
Colorectal Cancer in Young and Older Adults in Uruguay: Changes in Recent Incidence and Mortality Trends

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Data Analysis
3. Results
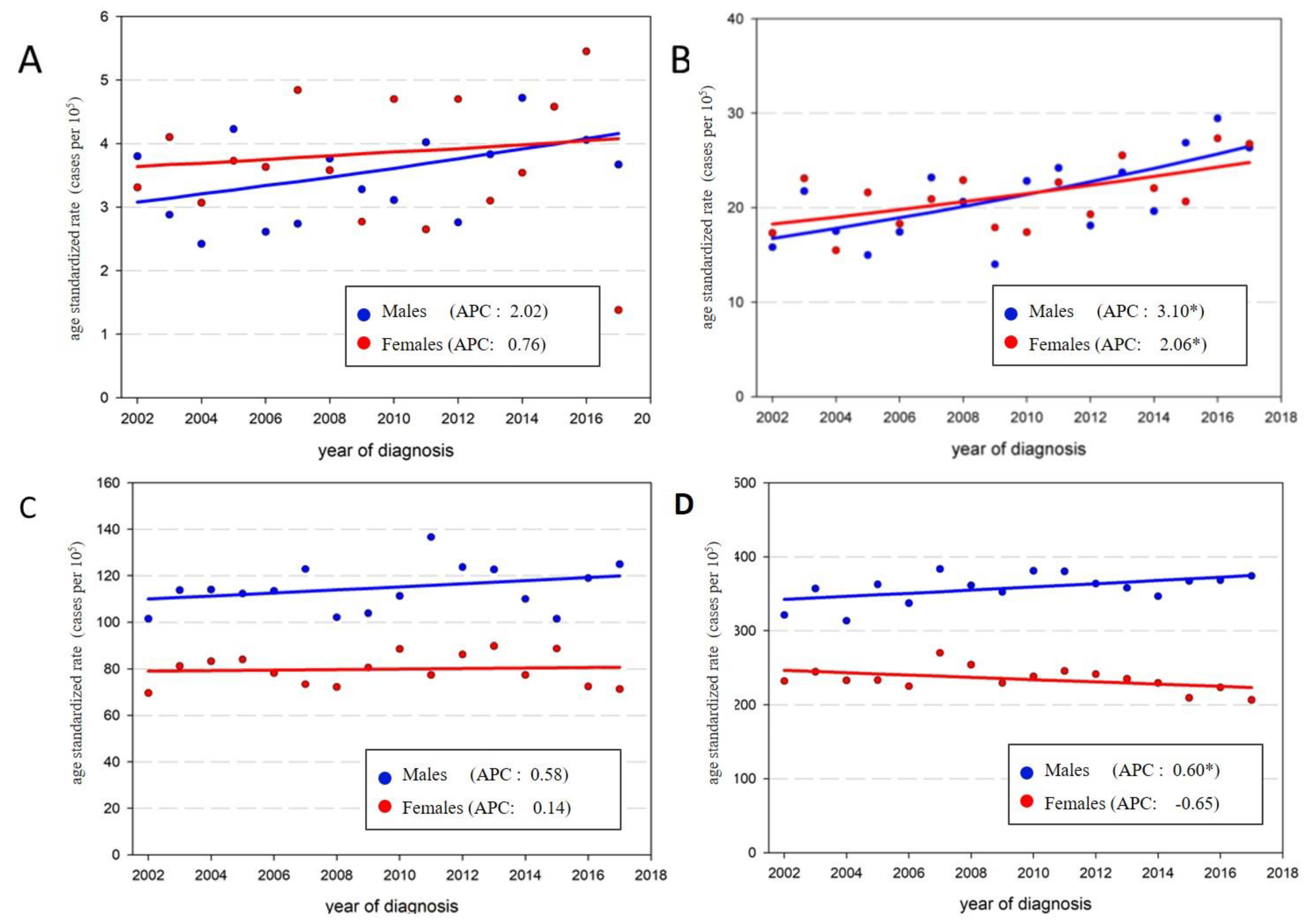
3.1. Incidence Time Trends 2002–2017
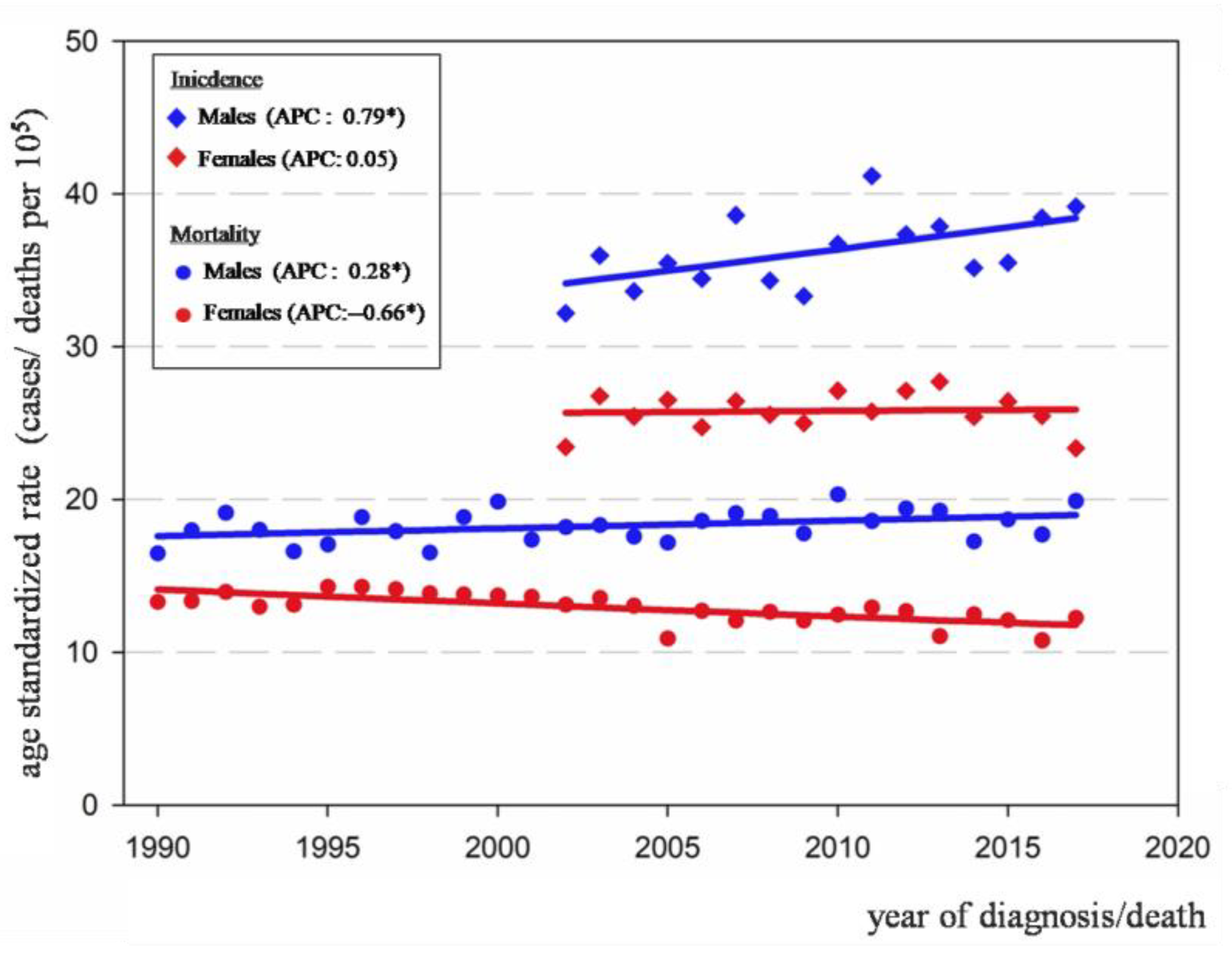
3.2. Mortality Time Trends 1990–2017
4. Discussion
4.1. Increasing Incidence among Young Adults
4.2. Divergent Trends by Sex in Older Adults
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020; Available online: https://gco.iarc.fr/today (accessed on 24 March 2021).
- Institute for Health Metrics and Evaluation. Global Burden of Disease (GBD) 2017 Data. 2018. Available online: http://www.healthdata.org/gbd (accessed on 9 July 2021).
- Colorectal Cancer. Decreasing disparities and promoting prevention are policy priorities. In World Cancer Report: Cancer Research for Cancer Prevention. Christopher Wild, Elisabete Weiderpass, Bernard Stewart; IARC Press: Lyon, France, 2020; pp. 344–354. [Google Scholar]
- Diet, Nutrition, Physical Activity and Colorectal Cancer. Continuous Update Project Expert Report 2018. World Cancer Research Fund/ American Institute for Cancer Research. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/Colorectal-cancer-report.pdf (accessed on 16 June 2021).
- Kim, S.E.; Paik, Y.; Yoon, H.; Eun Lee, J.; Kim, N.; Sung, M.K.I. Sex, gender and colorectal cancer risk. World J. Gastroenterol. 2015, 21, 5167–5175. [Google Scholar] [CrossRef] [PubMed]
- White, A.; Ironmonger, L.; Steele, R.; Ormiston-Smith, N.; Crawford, C.; Seims, A. A review of sex-related differences in colorectal cancer incidence, screening uptrake, routes to diagnosis, cancer stage and survival in the UK. BMC Cancer 2018, 18, 906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Instituto Nacional de Estadística. Censos 2011 [Internet]. 2012. Available online: http://www.ine.gub.uy/web/guest/censos-2011 (accessed on 3 October 2020).
- UNDP, New York. UNDP. Human Development Report 2019. Beyond Income, Beyond Averages, Beyond Today: Inequalities in Human Development in the 21st Century. [Internet]. 2019. Available online: http://hdr.undp.org/en/content/human-development-report-2019 (accessed on 10 March 2021).
- Sierra, M.S.; Forman, D. Burden of colorectal cancer in Central and South America. Cancer Epidemiol. 2016, 44, S74–S81. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Registry—Uruguay. Colo Rectal Cancer Uruguay 2012–2016 Fact Sheet [Internet]. Available online: https://www.comisioncancer.org.uy/Ocultas/COLORECTAL-CANCER-uc261 (accessed on 10 April 2021).
- Garau, M.; Musetti, C.; Alonso, R.; Barrios, E. Trends in cancer incidence in Uruguay: 2002–2015. Colomb. Med. Cali. Colomb. 2019, 50, 224–238. [Google Scholar] [CrossRef]
- Siegel, R.L.; Torre, L.A.; Soerjomataram, I.; Hayes, R.B.; Bray, F.; Weber, T.K.; Jemal, A. Global patterns and trends in colorectal cancer incidence in young adults. Gut 2019, 68, 2179–2185. [Google Scholar] [CrossRef] [Green Version]
- Loomans-Kropp, H.A.; Umar, A. Increasing Incidence of Colorectal Cancer in Young Adults. J. Cancer Epidemiol. 2019, 2019, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Vuik, F.E.; Nieuwenburg, S.A.; Bardou, M.; Lansdorp-Vogelaar, I.; Dinis-Ribeiro, M.; Bento, M.J.; Zadnik, V.; Pellisé, M.; Esteban, L.; Kaminski, M.F.; et al. Increasing incidence of colorectal cancer in young adults in Europe over the last 25 years. Gut 2019, 68, 1820–1826. [Google Scholar] [CrossRef]
- Feletto, E.; Yu, X.Q.; Lew, J.-B.; St John, D.J.B.; Jenkins, M.A.; Macrae, F.A.; Mahady, S.E.; Canfell, K. Trends in Colon and Rectal Cancer Incidence in Australia from 1982 to 2014: Analysis of Data on Over 375,000 Cases. Cancer Epidemiol. Biomark. Prev. 2019, 28, 83–90. [Google Scholar] [CrossRef] [Green Version]
- Brenner, D.R.; Ruan, Y.; Shaw, E.; De, P.; Heitman, S.J.; Hilsden, R.J. Increasing colorectal cancer incidence trends among younger adults in Canada. Prev. Med. 2017, 105, 345–349. [Google Scholar] [CrossRef]
- Siegel, R.L.; Jakubowski, C.D.; Fedewa, S.A.; Davis, A.; Azad, N.S. Colorectal Cancer in the Young: Epidemiology, Prevention, Management. Am. Soc. Clin. Oncol. Educ. Book 2020, 40, e75–e88. [Google Scholar] [CrossRef]
- Araghi, M.; Soerjomataram, I.; Bardot, A.; Ferlay, J.; Cabasag, C.J.; Morrison, D.S.; De, P.; Tervonen, H.; Walsh, P.M.; Bucher, O.; et al. Changes in colorectal cancer incidence in seven high-income countries: A population-based study. Lancet Gastroenterol. Hepatol. 2019, 4, 511–518. [Google Scholar] [CrossRef]
- Zauber, A.G. The impact of screening on colorectal cancer mortality and incidence: Has it really made a difference? Dig. Dis.Sci. 2015, 60, 681–691. [Google Scholar] [CrossRef] [Green Version]
- MSP Guia Para el Tamizaje del Cáncer Colo-Rectal [Internet]. Available online: https://www.paho.org/uru/index.php?option=com_docman&view=download&slug=guia-de-practica-clinica-de-tamizaje-del-cancer-colo-rectal-2018&Itemid=307 (accessed on 2 January 2021).
- Fenocchi, E.; Martínez, L.; Tolve, J.; Montano, D.; Rondán, M.; Parra-Blanco, A.; Eishi, Y. Screening for colorectal cancer in Uruguay with an immunochemical faecal occult blood test. Eur. J. Cancer Prev. 2006, 15, 384–390. [Google Scholar] [CrossRef]
- Schreuders, E.H.; Ruco, A.; Rabeneck, L.; Schoen, R.E.; Sung, J.J.Y.; Young, G.P.; Kuipers, E.J. Colorectal cancer screening: A global overview of existing programmes. Gut 2015, 64, 1637–1649. [Google Scholar] [CrossRef]
- Forman, D.; Bray, F.; Brewster, D.H.; Gombe Mbalawa, C.; Kohler, B.; Piñeros, M.; Steliarova Foucher, E.; Swaminathan, R.; Ferlay, J. (Eds.) Cancer Incidence in Five Continents, Vol. X; International Agency for Research on Cancer: Lyon, France; IARC Scientific Publication N°164: Lyon, France, 2014. [Google Scholar]
- Bray, F.; Ferlay, J.; Laversanne, M.; Brewster, D.H.; Gombe Mbalawa, C.; Kohler, B.; Piñeros, M.; Steliarova-Foucher, E.; Swaminathan, R.; Antoni, S.; et al. Cancer Incidence in Five Continents: Inclusion criteria, highlights from Volume X and the global status of cancer registration. Int. J. Cancer 2015, 137, 2060–2071. [Google Scholar] [CrossRef]
- Bray, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Zanetti, R.; Ferlay, J. Cancer Incidence in Five Continents, Vol. XI; International Agency for Research on Cancer: Lyon, France; IARC Scientific Publication N°166: Lyon, France, 2017. [Google Scholar]
- Fritz, A.G. International Classification of Diseases for Oncology: ICD-O, 3rd ed.; First Revision; World Health Organization: Geneva, Switzerland, 2013; p. 242. [Google Scholar]
- Segi, M. Cancer Mortality for Selected Sites in 24 Countries (1950–1957); Tohoku University of Medicine, Department of Public Health: Sendai, Japan, 1960. [Google Scholar]
- Instituto Nacional de Estadística. Censos 1963–1996—[Internet]. 1997. Available online: http://www.ine.gub.uy/web/guest/censos-1963-1996 (accessed on 3 October 2020).
- Instituto Nacional de Estadística. Censo 2004 Fase I [Internet]. 2005. Available online: http://www.ine.gub.uy/web/guest/censo-2004-fase-i (accessed on 3 October 2020).
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Statistical Research and Applications Branch, National Cancer Institute. Joinpoint Regression Program, Ver 4.1.0; Bethesda: Rockville, MD, USA, 2014.
- Barrios, E.; Garau, M.; Alonso, R.; Musetti, C. VAtlas de Incidencia de Cáncer en el Uruguay 2012–2016; Comisión Honoraria de Lucha Contra el Cáncer: Montevideo, Uruguay, 2020; 117p, Available online: https://www.comisioncancer.org.uy/Ocultas/V-Atlas-de-Incidencia-del-Cancer-en-el-Uruguay-Periodo-2012-2016-uc250 (accessed on 3 March 2021).
- The GBD 2015 Obesity Collaborators. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Friedenreich, C.; Leitzmann, M. Physical activity, sedentary behaviour and obesity. Established and emerging modifiable risk factors. In World Cancer Report: Cancer Research for Cancer Prevention.Christopher Wild, Elisabete Weiderpass, BernardStewart; IARC Press: Lyon, France, 2020; pp. 101–108. [Google Scholar]
- PPNET; MSP. Second National Survey un Risk Factors for Non Comunicable Diseases—STEPS Methodology [Internet]. STEPS Collection. 2013. Available online: https://extranet.who.int/ncdsmicrodata/index.php/catalog/628 (accessed on 3 March 2021).
- Monteiro, C.A.; Moubarac, J.-C.; Cannon, G.; Ng, S.W.; Popkin, B. Ultra-processed products are becoming dominant in the global food system. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2013, 14 (Suppl. S2), 21–28. [Google Scholar] [CrossRef]
- Tabung, F.K.; Liu, L.; Wang, W.; Fung, T.T.; Wu, K.; Smith-Warner, S.A.; Cao, Y.; Hu, F.B.; Ogino, S.; Fuchs, C.S.; et al. Association of Dietary Inflammatory PotentialWith Colorectal Cancer Risk in Men and Women. JAMA Oncol. 2018, 4, 366. [Google Scholar] [CrossRef] [Green Version]
- Lynch, H.T.; Lynch, J.F.; Lynch, P.M.; Attard, T. Hereditary colorectal cancer syndromes: Moleculargenetics, genetic counseling, diagnosis and management. Fam. Cancer 2008, 7, 27–39. [Google Scholar] [CrossRef]
- Stoffel, E.M.; Koeppe, E.; Everett, J.; Ulintz, P.; Kiel, M.; Osborne, J.; Williams, L.; Hanson, K.; Gruber, S.B.; Rozek, L.S. Germline Genetic Features of Young Individuals WithColorectal Cancer. Gastroenterology 2018, 154, 897–905.e1. [Google Scholar] [CrossRef]
- Sarroca, C.; Della Valle, A.; Fresco, R.; Renkonen, E.; Peltömaki, P.; Lynch, H. Frequency of hereditary non-polyposis colorectal cancer among Uruguayan patients with colorectal cancer: Frequency of HNPCC in Uruguay. Clin. Genet. 2005, 68, 80–87. [Google Scholar] [CrossRef]
- Neffa, F.; Della Valle, A.; Sarroca, C. Incidence and Clinical Characteristics of Colonic and Extra Colonic Lynch Syndrome Manifestations in Uruguayan Mismatch Repair Carriers. 2017. Available online: http://colorectal-cancer.imedpub.com/incidence-and-clinical-characteristics-of-colonic-and-extra-colonic-lynch-syndrome-manifestations-in-uruguayan-mismatch-repair-car.php?aid=19394 (accessed on 16 March 2021).
- Schellerer, V.S.; Merkel, S.; Schumann, S.C.; Schlabrakowski, A.; Förtsch, T.; Schildberg, C.; Hohenberger, W.; Croner, R.S. Despite aggressive histopathology survival is not impaired in young patients with colorectal cancer: CRC in patients under 50 years of age. Int. J. Colorectal. Dis. 2012, 27, 71–79. [Google Scholar] [CrossRef]
- Joseph, K.; Mergen, D. Uruguay Livestock and Products Annual 2015. [Internet]. Global Agricultural Information Network. 2015. Available online: https://www.fas.usda.gov/data/uruguay-livestock-and-products-annual-0 (accessed on 12 March 2021).
- Christy, S.M.; Mosher, C.E.; Rawl, S.M. Integrating men’s health and Masculinity Theories to explain Colorectal Cancer Screening Behavior. Am. J. Men’s Health 2014, 8, 54–65. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Age Group | Male | Female | Both | |||
|---|---|---|---|---|---|---|
| Cases | % | Cases | % | Cases | % | |
| All Ages | 13,791 | 100 | 13,770 | 100 | 27,561 | 100 |
| 20–39 | 270 | 1.96 | 297 | 2.15 | 567 | 2.06 |
| 40–49 | 650 | 4.71 | 700 | 5.08 | 1350 | 4.90 |
| 50–69 | 5480 | 39.73 | 4433 | 32.19 | 9913 | 35.97 |
| 70+ | 7376 | 53.48 | 8326 | 60.46 | 15702 | 56.97 |
| Age Group | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|
| ASR 2002 | ASR 2017 | APC | CI 95% | ASR 2002 | ASR 2017 | APC | CI 95% | |
| All Ages | 32.19 | 39.15 | 0.79 * | (0.12; 1.47) | 23.43 | 23.35 | 0.05 | (−0.53; 0.64) |
| 20–39 | 3.80 | 3.67 | 2.02 | (−0.10; 4.19) | 3.31 | 1.38 | 0.76 | (−2.52; 4.15) |
| 40–49 | 15.81 | 26.34 | 3.10 * | (1.21; 5.03) | 17.31 | 26.74 | 2.06 * | (0.49; 3.66) |
| 50–69 | 101.5 | 124.97 | 0.58 | (−0.42; 1.59) | 69.63 | 71.34 | 0.14 | (−0.88; 1.18) |
| 70+ | 321.16 | 374.06 | 0.60 * | (0.02; 1.20) | 232.19 | 206.72 | −0.65 | (−1.37; 0.07) |
| Age Group | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|
| ASR 2002 | ASR 2017 | APC | CI 95% | ASR 2002 | ASR 2017 | APC | CI 95% | |
| All Ages | 16.48 | 19.89 | 0.28 * | (0.02; 0.53) | 13.29 | 12.25 | −0.66 * | (−0.92; −0.4) |
| 20–39 | 1.14 | 1.44 | 1.23 | (−0.55; 3.04) | 0.84 | 1.03 | −0.61 | (−2.75; 1.57) |
| 40–49 | 8.36 | 7.74 | −0.43 | (−1.38; 0.53) | 8.01 | 8.07 | −0.59 | (−1.59; 0.42) |
| 50–69 | 48.01 | 52.56 | −0.25 | (−0.72; 0.22) | 36.60 | 34.88 | −0.61 * | (−1.07; −0.14) |
| 70+ | 187.03 | 253.61 | 0.74 * | (0.47; 1.01) | 156.00 | 135.24 | −0.68 * | (−1.02; −0.34) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Musetti, C.; Garau, M.; Alonso, R.; Piñeros, M.; Soerjomataram, I.; Barrios, E. Colorectal Cancer in Young and Older Adults in Uruguay: Changes in Recent Incidence and Mortality Trends. Int. J. Environ. Res. Public Health 2021, 18, 8232. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158232
Musetti C, Garau M, Alonso R, Piñeros M, Soerjomataram I, Barrios E. Colorectal Cancer in Young and Older Adults in Uruguay: Changes in Recent Incidence and Mortality Trends. International Journal of Environmental Research and Public Health. 2021; 18(15):8232. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158232
Chicago/Turabian StyleMusetti, Carina, Mariela Garau, Rafael Alonso, Marion Piñeros, Isabelle Soerjomataram, and Enrique Barrios. 2021. "Colorectal Cancer in Young and Older Adults in Uruguay: Changes in Recent Incidence and Mortality Trends" International Journal of Environmental Research and Public Health 18, no. 15: 8232. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158232