
Relationships of Dietary Habits and Physical Activity Status with Non-Alcoholic Fatty Liver Disease Featuring Advanced Fibrosis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
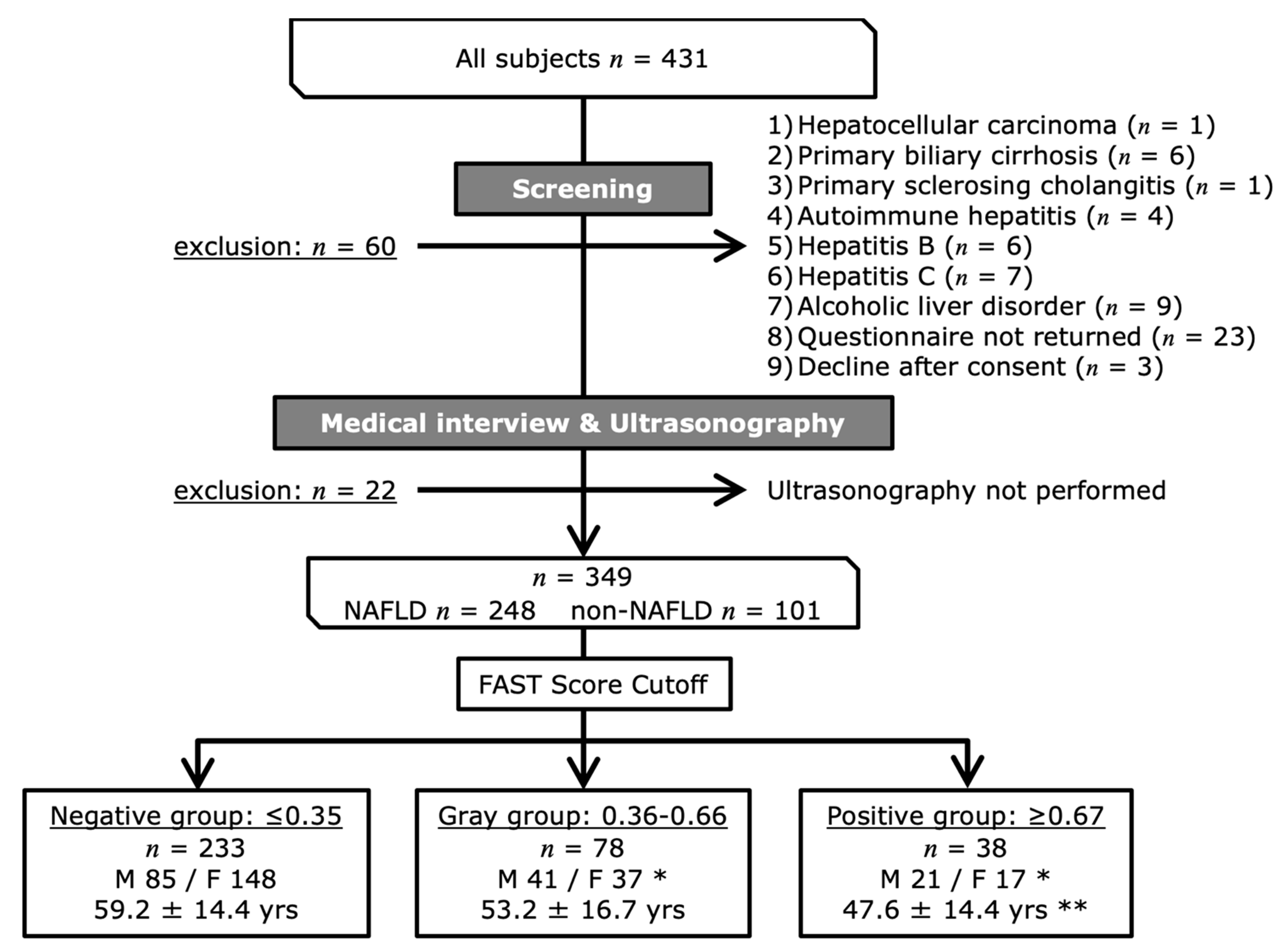
2.1. Participants
2.2. Questionnaire Survey Regarding Dietary Habits and Physical Activity
2.3. Anthropometric Measurements
2.4. Clinical and Laboratory Measurements
2.5. Liver Stiffness and Steatosis
2.6. FibroScan-AST Score
2.7. Statistical Analysis
3. Results
3.1. Categorization of the Participants According to Their FAST Score
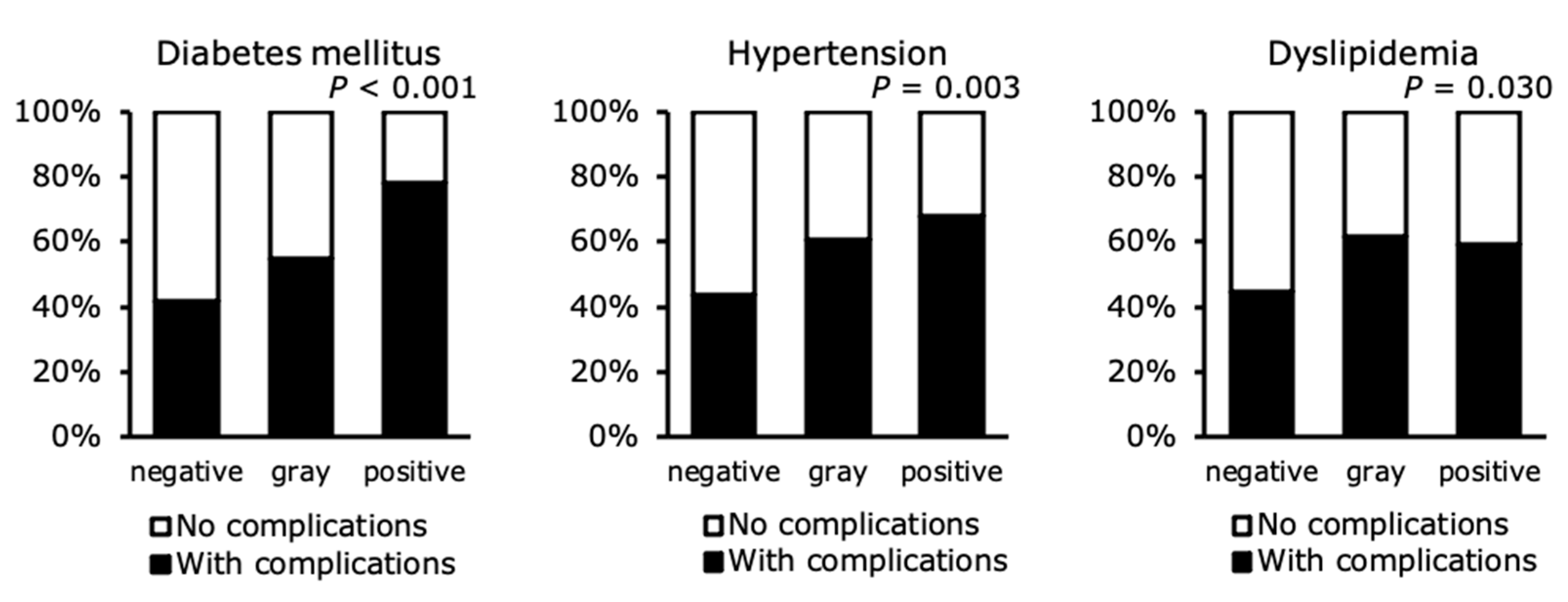
3.2. Prevalences of Lifestyle-Related Diseases
3.3. Clinical Data
3.4. Anthropometric Characteristics of the Groups
3.5. NAFLD-Related Parameters among the Groups
3.6. Muscle-Related Characteristics
3.7. Biochemical Characteristics
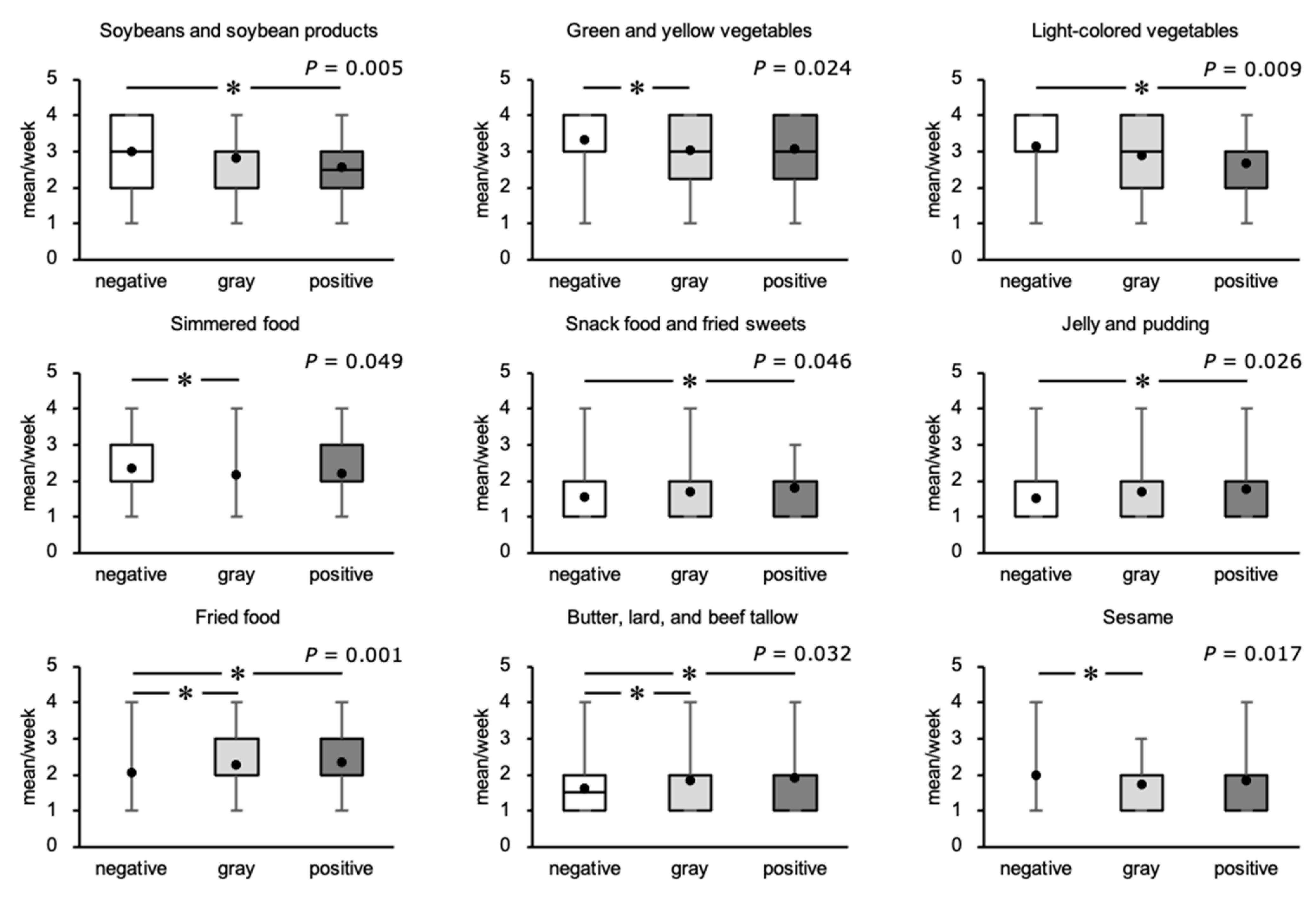
3.8. Food Consumption Frequency
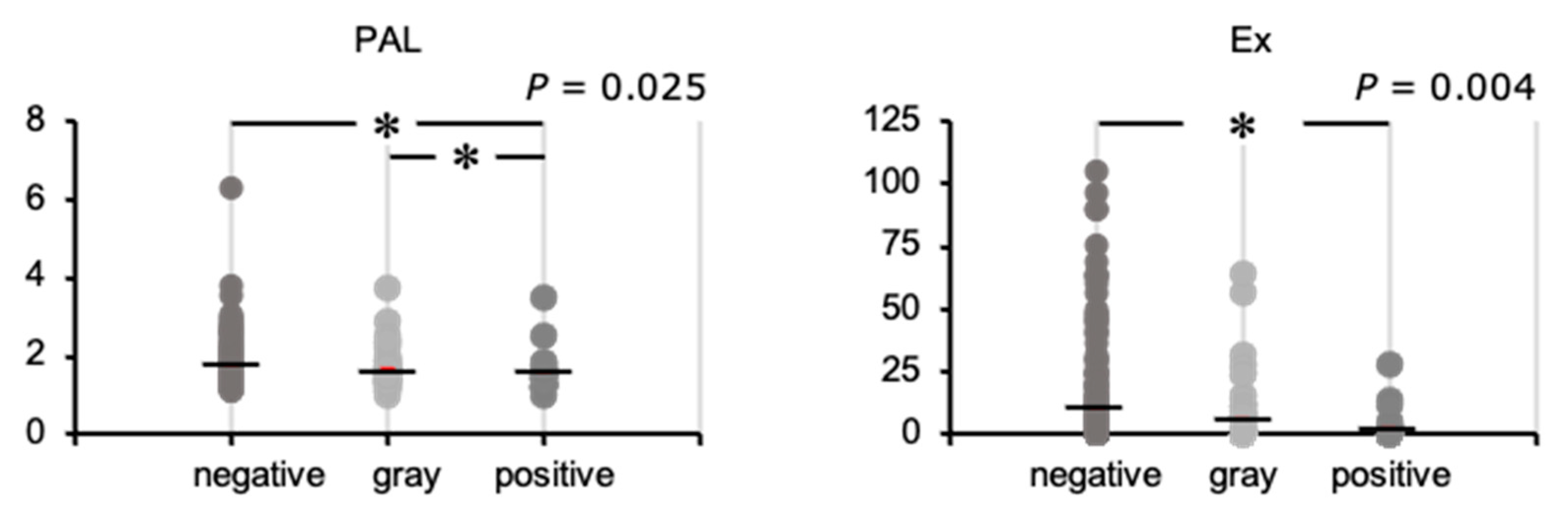
3.9. Physical Activity Status
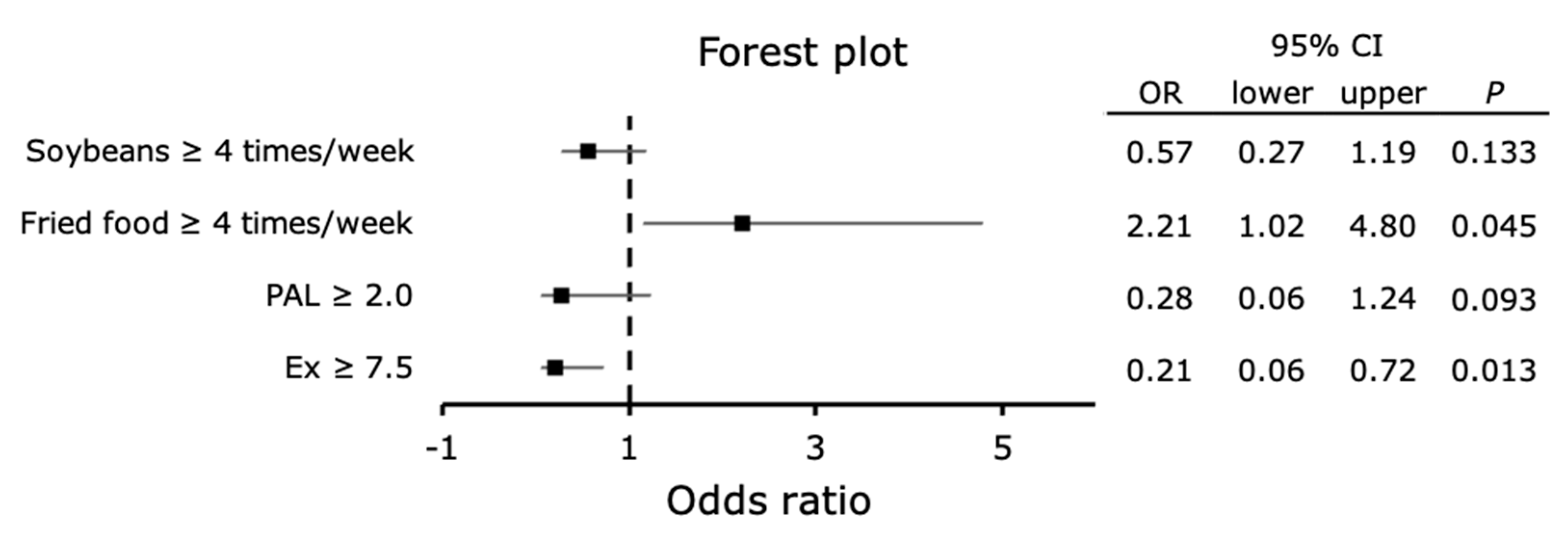
3.10. Relationship of Hepatic Fibrosis with the Frequency of Food-Type and Physical Activity Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Akihiro, O.; Takao, K.; Masahide, H.; Kiyoshi, N.; Kazutoshi, W.; Ryuhei, T.; Akio, O.; Fumiko, D.; Nobuaki, Y. Changes in Non-alcoholic Fatty Liver Disease (NAFLD) Frequency and Examination Results in Health Check-ups Over 20-year Period (1996 through 2015). Ningen Dock 2017, 32, 491–497. [Google Scholar]
- Targher, G. Non-alcoholic fatty liver disease, the metabolic syndrome and the risk of cardiovascular disease: The plot thickens. Diabet. Med. 2007, 24, 1–6. [Google Scholar] [CrossRef]
- Loomba, R.; Chalasani, N. The Hierarchical Model of NAFLD: Prognostic Significance of Histologic Features in NASH. Gastroenterology 2015, 149, 278–281. [Google Scholar] [CrossRef]
- Toshimitsu, K.; Matsuura, B.; Ohkubo, I.; Niiya, T.; Furukawa, S.; Hiasa, Y.; Kawamura, M.; Ebihara, K.; Onji, M. Dietary habits and nutrient intake in non-alcoholic steatohepatitis. Nutrition 2007, 23, 46–52. [Google Scholar] [CrossRef]
- Mayumi, T.; Kayoko, T.; Makoto, H.; Tatsuya, I.; Ikuyo, T. Increase of the Plasma Trans-fatty Acid Level in Middle-aged Japanese Men with Non-alcoholic Fatty Liver Disease. J. Jpn. Soc. Nutr. Food Sci. 2014, 67, 137–143. [Google Scholar]
- Vos, M.B.; Goran, M.I. Sugar, Sugar... Not So Sweet for the Liver. Gastroenterology 2017, 153, 642–645. [Google Scholar] [CrossRef] [Green Version]
- Abdelmalek, M.F.; Suzuki, A.; Guy, C.; Unalp-Arida, A.; Colvin, R.; Johnson, R.J.; Diehl, A.M. Increased fructose consumption is associated with fibrosis severity in patients with nonalcoholic fatty liver disease. Hepatology 2010, 51, 1961–1971. [Google Scholar] [CrossRef] [Green Version]
- Hashidume, T.; Kato, A.; Tanaka, T.; Miyoshi, S.; Itoh, N.; Nakata, R.; Inoue, H.; Oikawa, A.; Nakai, Y.; Shimizu, M.; et al. Single ingestion of soy β-conglycinin induces increased postprandial circulating FGF21 levels exerting beneficial health effects. Sci. Rep. 2016, 6, 28183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, J.H.; Sung, M.K.; Kawada, T.; Yoo, H.; Kim, Y.K.; Kim, J.S.; Yu, R. Soybean saponins suppress the release of proinflammatory mediators by LPS-stimulated peritoneal macrophages. Cancer Lett. 2005, 230, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Zou, J.; Chassaing, B.; Singh, V.; Pellizzon, M.; Ricci, M.; Fythe, M.D.; Kumar, M.V.; Gewirtz, A.T. Fiber-Mediated Nourishment of Gut Microbiota Protects against Diet-Induced Obesity by Restoring IL-22-Mediated Colonic Health. Cell Host Microbe 2018, 23, 41–53.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Service Bureau. Exercise and Physical Activity Reference for Health Promotion (EPAR) 2013; Ministry of Health, Labour and Welfare: Tokyo, Japan, 2013. [Google Scholar]
- Oh, S.; Shida, T.; Yamagishi, K.; Tanaka, K.; So, R.; Tsujimoto, T.; Shoda, J. Moderate to vigorous physical activity volume is an important factor for managing nonalcoholic fatty liver disease: A retrospective study. Hepatology 2015, 61, 205–215. [Google Scholar] [CrossRef]
- Oh, S.; Tanaka, K.; Tsujimoto, T.; So, R.; Shida, T.; Shoda, J. Regular exercise coupled to diet regimen accelerates reduction of hepatic steatosis and associated pathological conditions in nonalcoholic fatty liver disease. Metab. Syndr. Relat. Disord. 2014, 12, 290–298. [Google Scholar] [CrossRef]
- Angulo, P. Noninvasive assessment of fibrosis and steatosis in NASH and ASH. Gastroenterol. Clin. Biol. 2009, 33, 940–948. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Kim, K.I.; Kim, S.R. Overview of Nonalcoholic Fatty Liver Disease/Nonalcoholic Steatohepatitis Management. Yakugaku Zasshi 2019, 139, 1147–1153. [Google Scholar] [CrossRef]
- Newsome, P.N.; Sasso, M.; Deeks, J.J.; Paredes, A.; Boursier, J.; Chan, W.K.; Yilmaz, Y.; Czernichow, S.; Zheng, M.H.; Wong, V.W.; et al. FibroScan-AST (FAST) score for the non-invasive identification of patients with non-alcoholic steatohepatitis with significant activity and fibrosis: A prospective derivation and global validation study. Lancet Gastroenterol. Hepatol. 2020, 5, 362–373. [Google Scholar] [CrossRef] [Green Version]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef]
- Oeda, S.; Takahashi, H.; Imajo, K.; Seko, Y.; Kobayashi, T.; Ogawa, Y.; Moriguchi, M.; Yoneda, M.; Anzai, K.; Irie, H.; et al. Diagnostic accuracy of FibroScan-AST score to identify non-alcoholic steatohepatitis with significant activity and fibrosis in Japanese patients with non-alcoholic fatty liver disease: Comparison between M and XL probes. Hepatol. Res. 2020, 50, 31–839. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, Y. Food Frequency Questionnaire for Excel Eiyokun (FFQg), 5th ed.; Kenpakusha: Tokyo, Japan, 2016. [Google Scholar]
- Nobuo, Y.; Fumi, H.; Yukari, T.; Keiko, M.; Fukue, S. A New Food Guide in Japan: The Japanese Food Guide Spinning Top. Nutr. Rev. 2007, 65, 149–154. [Google Scholar]
- Junko, O.; Ayano, F.; Akiko, K.; Kiyoshi, T. Estimation of Physical Activity Level in Elderly Nursing Home Residents. Jpn. J. Nutr. Diet. 2013, 71, 235–241. [Google Scholar]
- Sergi, G.; De Rui, M.; Stubbs, B.; Veronese, N.; Manzato, E. Measurement of lean body mass using bioelectrical impedance analysis: A consideration of the pros and cons. Aging Clin. Exp. Res. 2017, 29, 591–597. [Google Scholar] [CrossRef]
- Shida, T.; Akiyama, K.; Oh, S.; Sawai, A.; Isobe, T.; Okamoto, Y.; Ishige, K.; Mizokami, Y.; Yamagata, K.; Onizawa, K.; et al. Skeletal muscle mass to visceral fat area ratio is an important determinant affecting hepatic conditions of non-alcoholic fatty liver disease. J. Gastroenterol. 2018, 53, 535–547. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M.; et al. The FNIH sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. A Bio.L Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.N.; Park, M.S.; Lim, K.I.; Yang, S.J.; Yoo, H.J.; Kang, H.J.; Song, W.; Seo, J.A.; Kim, S.G.; Kim, N.H.; et al. Skeletal muscle mass to visceral fat area ratio is associated with metabolic syndrome and arterial stiffness: The Korean Sarcopenic Obesity Study (KSOS). Diabetes Res. Clin. Pr. 2011, 93, 285–291. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef]
- Castera, L.; Forns, X.; Alberti, A. Non-invasive evaluation of liver fibrosis using transient elastography. J. Hepatol. 2008, 48, 835–847. [Google Scholar] [CrossRef] [PubMed]
- Karlas, T.; Petroff, D.; Sasso, M.; Fan, J.G.; Mi, Y.Q.; de Lédinghen, V.; Kumar, M.; Lupsor-Platon, M.; Han, K.H.; Cardoso, A.C.; et al. Individual patient data meta-analysis of controlled attenuation parameter (CAP) technology for assessing steatosis. J. Hepatol. 2017, 66, 1022–1030. [Google Scholar] [CrossRef]
- Yoneda, M.; Imajo, K.; Nakajima, A. Non-Invasive Diagnosis of Nonalcoholic Fatty Liver Disease. Am. J. Gastroenterol. 2018, 113, 1409–1411. [Google Scholar] [CrossRef] [PubMed]
- Science and Technology Policy Bureau. Standards Tables of Food Composition in Japan-2015-(Seventh Revised Edition) Documentation and Table; Ministry of Education, Culture, Sports, Science and Technology: Tokyo, Japan, 2015. [Google Scholar]
- Tadashi, Y.; Shigeyuki, O.; Katsutoshi, A.; Yasuteru, E.; Shuji, K.; Daisuke, S.; Hisakazu, I. Effects on Intestinal Flora of a Beverage Containing Non-fermentable Depolymerized Sodium Alginate and Water-soluble Fermentable Corn Bran Fiber. Jpn. J. Nutr. Diet. 2002, 60, 137–143. [Google Scholar]
- Romero-Gómez, M.; Zelber-Sagi, S.; Trenell, M. Treatment of NAFLD with diet, physical activity and exercise. J. Hepatol. 2017, 67, 829–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marra, F.; Svegliati-Baroni, G. Lipotoxicity and the gut-liver axis in NASH pathogenesis. J. Hepatol. 2018, 68, 280–295. [Google Scholar] [CrossRef] [PubMed]
- Delarue, J.; Lallès, J.P. Nonalcoholic fatty liver disease: Roles of the gut and the liver and metabolic modulation by some dietary factors and especially long-chain n-3 PUFA. Mol. Nutr. Food Res. 2016, 60, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.C.; Itsiopoulos, C.; Thodis, T.; Ward, G.; Trost, N.; Hofferberth, S.; O’Dea, K.; Desmond, P.V.; Johnson, N.A.; Wilson, A.M. The Mediterranean diet improves hepatic steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J. Hepatol. 2013, 59, 138–143. [Google Scholar] [CrossRef]
- Bjermo, H.; Iggman, D.; Kullberg, J.; Dahlman, I.; Johansson, L.; Persson, L.; Berglund, J.; Pulkki, K.; Basu, S.; Uusitupa, M.; et al. Effects of n-6 PUFAs compared with SFAs on liver fat, lipoproteins, and inflammation in abdominal obesity: A randomized controlled trial. Am. J. Clin. Nutr. 2012, 95, 1003–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takayuki, I.; Aisa, M.; Takashi, Y.; Naofumi, Y.; Atsushi, K.; Naoko, M.; Yuji, B.; Maasmitsu, I. Physical Activity of More than 10 Exercise Per Week Prevents Visceral Fat Obesity. Ningen Dock 2011, 25, 5. [Google Scholar]
- Junichi, S.; Sechang, O.; Takashi, S.; Kiyoji, T. Liver, Muscle, and Insulin Resistance in Obese Subjects: Exercise Effects. Jpn. J. Phys. Fit. Sports Med. 2015, 64, 42. [Google Scholar]
- Nelson, M.; Black, A.E.; Morris, J.A.; Cole, T.J. Between- and within-subject variation in nutrient intake from infancy to old age: Estimating the number of days required to rank dietary intakes with desired precision. Am. J. Clin. Nutr. 1989, 50, 155–167. [Google Scholar] [CrossRef] [Green Version]
- Okubo, H.; Sasaki, S.; Hirota, N.; Notsu, A.; Todoriki, H.; Miura, A.; Fukui, M.; Date, C. The influence of age and body mass index on relative accuracy of energy intake among Japanese adults. Public Health Nutr. 2006, 9, 651–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (Q1) | Survey of daily physical activity | (Q25) | How many green and yellow vegetables do you eat? |
| 1. | How many hours of sleep do you get? | (Q26) | How many light-colored vegetables do you eat? |
| 2. | How many hours do you spend relaxing in a lying or sitting position? | (Q27) | How much oligosaccharide do you eat? |
| 3. | How many hours of light work do you do sitting down? | (Q28) | How much jam and honey do you eat? |
| 4. | How many hours of slow walking and housework do you do? | (Q29) | How much simmered food that uses sugar or mirin do you eat? |
| 5. | How many hours of life activities and work are sustainable for a long time? | (Q30) | How many vinegared and dressed vegetables do you eat? |
| 6. | How many hours of daily life activities/work do you need to rest frequently? | (Q31) | How many Japanese sweets do you eat? |
| 7. | How many hours of exercise do you do every day, including weekends, excluding daily activities and work? | (Q32) | How much pastry and cake do you eat? |
| (Q2) | Survey of hours of exercise per week | (Q33) | How many snack foods and fried sweets do you eat? |
| 1. | How many hours of exercise such as normal walking (less than 3 to 4 METs)? | (Q34) | How many rice crackers and cookies do you eat? |
| 2. | How many hours of exercise such as fast walking (less than 4 to 6 METs)? | (Q35) | How much ice cream do you eat? |
| 3. | How many hours of exercise such as jogging (less than 6 to 8 METs)? | (Q36) | How much chocolate do you eat? |
| 4. | How many hours of running or other exercise (8–15 METs)? | (Q37) | How much candy and caramels do you eat? |
| (Q3) | How many people are in your family? Who is the main cook in your family? | (Q38) | How much jelly and pudding do you eat? |
| (Q4) | What is your current employment status? | (Q39) | How much preference beverage do you drink? |
| (Q5) | What is your current main occupation? | (Q40) | How much fried food do you eat? |
| (Q6) | What is your last educational background? | (Q41) | How much stir-fry do you eat? |
| (Q7) | What is the highest weight you have ever weighed? | (Q42) | How much mayonnaise and dressing do you use? |
| (Q8) | What was your weight when you were 20 years old? | (Q43) | How much margarine and fat spread do you use? |
| (Q9) | Are there any diseases you are currently suffering from? | (Q43) | How much butter, lard, and beef tallow do you use? |
| (Q10) | Have you had any illnesses in the past? | (Q44) | How many peanuts and almonds do you eat? |
| (Q11) | Are there any medications that you are currently taking? | (Q45) | How much sesame do you eat? |
| (Q12) | Do you eat three meals a day? | (Q46) | How much olive oil and canola oil (rapeseed oil) do you use? |
| (Q13) | What times do you eat meals each day? | (Q47) | How much safflower oil, cottonseed oil, and soybean oil do you use? |
| (Q14) | How much staple food do you eat? | (Q48) | How much perilla oil, egoma oil, and flaxseed oil do you use? |
| (Q15) | How many potatoes, pumpkin, and lotus root do you eat? | (Q49) | How many salty things do you eat? |
| (Q16) | How much fruit do you eat? | (Q50) | How many pickles do you eat? |
| (Q17) | How much meat and meat products do you eat? | (Q51) | How often do you use tabletop soy sauce and sauces? |
| (Q18) | How much fish and fish products do you eat? | (Q52) | How much miso soup do you eat? |
| (Q19) | How much seafood do you eat? | (Q53) | How much soup other than miso soup do you eat? |
| (Q20) | How many eggs do you eat? | (Q54) | How often do you eat noodles? |
| (Q21) | How many soybeans and soybean products do you eat? | (Q55) | How much of the noodle soup do you drink? |
| (Q22) | How much milk and milk products do you consume? | (Q56) | How do you feel about the taste of restaurants? |
| (Q23) | How much seaweed do you eat? | (Q57) | Do you currently smoke cigarettes? |
| (Q24) | How much small fish do you eat? | (Q58) | How much alcohol do you drink? |
| Negative | Gray | Positive | p | Multi-Comparison | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | mean | SD | |||||||
| BMI | kg/m2 | 24.6 | ± | 4.3 | 29.6 | ± | 6.1 | 34.5 | ± | 9.5 | <0.001 | a |
| Skeletal muscle | kg | 23.7 | ± | 5.3 | 27.7 | ± | 7.6 | 30.7 | ± | 8.9 | <0.001 | a |
| Body fat percentage | % | 30.6 | ± | 9.3 | 35.8 | ± | 7.6 | 39.9 | ± | 8.6 | <0.001 | a |
| Waist-to-hip ratio | 0.9 | ± | 0.1 | 1.1 | ± | 1.1 | 1.0 | ± | 0.1 | <0.001 | a | |
| SMI | kg/m2 | 6.8 | ± | 1.0 | 7.7 | ± | 1.5 | 8.4 | ± | 1.7 | <0.001 | a |
| SI | kg/(kg/m2) | 0.7 | ± | 0.2 | 0.7 | ± | 0.2 | 0.7 | ± | 0.1 | 0.245 | |
| SV ratio | kg/cm2 | 324.7 | ± | 199.6 | 243.5 | ± | 84.1 | 228.5 | ± | 96.4 | <0.001 | a |
| Visceral fat cross section | cm2 | 91.7 | ± | 42.0 | 125.6 | ± | 47.1 | 151.9 | ± | 61.4 | <0.001 | a |
| Knee Extension Stretch | kgf | 36.8 | ± | 12.3 | 42.9 | ± | 16.0 | 45.9 | ± | 16.9 | <0.001 | a |
| Grip (of hand) | kgf | 28.9 | ± | 8.3 | 32.5 | ± | 10.3 | 32.4 | ± | 9.8 | 0.005 | a |
| ALB | g/dL | 4.3 | ± | 0.3 | 4.4 | ± | 0.5 | 4.3 | ± | 0.4 | 0.088 | |
| AST | U/L | 23.7 | ± | 7.1 | 44.6 | ± | 18.6 | 76.3 | ± | 36.8 | <0.001 | a,b |
| ALT | U/L | 24.3 | ± | 14.7 | 68.0 | ± | 43.0 | 103.9 | ± | 51.8 | <0.001 | a,b |
| γGT | U/L | 38.2 | ± | 41.5 | 65.0 | ± | 48.5 | 95.1 | ± | 71.2 | <0.001 | a,b |
| HDLC | mg/dL | 59.6 | ± | 16.7 | 48.6 | ± | 10.7 | 49.1 | ± | 10.7 | <0.001 | a |
| LDLC | mg/dL | 118.2 | ± | 30.1 | 122.9 | ± | 36.0 | 119.5 | ± | 28.5 | 0.644 | |
| TG | mg/dL | 111.5 | ± | 65.9 | 137.8 | ± | 59.9 | 156.1 | ± | 93.4 | <0.001 | a |
| Fasting glucose | mg/dL | 110.8 | ± | 27.2 | 117.8 | ± | 30.2 | 131.9 | ± | 38.0 | <0.001 | a,b |
| HbA1c | % | 6.0 | ± | 0.8 | 6.3 | ± | 1.3 | 6.5 | ± | 1.0 | 0.001 | a,b |
| Insulin | μU/mg | 9.9 | ± | 11.7 | 19.4 | ± | 18.1 | 25.8 | ± | 14.6 | <0.001 | a,b |
| HOMA-IR | 2.8 | ± | 4.0 | 5.6 | ± | 5.7 | 8.5 | ± | 7.0 | <0.001 | a,b | |
| Ferritin | ng/mL | 96.8 | ± | 77.9 | 164.4 | ± | 196.0 | 213.2 | ± | 294.0 | 0.001 | a |
| Type IV collagen | ng/mL | 111.0 | ± | 29.5 | 131.9 | ± | 49.8 | 188.0 | ± | 117.5 | <0.001 | a,b |
| CRP | mg/dL | 0.1 | ± | 0.2 | 0.3 | ± | 0.4 | 0.4 | ± | 0.4 | <0.001 | a,b |
| M2BPGi | C.O.I. | 0.7 | ± | 0.4 | 1.2 | ± | 1.9 | 1.3 | ± | 1.1 | <0.001 | a |
| LSM | kPa | 5.1 | ± | 1.9 | 10.5 | ± | 6.7 | 20.3 | ± | 13.8 | <0.001 | a,b |
| CAP | dB/m | 249.1 | ± | 61.5 | 316.6 | ± | 48.6 | 319.6 | ± | 55.8 | <0.001 | a |
| FIB-4 index | 1.6 | ± | 2.2 | 1.7 | ± | 1.5 | 2.2 | ± | 1.8 | 0.394 | ||
| NFS | -1.6 | ± | 1.6 | −1.6 | ± | 2.0 | -1.0 | ± | 1.9 | 0.05 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yabe, Y.; Kim, T.; Oh, S.; Shida, T.; Oshida, N.; Hasegawa, N.; Okada, K.; Someya, N.; Mizokami, Y.; Shoda, J. Relationships of Dietary Habits and Physical Activity Status with Non-Alcoholic Fatty Liver Disease Featuring Advanced Fibrosis. Int. J. Environ. Res. Public Health 2021, 18, 8918. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18178918
Yabe Y, Kim T, Oh S, Shida T, Oshida N, Hasegawa N, Okada K, Someya N, Mizokami Y, Shoda J. Relationships of Dietary Habits and Physical Activity Status with Non-Alcoholic Fatty Liver Disease Featuring Advanced Fibrosis. International Journal of Environmental Research and Public Health. 2021; 18(17):8918. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18178918
Chicago/Turabian StyleYabe, Yoshito, Taeho Kim, Sechang Oh, Takashi Shida, Natsumi Oshida, Naoyuki Hasegawa, Kosuke Okada, Noriko Someya, Yuji Mizokami, and Junichi Shoda. 2021. "Relationships of Dietary Habits and Physical Activity Status with Non-Alcoholic Fatty Liver Disease Featuring Advanced Fibrosis" International Journal of Environmental Research and Public Health 18, no. 17: 8918. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18178918