
Relationship Dynamics among Couples Dealing with Breast Cancer: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Search Strategy
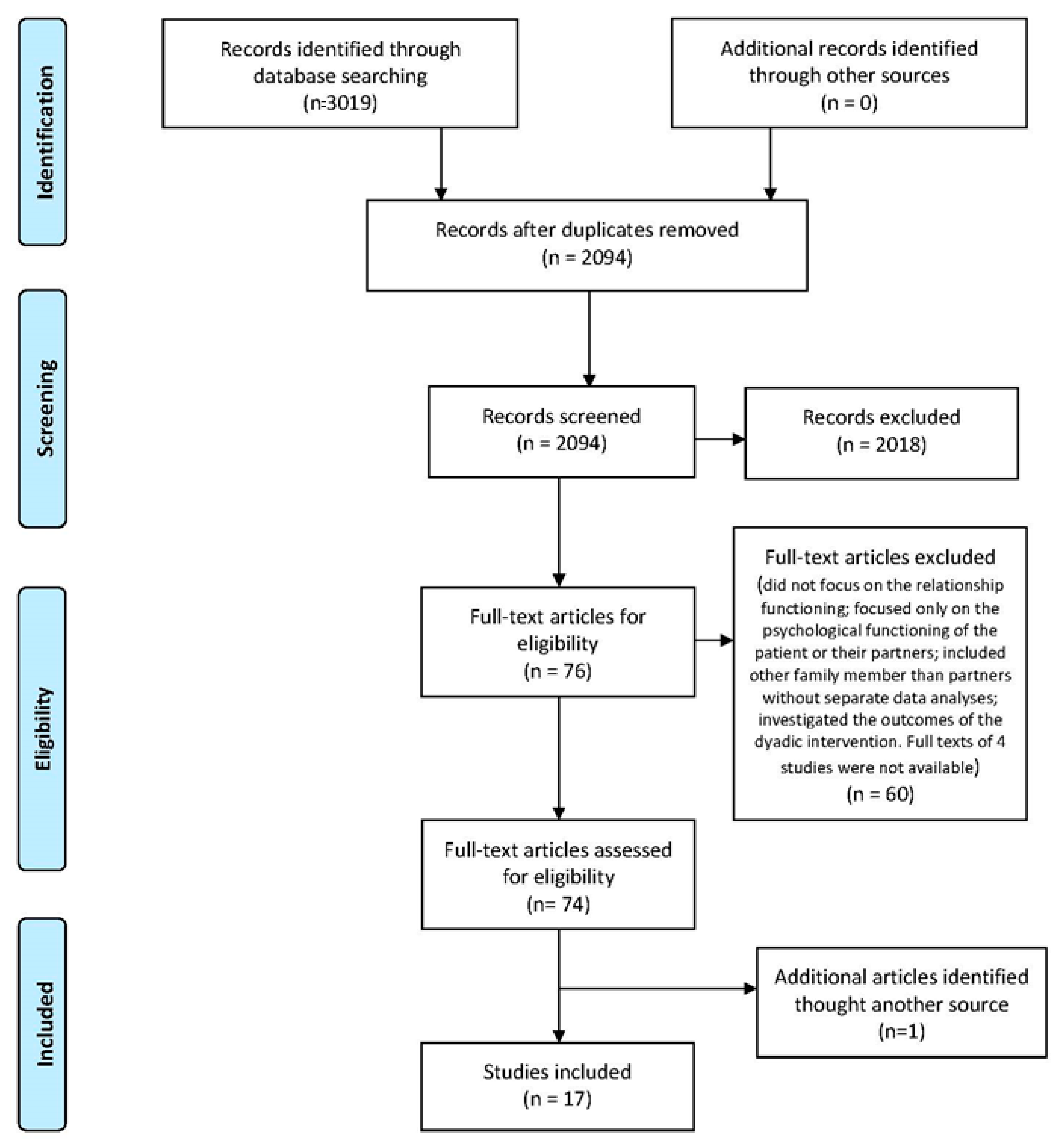
2.3. Study Screening
2.4. Data Extraction
2.5. Quality Assessment
3. Results
3.1. Quality Check
3.2. Study Characteristics
3.3. Findings
3.3.1. Relationship Dynamics
3.3.2. Diagnosis and Acute Phase of Treatment
3.3.3. Impact on Each Member of Dyad
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barton, H.; Shatti, D.; Jones, C.A.; Sakthithasan, M.; Loughborough, W.W. Review of radiological screening programmes for breast, lung and pancreatic malignancy. Quant. Imaging Med. Surg. 2018, 8, 525–534. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oeffinger, K.C.; Fontham, E.T.; Etzioni, R.; Herzig, A.; Michaelson, J.S.; Shih, Y.C.; Walter, L.C.; Church, T.R.; Flowers, C.R.; LaMonte, S.J.; et al. Breast Cancer Screening for Women at Average Risk: 2015 Guideline Update from the American Cancer Society. JAMA 2015, 314, 1599–1614. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [Green Version]
- Carlsson, M.; Hamrin, E. Psychological and psychosocial aspects of breast cancer and breast cancer treatment. A literature review. Cancer Nurs. 1994, 17, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Given, C.W.; Given, B.A. Symptom management and psychosocial outcomes following cancer. Semin. Oncol. 2013, 40, 774–783. [Google Scholar] [CrossRef] [PubMed]
- Ganz, P.A. Psychological and social aspects of breast cancer. Oncology 2008, 22, 642–653. [Google Scholar] [PubMed]
- Lethborg, C.E.; Kissane, D.; Burns, W.I.; Snyder, R. Cast Adrift the Experience of Completing Treatment Among Women with Early Stage Breast Cancer. J. Psychosoc. Oncol. 2000, 18, 73–90. [Google Scholar] [CrossRef]
- Hewitt, M.; Greenfield, S.; Stovall, E. From Cancer Patient to Cancer Survivor: Lost in Transition; National Academies Press: Washington, DC, USA, 2005. [Google Scholar]
- Fang, S.Y.; Lee, K.T. From Patient to Survivor: Women’s Experience with Breast Cancer after 5 Years. Cancer Nurs. 2016, 39, E40–E48. [Google Scholar] [CrossRef]
- Carter, B.J. Long-term survivors of breast cancer. A qualitative descriptive study. Cancer Nurs. 1993, 16, 354–361. [Google Scholar] [CrossRef]
- Zimmermann, T. Intimate Relationships Affected by Breast Cancer: Interventions for Couples. Breast Care 2015, 10, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Brandão, T.; Pedro, J.; Nunes, N.; Martins, M.V.; Costa, M.E.; Matos, P.M. Marital adjustment in the context of female breast cancer: A systematic review. J. Psychol. Soc. Behav. Dimens. Cancer 2017, 26, 2019–2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Northouse, L.L.; Cracchiolo-Caraway, A.; Appel, C.P. Psychologic consequences of breast cancer on partner and family. Semin. Oncol. Nurs. 1991, 7, 216–223. [Google Scholar] [CrossRef]
- Miaja, M.; Platas, A.; Martinez-Cannon, B.A. Psychological Impact of Alterations in Sexuality, Fertility, and Body Image in Young Breast Cancer Patients and Their Partners. Rev. Investig. Clin. 2017, 69, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Congard, A.; Christophe, V.; Duprez, C.; Baudry, A.S.; Antoine, P.; Lesur, A.; Loustalot, C.; Guillemet, C.; Leclercq, M.; Segura, C.; et al. The self-reported perceptions of the repercussions of the disease and its treatments on daily life for young women with breast cancer and their partners. J. Psychosoc. Oncol. 2019, 37, 50–68. [Google Scholar] [CrossRef]
- Kayser, K.; Watson, L.E.; Andrade, J.T. Cancer as a we-disease: Examining the process of coping from a relational perspective. Fam. Syst. Health 2007, 25, 404. [Google Scholar] [CrossRef]
- Hagedoorn, M.; Sanderman, R.; Bolks, H.N.; Tuinstra, J.; Coyne, J.C. Distress in couples coping with cancer: A meta-analysis and critical review of role and gender effects. Psychol. Bull. 2008, 134, 1–30. [Google Scholar] [CrossRef] [Green Version]
- Kayser, K.; Acquati, C. The influence of relational mutuality on dyadic coping among couples facing breast cancer. J. Psychosoc. Oncol. 2019, 37, 194–212. [Google Scholar] [CrossRef]
- O’Mahoney, J.M.; Carroll, R.A. The impact of breast cancer and its treatment on marital functioning. J. Clin. Psychol. Med. Settings 1997, 4, 397–415. [Google Scholar] [CrossRef]
- Badr, H.; Carmack, C.L.; Kashy, D.A.; Cristofanilli, M.; Revenson, T.A. Dyadic Coping in Metastatic Breast Cancer. Health Psychol. 2010, 29, 169–180. [Google Scholar] [CrossRef] [Green Version]
- Manne, S.L.; Siegel, S.; Kashy, D.; Heckman, C.J. Cancer-specific relationship awareness, relationship communication, and intimacy among couples coping with early-stage breast cancer. J. Soc. Pers. Relatsh. 2014, 31, 314–334. [Google Scholar] [CrossRef] [Green Version]
- Wittmann, D. Emotional and sexual health in cancer: Partner and relationship issues. Curr. Opin. Supportive Palliat. Care 2016, 10, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Wellisch, D.K. The psychologic impact of breast cancer on relationships. Semin. Oncol. Nurs. 1985, 1, 195–199. [Google Scholar] [CrossRef]
- Staff, H.R.; Didymus, F.F.; Backhouse, S.H. The antecedents and outcomes of dyadic coping in close personal relationships: A systematic review and narrative synthesis. Anxiety Stress Coping 2017, 30, 498–520. [Google Scholar] [CrossRef] [PubMed]
- Kelley, H.H.; Thibaut, J.W. Interpersonal Relations: A Theory of Interdependence; Wiley: New York, NY, USA, 1978. [Google Scholar]
- Rusbult, C.E.; Buunk, B.P. Commitment processes in close relationships: An interdependence analysis. J. Soc. Pers. Relatsh. 1993, 10, 175–204. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Higgins, M.D.; Green, R.J.; Leeson, M.S. Optical wireless for intravehicle communications: A channel viability analysis. IEEE Trans. Veh. Technol. 2011, 61, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Mallen, C.; Peat, G.; Croft, P. Quality assessment of observational studies is not commonplace in systematic reviews. J. Clin. Epidemiol. 2006, 59, 765–769. [Google Scholar] [CrossRef]
- Walsh, D.; Downe, S. Appraising the quality of qualitative research. Midwifery 2006, 22, 108–119. [Google Scholar] [CrossRef]
- Skerrett, K. Couple adjustment to the experience of breast cancer. Fam. Syst. Health 1998, 16, 281. [Google Scholar] [CrossRef]
- Morgan, P.D.; Fogel, J.; Rose, L.; Barnett, K.; Mock, V.; Davis, B.L.; Gaskins, M.; Brown-Davis, C. African American couples merging strengths to successfully cope with breast cancer. Oncol. Nurs. Forum 2005, 32, 979–987. [Google Scholar] [CrossRef]
- Picard, L.; Dumont, S.; Gagnon, P.; Lessard, G. Coping strategies among couples adjusting to primary breast cancer. J. Psychosoc. Oncol. 2005, 23, 115–135. [Google Scholar] [CrossRef]
- Chung, C.; Hwang, E. Couples’ experiences of breast cancer in Korea: A descriptive qualitative study. Cancer Nurs. 2012, 35, 211–220. [Google Scholar] [CrossRef]
- Antoine, P.; Vanlemmens, L.; Fournier, E.; Trocmé, M.; Christophe, V. Young couples’ experiences of breast cancer during hormone therapy: An interpretative phenomenological dyadic analysis. Cancer Nurs. 2013, 36, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Keesing, S.; Rosenwax, L.; McNamara, B. A dyadic approach to understanding the impact of breast cancer on relationships between partners during early survivorship. BMC Womens Health 2016, 16, 57. [Google Scholar] [CrossRef] [Green Version]
- Meier, F.; Cairo Notari, S.; Bodenmann, G.; Revenson, T.A.; Favez, N. We are in this together—Aren’t we? Congruence of common dyadic coping and psychological distress of couples facing breast cancer. J. Psychol. Soc. Behav. Dimens. Cancer 2019, 28, 2374–2381. [Google Scholar] [CrossRef]
- Northouse, L.L.; Templin, T.; Mood, D.; Oberst, M. Couples’ adjustment to breast cancer and benign breast disease: A longitudinal analysis. J. Psychol. Soc. Behav. Dimens. Cancer 1998, 7, 37–48. [Google Scholar] [CrossRef]
- Hoskins, C.N. Adjustment to breast cancer in couples. Psychol. Rep. 1995, 77, 435–454. [Google Scholar] [CrossRef]
- Manne, S.L.; Ostroff, J.S.; Norton, T.R.; Fox, K.; Goldstein, L.; Grana, G. Cancer-related relationship communication in couples coping with early stage breast cancer. J. Psychol. Soc. Behav. Dimens. Cancer 2006, 15, 234–247. [Google Scholar] [CrossRef]
- Canzona, M.R.; Fisher, C.L.; Ledford, C. Perpetuating the cycle of silence: The intersection of uncertainty and sexual health communication among couples after breast cancer treatment. Supportive Care Cancer 2019, 27, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Çömez, S.; Karayurt, Ö. We as Spouses Have Experienced a Real Disaster! A Qualitative Study of Women with Breast Cancer and Their Spouses. Cancer Nurs. 2016, 39, E19–E28. [Google Scholar] [CrossRef]
- Dorval, M.; Guay, S.; Mondor, M.; Masse, B.; Falardeau, M.; Robidoux, A.; Maunsell, E. Couples Who Get Closer after Breast Cancer: Frequency and Predictors in a Prospective Investigation; American Society of Clinical Oncology: Alexandria, VA, USA, 2005; Volume 23, pp. 3588–3596. [Google Scholar]
- Northouse, L. A longitudinal study of the adjustment of patients and husbands to breast cancer. Oncol. Nurs. Forum 1989, 16, 511–516. [Google Scholar]
- Kim, Y.; Kashy, D.A.; Wellisch, D.K.; Spillers, R.L.; Kaw, C.K.; Smith, T.G. Quality of life of couples dealing with cancer: Dyadic and individual adjustment among breast and prostate cancer survivors and their spousal caregivers. Ann. Behav. Med. 2008, 35, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Ptacek, J.T.; Ptacek, J.J.; Dodge, K.L. Coping with breast cancer from the perspectives of husbands and wives. J. Psychosoc. Oncol. 1994, 12, 47–72. [Google Scholar] [CrossRef]
- Manne, S.; Sherman, M.; Ross, S.; Ostroff, J.; Heyman, R.E.; Fox, K. Couples’ support-related communication, psychological distress, and relationship satisfaction among women with early stage breast cancer. J. Consult. Clin. Psychol. 2004, 72, 660. [Google Scholar] [CrossRef]
- Akram, M.; Iqbal, M.; Daniyal, M.; Khan, A.U. Awareness and current knowledge of breast cancer. Biol. Res. 2017, 50, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baser, R.E.; Li, Y.; Carter, J. Psychometric validation of the Female Sexual Function Index (FSFI) in cancer survivors. Cancer 2012, 118, 4606–4618. [Google Scholar] [CrossRef] [PubMed]
- Ghizzani, A.; Bruni, S.; Luisi, S. The sex life of women surviving breast cancer. Gynecol. Endocrinol. 2018, 34, 821–825. [Google Scholar] [CrossRef] [PubMed]
- Decker, C.L.; Pais, S.; Miller, K.D.; Goulet, R.; Fifea, B.L. A brief intervention to minimize psychosexual morbidity in dyads coping with breast cancer. Oncol. Nurs. Forum 2012, 39, 176–185. [Google Scholar] [CrossRef] [Green Version]
- Manne, S.; Badr, H. Intimacy and relationship processes in couples’ psychosocial adaptation to cancer. Cancer 2008, 112, 2541–2555. [Google Scholar] [CrossRef] [Green Version]
- Villagran, M.; Canzona, M.R.; Ledford, C.J. The milspouse battle rhythm: Communicating resilience throughout the deployment cycle. Health Commun. 2013, 28, 778–788. [Google Scholar] [CrossRef] [PubMed]
- Cutrona, C.E.; Russell, D.W. Type of Social Support and Specific Stress: Toward a Theory of Optimal Matching; Social Support: An Interactional View; Wiley: New York, NY, USA, 1990; pp. 319–366. [Google Scholar]
- Bodenmann, G.; Cina, A. Stress and coping among stable-satisfied, stable-distressed and separated/divorced Swiss couples: A 5-year prospective longitudinal study. J. Divorce Remarriage 2006, 44, 71–89. [Google Scholar] [CrossRef] [Green Version]
- Helgeson, V.S.; Cohen, S. Social support and adjustment to cancer: Reconciling descriptive, correlational, and intervention research. Health Psychol. 1996, 15, 135–148. [Google Scholar] [CrossRef]
- Scholz, U.; Kliegel, M.; Luszczynska, A.; Knoll, N. Associations between received social support and positive and negative affect: Evidence for age differences from a daily-diary study. Eur. J. Ageing 2012, 9, 361–371. [Google Scholar] [CrossRef] [Green Version]
- Giese-Davis, J.; Hermanson, K.; Koopman, C.; Weibel, D.; Spiegel, D. Quality of couples’ relationship and adjustment to metastatic breast cancer. J. Fam. Psychol. 2000, 14, 251–266. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Lei, X.; Chavez-MacGregor, M.; He, W.; Niu, J.; Giordano, S.H. Adherence to Hormonal Therapy among Commercially Insured Breast Cancer Patients. J. Clin. Oncol. 2018, 36, 532. [Google Scholar] [CrossRef]
- Uchino, B.N. Social support and health: A review of physiological processes potentially underlying links to disease outcomes. J. Behav. Med. 2006, 29, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Fradelos, E.C.; Latsou, D.; Mitsi, D.; Tsaras, K.; Lekka, D.; Lavdaniti, M.; Tzavella, F.; Papathanasiou, I.V. Assessment of the relation between religiosity, mental health, and psychological resilience in breast cancer patients. Contemp. Oncol. 2018, 22, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, V.B.; Walker, R.; Phillips, W.; Hudson, V.; Xu, H.; Cabling, M.L.; He, J.; Sutton, A.L.; Hamilton, J. Spirituality in African-American Breast Cancer Patients: Implications for Clinical and Psychosocial Care. J. Relig. Health 2018, 57, 1918–1930. [Google Scholar] [CrossRef]
- Kenny, D.A. Design Issues in Dyadic Research. In Review of Personality and Social Psychology: Research Methods in Personality and Social Psychology; Hendrick, C., Clark, M.S., Eds.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1990; Volume 11, pp. 164–184. [Google Scholar]
- Page, A.E.; Adler, N.E. Cancer Care for the Whole Patient: Meeting Psychosocial Health Needs; National Academies Press: Alexandria, VA, USA, 2008. [Google Scholar]
- Ben-Zur, H.; Gilbar, O.; Lev, S. Coping with breast cancer: Patient, spouse, and dyad models. Psychosom. Med. 2001, 63, 32–39. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Distress management. Clinical practice guidelines. J. Natl. Compr. Cancer Netw. 2003, 1, 344–374. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Search Terms |
|---|
|
| Northouse, 1989 | Carter, 1993 | Ptacek et al., 1994 | Hoskins, 1995 | Northouse et al., 1998 | Meier et al., 2019 | Kim et al., 2008 | Manne et al., 2006 | |
|---|---|---|---|---|---|---|---|---|
| Accurate and appropriate outcome (intervention) measures in all participants | + | + | + | + | + | + | + | + |
| Adjustment for confounding | + | + | + | + | + | + | + | + |
| Case/controls recruited from same population | − | − | − | − | + | − | − | − |
| Appropriate statistical tests used | + | + | + | + | + | + | + | + |
| Participants representative of population | + | + | + | + | + | + | + | + |
| Potential confounders described | − | − | − | − | − | − | − | − |
| Recruitment of case/control over same time frame | − | − | − | − | − | − | − | − |
| Participants characteristics described | + | + | + | + | + | + | + | + |
| Numerical description of important outcomes given | + | + | + | + | + | + | + | + |
| Outcomes clearly described | + | + | + | + | + | + | + | + |
| Response/nonresponse rate described | + | + | + | + | + | + | + | + |
| Clear case/control definition | − | − | − | − | + | + | − | − |
| Power calculation used | N/A | N/A | N/A | N/A | N/A | − | N/A | N/A |
| Losses and completers described | + | N/A | +/− | + | +/− | − | − | + |
| Reliable assessment of disease state | + | + | + | + | + | + | + | + |
| Clear inclusion/exclusion criteria | + | + | + | + | + | + | + | + |
| Clear hypothesis | + | + | + | + | + | + | + | + |
| Reported probability characteristics | + | + | + | + | + | + | + | + |
| Type of study stated | + | + | + | + | + | + | + | + |
| Main findings described | + | + | + | + | + | + | + | + |
| Disclosure of funding source | N/A | N/A | N/A | N/A | N/A | + | N/A | N/A |
| Conclusions supported by findings | + | + | + | + | + | + | + | + |
| Statistical tests of heterogeneity | − | − | − | − | − | − | − | − |
| Total Score | 16 | 15 | 15.5 | 16 | 17.5 | 17 | 15 | 16 |
| Antoine et al., 2013 | Skerrett, 1998 | Picard et al., 2005 | Keesing et al., 2016 | Chung et al., 2012 | Canzona et al.,2019 | Dorval et al., 2005 | Morgan et al., 2005 | Cömez et al., 2016 | |
|---|---|---|---|---|---|---|---|---|---|
| Clear statement of, and rationale for, research question/aims/purposes | + | + | + | + | + | + | + | + | + |
| Study thoroughly contextualized by existing literature | +/− | + | + | + | + | + | + | + | + |
| Method/design apparent, and consistent with research intent | + | + | + | + | + | +/− | + | + | +/− |
| Data collection strategy apparent and appropriate | + | + | +/− | +/− | + | − | + | + | + |
| Sample and sampling method appropriate | +/− | + | − | + | + | + | + | + | + |
| Analyticapproach appropriate | − | + | − | + | + | + | +/− | + | + |
| Context described and taken account of in interpretation | + | + | + | + | + | + | + | + | + |
| Clear audit trailgiven | + | +/− | + | + | + | + | + | +/− | + |
| Data used to support interpretation | + | + | + | + | + | + | + | + | + |
| Researcherreflexivitydemonstrated | − | − | − | + | +/− | − | − | − | − |
| Demonstration of sensitivity to ethical concerns | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Relevance and transferabilityevident | + | + | + | + | + | + | + | + | + |
| Total Score | 8 | 8.5 | 7.5 | 10.5 | 10.5 | 8.5 | 9.5 | 9.5 | 8.5 |
| Author | Country | N of Dyads | Design | Measurement Point/Intervals | Variables | Key Results |
|---|---|---|---|---|---|---|
| Northouse, 1989 | USA | 41 | Observational | At three points in time: 3 days, 30 days, and 18 months post-surgery | Mood, roles functioning and symptoms over distress as post indicators of adjustment. | At 18 months post-surgery, approximately 35% of patients and 24% of partners reported a moderate level of distress. Both patients and partners had few difficulties carrying out the role functions at work, family and social levels. No correlation between demographic factors (e.g., age, level of education, length of marriage) and adjustment was found. Furthermore, no significant differences resulted between medical factors (type of surgery, evidence of recurrence, current treatment, completion of breast reconstruction) and psychological distress or mood symptoms. As for husbands, demographic factors were related to mood disturbance. Younger men and in marriage for a shorter period of time reported a lower level of positive states. Husbands of women with recurrent cancer or women on chemotherapy reported more role problems. |
| Carter, 1993 | USA | 14 | Mixed Methodology | 2–3 years from the mastectomy | How the couples adapt over the term of treatment. What interactional factors characterize couples affected by BC. | No apparent psychological consequences took place over time to either the husband or the patient as a single individual. Differences did not occur between husbands and wives on individual adjustment to illness. In contrast, significant differences were found in marital interactions that define the psychology of the couple system. Marriages are characterized by extraordinarily high levels of enmeshment. Less rigidity, in terms of rules and roles, flexible interaction patterns (three components: marital domination, the punitiveness of one spouse toward the other and conflict resolution through negotiations), communication patterns that facilitate disclosure and free exchange represent crucial components of adaptability. |
| Antoine et al., 2013 | FR | 11 | Qualitative | Undergoing hormone therapy | Identify the experiences of partners and young women who had breast cancer, identify the marriage functioning in BC hormone treatment. | Five main themes emerged: the disease cemented our relationship; the mirror breaks (i.e., refers to physical, psychological and emotional symptoms); the onslaught of solidarity (means the support, both instrumental and emotional one, by close and distant family and friends); a suspended future (cancer and recurrence, difficulties with long term perspectives and family planning); what the disease revealed to me. |
| Skerrett, 1998 | USA | 20 | Qualitative | From 18 to 31 months post diagnosis | How a diagnosis of breast cancer affects the marital relationship. How different aspects of the relationship can help or impede couple adaptation. | High Adapters: challenging impact identifiable, united coping philosophy, selective communication patterns, positive use of multigenerational legacies (i.e., the information about their history to fashion personal theories about a method of coping that would work for them), articulated beliefs on health and illness, and beliefs regarding one’s ability to control or influence the course of illness and well-being, resilient sexuality. At-Risk Adapters: devastating impact, lack of dyadic coping, mutual isolation, strained communication, difficulty using multigenerational legacies, absent or conflictual beliefs, multiple stressors (e.g., medical complications, past losses and traumatic histories). |
| Ptacek et al., 1994 | USA | 36 | Observational | Currently disease free (1.5 years from the end of radiotherapy) | The couple’s modalities of coping with treatment. | A consistent pattern of correlations among coping techniques for both spouses was reported. Respectively, it was found a strong correlation, for both husbands and wives, among the coping strategies of self-blame, wishful thinking and avoidance. However, the self-reported coping of one spouse was largely unrelated to the self-reported coping of the other spouse. In terms of well-being, for both husbands and wives, the greater relative use of seeking support and less use of avoidance was associated with better mental health. A low level of well-being was also related to the use of problem-focused coping and wishful thinking in wives and blaming oneself in husbands. Satisfaction with the marital relationship was far less strongly correlated to cancer-specific coping. |
| Picard et al., 2005 | FR | 16 | Qualitative | From 10 to 12 following the initial diagnosis | Ways in which the couple as a dyad deal with the disease and associated treatments. | Four themes: dealing with the Unknown; dealing with the Threat of Loss and the Uncertainty of the Future; dealing with the Woman’s Personal Transformations in the Couple’s Sex Life; organizing a Social Support Network. |
| Keesing et al., 2016 | AUS | 8 | Qualitative | Till 6 months to 5 years from completing the treatment, excluding adjuvant hormone treatment | How wives and spouses communicate with each other; the pattern used by the couples to maintain their relationship; the needs and supports required by women and their partners. | Three themes: A disconnection within the relationship (the woman survivor of breast cancer needing to prioritize her own needs, sometimes at the expense of her partner and the relationship); Reformulating the relationship (i.e., reflects the strategies used by couples to negotiate changes within the relationship); Support is needed to negotiate the future of the relationship (i.e., couples emphasized the need for additional support and resources to assist them in maintaining their relationship during early survivorship). |
| Chung et al., 2012 | KR | 7 | Qualitative | From 5 to 63 months following the initial diagnosis | The aspects of couples’ going throw after BC diagnosis. | Nine themes: HITTING A WALL (when the women and their husbands initially heard about the cancer diagnosis, a feeling of shock was the most common immediate response); FACING HARDSHIPS WITH TREATMENT AND SUPPORT (after their immediate responses, couples underwent a difficult phase of facing hardships with treatment and support as summarized with “suffering with treatment” and “feeling; CONTROLLING AND PROTECTING MYSELF (women focused on themselves: controlling and protecting myself); REFORMING MY LIFE TO CARE FOR HER (husbands try to find ways to help their wives more actively, three categories of “reforming my life,” “providing care” and “keeping a positive attitude”); WORKING TO SURVIVE THE REALITY (couples agreed to deal with the situation together as categorized by “following standards,” “accepting the new reality” and “working to survive”); COMING INTO MY OWN (cancer as a turning point for women to change their attitude from being introspective or forbearing to being more assertive and expressive, BEING A CARING PERSON (changes in husbands); KNOWING THINGS’ WORTH (the couples learned lessons, involving four categories of “appreciating partners,” “thinking what this event means,” “thinking about what is important” and “asking for further support”); BEING SUSPENDED WITHOUT RESOLUTION (several issues were still challenging the couple) |
| Canzona et al., 2019 | USA | 53 | Qualitative | End the treatment from 3 months to 25 years prior to recruitment | How couples attempt and experience the challenging of BC. | Five sources of uncertainty: perceptions of post treatment bodies, worry about effects on relational partners, ethical concerns about dissatisfaction with sexual relationship (partner prospective), fears about future of the relationship and apprehension about Sexual Health treatment uselessness. Four themes of communication efforts: supporting survivors’ body esteem (partner prospective), navigating potentially hurtful disclosures, responding to partners’ obstructive behavior and believing communications useless. |
| Dorval et al., 2005 | CA | 282 | Qualitative | Three measurement points: at 2 weeks and 3 and 12 months after treatment start | The potential adaptation Predictors from the perspective of both couple Members. | A global agreement between the patients and their spouses about the effect of the disease on their relationships emerged. Most of the couples reported that breast cancer and associated treatments had made them closer. In terms of marital satisfaction, at twelve months, significantly higher levels were found among couples where both partners reported individually that breast cancer had made them closer. Four factor predictors were found: giving advice to the spouse about coping with breast cancer, the spouse’s accompanying the patient to surgery, and the spouse reporting the patient as a confidant. The fourth factor consisted of tenderness and affection from her spouse since diagnosis. |
| Morgan et al., 2005 | USA | 12 | Qualitative | Not specified field | The pattern by which African American couples cope with BC. | Two main dimensions: merging strengths (as uniting and working together to cope with the challenges of a breast cancer diagnosis) to cope with and survive a breast cancer diagnosis. Six categories of merging strengths were reported: walking together; praying together; seeking together information and supportive network; trusting together; adjusting together; being together. Spirituality was an integral component that influenced the effectiveness of each of these major categories. |
| Comez et al., 2016 | TR | 14 | Qualitative | At least 1 year prior to recruitment | The process of women with BC and their spouses from diagnosis to treatment completion. | Different themes related to the phase of treatment—When the couples received the diagnosis, two main themes emerged: perceptions of breast cancer (BC) and reactions to BC. During the treatment process, four themes emerged: symptoms experienced, fear, understanding each other’s worth and needs and counseling. Three themes characterized the stage related to coping with the disease and treatment: process body image and sexuality, religious beliefs and support systems. After the treatment period, three themes were found: changes in roles, health-promoting behaviors and living for oneself and not for others. |
| Hoskins, 1995 | USA | 128 | Observational | Six measurements points: at 7–10 days, atone, 2, 3, and 6 months, and 1 year post surgery | Adjustment outcomes as an interpersonal variable. | Emotional adjustment in both patients and partners could be predicted by satisfaction of interactional and emotional needs. The effects of cancer accentuated the dynamics of a complementary pattern of interaction (partners perceived and complemented i each other’s needs) as a strategy for coping with the experience. This interaction may be enhancing the likelihood of positive emotions. |
| Northouse et al., 1998 | USA | 73 | Observational | Three measurements points: at the time of diagnosis and at 60 days and 1 year post diagnosis | The concurrent stress, resources, appraisal and patterns of adjustment of couples in the benign and malignant groups, comparing the psychosocial responses of patients versus spouses. | During the first year following diagnosis, the patterns of adjustment (emotional distress and role problems) were clearly dissimilar for couples facing benign versus malignant disease. Couples in the malignant group reported significantly higher levels of emotional distress and more role problems than couples in the benign group, and these differences persisted over time. Couples in the malignant group reported greater decreases in marital satisfaction and family functioning than couples in the benign group. A significant decline of social support over time was reported by women with malignant breast cancer. Couples in the malignant group reported more uncertainty about the nature and course of the illness than couples in the benign group. The uncertainty of women with breast cancer decreased over time, but their uncertainty and that one of their husbands remained markedly higher than the level of uncertainty reported by couples in the benign group. |
| Meier et al., 2019 | OH | 70 | Observational | Three measurements points at 2 weeks, at 3 months, and 1 year after cancer surgery | The effect of Common Dyadic Coping (CDC) on individuals 1 year after cancer surgery. Psychological distress in patients and their partners. | At 1 year after cancer surgery, patients and partners reported lower psychological distress when the couple showed a CDC in terms of couples’ agreement on how partners cope as a couple. Specifically, high CDC congruence was related to lower psychological distress among female patients. However, CDC may lose its importance over time when couples cope with chronic issues related to the disease. |
| Manne et al., 2006 | USA | 127 | Observational | Two measurement points: during cancer treatment and at 9 months after the baseline (Time 2) | The association between types of couple’s communication strategies and couple’s ability to handle breast cancer’ stressors. | Partners who reported more constructive mutual communication had lower levels of discomfort at Time 2, while partners who reported greater avoidance of discussing problems and stressors or greater use of request-withdrawal communication experienced higher levels of suffering. Greater communication regarding stressors due to illness between patient and partner reduced the partner’s anguish levels and increased relationship satisfaction while potentially modulating the perception of the patient’s physical damage. Greater mutual constructive communication was a significant predictor of low partner distress, and greater mutual omission was a marginally significant predictor of partner suffering. Furthermore, request-withdrawal communication was not a significant predictor of the partner’s distress. |
| Kim et al., 2008 | USA | 168 | Observational | Approximately 2 years from the diagnosis prior to recruitment | The dyadic effects of psychological distress on the quality of life of couples dealing with cancer. | The strongest predictor of the couple’s quality of life was the individual psychological distress, and it was strongly related to mental health. At 2 years post diagnosis, cancer survivors and their spouses displayed normal levels of psychological wellbeing and quality of life. Patients and partners caregivers reported similar levels of psychological distress and quality of life. The partner’s distress and the (dis)similarity in the levels of distress of the couple played a significant role in the individual quality of life. At the dyadic level, for men, a greater dissimilarity in psychological distress was associated with better physical health. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valente, M.; Chirico, I.; Ottoboni, G.; Chattat, R. Relationship Dynamics among Couples Dealing with Breast Cancer: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7288. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147288
Valente M, Chirico I, Ottoboni G, Chattat R. Relationship Dynamics among Couples Dealing with Breast Cancer: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(14):7288. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147288
Chicago/Turabian StyleValente, Marco, Ilaria Chirico, Giovanni Ottoboni, and Rabih Chattat. 2021. "Relationship Dynamics among Couples Dealing with Breast Cancer: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 14: 7288. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147288