
Evaluation of a Pediatric Obesity Management Toolkit for Health Care Professionals: A Quasi-Experimental Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Video Development
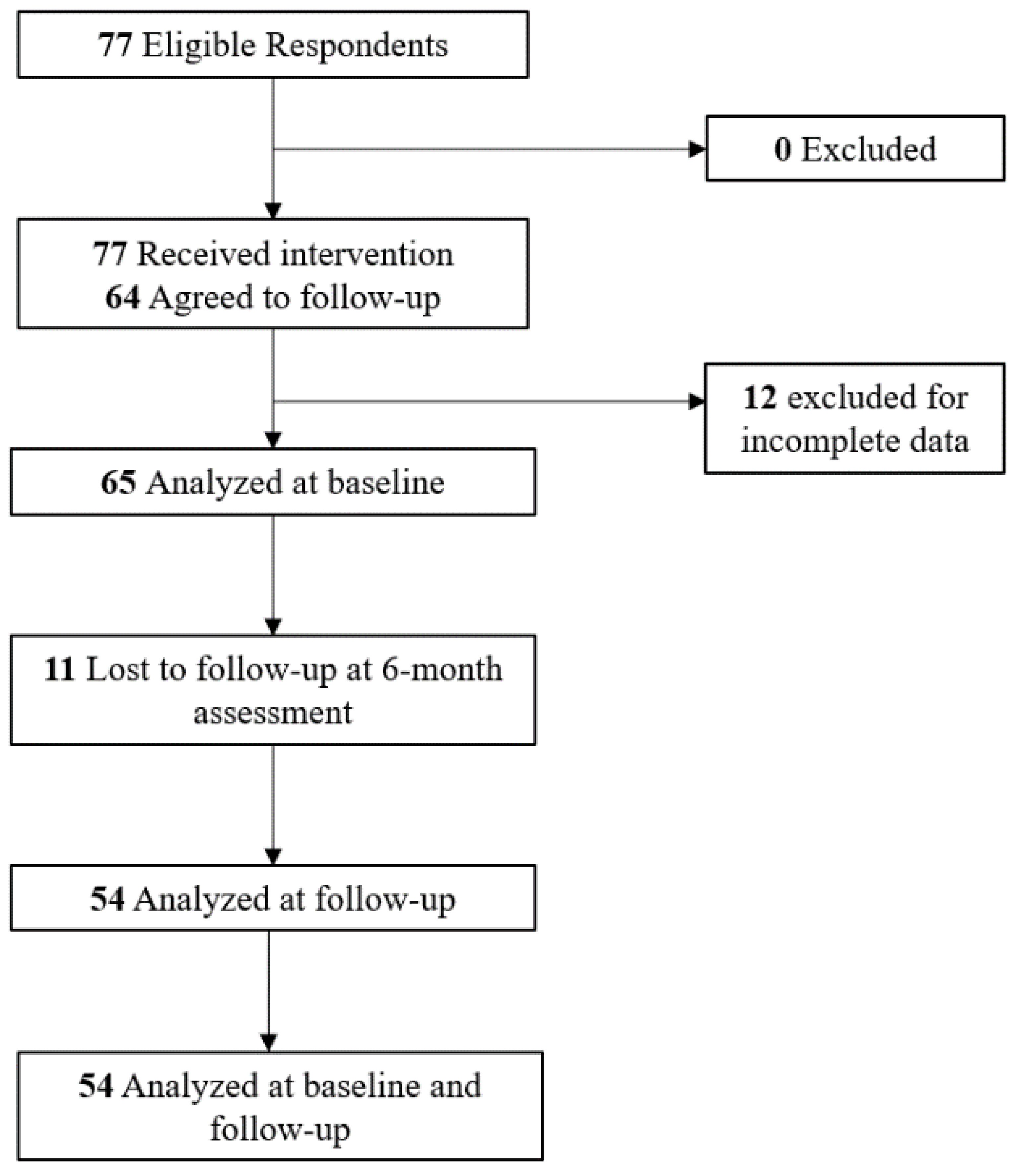
2.2. Participants/Data Collection
2.3. Study Outcomes
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Questions about Current Practice and 5A’s
3.3. Baseline and Post-Video Knowledge and Self-Efficacy Ratings
3.4. Evaluation of the Videos
3.5. Follow-Up Assessment
3.6. Impact on Clinic Practice at Follow-Up
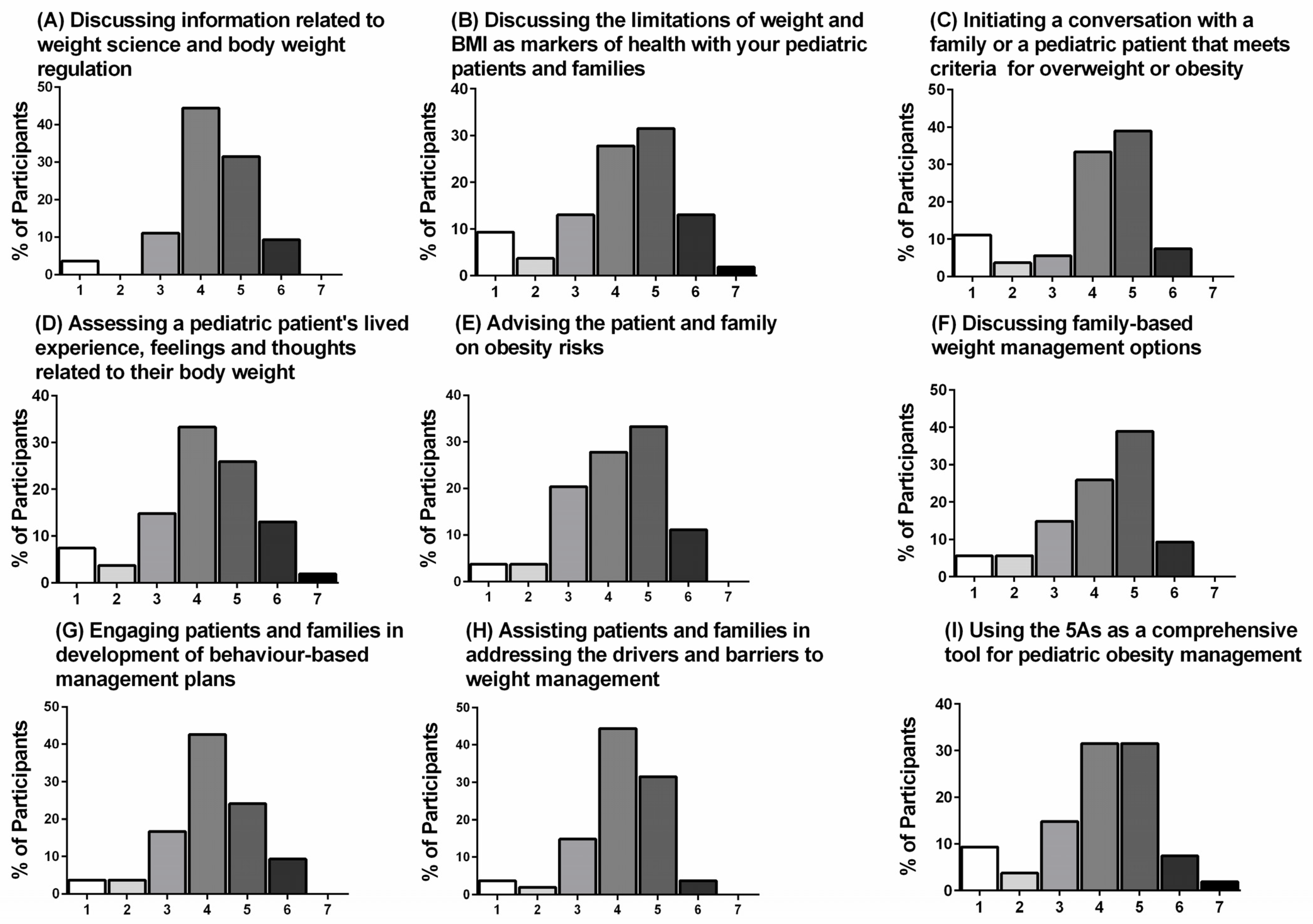
3.7. Self-Efficacy Ratings from Baseline to Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ruiz, L.D.; Zuelch, M.L.; Dimitratos, S.M.; Scherr, R.E. Adolescent Obesity: Diet Quality, Psychosocial Health, and Cardiometabolic Risk Factors. Nutrients 2019, 12, 43. [Google Scholar] [CrossRef] [Green Version]
- Campbell-Scherer, D.L.; Asselin, J.; Osunlana, A.M.; Fielding, S.; Anderson, R.; Rueda-Clausen, C.F.; Johnson, J.A.; Ogunleye, A.A.; Cave, A.; Manca, D.; et al. Implementation and evaluation of the 5As framework of obesity management in primary care: Design of the 5As Team (5AsT) randomized control trial. Implement. Sci. 2014, 9, 78. [Google Scholar] [CrossRef] [Green Version]
- Jelalian, E.; Boergers, J.; Alday, C.S.; Frank, R. Survey of physician attitudes and practices related to pediatric obesity. Clin. Pediatr. 2003, 42, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Alexander, S.C.; Østbye, T.; Pollak, K.I.; Gradison, M.; Bastian, L.A.; Brouwer, R.J.N. Physicians’ beliefs about discussing obesity: Results from focus groups. Am. J. Health Promot. 2007, 21, 498–500. [Google Scholar] [CrossRef] [PubMed]
- Cooke, N.K.; Ash, S.L.; Goodell, L.S. Medical students’ perceived educational needs to prevent and treat childhood obesity. Educ. Health 2017, 30, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Smith, M.L.; Kromann, L.; Ory, M.G. Medical Students and Childhood Obesity: Health Disparity and Implication for Education. Int. J. Environ. Res. Public Health 2019, 16, 2578. [Google Scholar] [CrossRef] [Green Version]
- Lenders, C.M.; Manders, A.J.; Perdomo, J.E.; Ireland, K.A.; Barlow, S.E. Addressing Pediatric Obesity in Ambulatory Care: Where Are We and Where Are We Going? Curr. Obes. Rep. 2016, 5, 214–240. [Google Scholar] [CrossRef] [Green Version]
- Van Gerwen, M.; Franc, Č.; Rosman, S.; Le Vaillant, M.; Pelletier-Fleury, N. Primary care physicians’ knowledge, attitudes, beliefs and practices regarding childhood obesity: A systematic review. Obes. Rev. 2009, 10, 227–236. [Google Scholar] [CrossRef]
- Mikhailovich, K.; Morrison, P. Discussing childhood overweight and obesity with parents: A health communication dilemma. J. Child Health Care 2007, 11, 311–322. [Google Scholar] [CrossRef]
- Walker, O.; Strong, M.; Atchinson, R.; Saunders, J.; Abbott, J. A qualitative study of primary care clinicians’ views of treating childhood obesity. BMC Fam. Pract. 2007, 8, 50. [Google Scholar] [CrossRef] [Green Version]
- McPherson, A.C.; Knibbe, T.J.; Oake, M.; Swift, J.A.; Browne, N.; Ball, G.D.C.; Hamilton, J. “Fat is really a four-letter word”: Exploring weight-related communication best practices in children with and without disabilities and their caregivers. Child Care Health Dev. 2018, 44, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Latner, J.D. Stigma, obesity, and the health of the nation’s children. Psychol. Bull. 2007, 133, 557–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gudzune, K.A.; Johnson, V.R.; Bramante, C.T.; Stanford, F.C. Geographic Availability of Physicians Certified by the American Board of Obesity Medicine Relative to Obesity Prevalence. Obesity 2019, 27, 1958–1966. [Google Scholar] [CrossRef]
- Mastrocola, M.R.; Roque, S.S.; Benning, L.V.; Stanford, F.C. Obesity education in medical schools, residencies, and fellowships throughout the world: A systematic review. Int. J. Obes. 2020, 44, 269–279. [Google Scholar] [CrossRef]
- Flodgren, G.; Deane, K.; Dickinson, H.O.; Kirk, S.; Alberti, H.; Beyer, F.R.; Brown, J.G.; Penney, T.L.; Summerbell, C.D.; Eccles, M.P. Interventions to change the behaviour of health professionals and the organisation of care to promote weight reduction in overweight and obese people. Cochrane Database Syst. Rev. 2010, 3, CD000984. [Google Scholar] [CrossRef] [PubMed]
- Dietz, W.H.; Baur, L.; Hall, K.; Puhl, R.M.; Taveras, E.M.; Uauy, R.; Kopelman, P. Management of obesity: Improvement of health-care training and systems for prevention and care. Lancet 2015, 385, 2521–2533. [Google Scholar] [CrossRef]
- Mayer, R.E. Applying the science of learning to medical education. Med. Educ. 2010, 44, 543–549. [Google Scholar] [CrossRef]
- Kenny, K.P.; Alkazme, A.M.; Day, P.F. The effect of viewing video clips of paediatric local anaesthetic administration on the confidence of undergraduate dental students. Eur. J. Dent. Educ. 2017, 22, e57–e62. [Google Scholar] [CrossRef]
- Thomson, A.A.; Brown, M.; Zhang, S.; Stern, E.; Hahn, P.M.; Reid, R.L. Evaluating Acquisition of Knowledge about Infertility Using a Whiteboard Video. J. Obstet. Gynaecol. Can. 2016, 38, 646–650. [Google Scholar]
- Haywood, C., Jr.; Lanzkron, S.; Hughes, M.T.; Brown, R.; Massa, M.; Ratanawongsa, N.; Beach, M.C. A video-intervention to improve clinician attitudes toward patients with sickle cell disease: The results of a randomized experiment. J. Gen. Intern. Med. 2011, 26, 518–523. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, G.; Roddy, M.; Langsam, D.; Agrawal, D. An educational video improves technique in performance of pediatric lumbar punctures. Pediatr. Emerg. Care 2012, 28, 12–16. [Google Scholar] [CrossRef]
- Rincon-Subtirelu, M. Education as a tool to modify anti-obesity bias among Pediatric residents. Int. J. Med. Educ. 2017, 8, 77–78. [Google Scholar] [CrossRef]
- Whitlock, E.P. Evaluating primary care behavioral counseling interventions: An evidence-based approach. Am. J. Prev. Med. 2002, 22, 267–284. [Google Scholar] [CrossRef]
- Rueda-Clausen, C.F.; Benterud, E.; Bond, T.; Olszowka, R.; Vallis, M.T.; Sharma, A.M. Effect of implementing the 5As of obesity management framework on provider-patient interactions in primary care. Clin. Obes. 2014, 4, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, J.; Hadjiyannakis, S.; Clark, L.; Buchholz, A. 5As of Pediatric Obesity Management in the 3rd National Obesity Summit. Can. J. Diabetes. 2013, 37, S217–S218. [Google Scholar] [CrossRef] [Green Version]
- Bernard-Genest, J.; Chu, L.; Dettmer, E.; Walsh, C.M.; McPherson, A.C.; Strub, J.; Steinberg, A.; Steinegger, C.; Hamilton, J.K. Talking about Weight With Families-Helping Health Care Professionals Start the Conversation: A Nonrandomized Controlled Trial. Clin. Pediatr. 2020, 59, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Campoverde Reyes, K.J.; Perez, N.P.; Czepiel, K.S.; Shaw, A.Y.; Stanford, F.C. Exploring Pediatric Obesity Training, Perspectives, and Management Patterns Among Pediatric Primary Care Physicians. Obesity 2021, 29, 159–170. [Google Scholar] [CrossRef]
- McPherson, A.C.; Hamilton, J.; Kingsnorth, S.; Knibbe, T.J.; Peters, M.; Swift, J.A.; Krog, K.; Chen, L.; Steinberg, A.; Ball, G.D.C. Communicating with children and families about obesity and weight-related topics: A scoping review of best practices. Obes. Rev. 2017, 18, 164–182. [Google Scholar] [CrossRef]
- Hadjiyannakis, S.; Buchholz, A.; Chanoine, J.-P.; Jetha, M.M.; Gaboury, L.; Hamilton, J.; Birken, C.; Morrison, K.M.; Legault, L.; Bridger, T.; et al. The Edmonton Obesity Staging System for Pediatrics: A proposed clinical staging system for paediatric obesity. Paediatr. Child Health 2016, 21, 21–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inf. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Guide for constructing self-efficacy scales. Self-Effic. Beliefs Adolesc. 2006, 5, 307–337. [Google Scholar]
- Whittemore, R.; Grey, M.; Lindemann, E.; Ambrosino, J.; Jaser, S. Development of an Internet coping skills training program for teenagers with type 1 diabetes. Comput. Inf. Nurs. 2010, 28, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croghan, I.T.; Ebbert, J.O.; Njeru, J.W.; Rajjo, T.I.; Lynch, B.A.; DeJesus, R.S.; Jensen, M.D.; Fischer, K.M.; Phelan, S.; Kaufman, T.K.; et al. Identifying Opportunities for Advancing Weight Management in Primary Care. J. Prim. Care Community Health 2019, 10, 2150132719870879. [Google Scholar] [CrossRef] [PubMed]
- Davis, D.A.; Mazmanian, P.E.; Fordis, M.; Van Harrison, R.T.K.E.; Thorpe, K.E.; Perrier, L. Accuracy of physician self-assessment compared with observed measures of competence: A systematic review. JAMA 2006, 296, 1094–1102. [Google Scholar] [CrossRef]
- Holloway, A.; Watson, H.E. Role of self-efficacy and behaviour change. Int. J. Nurs. Pract. 2002, 8, 106–115. [Google Scholar]
- Woolfitt, Z. The Effective Use of Video in Higher Education. 2015. Cited 28 September 2016. Available online: https://www.inholland.nl/media/10230/the-effective-use-of-video-in-higher-education-woolfitt-october-2015.pdf (accessed on 21 August 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Video | Description | |
|---|---|---|
| 1. Introduction to Weight Science | This video presents background information, including the biologic processes involved in body weight regulation. |  |
| 2. A Word About BMI | This video discusses how to use growth charts, as well as the limitations of weight and BMI as markers of health. |  |
| 3. ASK | This video reviews how to approach discussions about obesity with pediatric patients and their caregivers. |  |
| 4. ASSESS | This video reviews how to comprehensively assess children and youth with obesity using The Edmonton Obesity Staging System for Pediatrics, which captures the severity of disease, as well as factors that complicate management, within four domains of health most commonly encountered in obesity—metabolic, mechanical, mental health, and social milieu (the 4Ms). |  |
| 5. ADVISE, AGREE, and ASSIST | This video discusses the interventions for pediatric obesity management in the primary care setting, how to ensure patient engagement in the process, and how to sustain therapy. |  |
| 6. Putting it All Together | This video summarizes each of the 5As and how to use them as a comprehensive tool for pediatric obesity management, within a sample patient encounter. |  |
| Baseline (n = 65) | Follow-Up (n = 54) | |
|---|---|---|
| Age group (%) | ||
| • <18 years | 0 | 0 |
| • 18–24 years | 1.5 | 1.9 |
| • 25–34 years | 44.6 | 48.1 |
| • 35–44 years | 24.6 | 24.1 |
| • 45–54 years old | 7.7 | 3.7 |
| • >55 years | 20.0 | 20.4 |
| I prefer not to answer | 1.5 | 1.9 |
| Sex (%) | ||
| • Male | 16.9 | 18.5 |
| • Female | 83.1 | 81.5 |
| Ethnicity (%) | ||
| • White | 73.8 | 72.2 |
| • Black | 0 | 0 |
| • Hispanic or Latino | 3.1 | 3.7 |
| • Aboriginal | 1.5 | 1.9 |
| • Asian or Pacific Islander | 12.3 | 13.0 |
| • South Asian or Middle Eastern | 4.6 | 5.6 |
| • I prefer not to answer | 4.6 | 3.7 |
| Number of years in practice 1 | 9.5 (2.9–20.0) | 8.5 (2.6–20.0) |
| Baseline (n = 65) | Follow-Up (n = 54) | |
|---|---|---|
| In your current practice, how often do you see children who are overweight or obese? (%) | ||
| Never | 0 | 0 |
| Fewer than one patient every 12 months | 4.6 | 3.7 |
| At least one patient every 12 months | 3.1 | 3.7 |
| At least one patient every 6 months | 10.8 | 22.2 |
| At least one patient a month | 32.3 | 38.9 |
| At least one patient a week | 36.9 | 18.5 |
| At least one patient per day or more | 12.3 | 13.0 |
| In your current practice, do you use the 5As approach to Pediatric Obesity Management? (%) | ||
| Yes | 24.6 | 25.9 |
| No | 55.4 | 51.9 |
| I don’t know | 20.0 | 22.2 |
| Have you received training on using the 5As of Pediatric Obesity Management? (%) | ||
| Yes | 16.9 | |
| No | 78.5 | |
| I don’t know | 4.6 | |
| If yes, when did you receive this training? (%) | ||
| During health professional school | 27.3 | |
| An academic/education meeting | 54.5 | |
| Other | 18.2 | |
| If yes, what type of training did you receive? (%) | ||
| Didactive (Lecture format) | 27.3 | |
| Interactive | 9.1 | |
| E-learning | 9.1 | |
| Self-directed | 18.2 | |
| Combination | 36.4 | |
| If yes, how long was your training in total? (%) | ||
| <1 h | 54.5 | |
| 4 h | 9.1 | |
| 1 day–1 week | 36.4 | |
| 1 week | 0 |
| Question. | Baseline Rating (0–100) |
|---|---|
| Video 1: “Understanding information related to weight science and body weight regulation” | 73.0 (50.0–80.0) |
| Video 2: “Understanding how to use BMI growth charts in your practice” | 85.0 (65.5–95.0) |
| “Understanding the limitations of weight and BMI as markers of health” | 76.0 (50.0–92.5) |
| Video 4: “Understanding obesity related comorbidities” | 75.0 (60.0–85.0) |
| “Understanding the 4Ms framework” | 41.0 (8.5–70.0) |
| “Understanding potential root causes and drivers of weight gain and barriers for weight management” | 70.0 (50.0–80.0) |
| Video 6: “Knowledge about the 5As as a comprehensive tool for pediatric obesity management” | 31.0 (6.5–53.0) |
| Task | Baseline Rating (0–100) |
|---|---|
| Video 1: “Discussing information related to weight science and body weight regulation” | 69.0 (50.0–80.0) |
| Video 2: “Using BMI growth charts in your practice” | 90.0 (71.5–97.0) |
| “Discussing the limitations of weight and BMI as markers of health” | 75.0 (50.0–87.5) |
| Video 3: “Initiating conversation with a family or a pediatric patient that meets criteria for overweight or obesity” | 73.0 (50.0–90.0) |
| Video 4: “Assessing a pediatric patient’s lived experience, feelings, and thoughts related to their body weight” | 65.0 (43.0–80.0) |
| “Using the 4Ms framework” | 40.0 (11.0–67.5) |
| Video 5: “Advising the patient and family on obesity risks” | 75.0 (64.2–83.7) |
| “Discussing family-based weight management options” | 74.0 (50.0–84.5) |
| “Engaging patients and families in development of behavior-based management plans” | 62.0 (50.0–81.5) |
| “Assisting patients and families in addressing the drivers and barriers to weight management” | 60.0 (50.0–80.0) |
| Video 6: “Using the 5As as a comprehensive tool for pediatric obesity management” | 31.0 (6.5–53.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, B.P.; Hadjiyannakis, S.; Clark, L.; Buchholz, A.; Noseworthy, R.; Bernard-Genest, J.; Walsh, C.M.; McPherson, A.C.; Strub, J.; Strom, M.; et al. Evaluation of a Pediatric Obesity Management Toolkit for Health Care Professionals: A Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2021, 18, 7568. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147568
Patel BP, Hadjiyannakis S, Clark L, Buchholz A, Noseworthy R, Bernard-Genest J, Walsh CM, McPherson AC, Strub J, Strom M, et al. Evaluation of a Pediatric Obesity Management Toolkit for Health Care Professionals: A Quasi-Experimental Study. International Journal of Environmental Research and Public Health. 2021; 18(14):7568. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147568
Chicago/Turabian StylePatel, Barkha P., Stasia Hadjiyannakis, Laurie Clark, Annick Buchholz, Rebecca Noseworthy, Julie Bernard-Genest, Catharine M. Walsh, Amy C. McPherson, Jonah Strub, Michele Strom, and et al. 2021. "Evaluation of a Pediatric Obesity Management Toolkit for Health Care Professionals: A Quasi-Experimental Study" International Journal of Environmental Research and Public Health 18, no. 14: 7568. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147568