
Development and Validation of a Knowledge, Attitudes and Practices Questionnaire on COVID-19 (KAP COVID-19)


Abstract
:1. Introduction
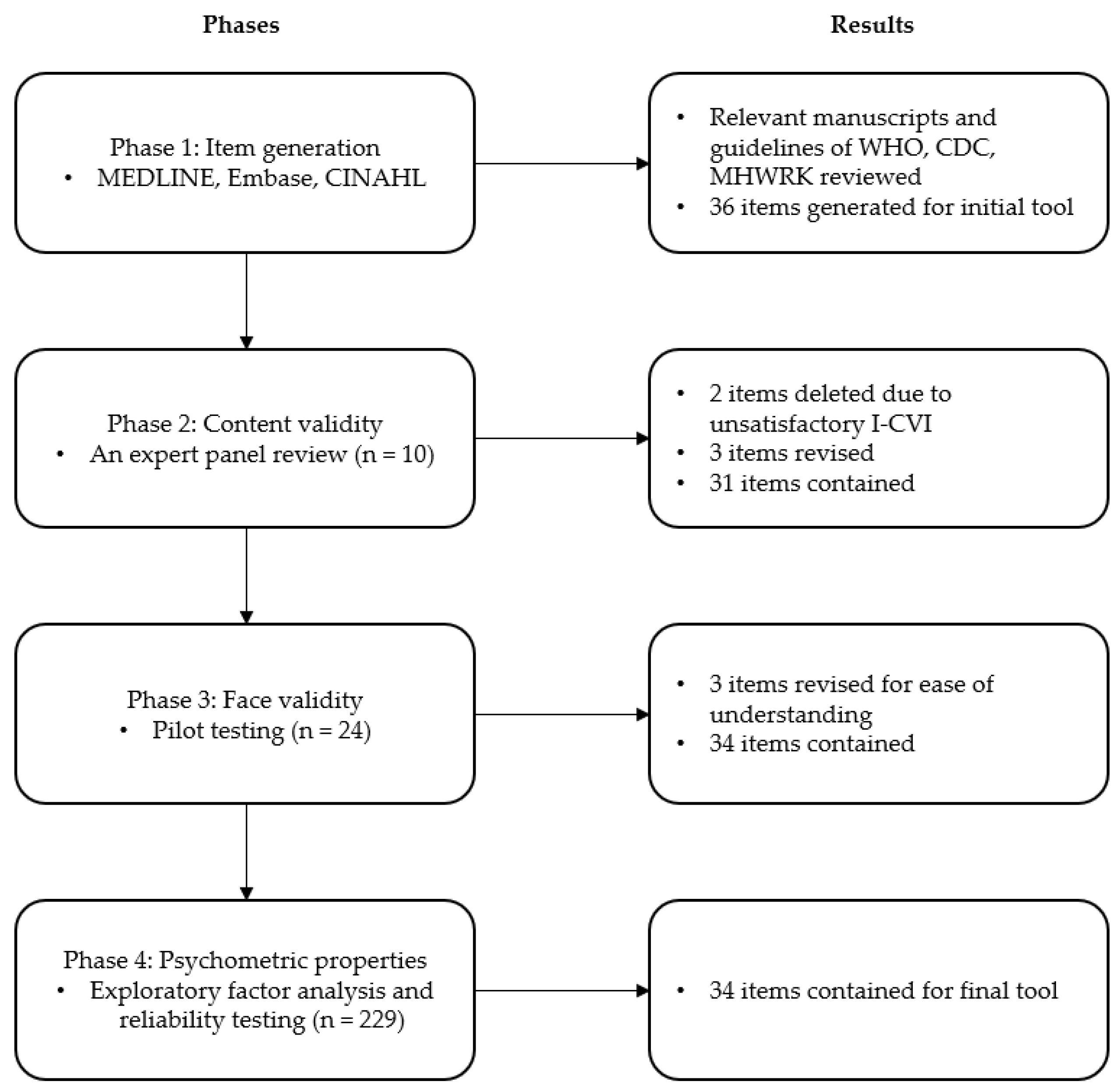
2. Materials and Methods
2.1. Phase 1: Item Generation
2.2. Phase 2: Content Validity
2.3. Phase 3: Face Validity
2.4. Phase 4: Psychometric Analysis
2.5. Sample and Data Collection
2.6. Statistical Analysis
2.7. Ethical Consideration
3. Results
3.1. Demographic Characteristics
3.1.1. Pilot Test
3.1.2. Main Study
3.2. Phase 1: Item Generation
3.3. Phase 2: Content Validity
3.4. Phase 3: Face Validity
3.5. Phase 4: Psychometric Properties
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hossain, M.F.; Hasana, S.; Al Mamun, A.; Uddin, M.S.; Wahed, M.I.I.; Sarker, S.; Behl, T.; Ullah, I.; Begum, Y.; Bulbul, I.J.; et al. COVID-19 Outbreak: Pathogenesis, Current Therapies, and Potentials for Future Management. Front. Pharmacol. 2020, 11, 563478. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease (COVID-19) Weekly Epidemiological Update. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update---27-january-2021 (accessed on 29 January 2021).
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Stasi, C.; Fallani, S.; Voller, F.; Silvestri, C. Treatment for COVID-19: An overview. Eur. J. Pharmacol. 2020, 889, 173644. [Google Scholar] [CrossRef] [PubMed]
- Charitos, I.A.; Ballini, A.; Bottalico, L.; Cantore, S.; Passarelli, P.C.; Inchingolo, F.; D’Addona, A.; Santacroce, L. Special features of SARS-CoV-2 in daily practice. World J. Clin. Cases 2020, 8, 3920–3933. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare of the Republic of Korea. Coronavirus Disease-19 Latest Updates: Cases in Korea. 2021. Available online: http://ncov.mohw.go.kr/en/ (accessed on 1 February 2021).
- Zhong, B.-L.; Luo, W.; Li, H.-M.; Zhang, Q.-Q.; Liu, X.-G.; Li, W.-T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- Clements, J.M. Knowledge and Behaviors toward COVID-19 among US Residents during the Early Days of the Pandemic: Cross-Sectional Online Questionnaire. JMIR Public Health Surveill. 2020, 6, e19161. [Google Scholar] [CrossRef] [PubMed]
- Abuhammad, S. Parents’ knowledge and attitude towards COVID-19 in children: A Jordanian Study. Int. J. Clin. Pract. 2021, 75, e13671. [Google Scholar] [CrossRef] [PubMed]
- Al-Hanawi, M.K.; Angawi, K.; Alshareef, N.; Qattan, A.; Helmy, H.Z.; Abudawood, Y.; Alqurashi, M.; Kattan, W.M.; Kadasah, N.A.; Chijere, G.; et al. Knowledge, Attitude and Practice Toward COVID-19 Among the Public in the Kingdom of Saudi Arabia: A Cross-Sectional Study. Front. Public Health 2020, 8, 217. [Google Scholar] [CrossRef] [PubMed]
- Kasemy, Z.A.; Bahbah, W.A.; Zewain, S.K.; Haggag, M.G.; Alkalash, S.H.; Zahran, E.; Desouky, D.E. Knowledge, Attitude and Practice toward COVID-19 among Egyptians. J. Epidemiol. Glob. Health 2020, 10, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.; Chen, J.; Chow, K.; Law, B.; Chan, D.; So, W.; Leung, A.; Chan, C. Knowledge, Attitudes and Practices towards COVID-19 amongst Ethnic Minorities in Hong Kong. Int. J. Environ. Res. Public Health 2020, 17, 7878. [Google Scholar] [CrossRef] [PubMed]
- Devon, H.A.; Block, M.E.; Moyle-Wright, P.; Ernst, D.M.; Hayden, S.J.; Lazzara, D.J.; Savoy, S.M.; Kostas-Polston, E. A psychometric toolbox for testing validity and reliability. J. Nurs. Scholarsh. 2007, 39, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Beck, C.T. Nursing Research: Generating and Assessing Evidence in Nursing Practice, 10th ed.; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2016. [Google Scholar]
- Alduraywish, A.A.; Srivastava, K.C.; Shrivastava, D.; Sghaireen, M.G.; AlSharari, A.F.; Al-Johani, K.; Alam, M.K. A Countrywide Survey in Saudi Arabia Regarding the Knowledge and Attitude of Health Care Professionals about Coronavirus Disease (COVID-19). Int. J. Environ. Res. Public Health 2020, 17, 7415. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; SAGE Publications, Inc.: New York, NY, USA, 2015. [Google Scholar]
- Pett, M.A.; Lackey, N.R.; Sullivan, J.J. Making Sense of Factor Analysis: The Use of Factor Analysis for Instrument Development in Health Care Research, 1st ed.; SAGE Publications, Inc.: New York, NY, USA, 2003. [Google Scholar]
- Moridi, M.; Pazandeh, F.; Hajian, S.; Potrata, B. Development and psychometric properties of Midwives’ Knowledge and Practice Scale on Respectful Maternity Care (MKP-RMC). PLoS ONE 2020, 15, e0241219. [Google Scholar] [CrossRef] [PubMed]
- Fu, E.; White, M.A.; Hughto, J.M.; Steiner, B.; Willis, E. Development of the Physical Activity Tracking Preference Questionnaire. Int. J. Exerc. Sci. 2019, 12, 297–309. [Google Scholar]
- Ekolu, S.; Quainoo, H. Reliability of assessments in engineering education using Cronbach’s alpha, KR and split-half methods. Glob. J. Eng. Educ. 2019, 21, 24–29. [Google Scholar]
- Anthoine, E.; Moret, L.; Regnault, A.; Sébille, V.; Hardouin, J.B. Sample size used to validate a scale: A review of publications on newly-developed patient reported outcomes measures. Health Qual. Life Outcomes 2014, 12, 176. [Google Scholar] [CrossRef] [Green Version]
- Anthoine, E.; Delmas, C.; Coutherut, J.; Moret, L. Development and psychometric testing of a scale assessing the sharing of medical information and interprofessional communication: The CSI scale. BMC Health Serv. Res. 2014, 14, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; Zhou, M.; Tang, F.; Wang, Y.; Nie, H.; Zhang, L.; You, G. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China. J. Hosp. Infect. 2020, 105, 183–187. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | (N = 229) |
|---|---|
| Age (years), M ± SD (range) | 21.1 ± 1.7 (18–33) |
| Gender, n (%) | |
| Female | 210 (91.7) |
| Male | 19 (8.3) |
| Grade, n (%) | |
| Freshman | 26 (11.4) |
| Sophomore | 40 (17.5) |
| Junior | 95 (41.5) |
| Senior | 68 (29.7) |
| KAP COVID-19 | |
| Knowledge scale, M ± SD (range) | 8.9 ± 2.0 (3–13) |
| Attitude scale, M ± SD (range) | 32.8 ± 6.9 (16–46) |
| Practices scale M ± SD (range) | 41.4 ± 7.7 (19–56) |
| Total score, M ± SD (range) | 83.1 ± 11.1 (50–110) |
| Item | I-CVI |
|---|---|
| Knowledge subscale: Level of knowledge on COVID-19 symptoms, diagnosis, treatment and transmission | |
| 1.0 |
| 1.0 |
| 0.4 † |
| 0.8 |
| 0.8 |
| 0.8 |
| 0.9 |
| 1.0 ‡ |
| 0.9 |
| 1.0 |
| 0.5 † |
| 0.8 ‡ |
| 0.9 ‡ |
| 1.0 |
| 1.0 |
| Attitudes subscale: The level of attitude towards the pandemic crisis and healthcare system | |
| 1.0 |
| 0.9 |
| 0.8 |
| 1.0 |
| 1.0 |
| 0.8 |
| 1.0 |
| Practices subscale: The level of self-protecting practices during the pandemic crisis | |
| 1.0 |
| 1.0 |
| 1.0 |
| 1.0 |
| 1.0 |
| 0.9 |
| 0.9 |
| 0.8 |
| 0.9 |
| 1.0 |
| 0.9 |
| 1.0 |
| 0.8 |
| 0.7 |
| Factor | Item | Factor Loading a | Eigenvalue | VE (%) | CVE (%) | Cronbach’s α |
|---|---|---|---|---|---|---|
| Knowledge subscale | 0.532 b | |||||
| Nature of the disease | 1 | 0.781 | 4.219 | 12.409 | 12.409 | |
| 2 | 0.534 | |||||
| Signs and symptoms | 3 | 0.744 | 2.693 | 7.922 | 20.331 | |
| 4 | 0.651 | |||||
| Diagnosis | 5 | 0.657 | 2.545 | 7.485 | 27.816 | |
| 6 | 0.854 | |||||
| Medical management | 7 | 0.554 | 2.235 | 6.575 | 34.391 | |
| 8 | 0.677 | |||||
| 9 | 0.742 | |||||
| PUI management and quarantine | 10 | 0.751 | 1.678 | 4.963 | 39.326 | |
| 11 | 0.823 | |||||
| Precautionary strategy | 12 | 0.851 | 1.585 | 4.663 | 43.989 | |
| 13 | 0.820 | |||||
| Attitudes subscale | 0.720 | |||||
| Beliefs about COVID-19 prevention | 14 | 0.897 | 1.541 | 4.531 | 48.521 | |
| 15 | 0.963 | |||||
| 16 | 0.901 | |||||
| Beliefs about healthcare provider role | 17 | 0.496 | 1.481 | 4.355 | 52.875 | |
| 18 | 0.810 | |||||
| 19 | 0.731 | |||||
| 20 | 0.701 | |||||
| Practices subscale | 0.851 | |||||
| Personal hygiene practices | 21 | 0.716 | 1.400 | 4.117 | 56.992 | |
| 22 | 0.748 | |||||
| 23 | 0.593 | |||||
| 24 | 0.605 | |||||
| 25 | 0.561 | |||||
| Restricting behavior | 26 | 0.587 | 1.296 | 3.811 | 60.803 | |
| 27 | 0.512 | |||||
| 28 | 0.778 | |||||
| 29 | 0.781 | |||||
| 30 | 0.651 | |||||
| 31 | 0.680 | |||||
| 32 | 0.517 | |||||
| 33 | 0.621 | |||||
| 34 | 0.694 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, D.-I. Development and Validation of a Knowledge, Attitudes and Practices Questionnaire on COVID-19 (KAP COVID-19). Int. J. Environ. Res. Public Health 2021, 18, 7493. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147493
Park D-I. Development and Validation of a Knowledge, Attitudes and Practices Questionnaire on COVID-19 (KAP COVID-19). International Journal of Environmental Research and Public Health. 2021; 18(14):7493. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147493
Chicago/Turabian StylePark, Da-In. 2021. "Development and Validation of a Knowledge, Attitudes and Practices Questionnaire on COVID-19 (KAP COVID-19)" International Journal of Environmental Research and Public Health 18, no. 14: 7493. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147493