
Real-World Utilization of Target- and Immunotherapies for Lung Cancer: A Scoping Review of Studies Based on Routinely Collected Electronic Healthcare Data

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction
- (i)
- Data source characteristics: type of source, name, catchment area. Notably, data source types were classified into three main categories: (a) administrative/claims data (i.e., data for health system planning and management and health assistance claims), (b) “medical/health records” (i.e., documentation of clinical care) and (c) “cancer registries” [22,23];
- (ii)
- Study characteristics: study population, population size, cohort type (population-based, hospital-based), study period, follow-up duration and drugs or drugs regimens. Additionally, relevant information items such, as cancer-related characteristics, patients-related characteristics, drug utilizations, vital status, were also classified by sources of rcEHD used, whenever possible;
- (iii)
- Information on the utilization of target- and immunotherapies based on treatment line and LC histology (e.g., pattern of use, frequency molecular testing, survival).
3. Results
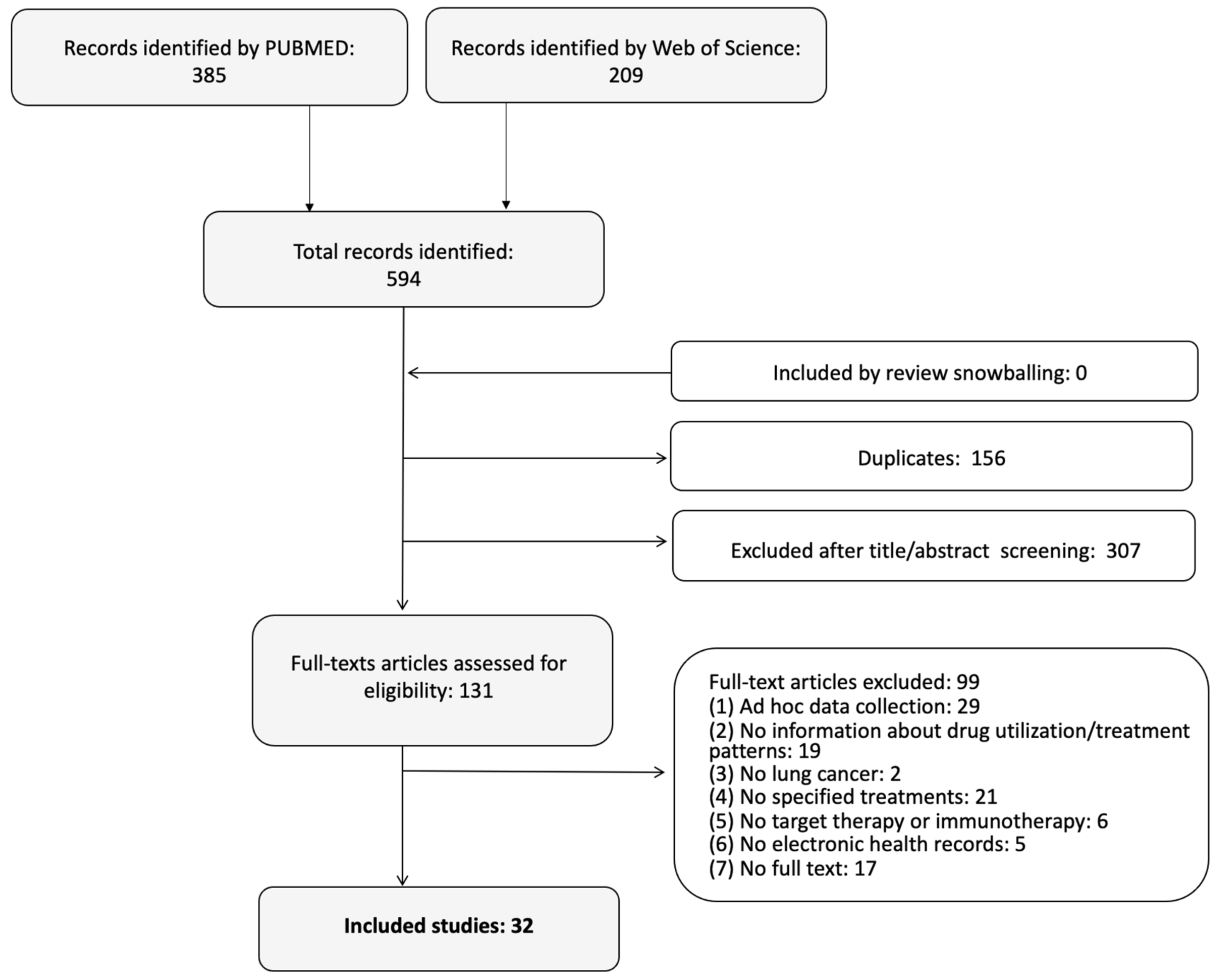
3.1. Literature Search Results
3.2. Source of Routinely Collected Electronic Healthcare Data (rcEHD) Used by Study
3.3. Characteristics of the Included Studies
3.4. Sources of rcEHD Used for Information Retrieval
3.5. Utilization of Target- or Immuno- Therapies for Non-Small-Cell Lung Cancers (NSCLC)
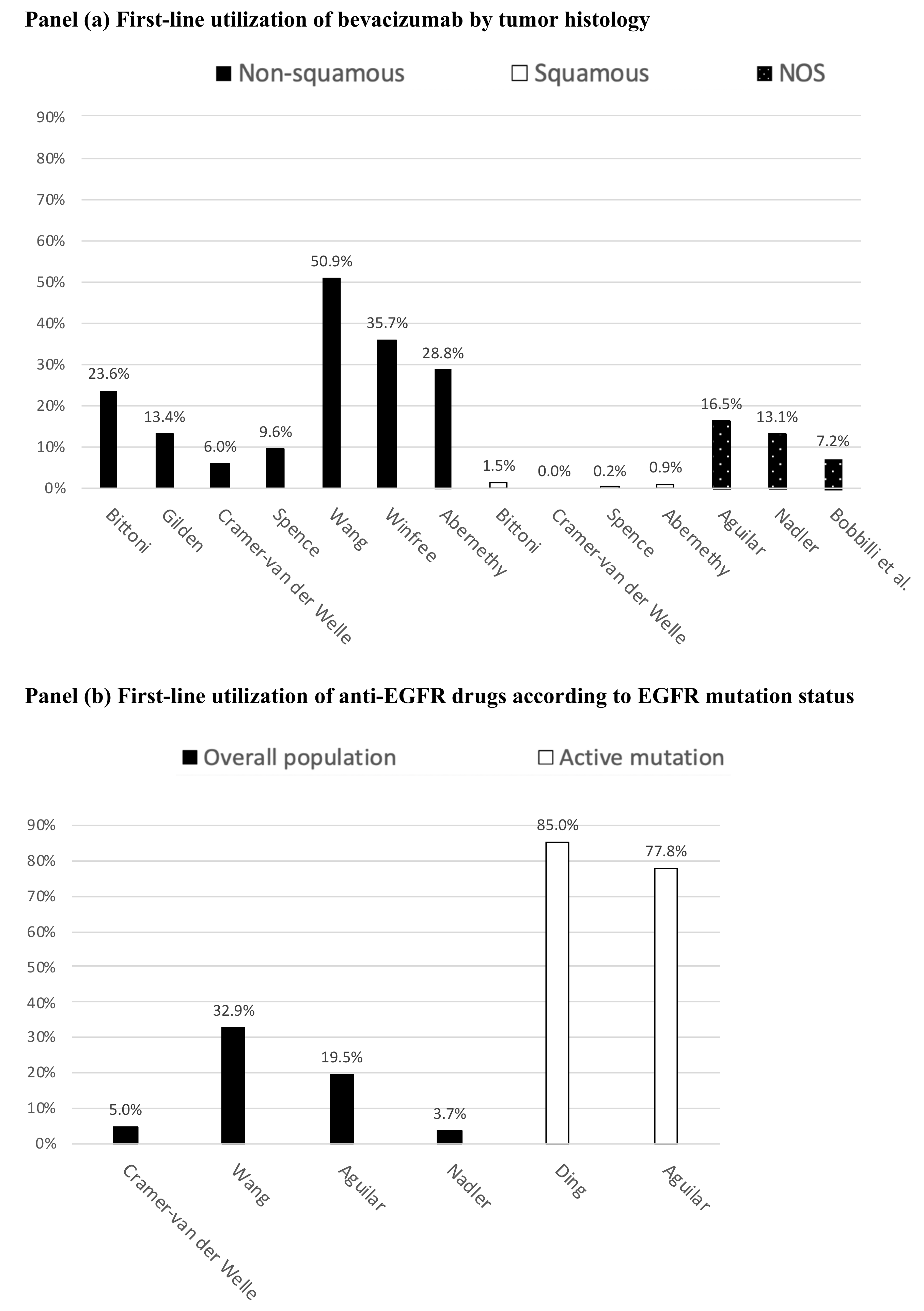
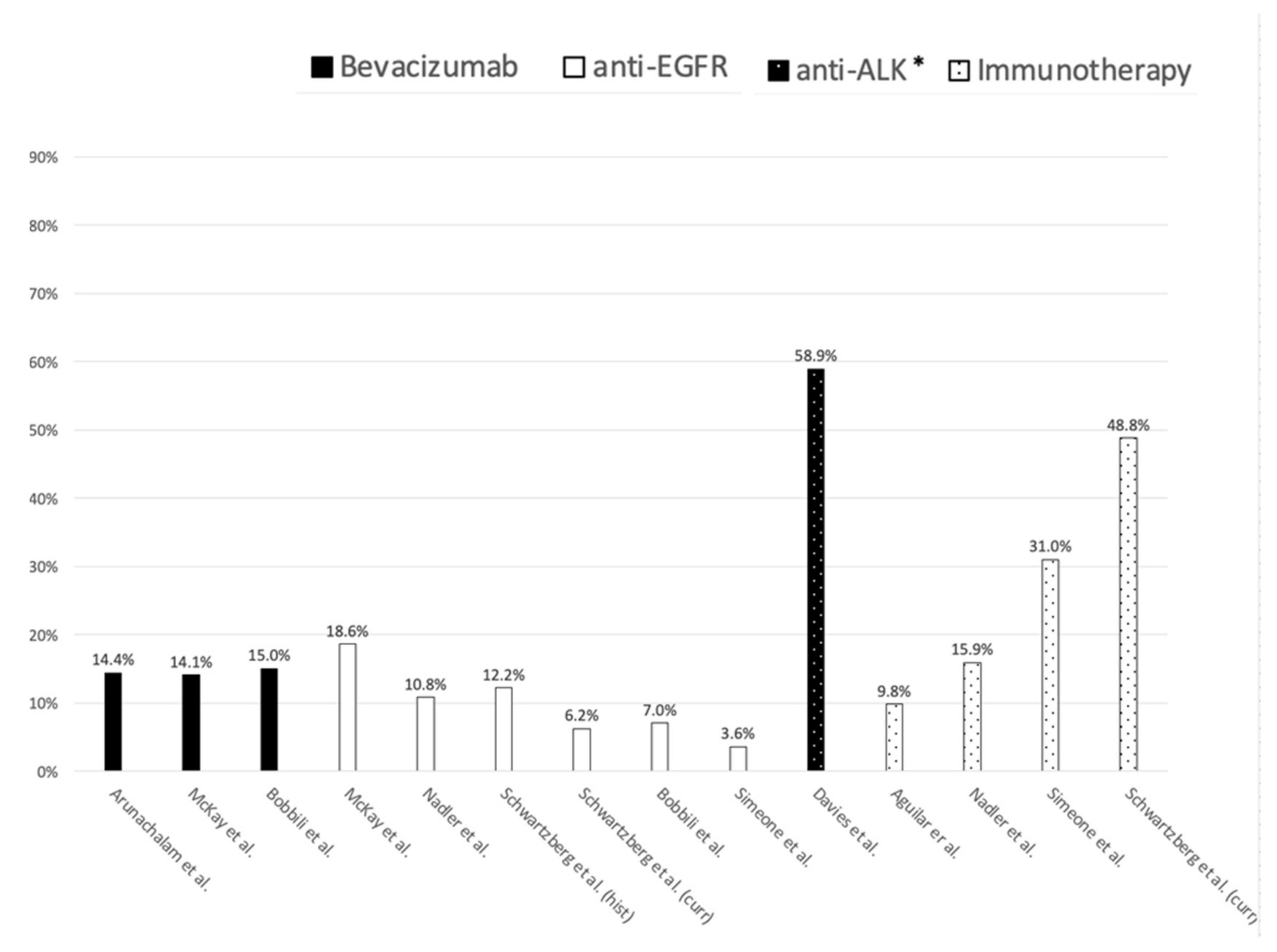
3.5.1. First-Line Treatments for Advanced NSCLC Patients (III–IV Stage)
3.5.2. Second-Line Treatments for Advanced NSCLC (III–IV Stage)
3.6. Utilization of Target- or Immuno-Therapies for Neuroendocrine Lung Cancer
3.7. Utilization of Target- or Immuno-Therapies for Unspecified Lung Cancer Histology
3.8. Survival of Patients Treated with Target- or Immuno- Therapies for Advanced NSCLC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Cancer. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 5 October 2019).
- World Health Organization PRGlobocanFinal Pdf. Available online: https://www.who.int/cancer/PRGlobocanFinal.pdf (accessed on 22 May 2019).
- Travis, W.D.; Brambilla, E.; Burke, A.P.; Marx, A.; Nicholson, A.G. Introduction to the 2015 World Health Organization Classification of Tumors of the Lung, Pleura, Thymus, and Heart. J. Thorac. Oncol. 2015, 10, 1240–1242. [Google Scholar] [CrossRef] [Green Version]
- Aiom Linee Guida Neoplasie Del Polmone—2019. Available online: https://www.aiom.it/linee-guida-aiom-neoplasie-del-polmone-2019/ (accessed on 7 July 2020).
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. NCCN Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer. Version 2.2021. Available online: https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf (accessed on 12 January 2021).
- Ho, C.; Tong, K.; Ramsden, K.; Ionescu, D.; Laskin, J. Histologic Classification of Non-Small-Cell Lung Cancer over Time: Reducing the Rates of Not-Otherwise-Specified. Curr. Oncol. 2015, 22, 164–170. [Google Scholar] [CrossRef] [Green Version]
- Zappa, C.; Mousa, S.A. Non-Small Cell Lung Cancer: Current Treatment and Future Advances. Transl. Lung Cancer Res. 2016, 5, 288–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AIOM Linee Guida Associazione Italiana Di Oncologia Medica—2018: Tumore al Polmone. Available online: https://www.aiom.it/wp-content/uploads/2018/11/2018_LG_AIOM_Polmone.pdf (accessed on 12 January 2021).
- Toschi, L.; Rossi, S.; Finocchiaro, G.; Santoro, A. Non-Small Cell Lung Cancer Treatment (r)Evolution: Ten Years of Advances and more to Come. Ecancermedicalscience 2017, 11, 787. [Google Scholar] [CrossRef] [PubMed]
- Mayekar, M.K.; Bivona, T.G. Current Landscape of Targeted Therapy in Lung Cancer. Clin. Pharmacol. Ther. 2017, 102, 757–764. [Google Scholar] [CrossRef] [PubMed]
- EMA Opdivo. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/opdivo (accessed on 4 October 2019).
- EMA Keytruda. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/keytruda (accessed on 4 October 2019).
- Absenger, G.; Terzic, J.; Bezan, A. ASCO Update: Lung Cancer. Memo Mag. Eur. Med. Oncol. 2017, 10, 224–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horn, L. Advances in the Treatment of Non-Small Cell Lung Cancer. J. Natl. Compr. Cancer Netw. 2014, 12, 764–767. [Google Scholar] [CrossRef] [PubMed]
- Melosky, B. Current Treatment Algorithms for Patients with Metastatic Non-Small Cell, Non-Squamous Lung Cancer. Front. Oncol. 2017, 7, 38. [Google Scholar] [CrossRef] [Green Version]
- Unger, J.M.; Cook, E.; Tai, E.; Bleyer, A. The Role of Clinical Trial Participation in Cancer Research: Barriers, Evidence, and Strategies. Am. Soc. Clin. Oncol. Educ. Book 2016, 36, 185–198. [Google Scholar] [CrossRef]
- Fahey, T. Applying the Results of Clinical Trials to Patients to General Practice: Perceived Problems, Strengths, Assumptions, and Challenges for the Future. Br. J. Gen. Pract. 1998, 48, 1173–1178. [Google Scholar]
- Snyder, C.F.; Wu, A.W.; Miller, R.S.; Jensen, R.E.; Bantug, E.T.; Wolff, A. The Role of Informatics in Promoting Patient-Centered Care. Cancer J. 2011, 17, 211–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houser, S.H.; Colquitt, S.; Clements, K.; Hart-Hester, S. The Impact of Electronic Health Record Usage on Cancer Registry Systems in Alabama. Perspect. Health Inf. Manag. 2012, 9, 9. Available online: http://europepmc.org/article/MED/22737098 (accessed on 19 July 2021).
- Benke, K.; Benke, G. Artificial Intelligence and Big Data in Public Health. Int. J. Environ. Res. Public Health 2018, 15, 2796. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between A Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sørensen, H.T.; von Elm, E.; Langan, S.M. RECORD Working Committee The REporting of Studies Conducted Using Observational Routinely-Collected Health Data (RECORD) Statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef] [PubMed]
- Hiatt, R.A.; Tai, C.G.; Blayney, D.W.; Deapen, D.; Hogarth, M.; Kizer, K.W.; Lipscomb, J.; Malin, J.; Phillips, S.K.; Santa, J.; et al. Leveraging State Cancer Registries to Measure and Improve the Quality of Cancer Care: A Potential Strategy for California and Beyond. J. Natl. Cancer Inst. 2015, 107, djv047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, F.; Mishina, S.; Takai, S.; Le, T.K.; Ochi, K.; Funato, K.; Matsuoka, S.; Ohe, Y. Systemic Treatment Patterns with Advanced or Recurrent Non–Small Cell Lung Cancer in Japan: A Retrospective Hospital Administrative Database Study. Clin. Ther. 2017, 39, 1146–1160. [Google Scholar] [CrossRef] [Green Version]
- Ding, P.N.; Roberts, T.L.; Chua, W.; Becker, T.M.; Descallar, J.; Yip, P.Y.; Bray, V. Clinical Outcomes in Patients with Advanced Epidermal Growth Factor Receptor-Mutated Non-Small-Cell Lung Cancer in South Western Sydney Local Health District. Intern. Med. J. 2017, 47, 1405–1411. [Google Scholar] [CrossRef]
- Peters, B.J.; Welle, C.M.C.-V.; Smit, A.A.; Schramel, F.M.; Van De Garde, E.M. Trends in Prescribing Systemic Treatment and Overall Survival for Non-Small Cell Lung Cancer Stage IIIB/IV in the Netherlands: 2008–2012. Cancer Epidemiol. 2017, 51, 1–6. [Google Scholar] [CrossRef]
- Kasymjanova, G.; Small, D.; Cohen, V.; Jagoe, R.T.; Batist, G.; Sateren, W.; Ernst, P.; Pepe, C.; Sakr, L.; Agulnik, J. Lung Cancer Care Trajectory at A Canadian Centre: An Evaluation of How Wait Times Affect Clinical Outcomes. Curr. Oncol. 2017, 24, 302–309. [Google Scholar] [CrossRef] [Green Version]
- Spence, M.M.; Hui, R.L.; Chang, J.T.; Schottinger, J.E.; Millares, M.; Rashid, N. Treatment Patterns and Overall Survival Associated with First-Line Systemic Therapy for Patients with Advanced Non-Small Cell Lung Cancer. J. Manag. Care Spéc. Pharm. 2017, 23, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Abernethy, A.P.; Arunachalam, A.; Burke, T.; McKay, C.; Cao, X.; Sorg, R.; Carbone, D.P. Real-World First-Line Treatment and Overall Survival in Non-Small Cell Lung Cancer without Known EGFR Mutations or ALK Rearrangements in US Community Oncology Setting. PLoS ONE 2017, 12, e0178420. [Google Scholar] [CrossRef]
- Gilden, D.M.; Kubisiak, J.M.; Pohl, G.M.; Ball, D.E.; Gilden, D.E.; John, W.J.; Wetmore, S.; Winfree, K.B. Treatment Patterns and Cost-Effectiveness of First Line Treatment of Advanced Non-Squamous Non-Small Cell Lung Cancer in Medicare Patients. J. Med. Econ. 2016, 20, 151–161. [Google Scholar] [CrossRef]
- Hopson, S.; Casebeer, A.; Stemkowski, S.; Antol, D.D.; Tao, Z.; Howe, A.; Patton, J.; Small, A.; Masaquel, A. Does Site-Of-Care for Oncology Infusion Therapy Influence Treatment Patterns, Cost, and Quality in the United States? J. Med. Econ. 2017, 21, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.-H.; Shao, Y.-Y.; Liao, B.-C.; Lee, H.-S.; Yang, J.C.-H.; Chen, H.-M.; Chiang, C.-J.; Cheng, A.-L.; Lai, M.-S. Cytotoxic Chemotherapy as First-Line Therapy for Advanced Non-Small-Cell Lung Cancer in Taiwan: Daily Practice. J. Cancer 2016, 7, 1515–1523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lunacsek, O.E.; Ravelo, A.; Coutinho, A.D.; Hazard, S.J.; Green, M.R.; Willey, J.; Eaddy, M.; Goertz, H.-P. First-Line Treatment with Bevacizumab and Platinum Doublet Combination in Non-Squamous Non-Small Cell Lung Cancer: A Retrospective Cohort Study in US Oncology Community Practices. Drugs-Real World Outcomes 2016, 3, 333–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadler, E.; Espirito, J.L.; Pavilack, M.; Boyd, M.; Vergara-Silva, A.; Fernandes, A. Treatment Patterns and Clinical Outcomes Among Metastatic Non-Small-Cell Lung Cancer Patients Treated in the Community Practice Setting. Clin. Lung Cancer 2018, 19, 360–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broder, M.S.; Cai, B.; Chang, E.; Neary, M.P.; Papoyan, E.; Iii, A.B.B. Real-World Treatment Patterns for Lung Neuroendocrine Tumors: A Claims Database Analysis. Oncology 2018, 94, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Dawe, D.E.; Pond, G.R.; Ellis, P.M. Assessment of Referral and Chemotherapy Treatment Patterns for Elderly Patients with Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2016, 17, 563–572. [Google Scholar] [CrossRef] [PubMed]
- McKay, C.; Burke, T.; Cao, X.; Abernethy, A.P.; Carbone, D.P. Treatment Patterns for Advanced Non-Small-Cell Lung Cancer after Platinum-Containing Therapy in U.S. Community Oncology Clinical Practice. Clin. Lung Cancer 2016, 17, 449–460.e7. [Google Scholar] [CrossRef]
- Dalal, A.A.; Guérin, A.; Mutebi, A.; Culver, K.W. Treatment Patterns, Clinical and Economic Outcomes of Patients with Anaplastic Lymphoma Kinase-Positive Non-Small Cell Lung Cancer Receiving Ceritinib: A Retrospective Observational Claims Analysis. J. Drug Assess. 2018, 7, 21–27. [Google Scholar] [CrossRef] [Green Version]
- Shen, C.; Kehl, K.L.; Zhao, B.; Simon, G.R.; Zhou, S.; Giordano, S.H. Utilization Patterns and Trends in Epidermal Growth Factor Receptor (EGFR) Mutation Testing Among Patients with Newly Diagnosed Metastatic Lung Cancer. Clin. Lung Cancer 2017, 18, e233–e241. [Google Scholar] [CrossRef]
- Shinde, R.; Cao, X.; Kothari, S. Biopsy Procedures and Molecular Testing Utilization and Related Costs in Patients with Metastatic Lung Cancer. J. Manag. Care Spéc. Pharm. 2016, 22, 1194–1203. [Google Scholar] [CrossRef]
- Aguilar, K.M.; Winfree, K.B.; Muehlenbein, C.E.; Zhu, Y.E.; Wilson, T.; Wetmore, S.; Nadler, E.S. Treatment Patterns by EGFR Mutation Status in Non-Small Cell Lung Cancer Patients in the USA: A Retrospective Database Analysis. Adv. Ther. 2018, 35, 1905–1919. [Google Scholar] [CrossRef] [PubMed]
- Cramer-van der Welle, C.M.; Peters, B.; Schramel, F.M.; Klungel, O.H.; Groen, H.J.; Van De Garde, E.M. Systematic Evaluation of the Efficacy—Effectiveness Gap of Systemic Treatments in Metastatic Nonsmall Cell Lung Cancer. Eur. Respir. J. 2018, 52, 1801100. [Google Scholar] [CrossRef] [PubMed]
- Winfree, K.B.; Torres, A.Z.; Zhu, Y.E.; Muehlenbein, C.; Aggarwal, H.; Woods, S.; Abernethy, A. Treatment Patterns, Duration and Outcomes of Pemetrexed Maintenance Therapy in Patients with Advanced NSCLC in A Real-World Setting. Curr. Med. Res. Opin. 2018, 35, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Arunachalam, A.; Li, H.; Bittoni, M.A.; Camacho, R.; Cao, X.; Zhong, Y.; Lubiniecki, G.M.; Carbone, D.P. Real-World Treatment Patterns, Overall Survival, and Occurrence and Costs of Adverse Events Associated with Second-Line Therapies for Medicare Patients with Advanced Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2018, 19, e783–e799. [Google Scholar] [CrossRef] [PubMed]
- Bittoni, M.A.; Arunachalam, A.; Li, H.; Camacho, R.; He, J.; Zhong, Y.; Lubiniecki, G.M.; Carbone, D.P. Real-World Treatment Patterns, Overall Survival, and Occurrence and Costs of Adverse Events Associated with First-Line Therapies for Medicare Patients 65 Years and Older with Advanced Non-Small-Cell Lung Cancer: A Retrospective Study. Clin. Lung Cancer 2018, 19, e629–e645. [Google Scholar] [CrossRef]
- Davies, J.; Martinec, M.; Coudert, M.; Delmar, P.; Crane, G. Real-World Anaplastic Lymphoma Kinase (ALK) Rearrangement Testing Patterns, Treatment Sequences, and Survival of ALK Inhibitor-Treated Patients. Curr. Med. Res. Opin. 2018, 35, 535–542. [Google Scholar] [CrossRef]
- Waterhouse, D.M.; Espirito, J.L.; Chioda, M.D.; Baidoo, B.; Mardekian, J.; Robert, N.J.; Masters, E.T. Retrospective Observational Study of ALK-Inhibitor Therapy Sequencing and Outcomes in Patients with ALK-Positive Non-Small Cell Lung Cancer. Drugs-Real World Outcomes 2020, 7, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Jahanzeb, M.; Lin, H.M.; Pan, X.; Yin, Y.; Wu, Y.; Nordstrom, B.; Socinski, M.A. Real-World Treatment Patterns and Progression-Free Survival Associated with Anaplastic Lymphoma Kinase (ALK) Tyrosine Kinase Inhibitor Therapies for ALK + Non-Small Cell Lung Cancer. Oncologist 2020, 25, 867–877. [Google Scholar] [CrossRef]
- Chiang, A.C.; Fernandes, A.W.; Pavilack, M.; Wu, J.W.; Laliberté, F.; Duh, M.S.; Chehab, N.; Subramanian, J. EGFR Mutation Testing and Treatment Decisions in Patients Progressing on First- or Second-Generation Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors. BMC Cancer 2020, 20, 356. [Google Scholar] [CrossRef]
- Bobbili, P.; Ryan, K.; Duh, M.S.; Dua, A.; Fernandes, A.W.; Pavilack, M.; Gomez, J. Treatment Patterns and Overall Survival among Patients with Unresectable, Stage III Non-Small-Cell Lung Cancer. Future Oncol. 2019, 15, 3381–3393. [Google Scholar] [CrossRef] [PubMed]
- Simeone, J.C.; Nordstrom, B.L.; Patel, K.; Klein, A.B. Treatment Patterns and Overall Survival in Metastatic Non-Small-Cell Lung Cancer in A Real-World, US Setting. Future Oncol. 2019, 15, 3491–3502. [Google Scholar] [CrossRef]
- Khozin, S.; Miksad, R.A.; Adami, J.; Boyd, M.; Brown, N.R.; Gossai, A.; Kaganman, I.; Kuk, D.; Rockland, J.M.; Pazdur, R.; et al. Real-World Progression, Treatment, and Survival Outcomes during Rapid Adoption of Immunotherapy for Advanced Non-Small Cell Lung Cancer. Cancer 2019, 125, 4019–4032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartzberg, L.; Korytowsky, B.; Penrod, J.R.; Zhang, Y.; Le, T.K.; Batenchuk, C.; Krug, L. Real-World Clinical Impact of Immune Checkpoint Inhibitors in Patients with Advanced/Metastatic Non-Small Cell Lung Cancer After Platinum Chemotherapy. Clin. Lung Cancer 2019, 20, 287–296.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molife, C.; Hess, L.M.; Cui, Z.L.; Li, X.I.; Beyrer, J.; Mahoui, M.; Oton, A.B. Sequential Therapy with Ramucirumab and/or Checkpoint Inhibitors for Non-Small-Cell Lung Cancer in Routine Practice. Futur. Oncol. 2019, 15, 2915–2931. [Google Scholar] [CrossRef] [Green Version]
- Levra, M.G.; Cotté, F.-E.; Corre, R.; Calvet, C.; Gaudin, A.-F.; Penrod, J.R.; Grumberg, V.; Jouaneton, B.; Jolivel, R.; Assié, J.-B.; et al. Immunotherapy Rechallenge after Nivolumab Treatment in Advanced Non-Small Cell Lung Cancer in the Real-World Setting: A National Data Base Analysis. Lung Cancer 2020, 140, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Roberto, G.; Leal, I.; Sattar, N.; Loomis, A.K.; Avillach, P.; Egger, P.; Van Wijngaarden, R.; Ansell, D.; Reisberg, S.; Tammesoo, M.-L.; et al. Identifying Cases of Type 2 Diabetes in Heterogeneous Data Sources: Strategy from the EMIF Project. PLoS ONE 2016, 11, e0160648. [Google Scholar] [CrossRef] [PubMed]
- Lythgoe, M.; Krell, J.; Warner, J.L.; Desai, A.; Khaki, A.R. Time Intervals between U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMA) New Cancer Therapy Approvals. J. Clin. Oncol. 2021, 39, 1575. [Google Scholar] [CrossRef]
- Major, J.M.; Penberthy, L.; McGlynn, K.A. Data Systems and Record Linkage: Considerations for Pharmacoepidemiologic Studies Examining Cancer Risk. Ann. Epidemiol. 2016, 26, 746–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrigan, G.; Whipple, S.; Taylor, M.D.; Torres, A.Z.; Gossai, A.; Arnieri, B.; Tucker, M.; Hofmeister, P.P.; Lambert, P.; Griffith, S.D.; et al. An Evaluation of the Impact of Missing Deaths on Overall Survival Analyses of Advanced Non-Small Cell Lung Cancer Patients Conducted in An Electronic Health Records Database. Pharmacoepidemiol. Drug Saf. 2019, 28, 572–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturkenboom, M.; Braeye, T.; van der Aa, L.; Danieli, G.; Dodd, C.; Duarte-Salles, T.; Emborg, H.-D.; Gheorghe, M.; Kahlert, J.; Gini, R.; et al. ADVANCE Database Characterisation and Fit for Purpose Assessment for Multi-Country Studies on the Coverage, Benefits and Risks of Pertussis Vaccinations. Vaccine 2020, 38, B8–B21. [Google Scholar] [CrossRef]
- Willame, C.; Dodd, C.; van der Aa, L.; Picelli, G.; Emborg, H.-D.; Kahlert, J.; Gini, R.; Huerta, C.; Martín-Merino, E.; McGee, C.; et al. Incidence Rates of Autoimmune Diseases in European Healthcare Databases: A Contribution of the ADVANCE Project. Drug Saf. 2021, 44, 383–395. [Google Scholar] [CrossRef] [PubMed]
- FDA OPDIVO (Nivolumab) Injection, for Intravenous Use. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/125554s070lbl.pdf (accessed on 13 July 2021).
- Orphanet. The Portal of Rare Diseases and Orphan Drugs. Small Cell Lung Cancer Schedule. Available online: https://www.orpha.net/consor/cgi-bin/Drugs_Search_Simple.php?lng=EN&LnkId=10953&Typ=Pat&fdp=y&from=rightMenu (accessed on 13 July 2021).
- European Medicines Agency. OPDIVO (Nivolumab). Injection, for Intravenous Use. Available online: https://www.ema.europa.eu/en/documents/product-information/opdivo-epar-product-information_en.pdf (accessed on 13 July 2021).
- Bajwa, S.S.; Theerth, K.; Gupta, A. The Increasing Trend of Observational Studies in Clinical Research: Have We Forgotten and Started Defying the Hierarchy? Indian J. Anaesth. 2021, 65, 186–190. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study Reference Study | Data Source Name | Catchment Area | Datasource Type | ||
|---|---|---|---|---|---|
| Administrative/Claims Data | Medical/Health Records | Cancer Registry | |||
| Dawe et al., 2016 [36] | Institute for Clinical Evaluative Sciences databases:Ontario Cancer Registry, OHIP billing claims data, Ontario Drug Benefit, Hospital Discharge Abstracts, National Ambulatory Care Reporting System, Home Care Database, Ontario vital statistics | Canada | ☑ | ☑ | ☑ |
| Spence et al., 2017 [28] | Kaiser Permanente California (KPSC) | USA | ☑ | ☑ | ☑ |
| Cramer-van der Welle et al., 2018 [42] |
| Netherlands | ☑ | ☑ | |
| Peters et al., 2017 [26] |
| Netherlands | ☑ | ☑ | |
| Broder et al., 2018 [35] |
| USA | ☑ | ☑ | |
| Arunachalam et al., 2018 [44] |
| USA | ☑ | ☑ | |
| Bittoni et al., 2018 [45] |
| USA | ☑ | ☑ | |
| Bobbili et al., 2019 [50] |
| USA | ☑ | ☑ | |
| Gilden et al., 2017 [30] |
| USA | ☑ | ☑ | |
| Liang et al., 2016 [32] | Taiwan Cancer Ragistry, National Health Insurance and National Death Registry | Taiwan | ☑ | ☑ | |
| Abernethy et al., 2017 [29] | Flatiron Health database | USA | ☑ | ||
| Aguilar et al., 2018 [41] | US Oncology Network’s iKnowMed database | USA | ☑ | ||
| Chiang et al., 2020 [49] | Flatiron Health database | USA | ☑ | ||
| Davies et al., 2019 [46] | Flatiron Health database | USA | ☑ | ||
| Ding et al., 2017 [25] | Electronic medical records from South Western Sydney Local Health District (SWSLHD) | Australia | ☑ | ||
| Jahanzeb et al., 2020 [48] | Flatiron Health database | USA | ☑ | ||
| Khozin et al., 2019 [52] | Flatiron Health database | USA | ☑ | ||
| Lunacsek et al., 2016 [33] |
| USA | ☑ | ||
| McKay et al., 2016 [37] | Flatiron Health database | USA | ☑ | ||
| Molife et al., 2019 [54] | Flatiron Health database | USA | ☑ | ||
| Nadler et al., 2018 [34] | US oncology iKnowMedTM (iKM) databaseSocial Security Death Index | USA | ☑ | ||
| Schwartzberg et al., 2019 [53] | Flatiron Health database | USA | ☑ | ||
| Simeone et al., 2019 [51] | Flatiron Health database | USA | ☑ | ||
| Waterhouse et al., 2020 [47] | US Oncology Network’s iKnowMed database | USA | ☑ | ||
| Winfree et al., 2018 [43] | Flatiron Health database | USA | ☑ | ||
| Kasymjanova et al., 2017 [27] | Jewish General Hospital’s Pulmonary Division Lung Cancer Registry | Canada | ☑ | ||
| Dalal et al., 2018 [38] |
| USA | ☑ | ||
| Hopson et al., 2018 [31] | Humana Research Database | USA | ☑ | ||
| Levra et al., 2020 [55] | Programme de Médicalisation des Systèmes d’Information (PMSI) | France | ☑ | ||
| Shen et al., 2017 [39] | Truven Health MarketScan database | USA | ☑ | ||
| Shinde et al., 2016 [40] | Truven Health MarketScan database | USA | ☑ | ||
| Wang et al., 2017 [24] | Medical Data Vision Database | Japan | ☑ | ||
| Study Reference |
| Observation Period | Follow-Up Duration | Drugs or Drug Regimens under Study | ||
|---|---|---|---|---|---|---|
| Target Therapy | Immunotherapy | Other | ||||
| Dawe et al. [36] |
| January 2000–December 2010 | - |
| - | Standard chemotherapy, Complex single or multi agents, Special single agents or multi agents |
| Spence et al. [28] |
| January 2008–September 2014 | - |
| - | Carboplatin, Cisplatin, Docetaxel, Etoposide, Gemcitabine, Paclitaxel, Pemetrexed, Vinorelbine |
| Cramer-van der Welle et al., [42] |
| January 2008–December 2014 | - |
| - | Carboplatin, Cisplatin, Docetaxel, Gemcitabine, Paclitaxel |
| Peters et al. [26] |
| January 2008–December 2012 | - |
| - | Carboplatin, Cisplatin, Gemcitabine, Pemetrexed |
| Broder et al. [35] |
| July 2009–June 2014 | 14.3 months (Median: 11 months) |
| - | Cytotoxic chemotherapy, Somatostatin analogues (+/−interferon) |
| Arunachalam et al. [44] |
| January 2007–December 2011 | 20 months; (Median 15.7 months) |
| - | Carboplatin, Cisplatin, Docetaxel, Gemcitabine, Pemetrexed, Vinorelbine |
| Bittoni et al. [45] |
| January 2007–December 2011 | 13.6 months; (Median 8.9 months) |
| - | Carboplatin, Cisplatin, Docetaxel, Gemcitabine, Pemetrexed, Vinorelbine |
| Gilden et al. [30] |
| January 2008–December 2010 | - |
| - | Carboplatin, Cisplatin, Paclitaxel, Pemetrexed |
| Liang et al. [32] |
| January 2005–December 2009 | Median 14 months |
| - | Carboplatin, Cisplatin, Docetaxel, Etoposide, Epirubicin, Gemcitabine, Paclitaxel Pemetrexed, Tegafur, Vinorelbine |
| Abernethy et al. [29] |
| November 2012–January 2015 | - |
| PD-1 inhibitors | Carboplatin, Cisplatin, Docetaxel, Etoposide, Gemcitabine, Paclitaxel, Pemetrexed, Vinorelbine |
| Aguilar et al. [41] |
| January 2011–June 2015 |
10.3 months (Median 7.6 months) |
| Nivolumab | Carboplatin, Docetaxel, Pemetrexed |
| Davies et al. [46] |
| January 2011–December 2014 | Median 16.6 months |
| - | Carboplatin, Cisplatin, Docetaxel, Gemcitabine, Pemetrexed, Vinorelbine |
| Ding et al. [25] |
| January 2010–June 2016 | Median 10.7 months |
| - | - |
| Lunacsek et al. [33] |
| April 2006–July 2013 | - |
| - | Carboplatin, Cisplatin, Docetaxel, Gemcitabine, Metotrexate, Paclitaxel, Pemetrexed, Temozolomide, Vinflunine, Vinorelbine |
| McKay et al. [37] |
| January 2011–April 2015 | - |
| - | Carboplatin, Cisplatin, Docetaxel, Gemcitabine, Paclitaxel, Pemetrexed Vinorelbine |
| Nadler et al. [34] |
| January 2012–April 2016 | Median 6.9 months |
| Nivolumab | Carboplatin, Docetaxel, Gemcitabine, Paclitaxel, Pemetrexed |
| Winfree et al. [43] |
| January 2011–October 2015 | Median 13.8 months |
| Nivolumab | Carboplatin, Cisplatin, Gemcitabine, Pemetrexed |
| Kasymjanova et al. [27] |
| January 2010–December 2014 | - |
| - | Chemotherapy: Combined agents, Double agents, Single agent |
| Dalal et al. [38] |
| January 2006–December 2015 | - |
| - | Standard chemotherapy |
| Hopson et al. [31] |
| January 2007–December 2013 | - |
| - | Carboplatin, Cisplatin, Docetaxel, Oxaliplatin, Paclitaxel |
| Shen et al. [39] |
| January 2013–June 2014 | - |
| - | Pemetrexed |
| Shinde et al. [40] |
| January 2009–September 2012 | - |
| - | - |
| Wang et al. [24] |
| April 2008–September 2015 | 10.3 months |
| - | Carboplatin, Cisplatin, Docetaxel, Gemcitabine, Paclitaxel, Tegafur |
| Waterhouse et al. [47] |
| September 2011–December 2017 | - |
| - | - |
| Jahanzeb et al. [48] |
| January 2011–June 2018 | - |
| - | - |
| Chiang et al. [49] |
| January 2011–September 2017 | Median: 10.3 months |
| Immunotherapy not specified | Chemotherapy not specified |
| Bobbili et al. [50] |
| January 2009–December 2014 | - |
| - | Carboplatin, Cisplatin, Docetaxel, Etoposide, Gemcitabine, Paclitaxel, Pemetrexed |
| Simeone et al. [51] |
| January 2013–January 2017 | Median: 8.4 months |
| Nivolumab | Carboplatin, Cisplatin, Docetaxel, Etoposide, Gemcitabine, Paclitaxel, Pemetrexed, Vinorelbine |
| Khozin et al. [52] |
| January 2011–December 2017 | - |
|
Atezolizumab Nivolumab Pembrolizumab | Platinum based chemotherapy, Non platinum based chemotherapy, Single agent Chemotherapy |
| Schwartzberg et al. [53] |
| Historical: January 2011–December 2013 Current: January 2015–May 2017 | Median: 5.8 months |
|
Atezolizumab Nivolumab Pembrolizumab | Carboplatin, Docetaxel, Gemcitabine, Paclitaxel, Pemetrexed, Vinorelbine |
| Molife et al. [54] |
| December 2014–May 2017 | - |
|
Atezolizumab Ipilimumab Nivolumab Pembrolizumab | Carboplatin, Cisplatin, Docetaxel, Gemcitabine, Etoposide, Paclitaxel, Pemetrexed, Vinorelbine |
| Levra et al. [55] |
| January 2015–December 2016 | - | - |
Nivolumab Pembrolizumab | Chemotherapy not specified |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spini, A.; Hyeraci, G.; Bartolini, C.; Donnini, S.; Rosellini, P.; Gini, R.; Ziche, M.; Salvo, F.; Roberto, G. Real-World Utilization of Target- and Immunotherapies for Lung Cancer: A Scoping Review of Studies Based on Routinely Collected Electronic Healthcare Data. Int. J. Environ. Res. Public Health 2021, 18, 7679. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147679
Spini A, Hyeraci G, Bartolini C, Donnini S, Rosellini P, Gini R, Ziche M, Salvo F, Roberto G. Real-World Utilization of Target- and Immunotherapies for Lung Cancer: A Scoping Review of Studies Based on Routinely Collected Electronic Healthcare Data. International Journal of Environmental Research and Public Health. 2021; 18(14):7679. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147679
Chicago/Turabian StyleSpini, Andrea, Giulia Hyeraci, Claudia Bartolini, Sandra Donnini, Pietro Rosellini, Rosa Gini, Marina Ziche, Francesco Salvo, and Giuseppe Roberto. 2021. "Real-World Utilization of Target- and Immunotherapies for Lung Cancer: A Scoping Review of Studies Based on Routinely Collected Electronic Healthcare Data" International Journal of Environmental Research and Public Health 18, no. 14: 7679. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147679