
Influence of Depression and Anxiety on Non-Surgical Periodontal Treatment Outcomes: A 6-Month Prospective Study

 and
and
Abstract
:1. Introduction
2. Materials and Methods
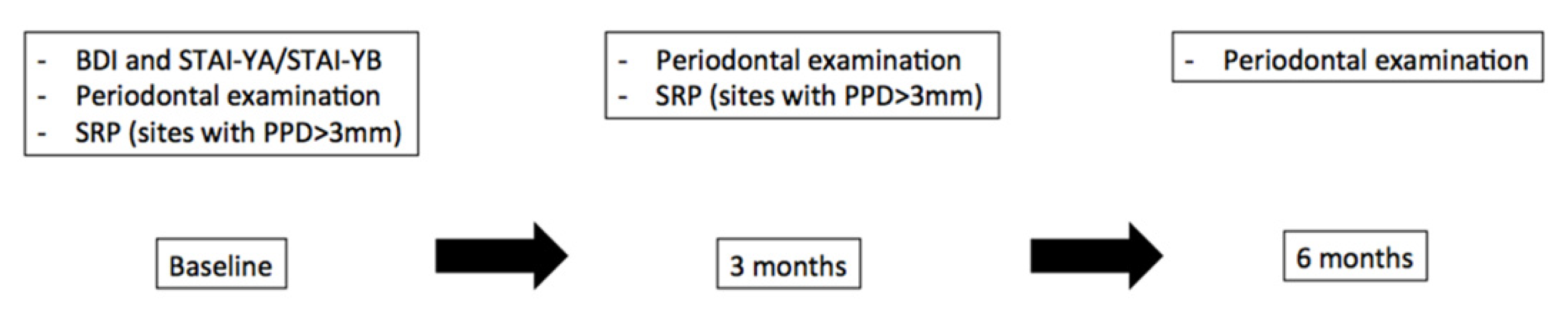
2.1. Study’s Protocol
2.2. Inclusion Criteria
2.3. Psychological Measurements
2.4. Non-Surgical Periodontal Treatment and Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Study’s Sample and Demographics
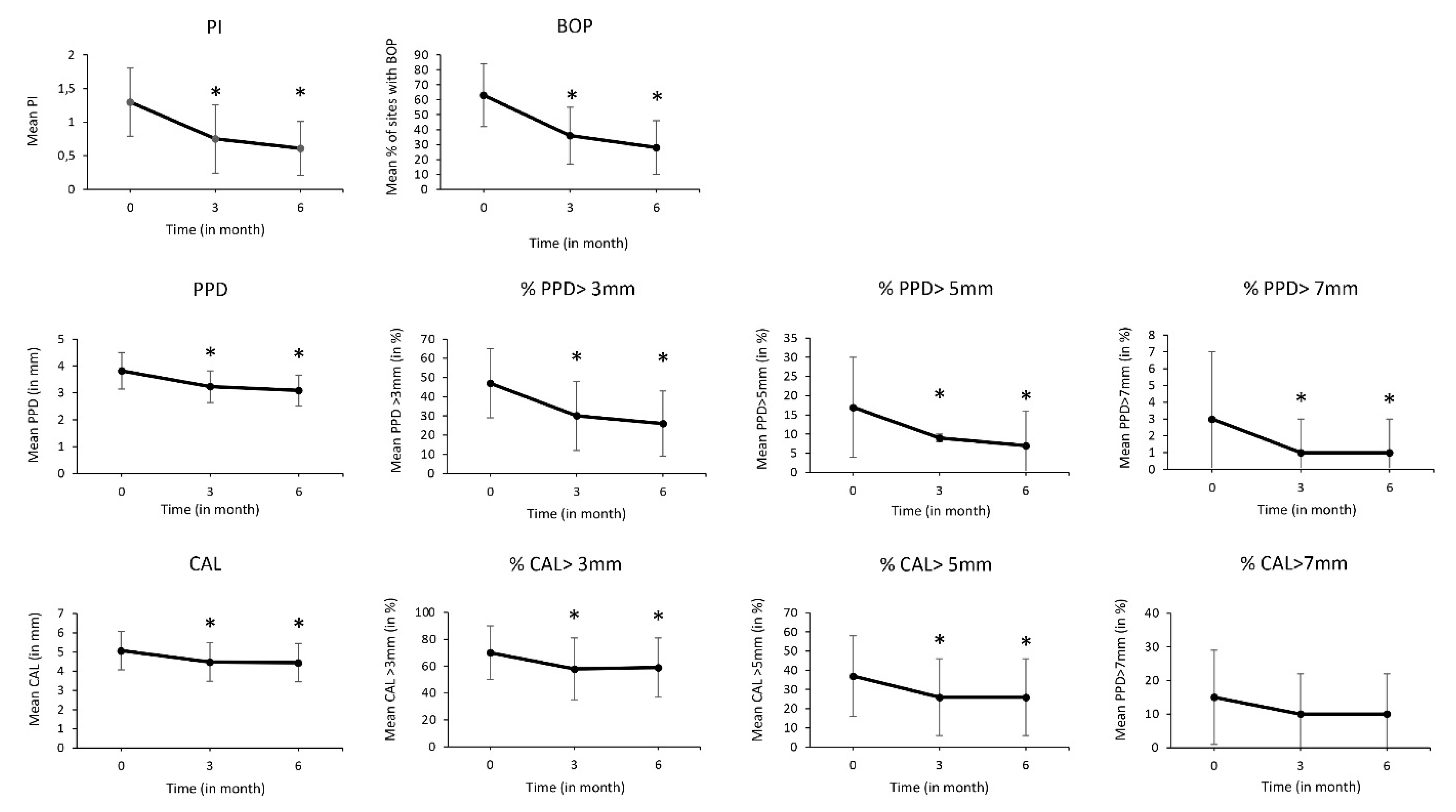
3.2. Non-Surgical Periodontal Treatment Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Curtis, M.A.; Diaz, P.I.; Van Dyke, T.E. The Role of the Microbiota in Periodontal Disease. Periodontol. 2000 2020, 83, 14–25. [Google Scholar] [CrossRef]
- GBD 2017 Oral Disorders Collaborators; Bernabe, E.; Marcenes, W.; Hernandez, C.R.; Bailey, J.; Abreu, L.G.; Alipour, V.; Amini, S.; Arabloo, J.; Arefi, Z.; et al. Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J. Dent. Res. 2020, 99, 362–373. [Google Scholar] [CrossRef]
- Schwendicke, F.; Krois, J.; Engel, A.S.; Seidel, M.; Graetz, C. Long-Term Periodontitis Treatment Costs According to the 2018 Classification of Periodontal Diseases. J. Dent. 2020, 99, 103417. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G.; Lamont, R.J. Polymicrobial Communities in Periodontal Disease: Their Quasi-Organismal Nature and Dialogue with the Host. Periodontol. 2000 2021, 86, 210–230. [Google Scholar] [CrossRef] [PubMed]
- Bugueno, I.M.; Batool, F.; Keller, L.; Kuchler-Bopp, S.; Benkirane-Jessel, N.; Huck, O. Porphyromonas Gingivalis Bypasses Epithelial Barrier and Modulates Fibroblastic Inflammatory Response in an in Vitro 3D Spheroid Model. Sci. Rep. 2018, 8, 14914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cekici, A.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Inflammatory and Immune Pathways in the Pathogenesis of Periodontal Disease. Periodontol. 2000 2014, 64, 57–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graves, D.T.; Li, J.; Cochran, D.L. Inflammation and Uncoupling as Mechanisms of Periodontal Bone Loss. J. Dent. Res. 2011, 90, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Decker, A.; Askar, H.; Tattan, M.; Taichman, R.; Wang, H.-L. The Assessment of Stress, Depression, and Inflammation as a Collective Risk Factor for Periodontal Diseases: A Systematic Review. Clin. Oral Investig. 2020, 24, 1–12. [Google Scholar] [CrossRef]
- Omer-Cihangir, R.; Baser, U.; Kucukgergin, C.; Aykol-Sahin, G.; Huck, O.; Yalcin, F. Impact of Smoking on Neutrophil Enzyme Levels in Gingivitis: A Case-Control Study. Int. J. Environ. Res. Public Health 2021, 18, 8075. [Google Scholar] [CrossRef] [PubMed]
- Akcali, A.; Huck, O.; Tenenbaum, H.; Davideau, J.L.; Buduneli, N. Periodontal Diseases and Stress: A Brief Review. J. Oral Rehabil. 2013, 40, 60–68. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A New Classification Scheme for Periodontal and Peri-Implant Diseases and Conditions–Introduction and Key Changes from the 1999 Classification. J. Periodontol. 2018, 89 (Suppl. 1), S1–S8. [Google Scholar] [CrossRef]
- Giannopoulou, C.; Kamma, J.J.; Mombelli, A. Effect of Inflammation, Smoking and Stress on Gingival Crevicular Fluid Cytokine Level. J. Clin. Periodontol. 2003, 30, 145–153. [Google Scholar] [CrossRef]
- Kamma, J.J.; Giannopoulou, C.; Vasdekis, V.G.S.; Mombelli, A. Cytokine Profile in Gingival Crevicular Fluid of Aggressive Periodontitis: Influence of Smoking and Stress. J. Clin. Periodontol. 2004, 31, 894–902. [Google Scholar] [CrossRef]
- Van Dyke, T.E.; Sima, C. Understanding Resolution of Inflammation in Periodontal Diseases: Is Chronic Inflammatory Periodontitis a Failure to Resolve? Periodontol. 2000 2020, 82, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Baeza, M.; Morales, A.; Cisterna, C.; Cavalla, F.; Jara, G.; Isamitt, Y.; Pino, P.; Gamonal, J. Effect of Periodontal Treatment in Patients with Periodontitis and Diabetes: Systematic Review and Meta-Analysis. J. Appl. Oral Sci. Rev. FOB 2020, 28, e20190248. [Google Scholar] [CrossRef] [PubMed]
- Kanmaz, B.; Lappin, D.F.; Nile, C.J.; Buduneli, N. Effects of Smoking on Non-Surgical Periodontal Therapy in Patients with Periodontitis Stage III or IV, and Grade C. J. Periodontol. 2020, 91, 442–453. [Google Scholar] [CrossRef]
- Boulaamaim, T.; Tenenbaum, H.; Davideau, J.-L.; Huck, O. Selective Influence of Smoking on Periodontal Treatment Outcomes after 3 Years of Follow-Up. Oral Health Prev. Dent. 2020, 18, 823–831. [Google Scholar] [CrossRef] [PubMed]
- Wimmer, G.; Janda, M.; Wieselmann-Penkner, K.; Jakse, N.; Polansky, R.; Pertl, C. Coping with Stress: Its Influence on Periodontal Disease. J. Periodontol. 2002, 73, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Vettore, M.; Quintanilha, R.S.; Monteiro da Silva, A.M.; Lamarca, G.A.; Leão, A.T.T. The Influence of Stress and Anxiety on the Response of Non-Surgical Periodontal Treatment. J. Clin. Periodontol. 2005, 32, 1226–1235. [Google Scholar] [CrossRef] [PubMed]
- Petit, C.; Anadon-Rosinach, V.; Rettig, L.; Schmidt-Mutter, C.; Tuzin, N.; Davideau, J.-L.; Huck, O. Influence of Psychological Stress on Non-Surgical Periodontal Treatment Outcomes in Patients with Severe Chronic Periodontitis. J. Periodontol. 2020, 92, 186–195. [Google Scholar] [CrossRef]
- Rawlinson, A.; Vettore, M.V.; Baker, S.R.; Robinson, P.G. Periodontal Treatment, Psychological Factors and Oral Health-Related Quality of Life. J. Clin. Periodontol. 2021, 48, 226–236. [Google Scholar] [CrossRef]
- Rawlinson, A.; Vettore, M.V.; Baker, S.R.; Robinson, P.G. Do Psychological Factors Predict Changes in Oral Health-Related Quality of Life and Clinical Status after Periodontal Treatment? J. Clin. Periodontol. 2021, 48, 795–804. [Google Scholar] [CrossRef]
- Lustman, P.J.; Clouse, R.E. Depression in Diabetic Patients: The Relationship between Mood and Glycemic Control. J. Diabetes Complicat. 2005, 19, 113–122. [Google Scholar] [CrossRef]
- Lwin, M.N.; Serhal, L.; Holroyd, C.; Edwards, C.J. Rheumatoid Arthritis: The Impact of Mental Health on Disease: A Narrative Review. Rheumatol. Ther. 2020, 7, 457–471. [Google Scholar] [CrossRef]
- Aldosari, M.; Helmi, M.; Kennedy, E.N.; Badamia, R.; Odani, S.; Agaku, I.; Vardavas, C. Depression, Periodontitis, Caries and Missing Teeth in the USA, NHANES 2009–2014. Fam. Med. Community Health 2020, 8, e000583. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.-C.; Hsu, Y.-C.; Chen, H.-J.; Lin, C.-C.; Chang, K.-H.; Lee, C.-Y.; Chong, L.-W.; Kao, C.-H. Association of Periodontitis and Subsequent Depression: A Nationwide Population-Based Study. Medicine 2015, 94, e2347. [Google Scholar] [CrossRef]
- Buchberger, B.; Huppertz, H.; Krabbe, L.; Lux, B.; Mattivi, J.T.; Siafarikas, A. Symptoms of Depression and Anxiety in Youth with Type 1 Diabetes: A Systematic Review and Meta-Analysis. Psychoneuroendocrinology 2016, 70, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Laforgia, A.; Corsalini, M.; Stefanachi, G.; Pettini, F.; Di Venere, D. Assessment of Psychopatologic Traits in a Group of Patients with Adult Chronic Periodontitis: Study on 108 Cases and Analysis of Compliance during and after Periodontal Treatment. Int. J. Med. Sci. 2015, 12, 832–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.-R.; Nam, S.-H. Comparison of Diagnosed Depression and Self-Reported Depression Symptom as a Risk Factor of Periodontitis: Analysis of 2016–2018 Korean National Health and Nutrition Examination Survey Data. Int. J. Environ. Res. Public Health 2021, 18, 871. [Google Scholar] [CrossRef]
- Overview of the DASS and Its Uses. Available online: http://www2.psy.unsw.edu.au/dass/over.htm (accessed on 27 August 2021).
- Spielberger, C.; Gorsuch, R.; Lushene, R.; Vagg, P.; Jacobs, G. Manual for the State-Trait Anxiety Inventory (Form Y1–Y2); Consulting Psychologists Press: Palo Alto, CA, USA, 1983; Volume IV. [Google Scholar]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Armitage, G.C. Development of a Classification System for Periodontal Diseases and Conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef]
- Hashioka, S.; Inoue, K.; Miyaoka, T.; Hayashida, M.; Wake, R.; Oh-Nishi, A.; Inagaki, M. The Possible Causal Link of Periodontitis to Neuropsychiatric Disorders: More Than Psychosocial Mechanisms. Int. J. Mol. Sci. 2019, 20, 3723. [Google Scholar] [CrossRef]
- Eger, T.; Wörner, F.; Simon, U.; Konrad, S.; Wolowski, A. Dental Anxiety and Higher Sensory Processing Sensitivity in a Sample of German Soldiers with Inflammatory Periodontal Disease. Int. J. Environ. Res. Public. Health 2021, 18, 1584. [Google Scholar] [CrossRef]
- Solis, A.C.O.; Marques, A.H.; Pannuti, C.M.; Lotufo, R.F.M.; Lotufo-Neto, F. Evaluation of Periodontitis in Hospital Outpatients with Major Depressive Disorder. J. Periodontal Res. 2014, 49, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Zheng, D.-X.; Kang, X.-N.; Wang, Y.-X.; Huang, Y.-N.; Pang, C.-F.; Chen, Y.-X.; Kuang, Z.-L.; Peng, Y. Periodontal Disease and Emotional Disorders: A Meta-Analysis. J. Clin. Periodontol. 2021, 48, 180–204. [Google Scholar] [CrossRef] [PubMed]
- Brédart, A.; Kop, J.-L.; Fall, M.; Pelissier, S.; Simondi, C.; Dolbeault, S.; Livartowski, A.; Tardivon, A. Magnetic Resonance Imaging study group (STIC IRM 2005) Anxiety and Specific Distress in Women at Intermediate and High Risk of Breast Cancer before and after Surveillance by Magnetic Resonance Imaging and Mammography versus Standard Mammography. Psychooncology 2012, 21, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Lahlou-Laforêt, K.; Ledru, F.; Niarra, R.; Consoli, S.M. PANIC Investigators Validity of Beck Depression Inventory for the Assessment of Depressive Mood in Chronic Heart Failure Patients. J. Affect. Disord. 2015, 184, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Cakmak, O.; Alkan, B.A.; Saatci, E.; Tasdemir, Z. The Effect of Nonsurgical Periodontal Treatment on Gingival Crevicular Fluid Stress Hormone Levels: A Prospective Study. Oral Dis. 2019, 25, 250–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vergne-Salle, P.; Pouplin, S.; Trouvin, A.P.; Bera-Louville, A.; Soubrier, M.; Richez, C.; Javier, R.M.; Perrot, S.; Bertin, P. The Burden of Pain in Rheumatoid Arthritis: Impact of Disease Activity and Psychological Factors. Eur. J. Pain 2020, 24, 1979–1989. [Google Scholar] [CrossRef] [PubMed]
- Hekimoglu, L.; Altun, Z.O.; Kaya, E.Z.; Bayram, N.; Bilgel, N. Psychometric Properties of the Turkish Version of the 42 Item Depression Anxiety Stress Scale (DASS-42) in a Clinical Sample. Int. J. Psychiatry Med. 2012, 44, 183–198. [Google Scholar] [CrossRef]
- Kesim, S.; Unalan, D.; Esen, C.; Ozturk, A. The Relationship between Periodontal Disease Severity and State-Trait Anxiety Level. J. Pak. Med. Assoc. 2012, 62, 1304–1308. [Google Scholar] [PubMed]
- Khambaty, T.; Stewart, J.C. Associations of Depressive and Anxiety Disorders with Periodontal Disease Prevalence in Young Adults: Analysis of 1999-2004 National Health and Nutrition Examination Survey (NHANES) Data. Ann. Behav. Med. 2013, 45, 393–397. [Google Scholar] [CrossRef]
- Delgado-Angulo, E.K.; Sabbah, W.; Suominen, A.L.; Vehkalahti, M.M.; Knuuttila, M.; Partonen, T.; Nordblad, A.; Sheiham, A.; Watt, R.G.; Tsakos, G. The Association of Depression and Anxiety with Dental Caries and Periodontal Disease among Finnish Adults. Community Dent. Oral Epidemiol. 2015, 43, 540–549. [Google Scholar] [CrossRef]
- Kolte, A.P.; Kolte, R.A.; Lathiya, V.N. Association between Anxiety, Obesity and Periodontal Disease in Smokers and Non-Smokers: A Cross-Sectional Study. J. Dent. Res. Dent. Clin. Dent. Prospect. 2016, 10, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Varotto, B.L.R.; Martinez, R.C.R.; Gouveia, F.V.; Antunes, G.F.; de Campos Fabri, G.M.; Ballester, G.; Antequera, R.; de Siqueira, S.R.D.T.; Fonoff, E.T.; Teixeira, M.J.; et al. Increased Anxiety-Like Behavior in the Acute Phase of a Preclinical Model of Periodontal Disease. Front. Neurol. 2020, 11, 598851. [Google Scholar] [CrossRef] [PubMed]
- Decker, A.M.; Kapila, Y.L.; Wang, H.-L. The Psychobiological Links between Chronic Stress-Related Diseases, Periodontal/Peri-Implant Diseases, and Wound Healing. Periodontol. 2000 2021, 87, 94–106. [Google Scholar] [CrossRef]
- Ramlogan, S.; Raman, V.; Abraham, K.; Pierre, K. Self-reported Stress, Coping Ability, Mental Status, and Periodontal Diseases among Police Recruits. Clin. Exp. Dent. Res. 2019, 6, 117–123. [Google Scholar] [CrossRef]
- Hashioka, S.; Inoue, K.; Hayashida, M.; Wake, R.; Oh-Nishi, A.; Miyaoka, T. Implications of Systemic Inflammation and Periodontitis for Major Depression. Front. Neurosci. 2018, 12, 483. [Google Scholar] [CrossRef]
- Martínez, M.; Martín-Hernández, D.; Virto, L.; MacDowell, K.S.; Montero, E.; González-Bris, Á.; Marín, M.J.; Ambrosio, N.; Herrera, D.; Leza, J.C.; et al. Periodontal Diseases and Depression: A Pre-Clinical in Vivo Study. J. Clin. Periodontol. 2021, 48, 503–527. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-X.; Kang, X.-N.; Cao, Y.; Zheng, D.-X.; Lu, Y.-M.; Pang, C.-F.; Wang, Z.; Cheng, B.; Peng, Y. Porphyromonas Gingivalis Induces Depression via Downregulating P75NTR-Mediated BDNF Maturation in Astrocytes. Brain Behav. Immun. 2019, 81, 523–534. [Google Scholar] [CrossRef] [PubMed]
- Johannsen, A.; Rydmark, I.; Söder, B.; Asberg, M. Gingival Inflammation, Increased Periodontal Pocket Depth and Elevated Interleukin-6 in Gingival Crevicular Fluid of Depressed Women on Long-Term Sick Leave. J. Periodontal Res. 2007, 42, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Johannsen, A.; Rylander, G.; Söder, B.; Asberg, M. Dental Plaque, Gingival Inflammation, and Elevated Levels of Interleukin-6 and Cortisol in Gingival Crevicular Fluid from Women with Stress-Related Depression and Exhaustion. J. Periodontol. 2006, 77, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- de Solis, A.C.O.; Marques, A.H.; Dominguez, W.V.; de Prado, E.B.A.; Pannuti, C.M.; Lotufo, R.F.M.; Lotufo-Neto, F. Evaluation of Periodontitis in Hospital Outpatients with Major Depressive Disorder. A Focus on Gingival and Circulating Cytokines. Brain Behav. Immun. 2016, 53, 49–53. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Score | Estimate (SD) | OR (CI) | p-Value |
|---|---|---|---|---|
| ΔPI | BDI | −0.01 (0.003) | <0.001 | |
| STAI-YA | −0.00 (0.002) | 0.96 | ||
| STAI-YB | 0.01 (0.002) | <0.001 | ||
| ΔBOP | BDI | 0.00 (0.003) | 0.91 | |
| STAI -YA | 0.019 (0.002) | <0.0001 | ||
| STAI-YB | −0.017 (0.002) | <0.0001 | ||
| ΔPPD (mean) | BDI | −0.010 (0.006) | 0.070 | |
| STAI-YA | 0.010 (0.004) | 0.014 | ||
| STAI-YB | −0.006 (0.004) | 0.202 | ||
| ΔPPD > 3 mm | BDI | 0.97 (0.95–0.99) | 0.004 | |
| STAI-YA | 1.01 (0.99–1.02) | 0.113 | ||
| STAI-YB | 0.999 (0.98–1.01) | 0.874 | ||
| ΔPPD > 5 mm | BDI | 1.011 (0.98–1.04) | 0.435 | |
| STAI-YA | 1.01 (0.99–1.03) | 0.290 | ||
| STAI-YB | 0.99 (0.97–1.01) | 0.584 | ||
| ΔPPD > 7 mm | BDI | 1.03 (0.97–1.10) | 0.321 | |
| STAI-YA | 1.01 (0.97–1.05) | 0.523 | ||
| STAI-YB | 0.98 (0.93–1.02) | 0.282 | ||
| ΔCAL (mean) | BDI | −0.014 (0.008) | 0.075 | |
| STAI-YA | 0.003 (0.005) | 0.637 | ||
| STAI-YB | 0.007 (0.006) | 0.272 | ||
| ΔCAL > 3 mm | BDI | 0.980 (0.96–1.00) | 0.03 | |
| STAI-YA | 1.007 (0.99–1.02) | 0.453 | ||
| STAI-YB | 1.007 (0.99–1.02) | 0.332 | ||
| ΔCAL > 5 mm | BDI | 0.99 (0.97–1.00) | 0.344 | |
| STAI-YA | 1.002 (0.98–1.02) | 0.787 | ||
| STAI-YB | 1.008 (0.99–1.02) | 0.268 | ||
| ΔCAL > 7 mm | BDI | 0.99 (0.96–1.01) | 0.486 | |
| STAI-YA | 1.003 (0.98–1.02) | 0.785 | ||
| STAI-YB | 1.006 (0.98–1.02) | 0.552 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petit, C.; Anadon-Rosinach, V.; Tuzin, N.; Davideau, J.-L.; Huck, O. Influence of Depression and Anxiety on Non-Surgical Periodontal Treatment Outcomes: A 6-Month Prospective Study. Int. J. Environ. Res. Public Health 2021, 18, 9394. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179394
Petit C, Anadon-Rosinach V, Tuzin N, Davideau J-L, Huck O. Influence of Depression and Anxiety on Non-Surgical Periodontal Treatment Outcomes: A 6-Month Prospective Study. International Journal of Environmental Research and Public Health. 2021; 18(17):9394. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179394
Chicago/Turabian StylePetit, Catherine, Victor Anadon-Rosinach, Nicolas Tuzin, Jean-Luc Davideau, and Olivier Huck. 2021. "Influence of Depression and Anxiety on Non-Surgical Periodontal Treatment Outcomes: A 6-Month Prospective Study" International Journal of Environmental Research and Public Health 18, no. 17: 9394. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179394