
Association between Having Cancer and Psychological Distress among Family Caregivers Using Three Years of a Nationwide Survey Data in Japan

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
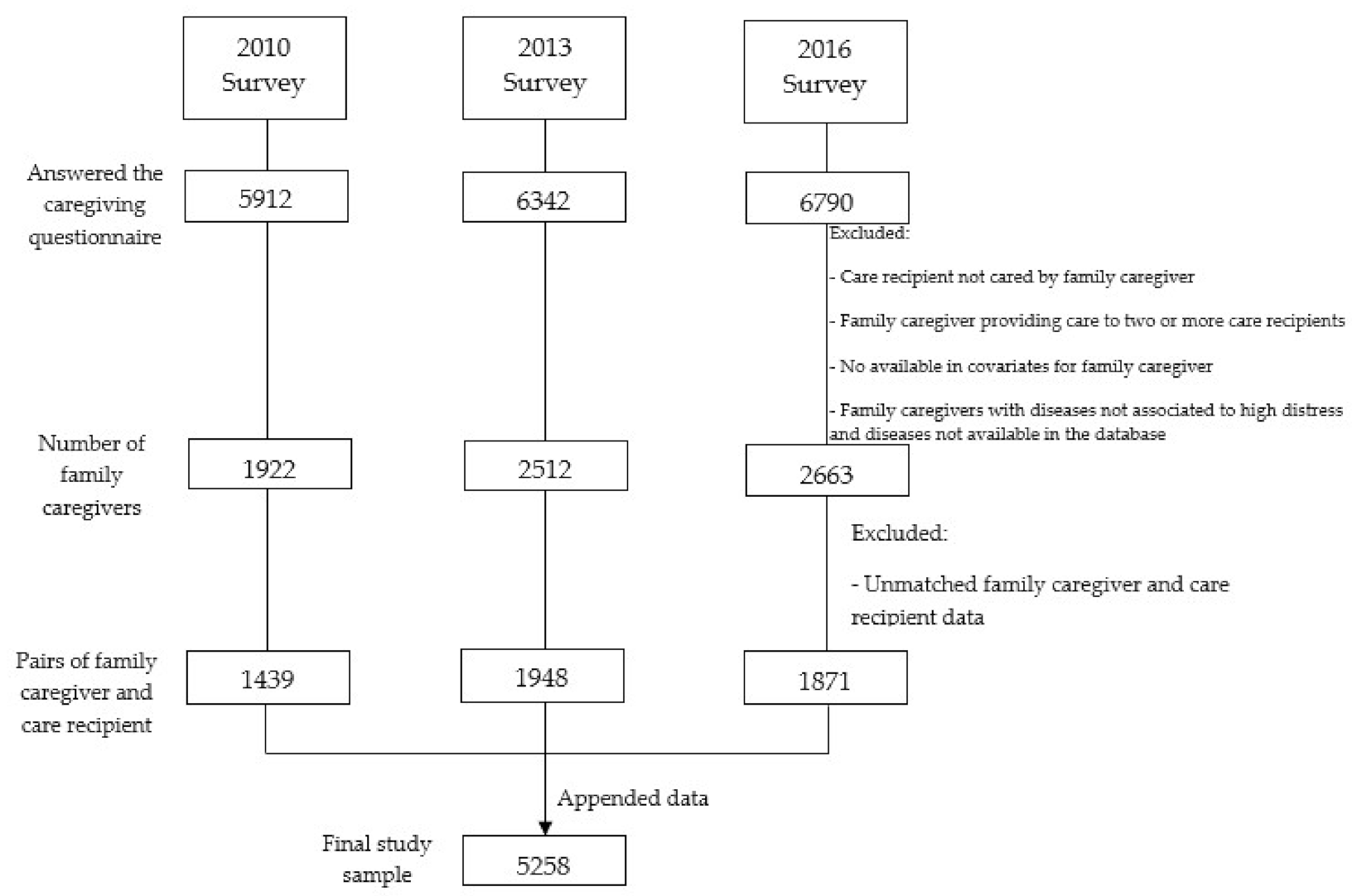
2.2. Participants
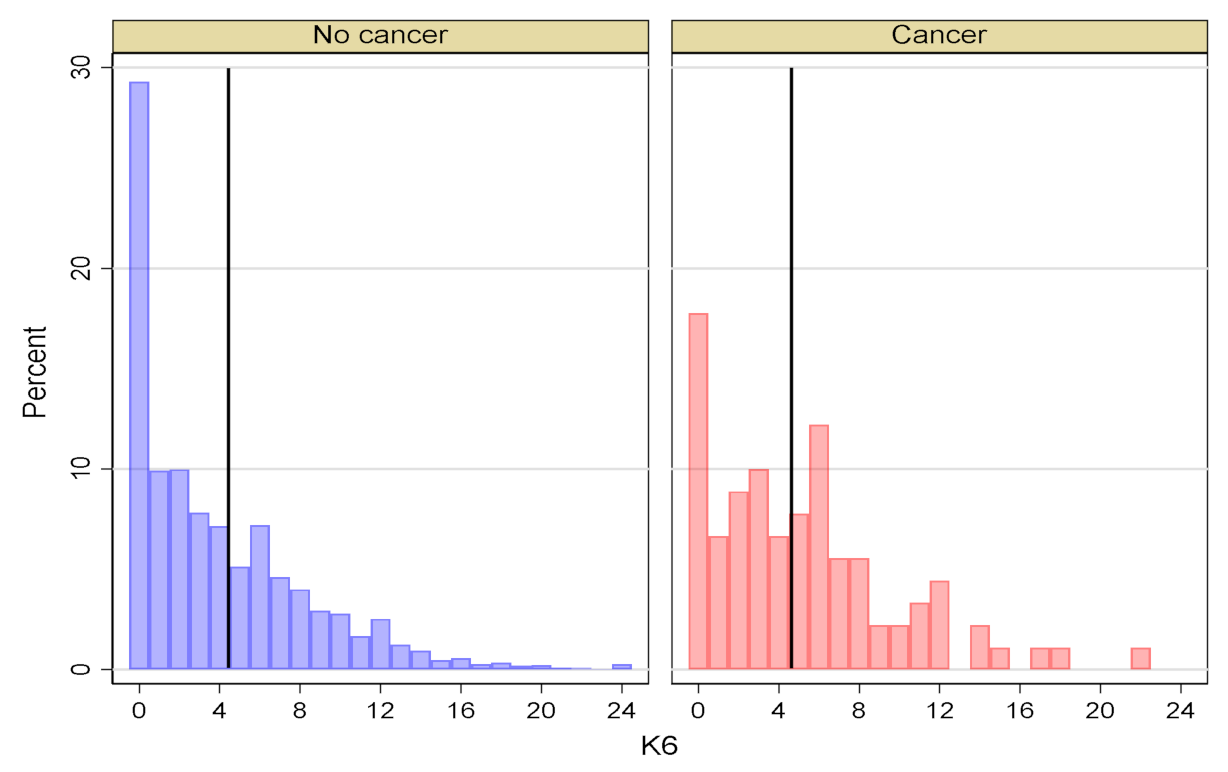
2.3. Dependent Variable (Outcome)
2.4. Independent Variable (Exposure)
2.5. Covariates
2.6. Data Analysis
2.7. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Suzman, R.; Beard, J.R.; Boerma, T.; Chatterji, S. Health in an ageing world—What do we know? Lancet 2015, 385, 484–486. [Google Scholar] [CrossRef]
- Tamiya, N.; Noguchi, H.; Nishi, A.; Reich, M.R.; Ikegami, N.; Hashimoto, H.; Shibuya, K.; Kawachi, I.; Campbell, J.C. Population ageing and wellbeing: Lessons from Japan’s long-term care insurance policy. Lancet 2011, 378, 1183–1192. [Google Scholar] [CrossRef]
- Saito, T.; Kondo, N.; Shiba, K.; Murata, C.; Kondo, K. Income-based inequalities in caregiving time and depressive symptoms among older family caregivers under the Japanese long-term care insurance system: A cross-sectional analysis. PLoS ONE 2018, 13, e0194919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shikimoto, R.; Sado, M.; Ninomiya, A.; Yoshimura, K.; Ikeda, B.; Baba, T.; Mimura, M. Predictive factors associated with psychological distress of caregivers of people with dementia in Japan: A cross-sectional study. Int. Psychogeriatr. 2018, 30, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Oshio, T. How is an informal caregiver’s psychological distress associated with prolonged caregiving? Evidence from a six-wave panel survey in Japan. Qual. Life Res. 2015, 24, 2907–2915. [Google Scholar] [CrossRef]
- Navaie-Waliser, M.; Feldman, P.H.; Gould, D.A.; Levine, C.; Kuerbis, A.N.; Donelan, K. When the caregiver needs care: The plight of vulnerable caregivers. Am. J. Public Health 2002, 92, 409–413. [Google Scholar] [CrossRef]
- Morimoto, T.; Schreiner, A.S.; Asano, H. Caregiver burden and health-related quality of life among Japanese stroke caregivers. Age Ageing 2003, 32, 218–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, S.C.; Chan, A.; Woo, J.; Chong, P.; Sham, A. Impact of caregiving on health and quality of life: A comparative population-based study of caregivers for elderly persons and noncaregivers. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 873–879. [Google Scholar] [CrossRef]
- Anand, K.S.; Dhikav, V.; Sachdeva, A.; Mishra, P. Perceived caregiver stress in Alzheimer’s disease and mild cognitive impairment: A case control study. Ann. Indian Acad. Neurol. 2016, 19, 58–62. [Google Scholar] [PubMed]
- Black, W.; Almeida, O.P. A systematic review of the association between the Behavioral and Psychological Symptoms of Dementia and burden of care. Int. Psychogeriatr. 2004, 16, 295–315. [Google Scholar] [CrossRef]
- Mausbach, B.T.; Patterson, T.L.; Rabinowitz, Y.G.; Grant, I.; Schulz, R. Depression and distress predict time to cardiovascular disease in dementia caregivers. Health Psychol. 2007, 26, 539–544. [Google Scholar] [CrossRef] [Green Version]
- Vitaliano, P.P.; Scanlan, J.M.; Krenz, C.; Schwartz, R.S.; Marcovina, S.M. Psychological Distress, Caregiving, and Metabolic Variables. J. Gerontol. Ser. B 1996, 51B, P290–P299. [Google Scholar] [CrossRef] [Green Version]
- Remes-Troche, J.M.; Torres-Aguilera, M.; Montes-Martínez, V.; Jiménez-García, V.A.; Roesch-Dietlen, F. Prevalence of irritable bowel syndrome in caregivers of patients with chronic diseases. Neurogastroenterol. Motil. 2015, 27, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, Y.; Shimizu, T.; Hayakawa, K. Depressive states and health problems in caregivers of the disabled elderly at home. Environ. Health Prev. Med. 1997, 1, 165–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Labour and Welfare of Japan. Comprehensive Survey of Living Conditions for 2016; Ministry of Health, Labour and Welfare of Japan: Tokyo, Japan, 2017.
- Foundation for Promotion of Cancer Research. Cancer Statistics in Japan 2018. Available online: https://ganjoho.jp/data/reg_stat/statistics/brochure/2018/cancer_statistics_2018_app_J.pdf (accessed on 20 July 2021).
- Ha, S.H.; Shim, I.H.; Bae, D.S. Differences in depressive and anxiety symptoms between cancer and noncancer patients with psychological distress. Indian J. Psychiatry 2019, 61, 395–399. [Google Scholar]
- Han, X.; Lin, C.C.; Li, C.; de Moor, J.S.; Rodriguez, J.L.; Kent, E.E.; Forsythe, L.P. Association between serious psychological distress and health care use and expenditures by cancer history. Cancer 2015, 121, 614–622. [Google Scholar] [CrossRef]
- Moon, H.; Dilworth-Anderson, P. Baby boomer caregiver and dementia caregiving: Findings from the National Study of Caregiving. Age Ageing 2015, 44, 300–306. [Google Scholar] [CrossRef] [Green Version]
- Sherner, T. The Case of the Caregiver With Cancer. ONS Connect 2016, 31, 20. [Google Scholar]
- Wright, P.; Downing, A.; Morris, E.J.; Corner, J.L.; Richards, M.A.; Sebag-Montefiore, D.; Finan, P.; Glaser, A.W. Identifying Social Distress: A Cross-Sectional Survey of Social Outcomes 12 to 36 Months After Colorectal Cancer Diagnosis. J. Clin. Oncol. 2015, 33, 3423–3430. [Google Scholar] [CrossRef]
- Vitaliano, P.P.; Scanlan, J.M.; Ochs, H.D.; Syrjala, K.; Siegler, I.C.; Snyder, E.A. Psychosocial stress moderates the relationship of cancer history with natural killer cell activity. Ann. Behav. Med. 1998, 20, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Ridner, S.H. Psychological distress: Concept analysis. J. Adv. Nurs. 2004, 45, 536–545. [Google Scholar] [CrossRef]
- Drapeau, A.; Marchand, A.; Beaulieu-Prevost, D. Epidemiology of Psychological Distress. In Mental Illnesses—Understanding, Prediction and Control; IntechOpen: London, UK, 2012. [Google Scholar]
- Kumagai, N. Distinct impacts of high intensity caregiving on caregivers’ mental health and continuation of caregiving. Health Econ. Rev. 2017, 7, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugiyama, T.; Tamiya, N.; Watanabe, T.; Wakui, T.; Shibayama, T.; Moriyama, Y.; Yamaoka, Y.; Noguchi, H. Association of care recipients’ care-need level with family caregiver participation in health check-ups in Japan. Geriatr. Gerontol. Int. 2018, 18, 26–32. [Google Scholar] [CrossRef] [Green Version]
- Tokunaga, M.; Hashimoto, H.; Tamiya, N. A gap in formal long-term care use related to characteristics of caregivers and households, under the public universal system in Japan: 2001–2010. Health Policy 2015, 119, 840–849. [Google Scholar] [CrossRef]
- Piazza, J.R.; Charles, S.T.; Almeida, D.M. Living with chronic health conditions: Age differences in affective well-being. J. Gerontol. Ser. B 2007, 62, P313–P321. [Google Scholar] [CrossRef] [PubMed]
- Hamashima, C. Cancer screening guidelines and policy making: 15 years of experience in cancer screening guideline development in Japan. Jpn. J. Clin. Oncol. 2018, 48, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y.; Tachimori, H.; Iwata, N.; Uda, H.; Nakane, H.; et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res. 2008, 17, 152–158. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Kessler, R.C.; Slade, T.; Andrews, G. The performance of the K6 and K10 screening scales for psychological distress in the Australian National Survey of Mental Health and Well-Being. Psychol. Med. 2003, 33, 357–362. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Sung, H.Y.; Max, W.; Shi, Y.; Ong, M. Validity study of the K6 scale as a measure of moderate mental distress based on mental health treatment need and utilization. Int. J. Methods Psychiatr. Res. 2012, 21, 88–97. [Google Scholar] [CrossRef]
- Sakurai, K.; Nishi, A.; Kondo, K.; Yanagida, K.; Kawakami, N. Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan. Psychiatry Clin. Neurosci. 2011, 65, 434–441. [Google Scholar] [CrossRef]
- Liu, Q.; Cai, H.; Yang, L.H.; Xiang, Y.B.; Yang, G.; Li, H.; Gao, Y.T.; Zheng, W.; Susser, E.; Shu, X.O. Depressive symptoms and their association with social determinants and chronic diseases in middle-aged and elderly Chinese people. Sci. Rep. 2018, 8, 3841. [Google Scholar] [CrossRef]
- Birk, J.L.; Kronish, I.M.; Moise, N.; Falzon, L.; Yoon, S.; Davidson, K.W. Depression and multimorbidity: Considering temporal characteristics of the associations between depression and multiple chronic diseases. Health Psychol. 2019, 38, 802–811. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Cao, H.; Zhu, H.; Zhang, H.; Niu, K.; Tang, N.; Cui, Z.; Pan, L.; Yao, C.; Gao, Q.; et al. Association of chronic diseases with depression, anxiety and stress in Chinese general population: The CHCN-BTH cohort study. J. Affect. Disord. 2021, 282, 1278–1287. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.M.; Chung, G.E.; Kang, S.J.; Kwak, M.S.; Yang, J.I.; Park, B.; Yim, J.Y. Association Between Anxiety and Depression and Nonalcoholic Fatty Liver Disease. Front. Med. 2020, 7, 585618. [Google Scholar] [CrossRef]
- Jin, X.; Tamiya, N.; Jeon, B.; Kawamura, A.; Takahashi, H.; Noguchi, H. Resident and facility characteristics associated with care-need level deterioration in long-term care welfare facilities in Japan. Geriatr. Gerontol. Int. 2018, 18, 758–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, G. A modified poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef]
- Lutz, B.J.; Young, M.E. Rethinking intervention strategies in stroke family caregiving. Rehabil. Nurs. 2010, 35, 152–160. [Google Scholar] [CrossRef]
- Burgio, L.D.; Collins, I.B.; Schmid, B.; Wharton, T.; McCallum, D.; Decoster, J. Translating the REACH caregiver intervention for use by area agency on aging personnel: The REACH OUT program. Gerontologist 2009, 49, 103–116. [Google Scholar] [CrossRef]
- Ankuda, C.K.; Maust, D.T.; Kabeto, M.U.; McCammon, R.J.; Langa, K.M.; Levine, D.A. Association Between Spousal Caregiver Well-Being and Care Recipient Healthcare Expenditures. J. Am. Geriatr. Soc. 2017, 65, 2220–2226. [Google Scholar] [CrossRef]
- Collins, L.G.; Swartz, K. Caregiver care. Am. Fam. Physician 2011, 83, 1309–1317. [Google Scholar] [PubMed]
- United Nations, Department of Economic and Social Affairs. World Population Prospects 2019. Available online: https://population.un.org/wpp/Download/Standard/Population/ (accessed on 10 September 2021).
- Pinquart, M.; Sorensen, S. Correlates of physical health of informal caregivers: A meta-analysis. J. Gerontol. B Psychol. Sci. Soc. Sci. 2007, 62, P126–P137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, B.; Kim, S.Y.; Shin, J.Y.; Sanson-Fisher, R.W.; Shin, D.W.; Cho, J.; Park, J.H. Prevalence and predictors of anxiety and depression among family caregivers of cancer patients: A nationwide survey of patient-family caregiver dyads in Korea. Support. Care Cancer 2013, 21, 2799–2807. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Internal Affairs and Communications. Overview of the 2015 Census Postcensal Survey. Available online: https://www.stat.go.jp/info/kenkyu/kokusei/yusiki27/pdf/05sy0300.pdf (accessed on 10 September 2021).
- Ministry of Health, Labour and Welfare. The Comprehensive Survey of Living Conditions, Outlines of Survey. Available online: https://www.mhlw.go.jp/toukei/list/20-21tyousa.html#anchor09 (accessed on 10 September 2021).



{kind=link}
{kind=link}
| Total | Cancer | No Cancer | |||
|---|---|---|---|---|---|
| n (%) ‡ | n (%) ‡ | n (%) ‡ | p-Value † | ||
| Total | 5258 (100.0) | 90 (1.7) | 5168 (98.3) | ||
| Survey year | 2010 | 1439 (27.4) | 23 (25.6) | 1416 (27.4) | 0.54 |
| 2013 | 1948 (37.1) | 30 (33.3) | 1918 (37.1) | ||
| 2016 | 1871 (35.6) | 37 (41.1) | 1834 (35.5) | ||
| Family caregivers’ Characteristics | |||||
| Sex | Male | 1616 (30.7) | 25 (27.8) | 1591 (30.8) | 0.54 |
| Female | 3642 (69.3) | 65 (72.2) | 3577 (69.2) | ||
| Age | 40–64 | 2724 (51.8) | 38 (42.2) | 2686 (52.0) | 0.24 |
| 65–74 | 1288 (24.5) | 29 (32.2) | 1259 (24.4) | ||
| 75–84 | 972 (18.5) | 17 (18.9) | 955 (18.5) | ||
| 85+ | 274 (5.2) | 6 (6.7) | 268 (5.2) | ||
| Education history | Elementary/junior high school | 1429 (27.2) | 18 (20.0) | 1411 (27.3) | 0.11 |
| High school | 2533 (48.2) | 53 (58.9) | 2480 (48.0) | ||
| University/graduate school | 1296 (24.7) | 19 (21.1) | 1277 (24.7) | ||
| Job status | Having any job | 2224 (42.3) | 25 (27.8) | 2199 (42.6) | 0.005 |
| Not having a job | 3034 (57.7) | 65 (72.2) | 2969 (57.5) | ||
| Monthly expenditure § | Less than 7.5 (×10,000 yen) per month | 2605 (49.5) | 40 (44.4) | 2565 (49.6) | 0.33 |
| From 7.5 (×10,000 yen) per month | 2653 (50.6) | 50 (55.6) | 2603 (50.4) | ||
| Current smoking status | Yes | 696 (13.2) | 3 (3.3) | 693 (13.4) | 0.005 |
| No | 4562 (86.8) | 87 (96.7) | 4475 (86.6) | ||
| Relationship with the care recipient | Spouse | 1920 (36.5) | 31 (34.4) | 1889 (36.5) | 0.61 |
| Son/daughter | 1872 (35.6) | 36 (40.0) | 1836 (35.5) | ||
| Son-in-law/daughter-in-law | 1331 (25.3) | 19 (21.1) | 1312 (25.4) | ||
| Parent | 25 (0.5) | 1 (1.1) | 24 (0.5) | ||
| Other relatives | 110 (2.1) | 3 (3.3) | 107 (2.1) | ||
| Help from family members | Having help from family members | 2552 (48.5) | 43 (47.8) | 2509 (48.6) | 0.89 |
| Not having help from family members | 2706 (51.5) | 47 (52.2) | 2659 (51.5) | ||
| Use of formal help services | Using any formal help services | 3357 (63.9) | 59 (65.6) | 3298 (63.8) | 0.73 |
| Not using any formal help services | 1901 (36.1) | 31 (34.4) | 1870 (36.2) | ||
| Adjusted † | |||
|---|---|---|---|
| Variable | RR | 95% CI | p-Value |
| Cancer | 1.33 | 1.05–1.69 | 0.016 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morales Aliaga, M.L.; Ito, T.; Sugiyama, T.; Bolt, T.; Tamiya, N. Association between Having Cancer and Psychological Distress among Family Caregivers Using Three Years of a Nationwide Survey Data in Japan. Int. J. Environ. Res. Public Health 2021, 18, 10479. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910479
Morales Aliaga ML, Ito T, Sugiyama T, Bolt T, Tamiya N. Association between Having Cancer and Psychological Distress among Family Caregivers Using Three Years of a Nationwide Survey Data in Japan. International Journal of Environmental Research and Public Health. 2021; 18(19):10479. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910479
Chicago/Turabian StyleMorales Aliaga, María Lisseth, Tomoko Ito, Takehiro Sugiyama, Timothy Bolt, and Nanako Tamiya. 2021. "Association between Having Cancer and Psychological Distress among Family Caregivers Using Three Years of a Nationwide Survey Data in Japan" International Journal of Environmental Research and Public Health 18, no. 19: 10479. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910479