and Treatment | ||
| Who should be tested for hepatitis B? | ||
| A35. Pregnant women should be tested for hepatitis B | 1906 | 95.3 |
| A36. HIV-infected people should be tested for hepatitis B | 1902 | 95.1 |
| A37. Men who have sex with men (MSM) should be tested for hepatitis B | 1875 | 93.8 |
| A38. Family members of those who have hepatitis B should be tested for hepatitis B | 1911 | 95.6 |
| A56. Serum HBsAg test for identification of patients infected with hepatitis B virus | 1777 | 88.9 |
| A57. What test should be used to identify immunity against the hepatitis B virus? | 1433 | 71.7 |
| Diagnosis | ||
| A40. What is the symptom most patients with chronic hepatitis B present? | 669 | 33.5 |
| A41. What are the criteria for indicating treatment in patients with CHB? | 1645 | 82.3 |
| A55. When should infants born to mothers with CHB be evaluated for HBsAg status? | 123 | 6.2 |
| Treatment | ||
| A42. There is no cure, but there are effective medications to manage and control the disease | 1387 | 69.4 |
| Treatment goal: What are the treatment goals for CHB patients? | ||
| A43. Inhibit the replication of the hepatitis B virus | 1843 | 92.2 |
| A44. Prevent disease progression of disease, particularly liver cirrhosis and liver cancer | 1938 | 96.9 |
| A45. Prevent mother-to-child transmission (MTCT) | 1927 | 96.4 |
| A46. Prevent flare of hepatitis B | 1855 | 92.8 |
| Treatment principles | ||
| A47. Is it true that Nucleos(t)ide Analogs (NAs) are a recommended first-line treatment for CHB? | 1349 | 67.5 |
| A48. Is treatment of CHB with NAs long term, possibly even lifetime? | 1528 | 76.4 |
| A49. Do patients need to strictly adhere to the treatment of CHB? | 1923 | 96.2 |
| A50. Do you think that all patients with chronic HBV need to be treated immediately? | 1397 | 69.9 |
| A51. Should all CHB patients be monitored and tested regardless of treatment status? | 1830 | 91.5 |
| Questions | Answered Yes | |
|---|---|---|
| n | % | |
| A20. Are you confident in counseling patients about prevention of HBV? | 1358 | 67.9 |
| A22. Do you think that the hepatitis B vaccine is safe? | 1220 | 61.0 |
| A25. Do you think it is necessary to vaccinate newborns for hepatitis B at birth? | 1914 | 95.7 |
| A53. Are you confident in ordering laboratory tests to monitor CHB patients? | 1229 | 61.5 |
| A54. Are you confident in prescribing treatment for a patient with chronic hepatitis B? | 550 | 27.5 |
| A58. Are you confident in ordering diagnosis tests for patients with chronic HBV? | 1279 | 63.9 |
| A59. Would you have any concerns having casual contact or working together with a chronic HBV patient in the same office? | 1185 | 59.3 |
| A60. Would you have any concerns sharing food or utensils with a CHB? | 1303 | 65.2 |
| Questions | Answered Yes | |
|---|---|---|
| n | % | |
| A28. Did you get the hepatitis B vaccine before entering practicum at teaching hospitals? | 402 | 20.1 |
| A29. Did you get tested for HBV before entering practicum at teaching hospitals? | 499 | 24.9 |
| A34. Do you consistently wear gloves when administrating injections or performing medical procedures to patients? | 1373 | 68.7 |
| Hepatitis B | Number of Questions | Mean | SD (Range) | Percentage of Maximum Score |
|---|---|---|---|---|
| Knowledge | 43 | 34.1 | 4.2 (7–41) | 79.3% |
| Prevalence and sequelae | 5 | 2.3 | 1.1 (0–5) | 46.0% |
| Transmission routes | 6 | 5.7 | 0.8 (0–6) | 95.0% |
| Prevention | 13 | 10.9 | 1.7 (2–13) | 83.8% |
| Diagnosis, treatment | 19 | 7.9 | 1.4 (0–9) | 41.6% |
| Attitude | 8 | 5.0 | 1.8 (0–8) | 62.5% |
| Practice | 3 | 1.1 | 0.9 (0–3) | 36.7% |
| Good Knowledge (n = 1784) | OR (95%CI) | p * | AOR (95%CI) | p ** | |
|---|---|---|---|---|---|
| Gender (n = 2000) | |||||
| Male (n= 910) | 785 (86.3) | ||||
| Female (n = 1090) | 999 (91.7) | 1.74 1.31–2.33 | <0.001 | 1.76 1.28–2.41 | <0.001 |
| Year of Education (n = 2000) | |||||
| 5th (n = 1250) | 1151 (92.1) | 2.15 1.61–2.86 | <0.001 | 2.95 2.02–4.31 | <0.001 |
| 6th (n = 750) | 633 (84.4) | ||||
| Region (n = 2000) | |||||
| North (n = 1000) | 873 (87.3) | ||||
| Middle (n = 250) | 235 (94.0) | 2.27 1.30–3.97 | 0.004 | 2.08 1.41–3.07 | <0.001 |
| South (n = 750) | 676 (90.1) | 1.33 0.98–1.80 | 0.07 | 1.07 0.58–1.96 | 0.83 |
| Test HBV before (n = 2000) | |||||
| Yes (n = 1685) | 1548 (91.9) | 3.78 2.78–5.15 | <0.001 | 1.06 0.56–2.01 | 0.85 |
| No (n = 315) | 236 (74.9) | ||||
| Status of HBV (n = 2000) | |||||
| Positive (n = 115) | 94 (81.7) | 0.37 0.22–0.61 | <0.001 | 0.60 0.34–1.08 | 0.09 |
| Negative (n = 1610) | 1487 (92.4) | ||||
| Unknown (n = 275) | 203 (73.8) | 0.23 0.16–0.32 | <0.001 | 0.35 0.18–0.69 | 0.002 |
| Got HBV vaccine before (n = 2000) | |||||
| Yes (n = 1678) | 1551 (92.4) | 4.31 3.05–6.09 | <0.001 | 2.39 1.58–3.61 | <0.001 |
| No (n = 230) | 170 (73.9) | ||||
| Unknown (n = 92) | 63 (68.5) | 0.77 0.45–1.30 | 0.33 | 0.72 0.39–1.29 | 0.27 |
| Met a hepatitis B patient before (n = 2000) | |||||
| Yes (n = 1885) | 330 (17.5) | 10.23 6.86–15.3 | <0.001 | 8.09 5.20–12.59 | <0.001 |
| No (n = 115) | 18 (59.1) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, T.T.L.; Pham, T.T.H.; So, S.; Hoang, T.H.V.; Nguyen, T.T.U.; Ngo, T.B.; Nguyen, M.P.; Thai, Q.H.; Nguyen, N.K.; Le Ho, T.Q.A.; et al. Knowledge, Attitudes and Practices toward Hepatitis B Virus Infection among Students of Medicine in Vietnam. Int. J. Environ. Res. Public Health 2021, 18, 7081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137081
Nguyen TTL, Pham TTH, So S, Hoang THV, Nguyen TTU, Ngo TB, Nguyen MP, Thai QH, Nguyen NK, Le Ho TQA, et al. Knowledge, Attitudes and Practices toward Hepatitis B Virus Infection among Students of Medicine in Vietnam. International Journal of Environmental Research and Public Health. 2021; 18(13):7081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137081
Chicago/Turabian StyleNguyen, Thi Thuy Linh, Thi Thanh Hang Pham, Samuel So, Thi Hai Van Hoang, Thi To Uyen Nguyen, Thanh Binh Ngo, Minh Phuong Nguyen, Quang Hung Thai, Ngoc Khoi Nguyen, Thi Quynh Anh Le Ho, and et al. 2021. "Knowledge, Attitudes and Practices toward Hepatitis B Virus Infection among Students of Medicine in Vietnam" International Journal of Environmental Research and Public Health 18, no. 13: 7081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137081