
Association between Depressed Mood and Sleep Duration among Various Ethnic Groups—The Helius Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethnicity
2.3. Depressive Symptoms
2.4. Sleep Duration
2.5. Other Measurements
2.6. Data Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Association between Depressed Mood and Short Sleep Duration
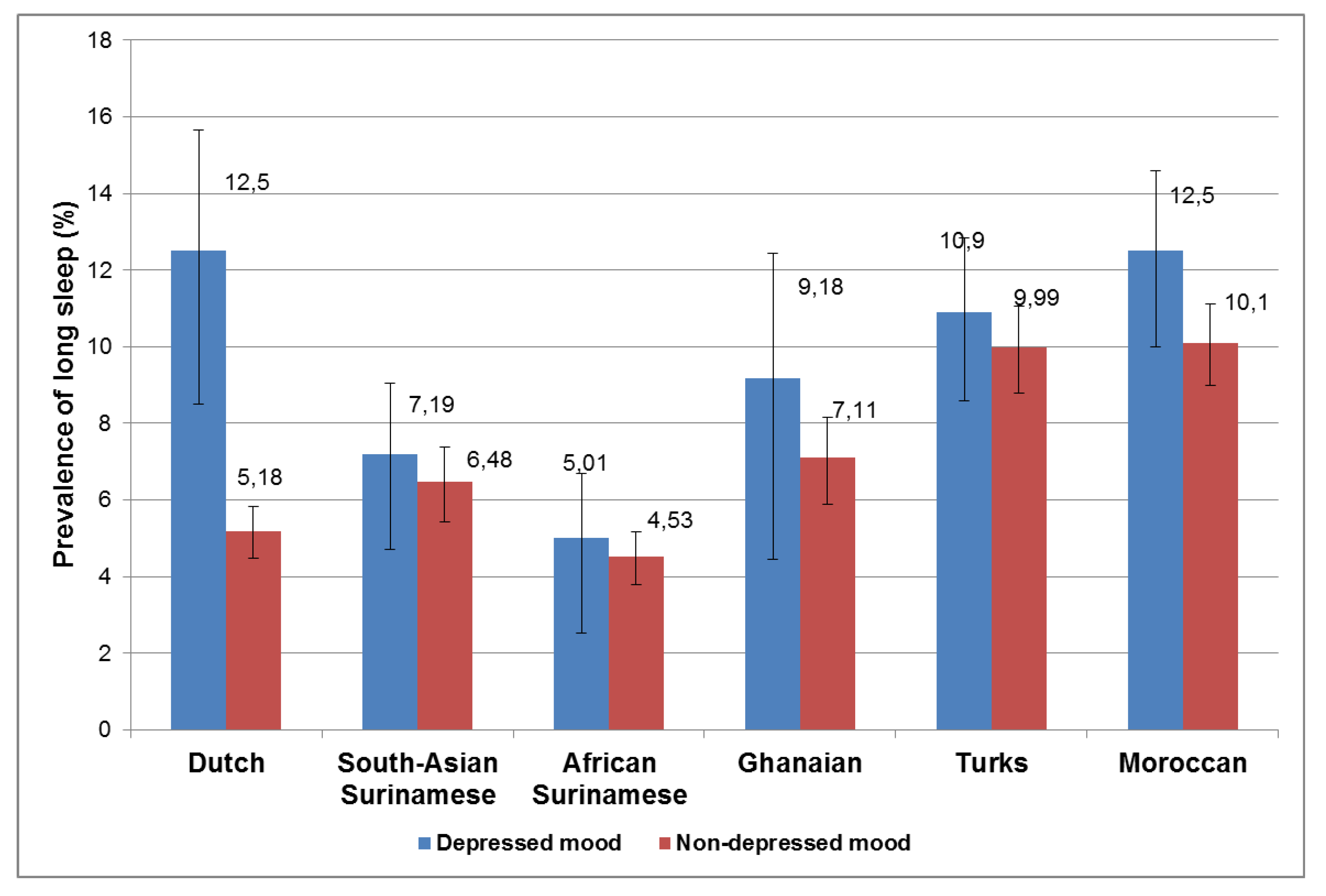
3.3. Association between Depressed Mood and Long Sleep Duration
3.4. The Extent to Which Depressed Mood Accounted for the Prevalence of Short and Long Sleep Duration among Ethnic Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Torres, C. Mental health: The great depression. Nature 2014, 515, 179. [Google Scholar]
- Depression Fact Sheet 2016. Available online: http://www.who.int/mediacentre/factsheets/fs369/en/ (accessed on 28 July 2016).
- Lépine, J.-P.; Briley, M. The increasing burden of depression. Neuropsychiatr Dis Treat. 2001, 7, 3–7. [Google Scholar]
- Patten, C.A.; Choi, W.S.; Jillin, J.C. Depressive symptoms and cigarette smoking predict development of sleep problems in US adolescents. Paediatrics 2000, 106, E23. [Google Scholar] [CrossRef] [Green Version]
- Kaneita, Y.; Ohida, T.; Uchiyama, M.; Takemura, S.; Kawahara, K.; Yokoyama, E.; Miyake, T.; Harano, S.; Suzuki, K.; Fujita, T. The relationship between depression and sleep disturbances: A Japanese nationwide general population survey. J. Clin. Psychiatry 2006, 67, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Matushita, M.; Koyama, A.; Ushijima, H.; Mikami, A.; Katsumata, Y.; Kikuchi, Y.; Ichimi, N.; Jono, T.; Fujise, N.; Ikeda, M. Sleep duration and its association with sleepiness and depression in “ronin-sei” preparatory school students. Asian J. Psychiatry 2014, 9, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Tsuno, N.; Besset, A.; Ritchie, K. Sleep and depression. J. Clin. Psychiatry 2005, 66, 1254–1269. [Google Scholar] [CrossRef]
- Benca, R.M.; Peterson, M.J. Insomnia and depression. Sleep Med. 2008, 1, S3–S9. [Google Scholar] [CrossRef]
- Sivertsen, B.; Harvey, A.G.; Lundervold, A.J. Sleep problems and depression in adolescence: Results from a large population-based study of Norwegian adolescents aged 16-18 years. Eur. Child Adolesc. Psychiatry 2014, 8, 681–689. [Google Scholar] [CrossRef]
- Carney, C.E.; Segal, Z.V.; Edinger, J.D. A comparison of rates of residual insomnia symptoms following pharmacotherapy or cognitive-behavioral therapy for major depressive disorder. J. Clin. Psychiatry 2007, 68, 254–260. [Google Scholar] [CrossRef]
- Van der Wurff, F.B.; Beekman, A.T.; Dijkshoorn, H.; Spiyker, J.A.; Smits, C.H.M.; Stek, M.L.; Verhoef, A. Prevalence and risk-factors of depression in elderly migrants in the Netherlands. J. Affect. Disord. 2004, 83, 33–41. [Google Scholar] [CrossRef]
- Ikram, U.Z.; Snijder, M.B.; Fasseart, T.J.; Schene, A.H.; Kunst, A.E.; Stronks, K. The contribution of perceived ethnic discrimination to the prevalence of depression. Eur. J. Public Health 2015, 25, 243–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anujuo, K.; Stronks, K.; Snijder, M.B.; Jean-Louis, G.; Ogedegbe, G.; Agyemang, C. Ethnic differences in self-reported sleep duration in the Netherlands—The HELIUS Study. Sleep Med. 2015, 15, 1115–1121. [Google Scholar] [CrossRef]
- Stronks, K.; Snijder, M.B.; Peters, R.J.; Prins, M.; Schene, A.H.; Zwinderman, A.H. Unravelling the impact of ethnicity on health in Europe: The HELIUS study. BMC Public Health 2013, 13, 402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snijder, M.B.; Galenkamp, H.; Prins, M.; Derks, E.M.; Peters, R.J.G.; Zwinderman, A.H.; Stronks, K. Cohort profile: The Healthy Life in an Urban Setting (HELIUS) study in Amsterdam, the Netherlands. BMJ Open 2017, 7, e017873. [Google Scholar] [CrossRef] [Green Version]
- Stronks, K.; Kulu-Glasgow, I.; Agyemang, C. The utility of ‘country of birth’ for the classification of ethnic groups in health research: The Dutch experience. Ethn Health 2009, 14, 255–269. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Lowe, B. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: A systematic review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef]
- Galenkamp, H.; Stronks, K.; Snijder, M.; Derks, E.M. The PHQ-9 was measurement invariant across six ethnic groups: The HELIUS study. BMC Psychiatry 2017, 17, 349. [Google Scholar] [CrossRef] [Green Version]
- Watson, N.F.; Badr, M.S.; Belenky, G.; Bliwise, D.L.; Buxton, O.M.; Buysse, D.; Dinges, D.F.; Gangwisch, J.; Grandner, M.A.; Kushida, D.; et al. Recommended amount of sleep for a healthy adult: A joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep 2015, 6, 843–844. [Google Scholar] [CrossRef]
- World Health Organization. Collaborating Centre for Drug Statistics Methodology Guidelines for ATC Classification and DDD Assignments 2014; WHO: Oslo, Norway, 2013. [Google Scholar]
- Williamson, D.F. The population attributable fraction and confounding: Buyer beware. Int. J. Clin. Pract. 2010, 64, 1019–1023. [Google Scholar] [CrossRef]
- Rockhill, B.; Newman, B.; Weinber, C. Use and misuse of population attributable fractions. Am. J. Public Health 1998, 88, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Dahl, R.E. The regulation of sleep and arousal: Development and Psychopathology. Dev. Psychopathol. 1996, 8, 3–27. [Google Scholar] [CrossRef]
- Lok, A.; Mocking, R.J.; Ruhé, H.G.; Visser, I.; Koeter, M.W.; Assies, J.; Bockting, C.L.; Olff, M.; Schene, A.H. Longitudinal hypothalamic-pituitary-adrenal axis trait and state effects in recurrent depression. Psychoneuroendocrinology 2012, 37, 892–902. [Google Scholar] [CrossRef] [PubMed]
- Gold, P.W. The organization of the stress system and its dysregulation in depressive illness. Mol. Psychiatry 2015, 20, 32–47. [Google Scholar] [CrossRef] [Green Version]
- Antypa, N.; Verkuil, B.; Molendijk, M.; Schoevers, R.; Pennins, B.W.J.H.; Van der Does, D. Association between chronotypes and psychological vulnerability factors of depression. Chronobiol. Int. 2017, 34, 1125–1135. [Google Scholar] [CrossRef]
- Levenson, J.C.; Benca, R.M.; Rumble, M.E. Sleep related cognitions in individuals with symptoms of insomnia and depression. J. Clin. Sleep. Med. 2015, 11, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Luca, A.; Luca, M.; Calandra, C. Sleep disorders and depression: Brief review of the literature, case report, and nonpharmacologic interventions for depression. Clin. Interv. Aging 2013, 8, 1033–1039. [Google Scholar] [PubMed] [Green Version]
- Sadeh, A.; Keinan, G.; Daon, K. Effects of stress on sleep: The moderating role of coping style. Health Psychol. 2004, 23, 542–545. [Google Scholar] [CrossRef] [Green Version]
- Watson, N.F.; Harden, K.P.; Buchward, D.; Vitiello, M.V.; Pack, A.I.; Strachan, E.; Goldberg, J. Sleep duration and depressive symptoms: A gene-environment interaction. Sleep 2014, 35, 351–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Dutch | South-Asian Surinamese | African Surinamese | Ghanaians | Turks | Moroccans | |
|---|---|---|---|---|---|---|
| n = 4540 | n = 2992 | n = 4052 | n = 2192 | n = 3494 | n = 3802 | |
| Age (years) | 46.2 (45.7–46.6) | 45.5 (45.0–46.0) | 47.9 (47.6–48.3) | 44.7 (44.3–45.2) | 40.4 (39.9–40.8) | 40.4 (40.0–40.8) |
| Men (%) | 45.8 (44.4–47.3) | 45.3 (43.5–47.1) | 39.0 (37.5–40.5) | 39.4 (37.3–41.4) | 45.4 (43.7–47.0) | 38.9 (37.4–40.5) |
| Sleep duration (hours) | 7.3 (7.24, 7.29) | 6.8 (6.79, 6.89) | 6.6 (6.6, 6.7) | 6.8 (6.71, 6.83) | 7.1 (7.10, 7.19) | 7.2 (7.12, 7.21) |
| Short sleep (% yes) | 16.0 (14.9–17.1) | 38.3 (36.6–40.1) | 45.0 (43.5–46.5) | 42.9 (40.9–45.0) | 28.2 (26.8–29.7) | 25.9 (24.5–27.3) |
| Long sleep (% yes) | 5.7 (5.1–6.4) | 6.61 (5.77–7.55) | 4.60 (3.99–5.28) | 7.25 (6.25–8.40) | 10.2 (9.29–11.3) | 10.7 (9.79–11.7) |
| Marital status | ||||||
| Married (% yes) | 37.8 (36.4–39.2) | 34.4 (32.7–36.1) | 18.4 (17.2–19.6) | 18.2 (16.7–19.8) | 61.1 (59.5–62.7) | 58.5 (56.9–60.1) |
| Living together (%yes) | 20.0 (18.9–21.2) | 10.2 (9.16–11.3) | 10.7 (9.84–11.7) | 18.4 (16.8–20.0) | 3.69 (3.12–4.37) | 2.83 (2.35–3.41) |
| Single (% yes) | 32.3 (30.9–33.7) | 33.0 (31.3–34.7) | 53.6 (52.1–55.2) | 32.8 (30.9–34.8) | 21.1 (19.8–22.5) | 26.0 (24.6–27.4) |
| Widowed (% yes) | 7.79 (7.04–8.60) | 18.9 (17.6–20.4) | 14.9 (13.8–16.0) | 28.2 (26.4–30.1) | 11.3 (10.3–12.3) | 10.4 (9.47–11.4) |
| Divorced (% yes) | 1.91 (1.55–2.36) | 3.02 (2.45–3.69) | 1.56 (1.23–1.99) | 0.98 (0.64–1.48) | 2.35 (1.92–2.93) | 1.77 (1.39–2.24) |
| Depressed mood (%yes) | 7.2 (6.5–8.0) | 18.5 (17.1–19.9) | 10.7 (9.79–11.7) | 9.0 (7.9–10.2) | 23.1 (21.7–24.5) | 20.8 (19.5–22.1) |
| Educational level | ||||||
| 1st and 2nd category (%) | 17.5 (16.4–18.6) | 47.8 (45.9–49.5) | 41.3 (39.7–42.8) | 68.5 (66.5–70.3) | 56.4 (54.8–58.0) | 48.9 (47.3–50.5) |
| 3rd category (%) | 21.4 (20.6–23.1) | 29.2 (27.6–30.9) | 35.8 (34.3–37.2) | 25.3 (23.5–27.1) | 28.5 (27.1–30.0) | 33.6 (32.1–35.1) |
| 4th category (%) | 60.7 (59.2–62.1) | 22.9 (21.5–24.5) | 22.9 (21.7–23.4) | 6.27 (5.33–7.36) | 15.0 (13.9–16.3) | 17.5 (16.4–18.8) |
| Occupation | ||||||
| Elementary (%) | 1.78 (1.42–2.22) | 10.8 (9.64–11.9) | 6.97 (6.19–7.83) | 63.6 (61.4–65.7) | 19.7 (18.2–21.2) | 17.9 (16.5–19.3) |
| Lower (%) | 15.1 (14.1–16.2) | 34.9 (33.2–36.8) | 35.2 (33.7–36.7) | 23.4 (21.6–25.4) | 40.8 (38.9–42.7) | 34.6 (32.9–36.4) |
| Middle (%) | 23.4 (22.2–24.7) | 31.1 (29.3–32.9) | 35.5 (33.9–37.1) | 9.02 (7.81–10.4) | 24.6 (22.9–26.2) | 28.9 (27.2–30.6) |
| Higher (%) | 38.7 (37.2–40.1) | 17.9 (16.6–19.5) | 19.5 (18.2–20.8) | 2.94 (2.27–3.79) | 10.8 (9.70–12.0) | 15.5 (14.2–16.9) |
| Scientific (%) | 20.9 (19.8–22.2) | 5.19 (4.41–6.10) | 2.85 (2.36–3.44) | 0.10 (0.64–1.56) | 4.11 (3.42–4.93) | 3.12 (2.53–3.83) |
| Current smoker (%yes) | 24.7 (23.4–25.9) | 28.4 (26.8–30.0) | 31.4 (29.9–32.8) | 4.54 (3.75–5.48) | 34.2 (32.6–35.8) | 13.5 (12.4–14.6) |
| Alcohol intake (%yes) | 90.9 (90.1–91.8) | 56.4 (54.6–58.2) | 68.1 (66.7–69.5) | 47.7 (46.1–50.2) | 22.6 (21.3–24.0) | 7.33 (6.55–8.20) |
| Psychotropic (% yes) | 7.02 (6.37–7.87) | 6.77 (5.93–7.73) | 4.74 (4.13–5.44) | 2.94 (2.31–3.72) | 7.68 (6.85–8.60) | 5.44 (4.76–6.20) |
| Dutch n = 4540 | South-Asian Surinamese n = 2992 | African Surinamese n = 4052 | Ghanaians n = 2192 | Turks n = 3494 | Moroccans n = 3802 | |
|---|---|---|---|---|---|---|
| OR (95%CI) | OR (95%CI) | OR (95%CI) | OR (95%CI) | OR (95%CI) | OR (95%CI) | |
| Short sleep (<7 h/night) | ||||||
| Model 1 | 2.8 (2.2–3.7) | 2.3 (1.9–2.8) | 2.3 (1.9–2.8) | 1.9 (1.4–2.6) | 2.5 (2.1–2.9) | 2.4 (2.0–2.8) |
| Model 2 | 2.4 (1.9–3.2) | 2.3 (1.9–2.8) | 2.2 (1.8–2.8) | 1.9 (1.4–2.6) | 2.5 (2.1–2.9) | 2.4 (2.0–2.8) |
| Model 3 | 2.5 (1.9–3.2) | 2.2 (1.8–2.7) | 2.2 (1.8–2.8) | 1.9 (1.5–2.7) | 2.4 (2.0–2.9) | 2.3 (1.9–2.8) |
| PAF a | 6.7 (4.4–9.0) | 8.9 (6.7–11.2) | 4.7 (3.5–5.9) | 3.5 (1.9–5.1) | 15.5 (12.3–18.7) | 13.9 (10.9–16.9) |
| Long sleep (≥9 h/night) | ||||||
| Model 1 | 2.5 (1.8–3.6) | 1.1 (0.7–1.5) | 1.0 (0.7–1.7) | 1.2 (0.7–2.1) | 1.1 (0.9–1.5) | 1.3 (1.0–1.6) |
| Model 2 | 2.3 (1.6–3.3) | 0.9 (0.7–1.4) | 0.9 (0.5–1.4) | 1.2 (0.7–1.9) | 1.0 (0.8–1.4) | 1.2 (0.9–1.5) |
| Model 3 | 1.9 (1.3–2.8) | 0.9 (0.6–1.3) | 0.8 (0.5–1.4) | 1.1 (0.7–1.9) | 1.0 (0.8–1.3) | 1.2 (0.8–1.4) |
| PAF a | 7.1 (2.1–11.7) | – | – | – | – | 2.0 (−3.5, 7.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anujuo, K.; Stronks, K.; Snijder, M.B.; Lok, A.; Jean-Louis, G.; Agyemang, C. Association between Depressed Mood and Sleep Duration among Various Ethnic Groups—The Helius Study. Int. J. Environ. Res. Public Health 2021, 18, 7134. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137134
Anujuo K, Stronks K, Snijder MB, Lok A, Jean-Louis G, Agyemang C. Association between Depressed Mood and Sleep Duration among Various Ethnic Groups—The Helius Study. International Journal of Environmental Research and Public Health. 2021; 18(13):7134. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137134
Chicago/Turabian StyleAnujuo, Kenneth, Karien Stronks, Marieke B. Snijder, Anja Lok, Girardin Jean-Louis, and Charles Agyemang. 2021. "Association between Depressed Mood and Sleep Duration among Various Ethnic Groups—The Helius Study" International Journal of Environmental Research and Public Health 18, no. 13: 7134. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137134