
Dental Fear and Associated Factors among Children and Adolescents: A School-Based Study in Lithuania

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample and Data Collection
2.3. Questionnaires
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
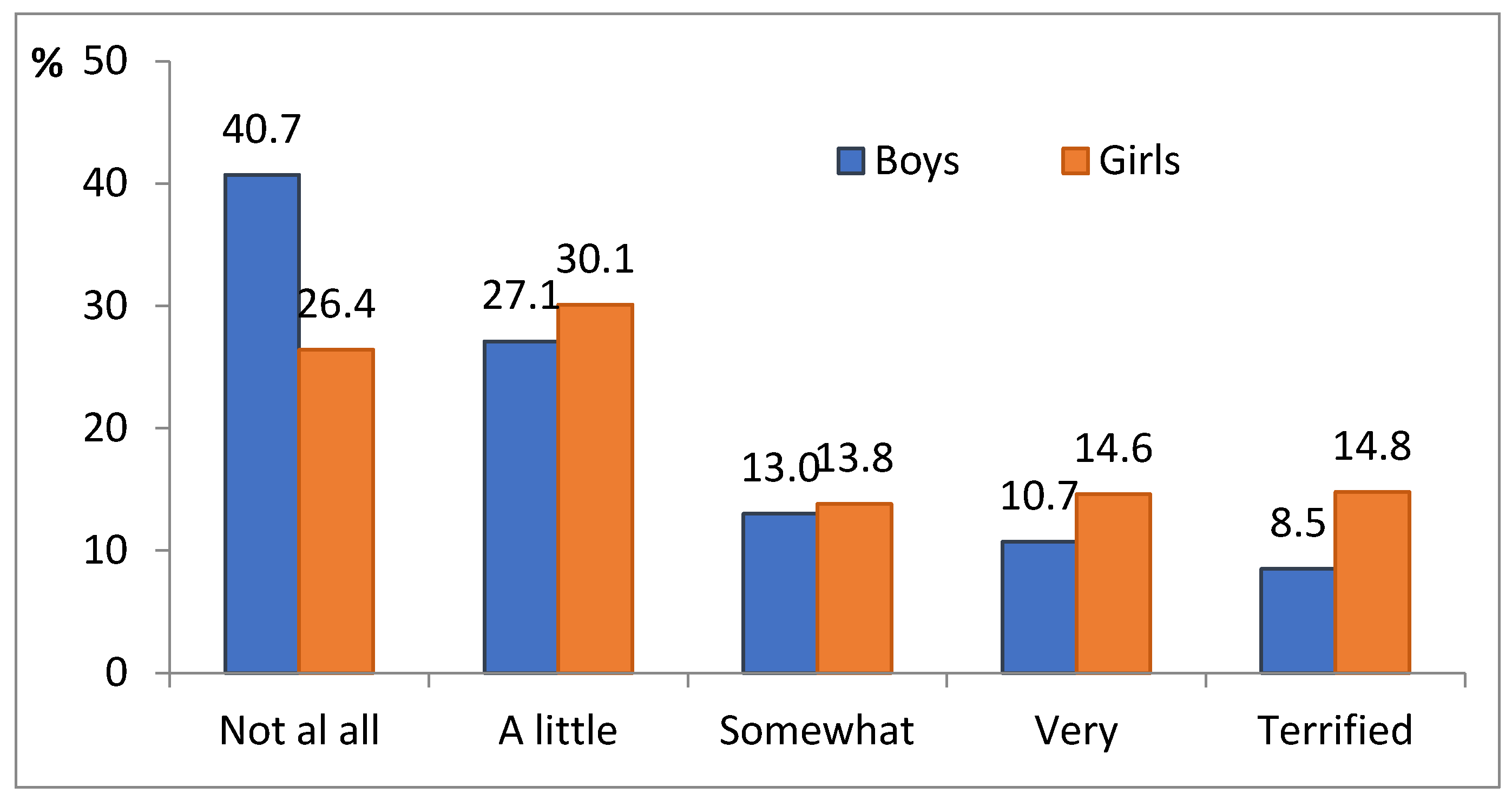
3.2. Level and Prevalence of Dental Fear
3.3. Dental Fear and Its Association with Other Factors
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Klingberg, G.; Broberg, A.G. Dental fear/anxiety and dental behaviour management problems in children and adolescents: A review of prevalence and concomitant psychological factors. Int. J. Paediatr. Dent. 2007, 17, 391–406. [Google Scholar] [CrossRef]
- Locker, D.; Thomson, W.M.; Poulton, R. Onset of and patterns of change in dental anxiety in adolescence and early adulthood: A birth cohort study. Community Dent. Health 2001, 18, 99–104. [Google Scholar] [PubMed]
- Porritt, J.; Marshman, Z.; Rodd, H.D. Understanding children’s dental anxiety and psychological approaches to its reduction. Int. J. Paediatr. Dent. 2012, 22, 397–405. [Google Scholar] [CrossRef]
- Cianetti, S.; Lombardo, G.; Lupatelli, E.; Pagano, S.; Abraha, I.; Montedori, A.; Caruso, S.; Gatto, R.; De Giorgio, S.; Salvato, R. Dental fear/anxiety among children and adolescents. A systematic review. Eur. J. Paediatr. Dent. 2017, 18, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Grisolia, B.M.; Dos Santos, A.P.P.; Dhyppolito, I.M.; Buchanan, H.; Hill, K.; Oliveira, B.H. Prevalence of dental anxiety in children and adolescents globally: A systematic review with meta-analyses. Int. J. Paediatr. Dent. 2021, 31, 168–183. [Google Scholar] [CrossRef]
- Shim, Y.S.; Kim, A.H.; Jeon, E.Y.; An, S.Y. Dental fear & anxiety and dental pain in children and adolescents; a systemic review. J. Dent. Anesth. Pain Med. 2015, 15, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Merdad, L.; El-Housseiny, A.A. Do children’s previous dental experience and fear affect their perceived oral health related quality of life (OHRQoL)? BMC Oral Health 2017, 17, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luoto, A.; Lahti, S.; Nevanperä, T.; Tolvanen, M.; Locker, D. Oral-health-related quality of life among children with and without dental fear. Int. J. Paediatr. Dent. 2009, 19, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Armfield, J.M.; Heaton, L.J. Management of fear and anxiety in the dental clinic: A review. Aust. Dent. J. 2013, 58, 390–407. [Google Scholar] [CrossRef]
- Gao, X.; Hamzah, S.H.; Yiu, C.K.; McGrath, C.; King, N.M. Dental fear and anxiety in children and adolescents: Qualitative study using YouTube. J. Med. Internet Res. 2013, 15, e29. [Google Scholar] [CrossRef]
- Armfield, J.M. How do we measure dental fear and what are we measuring anyway? Oral Health Prev. Dent. 2010, 8, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Viswanath, D.; Kumar, M.R.; Prabhuji, M.L.V. Dental anxiety, fear and phobia in children. Int. J. Dent. Res. Dev. 2014, 4, 1–14. [Google Scholar]
- Klinberg, G. Dental anxiety and behaviour management problems in paediatric dentistry—A review of background factors and diagnostics. Eur. Arch. Paediatr. Dent. 2008, 9 (Suppl. 1), 11–15. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, M.; Murielly, T.; Assis, P.; Maciel, C.; Colares, V. How to evaluate adolescents’ dental anxiety? A review of instruments. Arch. Health Investig. 2019, 8, 522–528. [Google Scholar] [CrossRef] [Green Version]
- Murad, M.H.; Ingle, N.A.; Assery, M.K. Evaluating factors associated with fear and anxiety to dental treatment—A systematic review. J. Fam. Med. Prim. Care 2020, 9, 4530–4535. [Google Scholar] [CrossRef] [PubMed]
- Sarapultseva, M.; Yarushina, M.; Kritsky, I.; Ibragimov, R.; Sarapultsev, A. Prevalence of dental fear and anxiety among Russian children of different ages: The cross-sectional study. Eur. J. Dent. 2020, 14, 621–625. [Google Scholar] [CrossRef]
- Oba, A.A.; Dülgergil, C.T.; Sönmez, I.S. Prevalence of dental anxiety in 7- to 11-year-old children and its relationship to dental caries. Med. Princ. Pract. 2009, 18, 453–457. [Google Scholar] [CrossRef]
- Rantavuori, K.; Zerman, N.; Ferro, R.; Lahti, S. Relationship between children’s first dental visit and their dental anxiety in the Veneto Region of Italy. Acta Odontol. Scand. 2002, 60, 297–300. [Google Scholar] [CrossRef]
- Carrillo-Diaz, M.; Crego, A.; Armfield, J.M.; Romero-Maroto, M. Treatment experience, frequency of dental visits, and children’s dental fear: A cognitive approach. Eur. J. Oral Sci. 2012, 120, 75–81. [Google Scholar] [CrossRef]
- Torriani, D.D.; Ferro, R.L.; Bonow, M.L.M.; Santos, I.S.; Matijasevich, A.; Barros, A.J.; Demarco, F.F.; Peres, K.G. Dental caries is associated with dental fear in childhood: Findings from a birth cohort study. Caries Res. 2014, 48, 263–270. [Google Scholar] [CrossRef]
- Soares, F.C.; Lima, R.A.; Salvador, D.M.; de Barros, M.V.G.; Dahllof, G.; Colares, V. Reciprocal longitudinal relationship between dental fear and oral health in schoolchildren. Int. J. Paediatr. Dent. 2020, 30, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Barreto, K.A.; Dos Prazeres, L.D.; Lima, D.S.M.; Soares, F.C.; Redivivo, R.M.; da Franca, C.; Colares, V. Factors associated with dental anxiety in Brazilian children during the first transitional period of the mixed dentition. Eur. Arch. Paediatr. Dent. 2017, 18, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Armfield, J.M.; Stewart, J.F.; Spencer, A.J. The vicious cycle of dental fear: Exploring the interplay between oral health, service utilization and dental fear. BMC Oral Health 2007, 7, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suprabha, B.S.; Rao, A.; Choudhary, S.; Shenoy, R. Child dental fear and behavior: The role of environmental factors in a hospital cohort. J. Indian Soc. Pedod. Prev. Dent. 2011, 29, 95–101. [Google Scholar] [CrossRef]
- Alharbi, A.; Freeman, R.; Humphris, G. Dental anxiety, child-oral health related quality of life and self-esteem in children and adolescents: A systematic review and meta-analysis of their patterns of association. Community Dent. Health 2021, 38, 119–126. [Google Scholar] [CrossRef]
- Gustafsson, A.; Arnrup, K.; Broberg, A.G.; Bodin, L.; Berggren, U. Psychosocial concomitants to dental fear and behaviour management problems. Int. J. Pediatr. Dent. 2007, 17, 449–459. [Google Scholar] [CrossRef]
- Wu, L.; Gao, X. Children’s dental fear and anxiety: Exploring family related factors. BMC Oral Health 2018, 18, 100. [Google Scholar] [CrossRef] [Green Version]
- Vigu, A.; Stanciu, D. When the fear of dentist is relevant for more than one’s oral health. A structural equation model of dental fear, self-esteem, oral-health-related well-being, and general well-being. Patient Prefer. Adherence 2019, 13, 1229–1240. [Google Scholar] [CrossRef] [Green Version]
- Kavaliauskienė, A. Impact of Malocclusion on Oral Health-Related Quality of Life among Adolescents in Lithuania. Ph.D. Thesis, Lithuanian University of Health Sciences, Kaunas, Lithuania, 2019. [Google Scholar]
- Žemaitienė, M. Prevalence and Experience of Dental Caries and Analysis of Behavioural and Biological Risk Indicators among Lithuanian Schoolchildren in Late Adolescence. Ph.D. Thesis, Lithuanian University of Health Sciences, Kaunas, Lithuania, 2017. [Google Scholar]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G. Strengthening the reporting of observational studies in epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [Green Version]
- Neverlien, P.O. Assessment of a single-item dental anxiety question. Acta Odontol. Scand. 1990, 48, 365–369. [Google Scholar] [CrossRef]
- Venckutė, R. Rosenbergo Savigarbos Skalė (Rosenberg’s Self-Esteem Scale). 2012. Available online: https://psichika.eu/blog/testas-rosenbergo-savigarbos-skale/ (accessed on 7 June 2021). (In Lithuanian).
- Kavaliauskienė, A.; Šidlauskas, A.; Zaborskis, A. Modification and psychometric evaluation of the Child Perceptions Questionnaire (CPQ11–14) in assessing oral health-related quality of life among Lithuanian children. BMC Oral Health 2019, 19, 1. [Google Scholar] [CrossRef]
- Currie, C.; Griebler, R.; Inchley, J.; Theunissen, A.; Molcho, M.; Samdal, O.; Dür, W. (Eds.) Health Behaviour in School-Aged Children (HBSC) Study Protocol: Background, Methodology and Mandatory Items for the 2009/2010 Survey; LBIHPR: Vienna, Austria; CAHRU: Edinburgh, UK, 2010. [Google Scholar]
- Čekanavičius, V.; Murauskas, G. Taikomoji Regresinė Analizė Socialiniuose Tyrimuose (Applied Regression Analysis in Social Sciences); Vilnius University: Vilnius, Lithuania, 2014. (In Lithuanian) [Google Scholar]
- Hayat, M.J.; Higgins, M. Understanding poisson regression. J. Nurs. Educ. 2014, 53, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Moksony, F.; Hegedus, R. The use of Poisson regression in the sociological study of suicide. Corvinus J. Sociol. Soc. Policy 2014, 5, 97–114. [Google Scholar] [CrossRef]
- Viinikangas, A.; Lahti, S.; Yuan, S.; Pietilä, I.; Freeman, R.; Humphris, G. Evaluating a single dental anxiety question in Finnish adults. Acta Odontol. Scand. 2007, 65, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Mathias, F.B.; Cademartori, M.G.; Goettems, M.L. Factors associated with children’s perception of pain following dental treatment. Eur. Arch. Paediatr. Dent. 2020, 21, 137–143. [Google Scholar] [CrossRef]
- Colares, V.; Franca, C.; Ferreira, A.; Amorim Filho, H.A.; Oliveira, M.C.A. Dental anxiety and dental pain in 5- to 12-year-old children in Recife, Brazil. Eur. Arch. Paediatr. Dent. 2013, 14, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Silveira, E.R.D.; Goettems, M.L.; Demarco, F.F.; Azevedo, M.S. Clinical and individual variables in children’s dental fear: A school-based investigation. Braz. Dent. J. 2017, 28, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Schuch, H.S.; Correa, M.B.; Torriani, D.D.; Demarco, F.F.; Goettems, M.L. Perceived dental pain: Determinants and impact on brazilian schoolchildren. J. Oral Facial Pain Headache 2015, 29, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Olak, J.; Saag, M.; Honkala, S.; Nommela, R.; Runnel, R.; Honkala, E.; Karjalainen, S. Children’s dental fear in relation to dental health and parental dental fear. Stomatol. Balt. Dent. Maxillofac. J. 2013, 15, 26–31. [Google Scholar]
- Nguyen, M.S.; Nguyen, T.T.; Nguyen, B.B.; Saag, M.; Olak, J. Dental fear and anxiety in Estonian and Vietnamese schoolchildren: A comparative study of two populations. Clin. Exp. Dent. Res. 2018, 4, 182–188. [Google Scholar] [CrossRef]
- Račienė, R. Dental Fear among Schoolchildren and Related Social and Psychological Factors. Ph.D. Thesis, Kaunas University of Medicine, Kaunas, Lithuania, 2009. (In Lithuanian). [Google Scholar]
- Do, C. Applying social learning theory to children with dental anxiety. J. Contemp. Dent. Pract. 2004, 5, 126–135. [Google Scholar] [CrossRef] [Green Version]
- Carter, A.E.; Carter, G.; Boschen, M.; AlShwaimi, E.; George, R. Pathways of fear and anxiety in dentistry: A review. World J. Clin. Cases 2014, 2, 642–653. [Google Scholar] [CrossRef] [PubMed]
- Pūrienė, A.; Petrauskienė, J.; Balčiūnienė, I.; Janulytė, V.; Kutkauskienė, J.; Musteikytė, M. Privati ar valstybinė odontologinė gydymo įstaiga? Lietuvos pacientų nuomonė ir patirtis (Private or public dental care institution? The patients’ opinions and experience in Lithuania). Medicina 2008, 10, 805–811. [Google Scholar] [CrossRef] [Green Version]
- Gao, S.; Lu, J.; Li, P.; Yu, D.; Zhao, W. Prevalence and risk factors of children’s dental anxiety in China: A longitudinal study. BMJ Open 2021, 11, e043647. [Google Scholar] [CrossRef]
- El-Housseiny, A.A.; Farsi, N.M.; Alamoudi, N.M.; Bagher, S.M.; El Derwi, D. Assessment for the Children’s fear survey schedule-dental subscale. J. Clin. Pediatr. Dent. 2014, 39, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.; Reid, C.; Wilson, K.; Girdler, N.M. Inter-rater agreement between children’s self-reported and parents’ proxy-reported dental anxiety. Br. Dent. J. 2015, 218, E6. [Google Scholar] [CrossRef]
- Rantavuori, K.; Lahti, S.; Hausen, H.; Seppä, L.; Kärkkäinen, S. Dental fear and oral health and family characteristics of Finnish children. Acta Odontol. Scand. 2004, 62, 207–213. [Google Scholar] [CrossRef]
- Nicolas, E.; Bessadet, M.; Collado, V.; Carrasco, P.; Rogerleroi, V.; Hennequin, M. Factors affecting dental fear in French children aged 5–12 years. Int. J. Paediatr. Dent. 2010, 20, 366–373. [Google Scholar] [CrossRef]
- Kakkar, M.; Wahi, A.; Thakkar, R.; Vohra, I.; Shukla, A.K. Prevalence of dental anxiety in 10–14 years old children and its implications. J. Dent. Anesth. Pain Med. 2016, 16, 199–202. [Google Scholar] [CrossRef] [Green Version]
- Alshoraim, M.A.; El-Housseiny, A.A.; Farsi, N.M.; Felemban, O.M.; Alamoudi, N.M.; Alandejani, A.A. Effects of child characteristics and dental history on dental fear: Cross-sectional study. BMC Oral Health 2018, 18, 33. [Google Scholar] [CrossRef] [Green Version]
- Boka, V.; Arapostathis, K.; Karagiannis, V.; Kotsanos, N.; van Loveren, C.; Veerkamp, J. Dental fear and caries in 6–12 year old children in Greece. Determination of dental fear cut-off points. Eur. J. Paediatr. Dent. 2017, 18, 45. [Google Scholar] [CrossRef]
- Goettems, M.L.; Shqair, A.Q.; Bergmann, V.F.; Cadermatori, M.G.; Correa, M.B.; Demarco, F.F. Oral health self-perception, dental caries, and pain: The role of dental fear underlying this association. Int. J. Paediatr. Dent. 2018, 28, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Kavaliauskienė, A.; Šidlauskas, A.; Žemaitienė, M.; Slabšinskienė, E.; Zaborskis, A. Relationships of dental caries and malocclusion with oral health-related quality of life in Lithuanian adolescents aged 15 to 18 years: A cross-sectional study. Int. J. Environ. Res. Public Health 2020, 17, 4072. [Google Scholar] [CrossRef] [PubMed]
- Chapman, H.R.; Kirby-Turner, N. Psychological intrusion—An overlooked aspect of dental fear. Front. Psychol 2018, 9, 501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Locker, D. Psychosocial consequences of dental fear and anxiety. Community Dent. Oral Epidemiol. 2003, 31, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Cinar, A.B.; Murtomaa, H. A comparison of psychosocial factors related to dental anxiety among Turkish and Finnish pre-adolescents. Oral Health Prev. Dent. 2007, 5, 173–179. [Google Scholar] [PubMed]
- American Academy of Pediatric Dentistry. Oral Health Policies & Recommendations (The Reference Manual of Pediatric Dentistry): Periodicity of Examination, Preventive Dental Services, Anticipatory Guidance/Counseling, and Oral Treatment for Infants, Children, and Adolescents. 2021. Available online: https://www.aapd.org/research/oral-health-policies--recommendations/ (accessed on 7 June 2021).
- Oliveira, L.B.; Massignan, C.; De Carvalho, R.M.; Savi, M.G.; Bolan, M.; Porporatti, A.L.; Luca Canto, G. Children’s perceptions of dentist’s attire and environment: A systematic review and meta-analysis. Int. J. Clin. Pediatr. Dent. 2020, 13, 700–716. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Levin, K.A. Study design III: Cross-sectional studies. Evid.-Based Dent. 2006, 7, 24–25. [Google Scholar] [CrossRef]


{kind=link}
| Gender | Age Group | Total | ||
|---|---|---|---|---|
| 11–14 Years | 15–16 Years | 17–18 Years | ||
| Boys | 128 (8.1%) | 313 (19.7%) | 222 (14.0%) | 663 (41.7%) |
| Girls | 179 (11.3%) | 407 (25.6%) | 341 (21.4%) | 927 (58.3%) |
| Total | 307 (19.3%) | 720 (45.3%) | 563 (35.4%) | 1590 (100%) |
| Characteristic | n (%) of Respondents | |
|---|---|---|
| Urban/rural residence: | ||
| urban | 1087 | (68.5) |
| rural | 500 | (31.5) |
| missing | 3 | |
| Family affluence: | ||
| high | 794 | (51.1) |
| medium | 573 | (36.9) |
| low | 186 | (12.0) |
| missing | 37 | |
| Self-reported general health status: | ||
| good health | 1356 | (85.3) |
| less good health | 233 | (14.7) |
| missing | 1 | |
| Self-reported rating of caries experience: | ||
| not at all | 1043 | (65.8) |
| treatment is needed | 542 | (34.2) |
| missing | 5 | |
| Self-reported rating of malocclusion: | ||
| no anomalies | 683 | (43.1) |
| anomalies were observed | 902 | (56.9) |
| missing | 5 | |
| Teeth brushing: | ||
| regular | 1008 | (63.4) |
| irregular | 582 | (36.6) |
| missing | 0 | |
| Self-esteem: | ||
| high | 787 | (51.0) |
| low | 755 | (49.0) |
| missing | 48 | |
| Overall life satisfaction: | ||
| high | 994 | (62.7) |
| low | 591 | (37.3) |
| missing | 5 | |
| Oral health-related quality of life: | ||
| high | 985 | (61.9) |
| low | 605 | (38.1) |
| missing | 0 | |
| Characteristic | No. (%) of Respondents | |
|---|---|---|
| Father’s education: | ||
| lower | 402 | (43.9) |
| higher | 514 | (56.1) |
| missing | 483 | |
| Mother’s education: | ||
| lower | 374 | (33.3) |
| higher | 748 | (66.7) |
| missing | 277 | |
| Age at the first visit to the dentist: | ||
| up to 6 years | 636 | (54.2) |
| 6 years or older | 537 | (45.8) |
| missing | 226 | |
| Parental opinion about child’s dental fear: | ||
| has a dental fear | 454 | (32.6) |
| earlier had a dental fear | 277 | (19.9) |
| no dental fear | 660 | (47.4) |
| missing | 8 | |
| Dental fear was caused by the toothache: | ||
| no | 1286 | (92.5) |
| yes | 105 | (7.5) |
| missing | 8 | |
| Dental fear was caused by dentist’s actions: | ||
| no | 1256 | (90.3) |
| yes | 135 | (9.7) |
| missing | 8 | |
| Dental fear was caused by too young a child: | ||
| no | 1126 | (80.9) |
| yes | 265 | (19.1) |
| missing | 8 | |
| Dental fear was caused by high child’s sensitivity: | ||
| no | 1168 | (83.9) |
| yes | 224 | (16.1) |
| missing | 7 | |
| Fear was caused by poor psychological readiness: | ||
| no | 1317 | (94.7) |
| yes | 74 | (5.3) |
| missing | 8 | |
| Variable | Category | Relative Ratio of the Fear Score Means (95% CI) and p-Value | |||||
|---|---|---|---|---|---|---|---|
| Total a | Gender b | Age Group c | |||||
| Boys | Girls | 11–14 Years | 15–16 Years | 17–18 Years | |||
| Gender | Girls | 1.19 (1.12–1.27) p < 0.001 | 1.19 (1.05–1.35) p = 0.006 | 1.24 (1.13–1.36) p < 0.001 | 1.14 (1.02–1.27) p = 0.023 | ||
| Boys | 1.00 | 1.00 | 1.00 | 1.00 | |||
| Age group | 17–18 years | 1.03 (0.95–1.12) p = 0.490 | 1.06 (0.94–1.20) p = 0.328 | 1.01 (0.90–1.13) p = 0.839 | |||
| 15–16 years | 1.05 (0.97–1.13) p = 0.240 | 1.02 (0.91–1.15) p = 0.691 | 1.06 (0.95–1.19) p = 0.264 | ||||
| 11–14 years | 1.00 | 1.00 | 1.00 | ||||
| Self-reported general health status | Less good health | 1.00 (0.92–1.09) p = 0.962 | 0.91 (0.78–1.05) p = 0.194 | 1.06 (0.95–1.17) p = 0.323 | 0.88 (0.72–1.07) p = 0.192 | 1.03 (0.90–1.17) p = 0.675 | 1.04 (0.90–1.20) p = 0.565 |
| Good health | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Self-reported rating of caries experience | Treatment is needed | 1.14 (1.07–1.22) p < 0.001 | 1.12 (1.02–1.24) p = 0.024 | 1.16 (1.07–1.26) p ≤ 0.001 | 1.14 (0.97–1.26) p = 0.143 | 1.14 (1.03–1.26) p = 0.009 | 1.17 (1.06–1.31) p = 0.003 |
| No carries lesions | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Self-reported rating of malocclusion | Anomalies were observed | 1.01 (0.95–1.08) p = 0.708 | 0.96 (0.87–1.05) p = 0.354 | 1.06 (0.97–1.15) p = 0.196 | 1.10 (0.97–1.25) p = 0.140 | 0.95 (0.86–1.04) p = 0.242 | 1.04 (0.93–1.16) p = 0.474 |
| No anomalies | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Tooth brushing | Irregular | 1.04 (0.97–1.11) p = 0.285 | 1.03 (0.94–1.13) p = 0.530 | 1.04 (0.95–1.14) p = 0.383 | 1.08 (0.95–1.23) p = 0.264 | 1.02 (0.92–1.12) p = 0.756 | 1.03 (0.92–1.16) p = 0.600 |
| Regular | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Variable | Category | Relative Ratio of the Fear Score Means (95% CI) and p-Value | |||||
|---|---|---|---|---|---|---|---|
| Total | Gender | Age Group | |||||
| Boys | Girls | 11–14 Years | 15–16 Years | 17–18 Years | |||
| Self-esteem | Low | 1.10 (1.04–1.18) p = 0.002 | 1.11 (1.01–1.22) p = 0.032 | 1.10 (1.01–1.19) p = 0.027 | 1.09 (0.96–1.24) p = 0.179 | 1.05 (0.96–1.16) p = 0.289 | 1.18 (1.06–1.31) p = 0.003 |
| High | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Oral health-related quality of life | Low | 1.13 (1.07–1.21) p < 0.001 | 1.13 (1.03–1.25) p = 0.013 | 1.14 (1.05–1.23) p = 0.002 | 1.23 (1.08–1.39) p = 0.002 | 1.06 (0.96–1.17) p = 0.241 | 1.17 (1.05–1.30) p = 0.004 |
| High | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Overall life satisfaction | Low | 1.07 (1.01–1.14) p = 0.036 | 1.10 (0.99–1.21) p = 0.062 | 1.05 (0.97–1.14) p = 0.260 | 1.03 (0.91–1.18) p = 0.636 | 1.05 (0.96–1.16) p = 0.296 | 1.13 (1.01–1.24) p = 0.042 |
| High | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Variable | Category | Relative Ratio of the Fear Score Means (95% CI) and p-Value | |||||
|---|---|---|---|---|---|---|---|
| Total | Gender | Age Group | |||||
| Boys | Girls | 11–14 Years | 15–16 Years | 17–18 Years | |||
| Urban/rural residence | Rural | 1.08 (1.01–1.15) p = 0.026 | 1.06 (0.95–1.16) p = 0.301 | 1.09 (1.01–1.19) p = 0.040 | 1.01 (0.88–1.16) p = 0.887 | 1.09 (0.99–1.20) p = 0.085 | 1.07 (0.96–1.20) p = 0.208 |
| Urban | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Family affluence | Low | 1.11 (1.01–1.22) p = 0.042 | 1.03 (0.87–1.21) p = 0.744 | 1.15 (1.02–1.30) p = 0.021 | 1.12 (0.91–1.37) p = 0.303 | 1.04 (0.90–1.20) p = 0.607 | 1.24 (1.05–1.46) p = 0.011 |
| Middle | 1.04 (0.98–1.11) p = 0.219 | 1.07 (0.96–1.19) p = 0.204 | 1.03 (0.94–1.12) p = 0.557 | 1.08 (0.95–1.24) p = 0.252 | 1.02 (0.92–1.12) p = 0.780 | 1.08 (0.96–1.21) p = 0.203 | |
| High | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Father’s education | Lower | 1.00 (0.93–1.09) p = 0.920 | 1.00 (0.87–1.14) p = 0.997 | 0.99 (0.89–1.09) p = 0.986 | 0.80 (0.65–0.97) p = 0.020 | 1.09 (0.97–1.22) p = 0.164 | 1.00 (0.86–1.14) p = 0.925 |
| Higher | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Mother’s education | Lower | 1.08 (1.01–1.17) p = 0.041 | 1.07 (0.95–1.21) p = 0.289 | 1.08 (0.98–1.19) p = 0.107 | 0.96 (0.81–1.13) p = 0.599 | 1.13 (1.01–1.20) p = 0.033 | 1.11 (0.97–1.26) p = 0.126 |
| Higher | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Variable | Category | Relative Ratio of the Fear Score Means (95% CI) and p-Value | |||||
|---|---|---|---|---|---|---|---|
| Total | Gender | Age Group | |||||
| Boys | Girls | 11–14 Years | 15–16 Years | 17–18 Years | |||
| Parental opinion about child’s dental fear | Have a dental fear | 1.59 (1.48–1.71) p < 0.001 | 1.53 (1.37–1.72) p < 0.001 | 1.63 (1.49–1.78) p < 0.001 | 1.56 (1.35–1.82) p < 0.001 | 1.66 (1.49–1.85) p < 0.001 | 1.52 (1.34–1.72) p < 0.001 |
| Earlier had a dental fear | 1.08 (0.99–1.19) p = 0.094 | 1.06 (0.92–1.24) p = 0.419 | 1.10 (0.98–1.24) p = 0.110 | 1.03 (0.84–1.27) p = 0.751 | 1.11 (0.97–1.28) p = 0.133 | 1.09 (0.92–1.28) p = 0.313 | |
| No dental fear | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Age at the first visit to the dentist | 6 years or older | 1.08 (1.01–1.16) p = 0.036 | 1.12 (0.99–1.26) p = 0.065 | 1.04 (0.95–1.14) p = 0.353 | 1.17 (1.01–1.36) p = 0.040 | 1.04 (0.94–1.16) p = 0.454 | 1.04 (0.92–1.16) p = 0.506 |
| Up to 6 years | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Fear was caused by toothache | Yes | 1.18 (1.06–1.32) p = 0.003 | 1.16 (0.98–1.36) p = 0.078 | 1.21 (1.05–1.41) p = 0.011 | 1.54 (1.22–1.95) p < 0.001 | 1.04 (0.88–1.22) p = 0.653 | 1.24 (1.02–1.52) p = 0.032 |
| No | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Fear was caused by the dentist’s actions | Yes | 1.09 (1.04–1.15) p = 0.001 | 0.97 (0.86–1.08) p = 0.529 | 1.13 (1.07–1.20) p < 0.001 | 1.01 (0.90–1.13) p = 0.914 | 1.09 (1.01–1.17) p = 0.031 | 1.16 (1.06–1.26) p = 0.001 |
| No | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Fear was caused by too young child | Yes | 1.01 (0.98–1.04) p = 0.448 | 1.02 (0.97–1.06) p = 0.498 | 1.01 (0.97–1.05) p = 0.634 | 1.04 (0.98–1.11) p = 0.181 | 1.03 (0.98–1.07) p = 0.242 | 0.98 (0.93–1.03) p = 0.354 |
| No | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Fear was caused by high child’s sensitivity | Yes | 1.08 (1.06–1.10) p < 0.001 | 1.05 (1.02–1.09) p = 0.005 | 1.09 (1.06–1.12) p < 0.001 | 1.06 (1.02–1.11) p = 0.010 | 1.08 (1.05–1.11) p < 0.001 | 1.08 (1.04–1.12) p < 0.001 |
| No | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
| Fear was caused by poor psychological readiness | Yes | 1.05 (1.02–1.08) p < 0.001 | 1.05 (1.01–1.10) p = 0.024 | 1.05 (1.02–1.09) p = 0.003 | 1.04 (0.96–1.13) p = 0.374 | 1.06 (1.03–1.10) p = 0.001 | 1.04 (0.99–1.08) p = 0.108 |
| No | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Slabšinskienė, E.; Kavaliauskienė, A.; Žemaitienė, M.; Vasiliauskienė, I.; Zaborskis, A. Dental Fear and Associated Factors among Children and Adolescents: A School-Based Study in Lithuania. Int. J. Environ. Res. Public Health 2021, 18, 8883. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168883
Slabšinskienė E, Kavaliauskienė A, Žemaitienė M, Vasiliauskienė I, Zaborskis A. Dental Fear and Associated Factors among Children and Adolescents: A School-Based Study in Lithuania. International Journal of Environmental Research and Public Health. 2021; 18(16):8883. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168883
Chicago/Turabian StyleSlabšinskienė, Eglė, Aistė Kavaliauskienė, Miglė Žemaitienė, Ingrida Vasiliauskienė, and Apolinaras Zaborskis. 2021. "Dental Fear and Associated Factors among Children and Adolescents: A School-Based Study in Lithuania" International Journal of Environmental Research and Public Health 18, no. 16: 8883. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168883