
A Health eLearning Ontology and Procedural Reasoning Approach for Developing Personalized Courses to Teach Patients about Their Medical Condition and Treatment

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Background
3. Materials and Methods
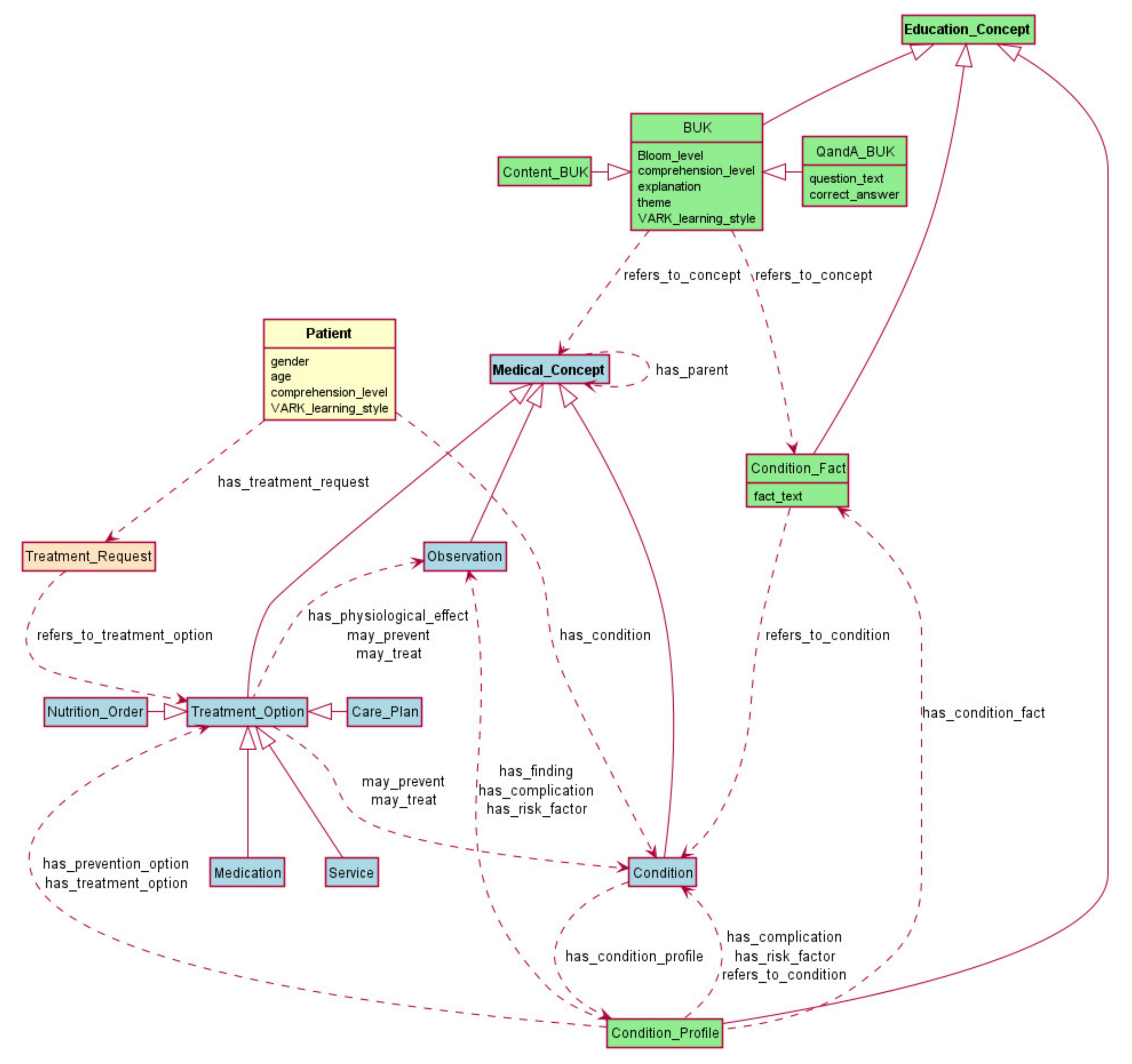
3.1. eLearning Ontology
3.2. Planning and Execution Framework
3.3. Proof-of-Concept Implementation
3.4. Course Generation
3.5. Evaluation Methods
4. Results
5. Discussion
6. Conclusions
- The structure of a course is fixed and progression through a course is linear;
- A patient’s comprehension level is known in advance;
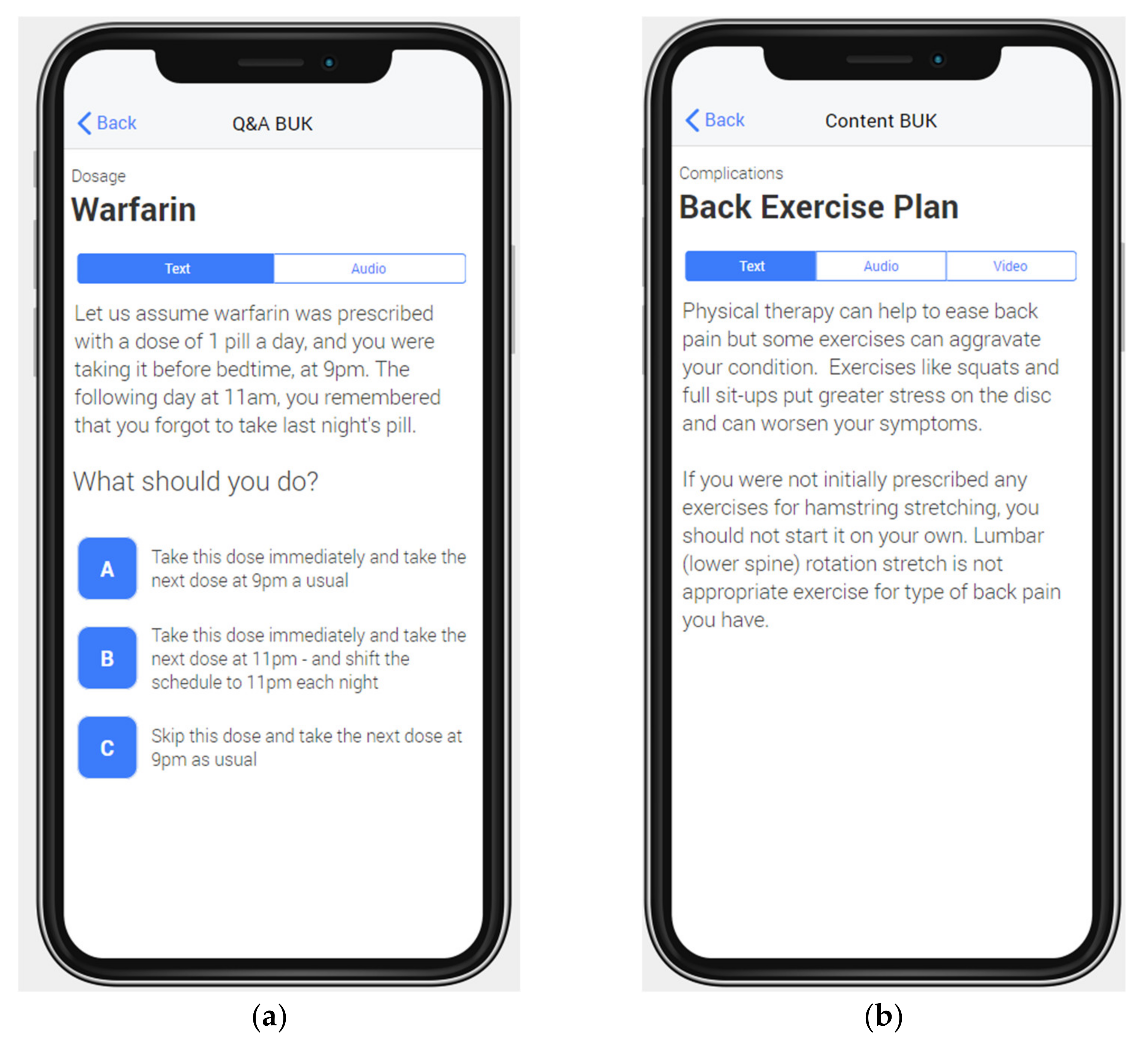
- Only a Content BUK and the explanation part of a Q&A BUK are associated with multimodal presentation;
- A patient’s learning style is set to a default and not determined a priori, and as such, a patient is free to change the mode of presentation for each BUK separately;
- BUKs are fixed and they need to be developed in advance for different comprehension levels.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Clinical Specialist #1 | Clinical Specialist #2 | Clinical Specialist #3 |
|---|---|---|---|
| Perceived Ease of Use | |||
| 1. Will the purpose of the lessons be clear to patients? (Strongly Agree, Agree, Neutral, Disagree, Strongly Disagree) | Strongly Agree (5). Lessons are intuitive and easy to follow. | Strongly Agree (5). It is a common question for patients. There is a lot of conflicting info on the web, erroneous beliefs, conflicting messages from pharmacists, physicians, relatives, etc. | Agree (4). The lesson on anticoagulants is helping patients be more aware of dietary interactions and troubleshooting medication issues while the back pain lesson is simple and straightforward. |
| 2. Will the structure (Q&A followed by Content BUK) of the lessons be clear to patients? (Strongly Agree, Agree, Neutral, Disagree, Strongly Disagree) | Strongly Agree (5). The structure is clear and easy to follow. | Strongly Agree (5). The fact that the explanation comes just after they answered the question will make it easier to integrate. | Strongly Agree (5). It is very clear that the scenario is followed by an appropriate unit of knowledge. |
| 3. Will the transitions between questions and explanations be intuitive and understandable to patients? (Strongly Agree, Agree, Neutral, Disagree, Strongly Disagree) | Strongly Agree (5). Excellent flow. | Strongly Agree (5). | Strongly Agree (5) although explanation for 1st anticoagulation lesson seems overly detailed. Transition appropriate though. |
| Perceived Usefulness | |||
| 4. Is the content of the lessons appropriately tailored to different level of health literacy? (Strongly Agree, Agree, Neutral, Disagree, Strongly Disagree) | Strongly Agree (5). The difference in health literacy is obvious and tailored appropriately to patients’ needs. | Unsure (3). For example, the calculation of actual vitamin K contents might not be appropriate for every patient. Some would likely need more general guidance. Or perhaps you could think of ordering the questions with increasing difficulty, so that patients don’t abandon too early if the questions seem too complex to them. | Agree (4). However, content of 1st anticoagulation lesson seems overly detailed. I would disagree with content in first back pain lesson. Spine practitioners are often trying to re-educate patients that degenerative discs are a normal ageing process and not necessarily a cause of pain. As such, I think this BUK is reinforcing erroneous information. I would change the question to what are the symptoms of a herniated disc…. answer would be back and/or leg pain (sciatica). |
| Perceived Intention to Use | |||
| 5. Can having access to personalized materials via lessons help patients to better manage their condition? (Strongly Agree, Agree, Neutral, Disagree, Strongly Disagree) | Strongly Agree (5). It is hard for clinicians to go through all the QAs in one encounter with the patient. Furthermore, different patients may have different questions or concerns which need to be addressed. Finally, patients often will only remember of [sic] questions once back home. Having access to personalized materials that they can have access to is important. | Neutral (3). Not clear how [the material is] ‘personalized.’ | Strongly Agree (5). Personalized information will allow patients to better understand their condition, have more productive discussions with their physician and potentially decrease the need for physician visits. |
| 6. Would you recommend such a personalized teaching framework to every patient? | Absolutely. All clinicians are looking for accurate/adequate patient-oriented material to provide. Any resources would be welcomed (but usually need to be “endorsed” by clinicians or clinical societies). Resources should probably also [be] tailored by countries (or culture)? | Yes. | I do think that if teaching materials were tailored that all patients could benefit in some capacity. |
| 7. How do you see patients use such a personalized teaching framework? | Yes. Patient will use it after the initial diagnosis but may also go back to it intermittently afterwards if questions are arising. It will be reassuring for patients to have access to a personalized teaching framework. Would probably go to it before contacting their health care provider. | At initiation of therapy to get general guidance, then perhaps whenever they face a specific challenge. | They could use personalized teaching through their health record (i.e., MYchart) prior to their healthcare visits so they can ask about and discuss their condition with their physician or after the visit to reinforce important points that they learned. |
| Other | |||
| 8. Are there any changes or additions to our personalized teaching framework that you would recommend? | No. Looks great. | Proposing sub-topics, so that patients could pick up training that relates to a specific question/training need (e.g., diet vs. missed dose vs. etc.). | As described above. |
| Question | Patient 1 | Patient 2 | Patient 3 |
|---|---|---|---|
| Perceived Ease of Use | |||
| 1. Will the purpose of the lessons be clear to patients? | Strongly Agree (5). The lessons provided were very clear to me and what the extent [sic] was. | Agree (4). Be explicit as to the purpose when supplying the Lesson. | Agree (4). |
| 2. Will the structure (Q&A followed by Content BUK) of the lessons be clear to patients? | Strongly Agree (5). The structure makes sense to me and is logically [sic]. It provides enough information to reinforce the topic. | Agree (4). The manner of delivery stimulates active reading and self-assessment, a desire to learn. | Neutral (3). |
| 3. Will the transitions between questions and explanations be intuitive and understandable to patients? | Strongly Agree (5). Was easy to follow and made logically [sic] sense to me. | Agree (4). The approach reinforces/deepens understanding, and teaches to improved thinking. | Neutral (3). |
| Perceived Usefulness | |||
| 4. Is the content of the lessons appropriately tailored to different level of health literacy? | Strongly Agree (5). I agree that the lessons about [sic] are probably for a patient with an expert level of literacy about their condition/disease. | Agree (4). The context is good for an expert literacy level reader. They can absorb and reason through the input. | Neutral (3). I would say this is okay for expert level. Can’t comment on basic level. |
| 5. Can having access to personalized materials via lessons help patients to better manage their condition? | Strongly Agree (5). Yes, I think that offering personalized materials is a great way to better education patients about their condition and how to manage it. There is a lot of information out on the internet that people can read and interpret in different ways. If I got this from my doctor, I would trust that this the information that I should be following to manage my condition | Agree (4). Socratic teaching in small bites when tightly focused on a specific issue captures attention. Insight sinks in [sic] with likely change in behavior resulting. | Neutral (3). Unclear how it is personalized. See final comments. |
| 6. Would you recommend such a personalized teaching framework to every patient? | Yes, I think that this should be offered to patients at the basic and expert level. I think that at the basic level, it would help educate on [sic] why they are taking blood thinners, guidelines to follow etc. For the expert, it’s a good resource for those who want to manage their condition at a high level. | I suggest that you run interviews with two or 3 [sic] patients to test receptivity. Upper moderate to high levels of literacy are necessary for this particular lesson content to work. | Perhaps. |
| 7. How do you see patients use such a personalized teaching framework? | Yes, I do see patients using this personalized teaching framework. I can see it being a helpful resource if someone was newly diagnosed to learn more. It could also be used when a clinician observes that the patient is lacking information and/or compliance in a specific area and it can be used as [a] teaching opportunity/reminder for the patient. What would the delivery methods be for this, it is [sic] solely online? Issue [sic] I can see around [sic] this: No access to computer and/or internet. Computer literacy. | To facilitate self-assessment and motivate learning in self. | Online? Please see final comments. |
| Other | |||
| 8. Are there any changes or additions to our personalized teaching framework that you would recommend? | For AF Q&A BUK # 3—I got the answer wrong and I think that most would. Based on the information given in the box, I wouldn’t have chosen to [sic] any of the possible answers. I would have probably eaten 4 asparagus spears at 48 mcg of vitamin K. Logic for this: I saw that green leaf lettuce as 45 mcg and Romaine lettuce was 48 mcg. So, of all the things on the list, the 4 spears of asparagus was the closest to that number in terms of mcg’s [sic] of vitamin K. It didn’t dawn on me to do a calculation like the answer | Tailor the framework differentially for different patient segments. If you use test subjects for multiple lessons then you’ll know how elements of the whole hang together within segments. | It is unclear how this is to be personalized. By patients [sic] level of understanding? If so, how is this determined? By drug type? e.g., Warfarin vs. Xarleto? I am unsure of the total benefit to a patient of this, with all due respect. It is difficult to assess not knowing how it is personalized, nor how the patient would access it. Would they be obliged to use it? Choose it electively? Based on my experience on Warfarin about 9 years ago, I would say there are 3 essential things. I know this is anecdotal, but for what it is worth— 1. The acclimation period presents many challenges to the patient and needs greater support than what follows. That is, until the level of the drug stabilizes in the patient. 2. Essential information is how to correct for a missed dose. The message is fairly succinct and could be communicated by the physician at the outset. 3. On warfarin, it is highly useful to know the Vitamin K content of various foods. At one time, there was an iOS app for this, and I am sure there are resources on the web as well. |
| Question | Patient 4 | Patient 5 | Patient 6 |
|---|---|---|---|
| Perceived Ease of Use | |||
| 1. Will the purpose of the lessons be clear to patients? | Agree (4). The purpose of the lesson is clear but left me with wondering why I am not learning more about my condition and how I could at least slightly improve my situation. | Agree (4). I think it’s clear [that] the purpose of the lessons is to help patients gain knowledge to better understand what’s going on with their backs, the causes of their pain and what can be done to alleviate it. The lessons could also importantly correct wrong information or misunderstandings, and reinforce correct knowledge already obtained elsewhere (from your physio, for example). The knowledge gained could help patients understand the therapies/exercises/drugs/interventions that are being recommended by health professionals as well as put them in a better position to support strengthening and healing their backs by knowing more about what to do/what not to do and why. Some of these points about the purpose might be emphasized to make it clearer to patients how this process could help them. | Neutral (3). It is not clear what the goal is. The first question seems targeted at the patient understanding the difference between a symptom and contributing factors. There are other important symptoms such as sciatica etc. I guess my criticism is that the logical progression in this example is not clear, but I think the format is good |
| 2. Will the structure (Q&A followed by Content BUK) of the lessons be clear to patients? | Strongly Agree (5). The structure is logical as first, it defines a condition for the patient (what) and then provides some guidance for a patient’s behavior (how). | Strongly Agree (5). The interactive structure is more interesting and relevant than googling and reading long articles. Multiple choice Q and As are more fun, frankly. Info presented in this interactive way and in shorter sections is also easier for most people to retain. | Strongly Agree (5). [My] only concern is (as you have already stated) [that] this may be too basic for some patients, making it non-interesting and less informative. |
| 3. Will the transitions between questions and explanations be intuitive and understandable to patients? | Strongly Agree (5). The transition is appropriate, please see my explanation provided in 2). | Agree (4). I think the transitions are understandable. I’m not sure what you mean by the transitions being intuitive unless it’s that the framework is multiple choice questions and answers, so it’s obvious what the process is. I think as one keeps answering the questions it becomes apparent that the depth of information and the tailoring to one’s personal situation increase with the right answers. (If one gets a wrong answer, then is a there a more basic question next that helps with something more foundational?) | Agree (4). This can be done. The example lacks a bit of this, but the structure allows for this concept to be true. |
| Perceived Usefulness | |||
| 4. Is the content of the lessons appropriately tailored to different level of health literacy? | Agree (4). I believe that the content should be appropriate to a patient with the basic level of health literacy; I would, however, replace such words as ‘manifests’ and ‘exacerbate’ with a more common vocabulary to assure that the explanations are very clear to a patient regardless of her/his literacy level. | Strongly Agree (5). Yes, in the two questions in the sample, the first was more basic than the second and the second built on the first in a way that was more personalized to treatment. The answers also addressed the incorrect choices, which I think will also be helpful to increasing health literacy. | Neutral (3). Hard to say without more examples. This example seems very basic. |
| 5. Can having access to personalized materials via lessons help patients to better manage their condition? | Agree (4). For the majority of patients, yes but it very much depends on individual. However, I believe that if it helps just one patient it should be developed and made available to all when possible | Strongly Agree (5). It has always been frustrating for me that the only way to obtain personalized information about my back issues is to go to a physio/chiropractor/doctor. They are obviously the first and very important line of support, but one doesn’t go to these therapists indefinitely, nor is one able to ask them questions between visits. Even at a visit one doesn’t necessarily ask the right questions or properly take in all the information presented. Back pain can be complex and not easy to understand so something educational tailored to me as an individual with a specific kind of back pain would be a very helpful complement to a program of therapy/exercise and support my efforts to manage my situation daily. | Strongly Agree (5). I really support the concept and if it can be tailored to different levels of understanding due to educational level, language barriers etc, it should be a useful tool. |
| 6. Would you recommend such a personalized teaching framework to every patient? | Yes, please see my explanation provided in 2) above. | I know I would like such a tool and framework and likely the majority of patients would, but I’m not sure I can answer with a yes or no for everyone. It might depend on literacy levels, for example, or how much people are motivated, or how much time this will take. This latter piece [sic] around time would be important to let people know about. 10 min a day? 20? Or is it structured differently in terms of time? | Yes, but only once I am convinced that it can be tailored to different levels. |
| 7. How do you see patients use such a personalized teaching framework? | It is a tough question because in my view there is no ‘one solution fits all’. Options could be developed based on existing behavioral models. The most appropriate one would be deployed by a physician treating the patient and should be based on the physician assessment of the patient. | This is a good question because this framework is about a learning path rather than having a specific question about one’s back pain and using a tool that lets you plug in the question and up pops the answer(s). How it’s presented to patients would be important. For me this would be about learning about my back, the origins of the pain in my particular case (Is it muscles, discs, nerves? Some of the above? All of the above?); then understanding why health care professionals are recommending certain exercises/therapies/drugs (how will those help), and what my part is in helping to ensure these are effective. Sometimes this is obvious, but at others [sic] it is not clear how to manage the pain or what is possible in terms of pain reduction or resolution. The teaching framework could also provide useful knowledge and info about how to best describe the pain and what questions to ask when I do see a health care professional. | Pre-op education. As a recent patient I would find this very helpful. |
| Other | |||
| 8. Are there any changes or additions to our personalized teaching framework that you would recommend? | I don’t have any comments | No, not really. I would just say the more personal and tailored to the individual the better, otherwise it won’t be as useful. Also, perhaps a way to continue the learning path if a new pain presents itself rather than starting over (probably you have thought of this already). | NO, other than what I have commented on above. |
References
- Devine, F.; Edwards, T.; Feldman, S.R. Barriers to Treatment: Describing Them from a Different Perspective. Patient Prefer. Adherence 2018, 12, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Jin, J.; Sklar, G.E.; Min Sen Oh, V.; Chuen Li, S. Factors Affecting Therapeutic Compliance: A Review from the Patient’s Perspective. Ther. Clin. Risk Manag. 2008, 4, 269–286. [Google Scholar] [CrossRef] [Green Version]
- Kvarnstrom, K.; Airaksinen, M.; Liira, H. Barriers and Facilitators to Medication Adherence: A Qualitative Study with General Practitioners. BMJ Open 2018, 8, e015332. [Google Scholar] [CrossRef]
- Taibanguay, N.; Chaiamnuay, S.; Asavatanabodee, P.; Narongroeknawin, P. Effect of Patient Education on Medication Adherence of Patients with Rheumatoid Arthritis: A Randomized Controlled Trial. Patient Prefer. Adherence 2019, 13, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Caro, J.J.; Ishak, K.J.; Huybrechts, K.F.; Raggio, G.; Naujoks, C. The Impact of Compliance with Osteoporosis Therapy on Fracture Rates in Actual Practice. Osteoporos. Int. 2004, 15, 1003–1008. [Google Scholar] [CrossRef] [PubMed]
- Lavielle, M.; Puyraimond-Zemmour, D.; Romand, X.; Gossec, L.; Senbel, E.; Pouplin, S.; Beauvais, C.; Gutermann, L.; Mezieres, M.; Dougados, M.; et al. Methods to Improve Medication Adherence in Patients with Chronic Inflammatory Rheumatic Diseases: A Systematic Literature Review. RMD Open 2018, 4, e000684. [Google Scholar] [CrossRef] [PubMed]
- Verloo, H.; Chiolero, A.; Kiszio, B.; Kampel, T.; Santschi, V. Nurse Interventions to Improve Medication Adherence among Discharged Older Adults: A Systematic Review. Age Ageing 2017, 46, 747–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bull, F.C.; Kreuter, M.W.; Scharff, D.P. Effects of Tailored, Personalized and General Health Messages on Physical Activity. Patient Educ. Couns. 1999, 36, 181–192. [Google Scholar] [CrossRef]
- Peleg, M.; Michalowski, W.; Wilk, S.; Parimbelli, E.; Bonaccio, S.; O’Sullivan, D.; Michalowski, M.; Quaglini, S.; Carrier, M. Ideating Mobile Health Behavioral Support for Compliance to Therapy for Patients with Chronic Disease: A Case Study of Atrial Fibrillation Management. J. Med. Syst. 2018, 42, 234. [Google Scholar] [CrossRef]
- Norcross, J.C.; Krebs, P.M.; Prochaska, J.O. Stages of Change. J. Clin. Psychol. 2011, 67, 143–154. [Google Scholar] [CrossRef]
- Abraham, C.; Michie, S. A Taxonomy of Behavior Change Techniques Used in Interventions. Health Psychol. 2008, 27, 379–387. [Google Scholar] [CrossRef] [Green Version]
- Schapira, M.M.; Swartz, S.; Ganschow, P.S.; Jacobs, E.A.; Neuner, J.M.; Walker, C.M.; Fletcher, K.E. Tailoring Educational and Behavioral Interventions to Level of Health Literacy: A Systematic Review. MDM Policy Pract. 2017, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sedlmeier, P. Intelligent Tutoring Systems. Int. Encycl. Soc. Behav. Sci. 2001, 7674–7678. [Google Scholar] [CrossRef]
- Fleming, N.D.; Mills, C. Not Another Inventory, Rather a Catalyst for Reflection. To Improv. Acad. 1992, 11, 137–155. [Google Scholar] [CrossRef] [Green Version]
- Bloom, B.S. Taxonomy of Educational Objectives; the Classification of Educational Goals; Longmans Green: London, UK, 1956; ISBN 0679302093. [Google Scholar]
- Ingrand, F.F.; Georgeff, M.P.; Rao, A.S. An Architecture for Real-Time Reasoning and System Control. IEEE Expert 1992, 7, 34–44. [Google Scholar] [CrossRef]
- Gruber, T.R. A Translation Approach to Portable Ontology Specifications. Knowl. Acquis. 1993, 5, 199–220. [Google Scholar] [CrossRef]
- Rector, A.; Schulz, S.; Rodrigues, J.M.; Chute, C.G.; Solbrig, H. On beyond Gruber: “Ontologies” in Today’s Biomedical Information Systems and the Limits of OWL. J. Biomed. Inform. X 2019, 2, 100002. [Google Scholar] [CrossRef]
- Noy, N.F.; Mcguinness, D.L. Ontology Development 101: A Guide to Creating Your First Ontology; Technical Report KSL-01-05 and SMI-2001-0880, Stanford Knowledge Systems Laboratory and Stanford Medical Informatics; Stanford University: Stanford, CA, USA, 2001. [Google Scholar]
- Hoving, C.; Mullen, P.D.; van den Borne, B. A History of Patient Education by Health Professionals in Europe and North America: From Authority to Shared Decision Making Education. Patient Educ. Couns. 2010, 78, 275–281. [Google Scholar] [CrossRef]
- Giguère, A.; Zomahoun, H.T.V.; Carmichael, P.H.; Uwizeye, C.B.; Légaré, F.; Grimshaw, J.M.; Gagnon, M.P.; Auguste, D.U.; Massougbodji, J. Printed Educational Materials: Effects on Professional Practice and Healthcare Outcomes. Cochrane Database Syst Rev. 2020, 8, CD004398. [Google Scholar] [CrossRef]
- Hamine, S.; Gerth-Guyette, E.; Faulx, D.; Green, B.B.; Ginsburg, A.S. Impact of MHealth Chronic Disease Management on Treatment Adherence and Patient Outcomes: A Systematic Review. J. Med. Internet Res. 2015, 17, e52. [Google Scholar] [CrossRef] [Green Version]
- Strandbygaard, U.; Thomsen, S.F.; Backer, V. A Daily SMS Reminder Increases Adherence to Asthma Treatment: A Three-Month Follow-up Study. Respir. Med. 2010, 104, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Quinn, C.C.; Shardell, M.D.; Terrin, M.L.; Barr, E.A.; Ballew, S.H.; Gruber-Baldini, A.L. Cluster-Randomized Trial of a Mobile Phone Personalized Behavioral Intervention for Blood Glucose Control. Diabetes Care 2011, 34, 1934–1942. [Google Scholar] [CrossRef] [Green Version]
- Khonsari, S.; Subramanian, P.; Chinna, K.; Latif, L.A.; Ling, L.W.; Gholami, O. Effect of a Reminder System Using an Automated Short Message Service on Medication Adherence Following Acute Coronary Syndrome. Eur. J. Cardiovasc. Nurs. 2015, 14, 170–179. [Google Scholar] [CrossRef]
- Hawkins, R.P.; Kreuter, M.; Resnicow, K.; Fishbein, M.; Dijkstra, A. Understanding Tailoring in Communicating about Health. Health Educ. Res. 2008, 23, 454–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suebnukarn, S.; Haddawy, P. A Bayesian Approach to Generating Tutorial Hints in a Collaborative Medical Problem-Based Learning System. Artif. Intell. Med. 2006, 38, 5–24. [Google Scholar] [CrossRef] [PubMed]
- Kabanza, F.; Bisson, G.; Charneau, A.; Jang, T.-S. Implementing Tutoring Strategies into a Patient Simulator for Clinical Reasoning Learning. Artif. Intell. Med. 2006, 38, 79–96. [Google Scholar] [CrossRef] [PubMed]
- Crowley, R.S.; Legowski, E.; Medvedeva, O.; Tseytlin, E.; Roh, E.; Jukic, D. Evaluation of an Intelligent Tutoring System in Pathology: Effects of External Representation on Performance Gains, Metacognition, and Acceptance. J. Am. Med. Inform. Assoc. 2007, 14, 182–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfe, C.R.; Reyna, V.F.; Widmer, C.L.; Cedillos, E.M.; Fisher, C.R.; Brust-Renck, P.G.; Weil, A.M. Efficacy of a Web-Based Intelligent Tutoring System for Communicating Genetic Risk of Breast Cancer. Med. Decis. Mak. 2015, 35, 46–59. [Google Scholar] [CrossRef] [PubMed]
- Chammas, N.; Juric, R.; Koay, N.; Gurupur, V.; Suh, S.C. Towards a Software Tool for Raising Awareness of Diabetic Foot in Diabetic Patients. In Proceedings of the 2013 46th Hawaii International Conference on System Sciences, Wailea, HI, USA, 7–10 January 2013; IEEE: Piscataway, NJ, USA, 2013; pp. 2646–2655. [Google Scholar]
- Adnan, M.; Warren, J.; Orr, M. Ontology Based Semantic Recommendations for Discharge Summary Medication Information for Patients. In Proceedings of the 2010 IEEE 23rd International Symposium on Computer-Based Medical Systems (CBMS), Bentley, WA, Australia, 12–15 October 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 456–461. [Google Scholar]
- Amith, M.; Gong, Y.; Cunningham, R.; Boom, J.; Tao, C. Developing VISO: Vaccine Information Statement Ontology for Patient Education. J. Biomed. Semant. 2015, 6, 23. [Google Scholar] [CrossRef] [Green Version]
- Abidi, S.S.R.; Abidi, S. An Ontology-Driven Personalization Framework for Designing Theory-Driven Self-management Interventions. In Process Support and Knowledge Representation in Health Care. ProHealth 2013; KR4HC 2013, Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2013; Volume 8268. [Google Scholar]
- Quinn, S.; Bond, R.; Nugent, C. A Two-Staged Approach to Developing and Evaluating an Ontology for Delivering Personalized Education to Diabetic Patients. Inform. Health Soc. Care 2018, 43, 264–279. [Google Scholar] [CrossRef]
- Bickmore, T.W.; Schulman, D.; Sidner, C.L. A Reusable Framework for Health Counseling Dialogue Systems Based on a Behavioral Medicine Ontology. J. Biomed. Inform. 2011, 44, 183–197. [Google Scholar] [CrossRef] [Green Version]
- Inott, T.; Kennedy, B.B. Assessing Learning Styles: Practical Tips for Patient Education. Nurs. Clin. N. Am. 2011, 46, 313–320. [Google Scholar] [CrossRef]
- Thompson, A.R.; O’Loughlin, V.D. The Blooming Anatomy Tool (BAT): A Discipline-Specific Rubric for Utilizing Bloom’s Taxonomy in the Design and Evaluation of Assessments in the Anatomical Sciences. Anat. Sci. Educ. 2015, 8, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Limongelli, C.; Sciarrone, F.; Temperini, M.; Vaste, G. Adaptive Learning with the LS-Plan System: A Field Evaluation. IEEE Trans. Learn. Technol. 2009, 2, 203–215. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Noriega, A.; Juárez-Ramírez, R.; Martínez-Ramírez, Y. Evaluation Module Based on Bayesian Networks to Intelligent Tutoring Systems. Int. J. Inf. Manag. 2017, 37, 1488–1498. [Google Scholar] [CrossRef]
- Castleberry, D.; Brandt, S. The Effect of Question Ordering Using Bloom’s Taxonomy in an e-Learning Environment. In Proceedings of the 7th Annual International Conference on Computer Science Education: Innovation & Technology (CSEIT 2016), Sydney, Australia, 10 October 2016. [Google Scholar]
- Nkanginieme, K.E.O. Clinical Diagnosis as a Dynamic Cognitive Process: Application of Bloom’s Taxonomy for Educational Objectives in the Cognitive Domain. Med. Educ. Online 1997, 2, 4288. [Google Scholar] [CrossRef]
- Chatterjee, D.; Corral, J. How to Write Well-Defined Learning Objectives. J. Educ. Perioper. Med. JEPM 2017, 19, E610. [Google Scholar] [PubMed]
- Krau, S.D. Creating Educational Objectives for Patient Education Using the New Bloom’s Taxonomy. Nurs. Clin. N. Am. 2011, 46, 299–312. [Google Scholar] [CrossRef]
- Fuster, V.; Rydén, L.E.; Cannom, D.S.; Crijns, H.J.; Curtis, A.B.; Ellenbogen, K.A.; Halperin, J.L.; Le Heuzey, J.Y.; Kay, G.N.; Lowe, J.E.; et al. ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients with Atrial Fibrillation). Circulation 2006, 114, e257–e354. [Google Scholar] [PubMed] [Green Version]
- Ogilvie, I.M.; Newton, N.; Welner, S.A.; Cowell, W.; Lip, G.Y.H. Underuse of Oral Anticoagulants in Atrial Fibrillation: A Systematic Review. Am. J. Med. 2010, 123, 638–645.e4. [Google Scholar] [CrossRef]
- Publication of “The Burden of Musculoskeletal Conditions at the Start of the New Millennium”. Morb. Mortal. Wkly. Rep. 2003, 52, 1081.
- Musen, M.A. The Protégé Project. AI Matters 2015, 1, 4–12. [Google Scholar] [CrossRef] [PubMed]
- OWL—Semantic Web Standards. Available online: https://www.w3.org/OWL/ (accessed on 19 March 2020).
- Condition—FHIR v4.0.1. Available online: https://www.hl7.org/fhir/condition.html (accessed on 19 March 2020).
- Martin, L.T.; Ruder, T.; Escarce, J.J.; Ghosh-Dastidar, B.; Sherman, D.; Elliott, M.; Bird, C.E.; Fremont, A.; Gasper, C.; Culbert, A.; et al. Developing Predictive Models of Health Literacy. J. Gen. Intern. Med. 2009, 24, 1211–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pander Maat, H.; Essink-Bot, M.L.; Leenaars, K.E.; Fransen, M.P. A Short Assessment of Health Literacy (SAHL) in the Netherlands. BMC Public Health 2014, 14, 990. [Google Scholar] [CrossRef] [Green Version]
- Beauchamp, A.; Buchbinder, R.; Dodson, S.; Batterham, R.W.; Elsworth, G.R.; McPhee, C.; Sparkes, L.; Hawkins, M.; Osborne, R.H. Distribution of Health Literacy Strengths and Weaknesses across Socio-Demographic Groups: A Cross-Sectional Survey Using the Health Literacy Questionnaire (HLQ). BMC Public Health 2015, 15, 678. [Google Scholar] [CrossRef] [Green Version]
- Drummond, N.; Rector, A.; Moulton, G.; Stevens, R.; Horridge, M.; Wang, H.; Seidenberg, J. Sequences in OWL. In Proceedings of the 9th International Protege Conference, Stanford, CA, USA, 23–26 July 2006. [Google Scholar]
- Committee on the Recommended Social and Behavioral Domains and Measures for Electronic Health Records; Board on Population Health and Public Health Practice; Institute of Medicine. Capturing Social and Behavioral Domains and Measures in Electronic Health Records: Phase 2; National Academies Press: Cambridge, MA, USA, 2015; ISBN 0309312426. [Google Scholar]
- CEP Providers|Low Back Pain. Available online: https://cep.health/clinical-products/low-back-pain/ (accessed on 19 March 2020).
- Lamy, J.B. Owlready: Ontology-Oriented Programming in Python with Automatic Classification and High Level Constructs for Biomedical Ontologies. Artif. Intell. Med. 2017, 80, 11–28. [Google Scholar] [CrossRef] [Green Version]
- Davis, F.D. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. MIS Q. Manag. Inf. Syst. 1989, 13, 319–339. [Google Scholar] [CrossRef] [Green Version]








| Level 1 Plan | |
| Goal: | Develop and deliver a personalized course to a patient |
| Parameters: | Patient P, diagnosed condition C, prescribed treatment T |
| Preconditions: | None |
| Body: |
|
| Level 2 Plan | |
| Goal: | Develop and deliver a lesson with an established scope to a patient |
| Parameters: | Patient P, lesson scope S |
| Preconditions: | None |
| Body: |
|
| Level 3 Plans | |
| Goal: | Deliver a BUK to a patient |
| Parameters: | Patient P, BUK B |
| Preconditions | B is a Content BUK |
| Body |
|
| Preconditions | B is a Q&A BUK |
| Body |
|
| Level 4 Plans | |
| Goal: | Update the comprehension level of a patient |
| Parameters: | Patient P, performance log L |
| Preconditions | L contains at least n entries capturing responses to questions from Q&A BUKs |
| Body |
|
| # | Interaction Description |
|---|---|
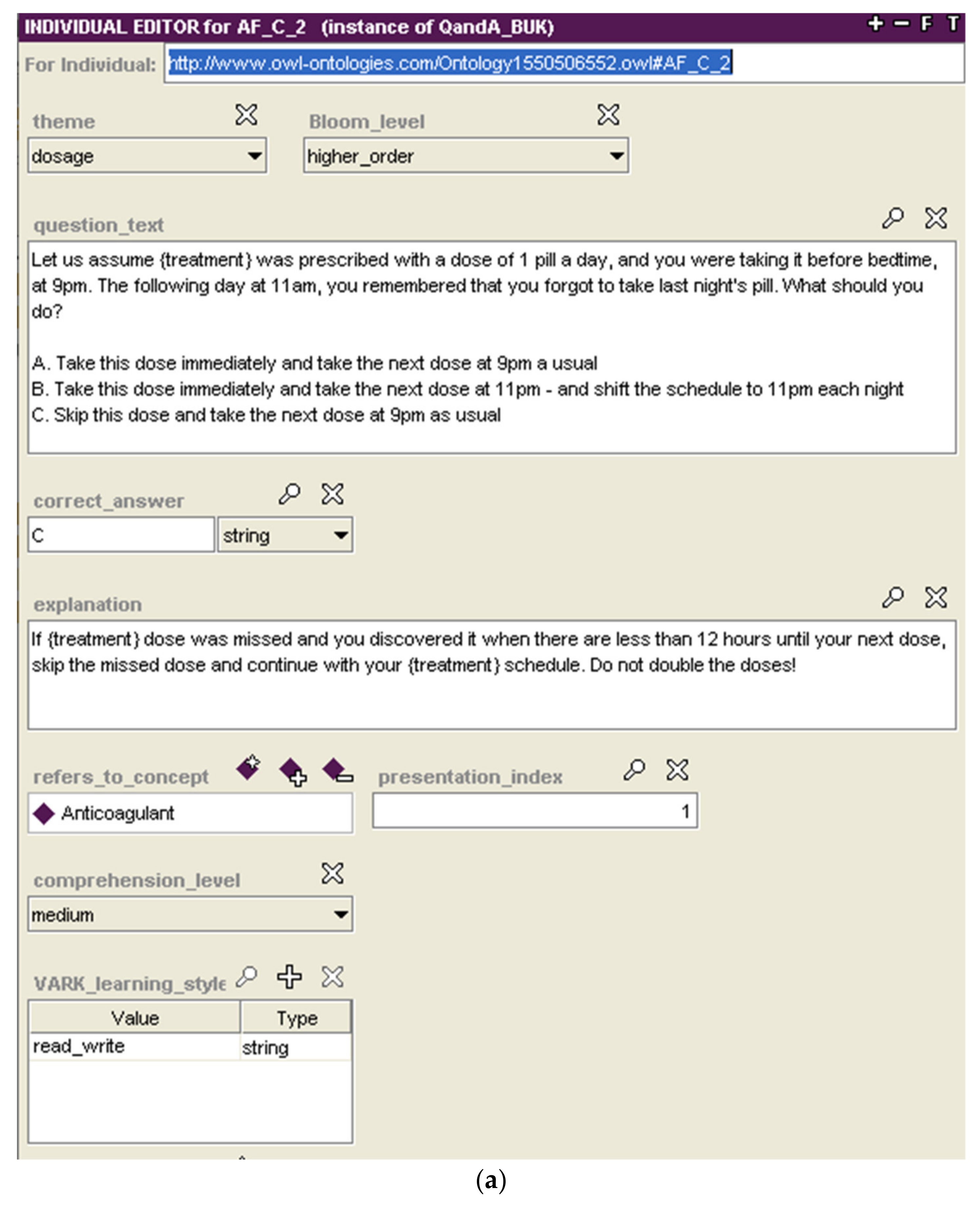
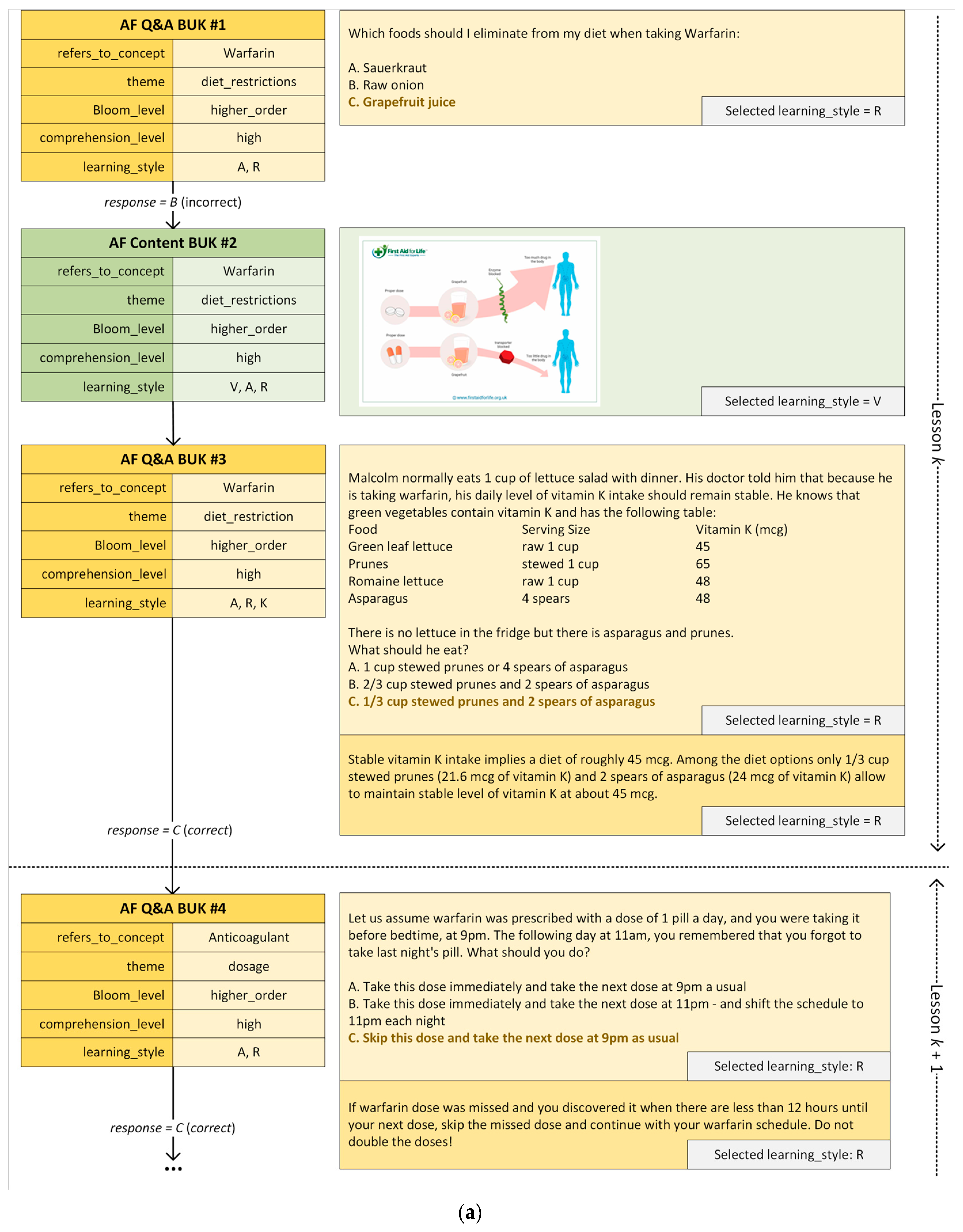
| 1 | Mario is presented a Q&A BUK (AF Q&A BUK #1) for diet restrictions while taking warfarin and associated with Bloom’s higher-order learning. |
| 2 | Mario provides an incorrect answer. However, due to his good performance track record (majority of his recent response were correct), Mario’s comprehension level is not changed. |
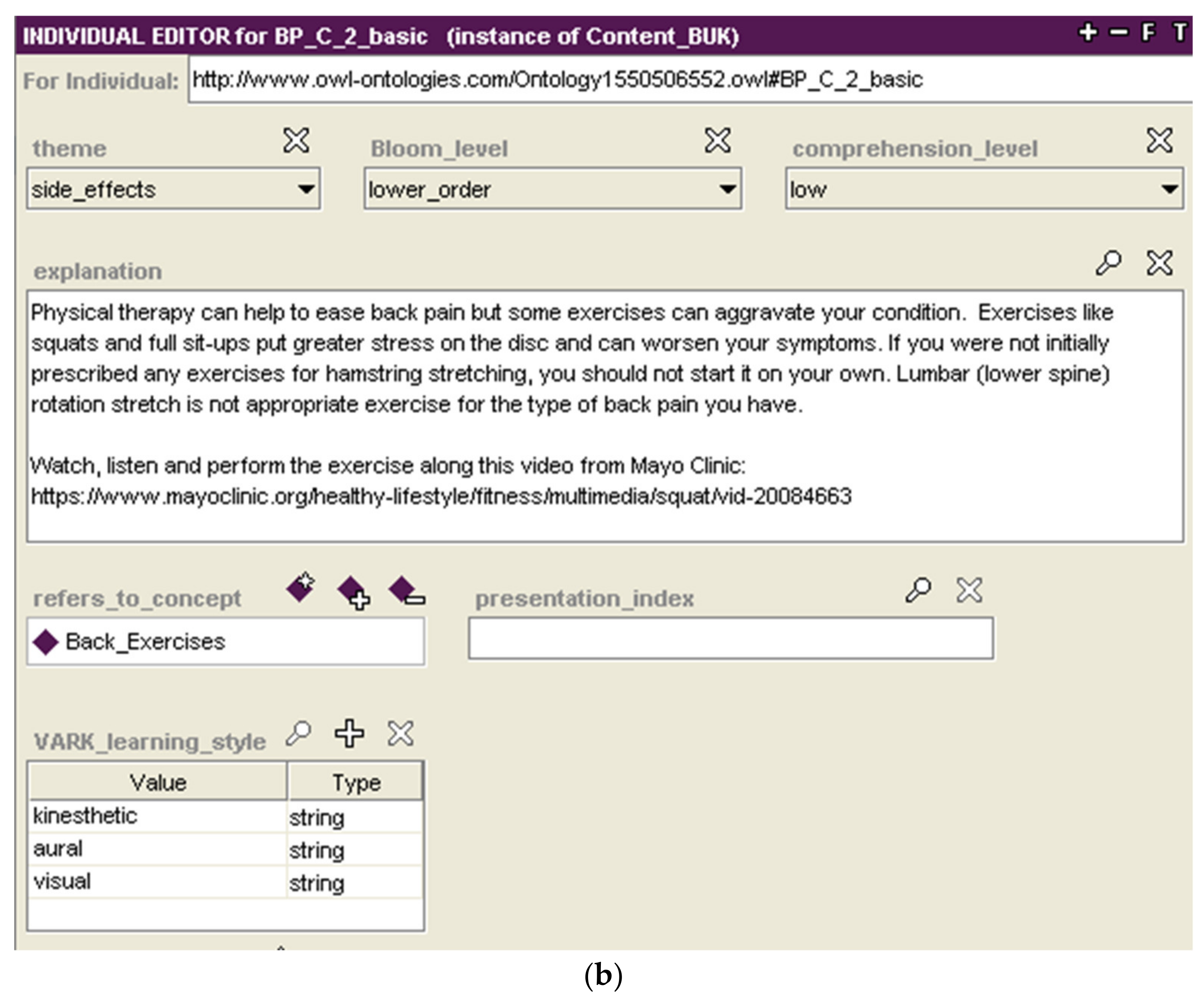
| 3 | Mario is presented a Content BUK (AF Content BUK #2) with additional explanation. |
| 4 | Because of the incorrect answer, Mario is presented with a different Q&A BUK (AF Q&A BUK #3) that is associated with the same concept, theme, and order of learning. |
| 5 | Mario provides the correct answer and is presented an additional short explanation to reinforce his learning. |
| 6 | Mario is presented a Q&A BUK (AF Q&A BUK #4) on dosing anticoagulant medication. Note that while this BUK is of a general nature and applicable to multiple anticoagulant medications, it has been customized for warfarin. |
| 7 | Mario provides the correct answer and is presented an additional short explanation to reinforce his learning. |
| # | Interaction Description |
|---|---|
| 1 | Anne is presented with a Q&A BUK (BP Q&A BUK #1) pertaining to symptoms of lumbar degenerative disk condition and associated with Bloom’s lower order learning. |
| 2 | Anne provides a correct answer and is presented with an additional short explanation in her preferred style. She also requests the explanation in the R style to further reinforce her learning. Moreover, due to her good recent performance, Anne’s comprehension level is promoted to medium. |
| 3 | Considering that Anne demonstrated a grasp of knowledge associated with a lower level of learning and that her comprehension level improved, a Q&A BUK associated with a higher-order learning and medium level (BP Q&A BUK #2) is presented to her. |
| 4 | Anne provides a correct answer and is presented with an additional short explanation to reinforce her learning. |
| Perceived Ease of Use | |||||||
| 1 | 2 | 3 | 4 | 5 | Mean | ||
| 1. The purpose of the lessons will be clear to patients? | Physicians | 1 | 2 | 4.67 | |||
| Patient representatives | 1 | 4 | 1 | 4.00 | |||
| 2. The structure (Q&A followed by Content BUK) of the lessons will be clear to patients? | Physicians | 3 | 5.00 | ||||
| Patient representatives | 1 | 1 | 4 | 4.50 | |||
| 3. The transitions between questions and explanations are intuitive and will be understandable to patients? | Physicians | 3 | 5.00 | ||||
| Patient representatives | 1 | 3 | 2 | 4.17 | |||
| Perceived Usefulness | |||||||
| 1 | 2 | 3 | 4 | 5 | Mean | ||
| 4. The content of the lessons is appropriately tailored to different level of health literacy? | Physicians | 1 | 1 | 1 | 4.00 | ||
| Patient representatives | 2 | 2 | 2 | 4.00 | |||
| Perceived Intention to Use | |||||||
| 1 | 2 | 3 | 4 | 5 | Mean | ||
| 5. Having access to personalized materials via lesson can help patients to better manage their condition? | Physicians | 1 | 2 | 4.33 | |||
| Patient representatives | 1 | 2 | 3 | 4.33 | |||
| Recommendation | |||||||
| No | Unsure | Yes | Not answered | ||||
| 6. Would you recommend such personalized teaching framework to every patient? | Physicians | 1 | 2 | 0 | |||
| Patient representatives | 1 | 3 | 2 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michalowski, M.; Wilk, S.; Michalowski, W.; O’Sullivan, D.; Bonaccio, S.; Parimbelli, E.; Carrier, M.; Le Gal, G.; Kingwell, S.; Peleg, M. A Health eLearning Ontology and Procedural Reasoning Approach for Developing Personalized Courses to Teach Patients about Their Medical Condition and Treatment. Int. J. Environ. Res. Public Health 2021, 18, 7355. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147355
Michalowski M, Wilk S, Michalowski W, O’Sullivan D, Bonaccio S, Parimbelli E, Carrier M, Le Gal G, Kingwell S, Peleg M. A Health eLearning Ontology and Procedural Reasoning Approach for Developing Personalized Courses to Teach Patients about Their Medical Condition and Treatment. International Journal of Environmental Research and Public Health. 2021; 18(14):7355. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147355
Chicago/Turabian StyleMichalowski, Martin, Szymon Wilk, Wojtek Michalowski, Dympna O’Sullivan, Silvia Bonaccio, Enea Parimbelli, Marc Carrier, Grégoire Le Gal, Stephen Kingwell, and Mor Peleg. 2021. "A Health eLearning Ontology and Procedural Reasoning Approach for Developing Personalized Courses to Teach Patients about Their Medical Condition and Treatment" International Journal of Environmental Research and Public Health 18, no. 14: 7355. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147355